
High-Dose Methylprednisolone Pulses for 3 Days vs. Low-Dose Dexamethasone for 10 Days in Severe, Non-Critical COVID-19: A Retrospective Propensity Score Matched Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
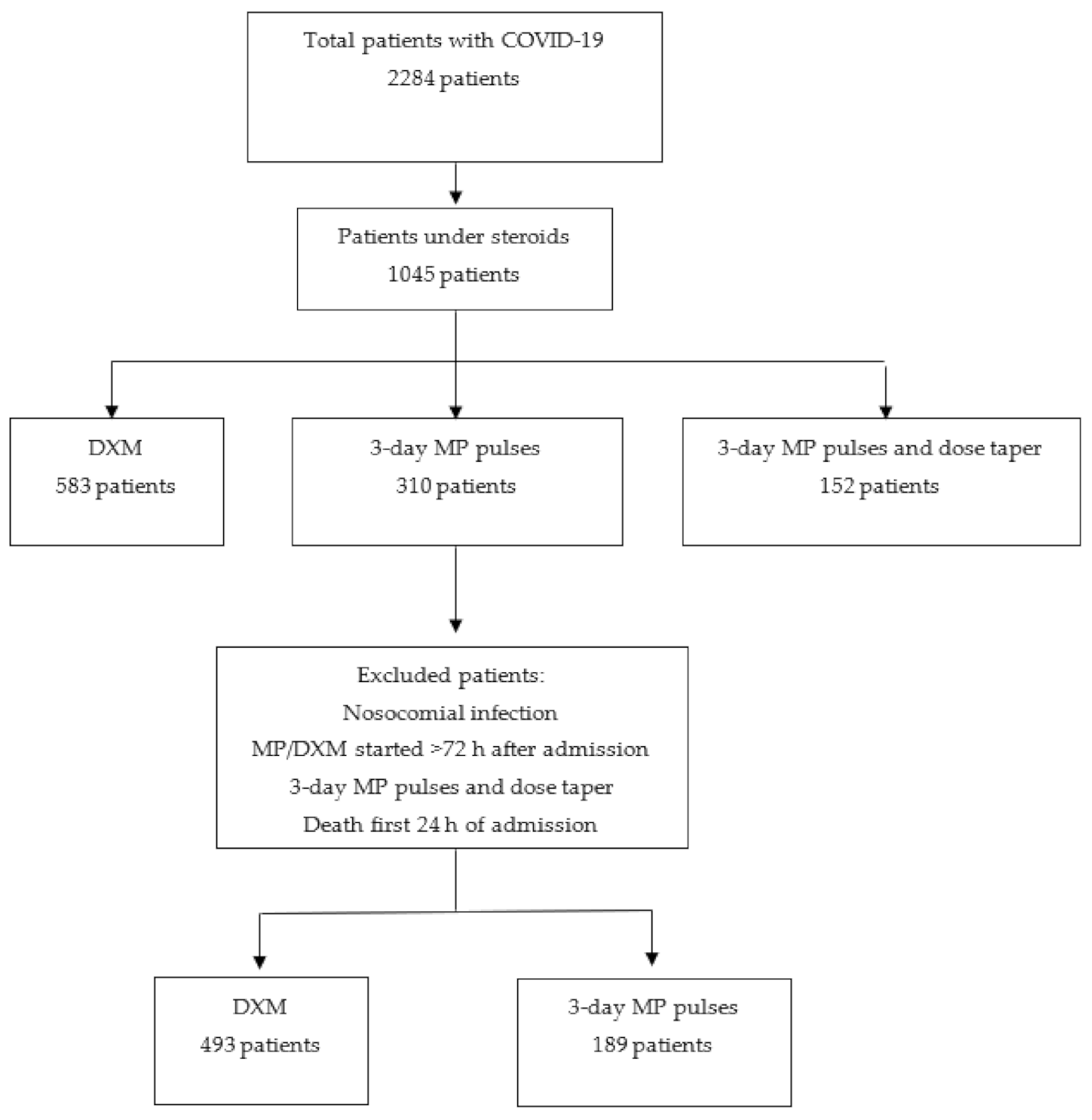
2.1. Study Design, Patients and Setting
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Treatments Prescribed and Definition of Groups
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Demographic, Comorbidity and Clinical Data
3.2. Laboratory Tests
3.3. Additional Treatments
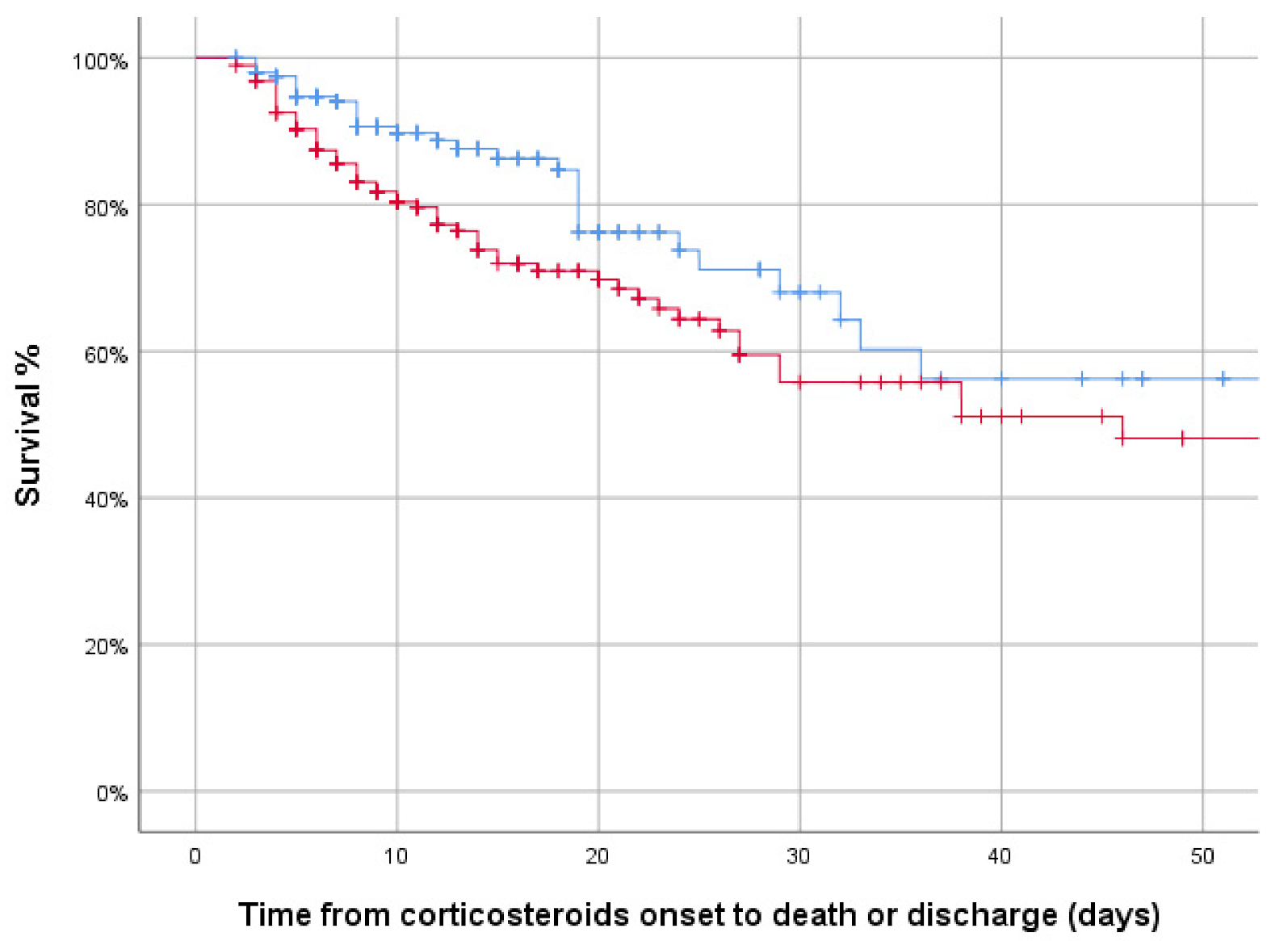
3.4. Primary and Secondary Outcomes
3.5. Risk Factors for In-Hospital Mortality and the Combined Variable
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult in patients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19)—China, 2020. China CDC Wkly. 2020, 2, 113–122. Available online: http://weekly.chinacdc.cn/en/article/id/e53946e2-c6c4-41e9-9a9b-fea8db1a8f51 (accessed on 12 March 2020). [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Du, R.H.; Liang, L.R.; Yang, C.Q.; Wang, W.; Cao, T.Z.; Li, M.; Guo, G.-Y.; Du, J.; Zheng, C.-L.; Zhu, Q.; et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: A prospective cohort study. Eur. Respir. J. 2020, 55, 2000524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodilla, E.; López-Carmona, M.D.; Cortes, X.; Cobos-Palacios, L.; Canales, S.; Sáez, M.C.; Campos Escudero, S.; Rubio-Rivas, M.; Díez Manglano, J.; Freire Castro, S.J.; et al. Impact of arterial stiffness on all-cause mortality in patients hospitalized with COVID-19 in Spain. Hypertension 2020, 77, 856–867. