
Topical Cyclosporine in Oral Lichen Planus—A Series of 21 Open-Label, Biphasic, Single-Patient Observations

 ,
,
Abstract
:1. Introduction
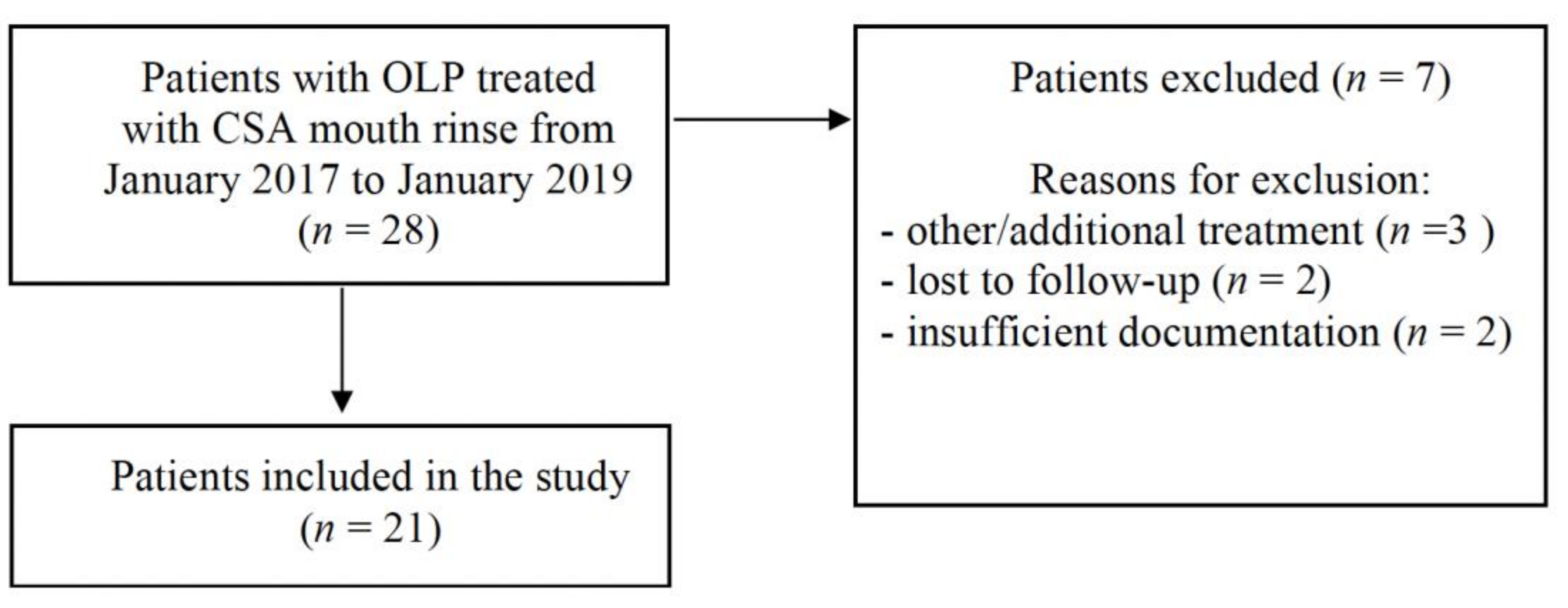
2. Materials and Methods
3. Results
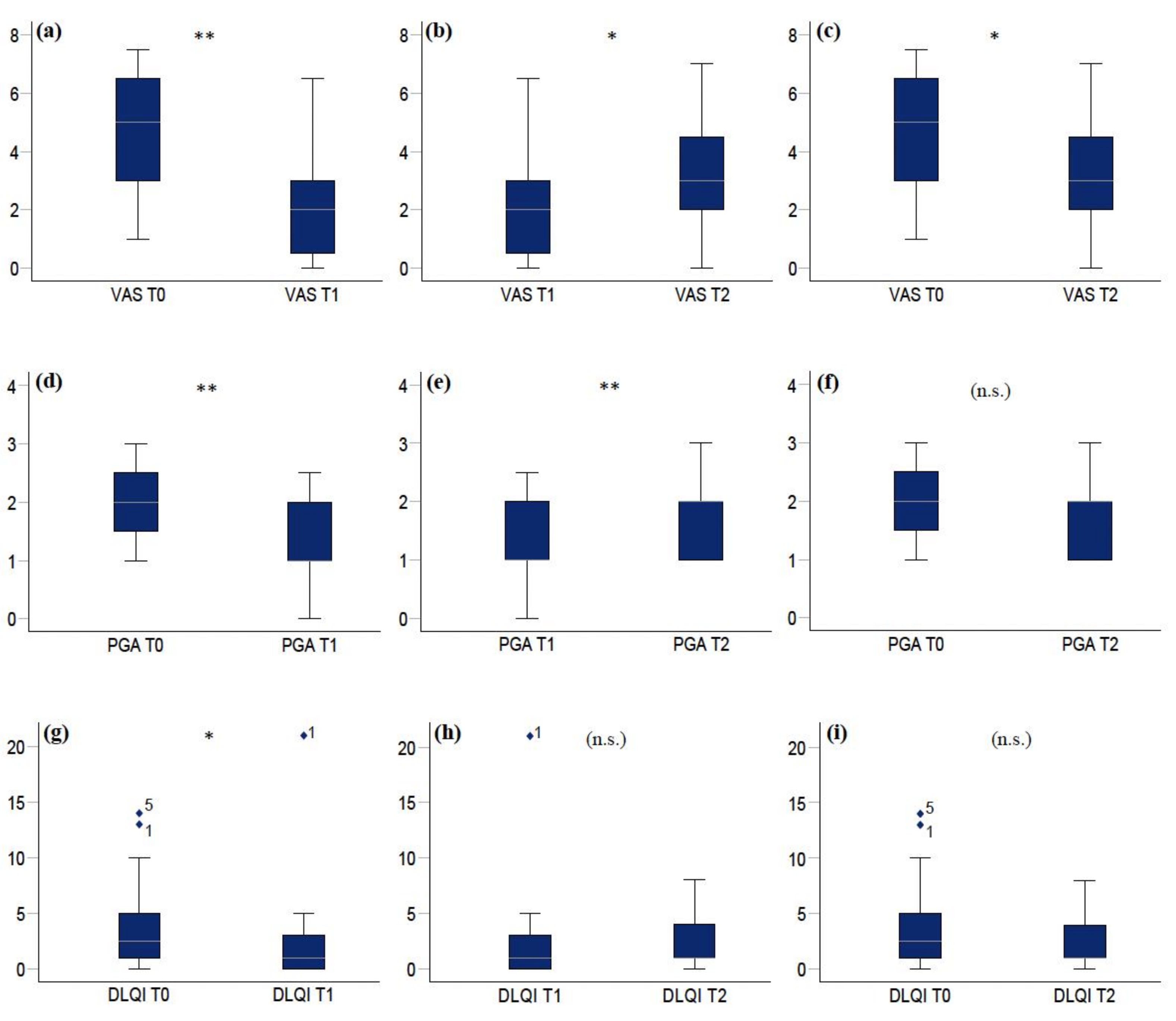
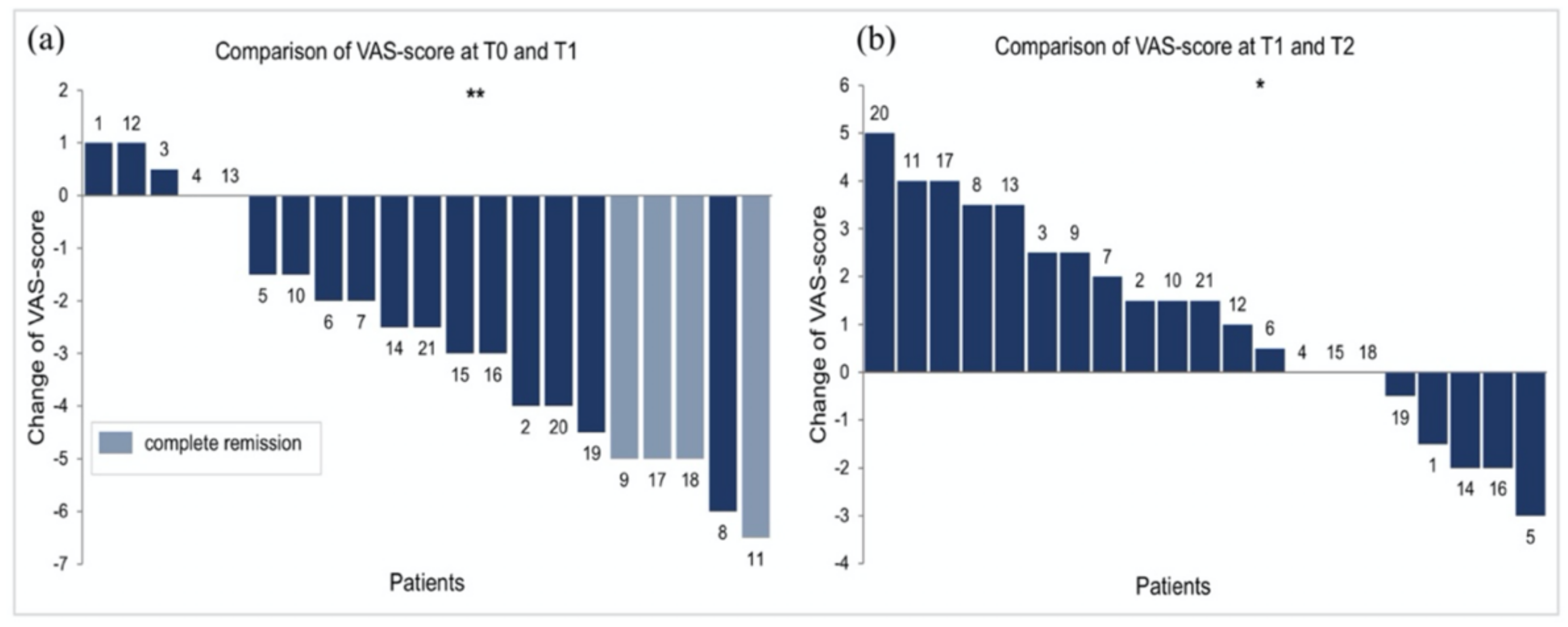
3.1. Pain (VAS Scores)
3.2. Disease Extent (PGA Scores)
3.3. Quality of Life (DLQI Scores)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al-Hashimi, I.; Schifter, M.; Lockhart, P.B.; Wray, D.; Brennan, M.; Migliorati, C.A.; Axéll, T.; Bruce, A.J.; Carpenter, W.; Eisenberg, E.; et al. Oral lichen planus and oral lichenoid le-sions: Diagnostic and therapeutic considerations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2007, 103, S25.e1–S25.e12. [Google Scholar] [CrossRef]
- Eisen, D.; Carrozzo, M.; Bagan Sebastian, J.-V.; Thongprasom, K. Number V Oral lichen planus: Clinical features and management. Oral Dis. 2005, 11, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, A.M.; Hodgson, T.A.; Lewsey, J.D.; Porter, S.R. Fluticasone propionate spray and betamethasone sodium phosphate mouthrinse: A randomized crossover study for the treatment of symptomatic oral lichen planus. J. Am. Acad. Dermatol. 2002, 47, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Brant, J.M.C.; Vasconcelos, A.C.; Rodrigues, L.V. Role of apoptosis in erosive and reticular oral lichen planus exhibiting variable epithelial thickness. Braz. Dent. J. 2008, 19, 179–185. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.; Kirtschig, G.; Cooper, S.; Thornhill, M.; Leonardi-Bee, J.; Murphy, R. Interventions for erosive lichen planus affecting mucosal sites. Cochrane Database Syst. Rev. 2012, CD008092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandolfo, S.; Richiardi, L.; Carrozzo, M.; Broccoletti, R.; Carbone, M.; Pagano, M.; Vestita, C.; Rosso, S.; Merletti, F. Risk of oral squamous cell carcinoma in 402 patients with oral lichen planus: A follow-up study in an Italian population. Oral Oncol. 2003, 40, 77–83. [Google Scholar] [CrossRef]