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Belmonte, L.M.; Torres-Peña, J.D.; López-Carmona, M.D.; Ayala-Gutiérrez, M.M.; Fuentes-Jiménez, F.; Huerta, L.J.; Muñoz, J.A.; Rubio-Rivas, M.; Madrazo, M.; Garcia, M.G.; et al. Mortality and other adverse outcomes in patients with type 2 diabetes mellitus admitted for COVID-19 in association with glucose-lowering drugs: A nationwide cohort study. BMC Med. 2020, 18, 359. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Rincon, J.-M.; Buonaiuto, V.; Ricci, M.; Martín-Carmona, J.; Paredes-Ruíz, D.; Calderón-Moreno, M.; Rubio-Rivas, M.; Beato-Pérez, J.; Arnalich-Fernández, F.; Monge-Monge, D.; et al. Clinical characteristics and risk factors for mortality in very old patients hospitalized with COVID-19 in Spain. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2021, 76, e28–e37. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef]
- Rubio-Rivas, M.; Corbella, X.; Mora-Luján, J.M.; Loureiro-Amigo, J.; López Sampalo, A.; Yera Bergua, C.; Esteve Atiénzar, P.J.; Díez García, L.F.; Gonzalez Ferrer, R.; Plaza Canteli, S.; et al. Predicting clinical outcome with phenotypic clusters in COVID-19 pneumonia: An analysis of 12,066 hospitalized patients from the spanish registry SEMI-COVID-19. J. Clin. Med. 2020, 9, 3488. [Google Scholar] [CrossRef]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2021, 93, 250–256. [Google Scholar] [CrossRef]