- Lodi, G.; Manfredi, M.; Mercadante, V.; Murphy, R.; Carrozzo, M. Interventions for treating oral lichen planus: Corticosteroid therapies. Cochrane Database Syst. Rev. 2020, CD001168. [Google Scholar] [CrossRef]
- Eisen, D.; Ellis, C.; Duell, E.A.; Griffiths, C.E.; Voorhees, J.J. Effect of Topical Cyclosporine Rinse on Oral Lichen Planus. N. Engl. J. Med. 1990, 323, 290–294. [Google Scholar] [CrossRef]
- Epstein, J.B.; Truelove, E.L. Topical cyclosporine in a bioadhesive for treatment of oral lichenoid mucosal reactions: An open label clinical trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1996, 82, 532–536. [Google Scholar] [CrossRef]
- Yeo, L.; Ormerod, A.D. Oral tacrolimus: A treatment option for recalcitrant erosive lichen planus. Clin. Exp. Dermatol. 2016, 41, 684–685. [Google Scholar] [CrossRef]
- Volz, T.; Caroli, U.; Lüdtke, H.; Bräutigam, M.; Röcken, M.; Biedermann, T.; Kohler-Späth, H. Pimecrolimus cream 1% in erosive oral lichen planus- a prospective randomized double-blind vehicle-controlled study. Br. J. Dermatol. 2008, 159, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Harpenau, L.A.; Plemons, J.M.; Rees, T.D. Effectiveness of a low dose of cyclosporine in the management of patients with oral erosive lichen planus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1995, 80, 161–167. [Google Scholar] [CrossRef]
- Reynolds, N.J.; Al-Daraji, W.I. Calcineurin inhibitors and sirolimus: Mechanisms of action and applications in dermatology. Clin. Exp. Dermatol. 2002, 27, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Dissemond, J. Pimecrolimus in an adhesive ointment is safe and effective in long-term treatment for oral lichen planus. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1009–1011. [Google Scholar] [CrossRef] [PubMed]
- McCaughey, C.; Machan, M.; Bennett, R.; Zone, J.; Hull, C. Pimecrolimus 1% cream for oral erosive lichen planus: A 6-week randomized, double-blind, vehicle-controlled study with a 6-week open-label extension to assess efficacy and safety. J. Eur. Acad. Dermatol. Venereol. 2010, 25, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Arduino, P.; Carbone, M.; Della Ferrera, F.; Elia, A.; Conrotto, D.; Gambino, A.; Comba, A.; Calogiuri, P.; Broccoletti, R. Pimecrolimus vs. tacrolimus for the topical treatment of unresponsive oral erosive lichen planus: A 8 week randomized double-blind controlled study. J. Eur. Acad. Dermatol. Venereol. 2013, 28, 475–482. [Google Scholar] [CrossRef]
- Sun, S.; Liu, J.; Zhong, B.; Wang, J.; Jin, X.; Xu, H.; Yin, F.; Liu, T.; Chen, Q.; Zeng, X. Topical calcineurin inhibitors in the treatment of oral lichen planus: A systematic review and meta-analysis. Br. J. Dermatol. 2019, 181, 1166–1176. [Google Scholar] [CrossRef]
- Naldi, L.; Stieger, M.; Hongang, T.; Bornstein, M.; Ribero, S.; Quaglino, P.; Borradori, L. Efficacy of topical tacrolimus for oral lichen planus: Real-life experience in a retrospective cohort of patients with a review of the literature. Acad. Dermatol. Venereol. 2015, 29, 1107–1113. [Google Scholar] [CrossRef]
- Chaudhry, S.I.; Pabari, S.; A Hodgson, T.; Porter, S. The use of topical calcineurin inhibitors in the management of oral lichen planus. J. Eur. Acad. Dermatol. Venereol. 2006, 21, 554–556. [Google Scholar] [CrossRef]
- Lodi, G.; Carrozzo, M.; Furness, S.; Thongprasom, K. Interventions for treating oral lichen planus: A systematic review. Br. J. Dermatol. 2012, 166, 938–947. [Google Scholar] [CrossRef]
- Conrotto, D.; Carbone, M.; Carrozzo, M.; Arduino, P.G.; Broccoletti, R.; Pentenero, M.; Gandolfo, S. Ciclosporin vs. clobetasol in the topical management of atrophic and erosive oral lichen planus: A double-blind, randomized controlled trial. Br. J. Dermatol. 2005, 154, 139–145. [Google Scholar] [CrossRef]
- Eisen, D. The clinical features, malignant potential, and systemic associations of oral lichen planus: A study of 723 patients. J. Am. Acad. Dermatol. 2002, 46, 207–214. [Google Scholar] [CrossRef]
- McCormack, H.M.; Horne, D.J.D.L.; Sheather, S. Clinical applications of visual analogue scales: A critical review. Psychol. Med. 1988, 18, 1007–1019. [Google Scholar] [CrossRef]
- Finlay, A.; Khan, G. Dermatology Life Quality Index (DLQI)-a simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematic review of the pain scales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Silverman, S.; Gorsky, M.; Lozada-Nur, F. A prospective follow-up study of 570 patients with oral lichen planus: Persistence, remission, and malignant association. Oral Surg. Oral Med. Oral Pathol. 1985, 60, 30–34. [Google Scholar] [CrossRef]
- Francès, C.; Boisnic, S.; Etienne, S.; Szpirglas, H. Effect of the Local Application of Ciclosporine A on Chronic Erosive Lichen planus of the Oral Cavity. Dermatology 1988, 177, 194–195. [Google Scholar] [CrossRef]
- Jungell, P.; Malmström, M. Cyclosporin A mouthwash in the treatment of oral lichen planus. Int. J. Oral Maxillofac. Surg. 1996, 25, 60–62. [Google Scholar] [CrossRef]
- Ho, V.C.; Conklin, R.J. Effect of Topical Cyclosporine Rinse on Oral Lichen Planus. N. Engl. J. Med. 1991, 325, 435. [Google Scholar] [CrossRef] [PubMed]
- Itin, P.; Surber, C.; Büchner, S. Lack of Effect after Local Treatment with a New Ciclosporin Formulation in Recalcitrant Erosive Oral Lichen planus. Dermatology 1992, 185, 262–265. [Google Scholar] [CrossRef] [PubMed]
- López-López, J.; Llabres, X.R. Cyclosporine A, an alternative to the oral lichen planus erosive treatment. Bull. Group. Int. Rech. Sci. Stomatol. Odontol. 1995, 38, 33–38. [Google Scholar]
- Yoke, P.C.; Tin, G.B.; Kim, M.-J.; Rajaseharan, A.; Ahmed, S.; Thongprasom, K.; Chaimusik, M.; Suresh, S.; Machin, D.; Bee, W.H.; et al. A randomized controlled trial to compare steroid with cyclosporine for the topical treatment of oral lichen planus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Thongprasom, K.; Chaimusig, M.; Korkij, W.; Sererat, T.; Luangjarmekorn, L.; Rojwattanasirivej, S. A randomized-controlled trial to compare topical cyclosporin with triamcinolone acetonide for the treatment of oral lichen planus. J. Oral Pathol. Med. 2007, 36, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Sieg, P.; VON Domarus, H.; VON Zitzewitz, V.; Iven, H.; Färber, L. Topical cyclosporin in oral lichen planus: A controlled, randomized, prospective trial. Br. J. Dermatol. 1995, 132, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Duan, N.; Kravitz, R.L.; Schmid, C.H. Single-patient (n-of-1) trials: A pragmatic clinical decision methodology for patient-centered comparative effectiveness research. J. Clin. Epidemiol. 2013, 66 (Suppl. 8), S21–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamseer, L.; Sampson, M.; Bukutu, C.; Schmid, C.; Nikles, J.N.; Tate, R.; Johnston, B.C.; Zucker, D.; Shadish, W.R.; Kravitz, R.; et al. CONSORT extension for reporting N-of-1 trials (CENT) 2015: Explanation and elaboration. J. Clin. Epidemiol. 2016, 76, 18–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escudier, M.; Ahmed, N.; Shirlaw, P.; Setterfield, J.; Tappuni, A.; Black, M.; Challacombe, S. A scoring system for mucosal disease severity with special reference to oral lichen planus. Br. J. Dermatol. 2007, 157, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Spencer, A.J. Development and evaluation of the Oral Health Impact Profile. Community Dent. Health 1994, 11, 3–11. [Google Scholar]
- Ni Riordain, R.; McCreary, C. Validity and reliability of a newly developed quality of life questionnaire for patients with chronic oral mucosal diseases. J. Oral Pathol. Med. 2011, 40, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-K.; Hurwitz, S.; Woo, S.-B. Oral lichen planus: REU scoring system correlates with pain. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 75–82. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Clinically and histologically confirmed diagnosis of OLP | Incomplete documentation |
| No prior treatments for OLP for at least two weeks before start of topical CSA | Treatment with other topical and/or systemic compounds in the two weeks before and/or during the study period |
| Treatment with topical CSA (2 mL twice daily) for four weeks | |
| After four weeks of CSA treatment, drug withdrawal for at least four weeks | |
| Baseline visit (T0), 1st follow-up (week 4; T1) and 2nd follow-up (week 8; T2) | Missed follow-up visits |
| Patients (n = 21) | Total Number (%) |
|---|---|
| Female Male | 15 (71) 6 (29) |
| Median age | Years (IQR) |
| All patients Female Male | 58 (52–67) 58 (52–66) 59 (58–70) |
| Duration until diagnosis of OLP | Months (IQR) |
| Median duration | 18 (12–44) |
| Localisation of lesions | Number of patients |
| Gingiva | 7 |
| Buccal muosa | 2 |
| Buccal mucosa/Gingiva | 6 |
| Buccal mucosa/Tongue | 3 |
| Buccal mucosa/Tongue/Lips | 2 |
| Tongue/Lips | 1 |
| Clinical subtype of OLP | Number of patients |
| Erosive/ulcerative | 15 |
| Erythematous/atrophic | 3 |
| Reticular | 3 |
| Involvement of other parts | Number of patients (%) |
| Genital involvement (%) | 3 (14) |
| Cutaneous involvement (%) | 2 (10) |
| Variable | Overall (n = 21) No. (%) Median (Q1–Q3) | Responder (n = 16) No. (%) Median (Q1–Q3) | Nonresponder (n = 5) No. (%) Median (Q1–Q3) | p-Value |
|---|---|---|---|---|
| Sex | 0.26 | |||
| Male | 6 (29%) | 6 (38%) | 0 (0%) | |
| Female | 15 (71%) | 10 (625) | 5 (100%) | |
| Age | 58 (52–66) | 59 (51–70) | 58 (52–58) | 0.50 |
| VAS T0 | 5 (3–6.5) | 5.2 (5–6.5) | 2 (2–3.5) | 0.02 |
| PGA T0 | 2 (1.5–2.5) | 2 (1.9–2.6) | 2 (1–2) | 0.18 |
| DLQI T0 * | 2.5 (1–5) | 3 (1–5) | 2 (1–10) | 0.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monshi, B.; Ellersdorfer, C.; Edelmayer, M.; Dvorak, G.; Ganger, C.; Ulm, C.; Rappersberger, K.; Vujic, I. Topical Cyclosporine in Oral Lichen Planus—A Series of 21 Open-Label, Biphasic, Single-Patient Observations. J. Clin. Med. 2021, 10, 5454. https://doi.org/10.3390/jcm10225454
Monshi B, Ellersdorfer C, Edelmayer M, Dvorak G, Ganger C, Ulm C, Rappersberger K, Vujic I. Topical Cyclosporine in Oral Lichen Planus—A Series of 21 Open-Label, Biphasic, Single-Patient Observations. Journal of Clinical Medicine. 2021; 10(22):5454. https://doi.org/10.3390/jcm10225454
Chicago/Turabian StyleMonshi, Babak, Christina Ellersdorfer, Michael Edelmayer, Gabriella Dvorak, Clemens Ganger, Christian Ulm, Klemens Rappersberger, and Igor Vujic. 2021. "Topical Cyclosporine in Oral Lichen Planus—A Series of 21 Open-Label, Biphasic, Single-Patient Observations" Journal of Clinical Medicine 10, no. 22: 5454. https://doi.org/10.3390/jcm10225454