- Zhang, J.J.Y.; Lee, K.S.; Ang, L.W.; Leo, Y.S.; Young, B.E. Risk Factors for severe disease and efficacy of treatment in patients infected with COVID-19: A systematic review, meta-analysis, and meta-regression analysis. Clin. Infect. Dis. 2020, 71, 2199–2206. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Angus, D.C.; Derde, L.; Al-Beidh, F.; Annane, D.; Arabi, Y.; Beane, A.; van Bentum-Puijk, W.; Berry, L.; Bhimani, Z.; Bonten, M.; et al. Effect of hydrocortisone on mortality and organ support in patients with severe COVID-19: The REMAP-CAP COVID-19 corticosteroid domain randomized clinical trial. JAMA 2020, 324, 1317–1329. [Google Scholar]
- Prado Jeronimo, C.M.; Leao Farias, M.E.; Almeida Val, F.F.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Safe, I.P.; Borba, M.G.S.; Abreu-Netto, R.L.; Maciel, A.B.S.; et al. Methylprednisolone as adjunctive therapy for patients hospitalized with COVID-19 (Metcovid): A randomized, double-blind, Phase IIb, placebo-controlled trial. Clin. Infect. Dis. 2020, 72, e373–e381. [Google Scholar] [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.; et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: The CoDEX randomized clinical trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef]
- Dequin, P.F.; Heming, N.; Meziani, F.; Plantefève, G.; Voiriot, G.; Badié, J.; François, B.; Aubron, C.; Ricard, J.-D.; Ehrmann, S.; et al. Effect of hydrocortisone on 21-day mortality or respiratory support among critically ill patients with COVID-19: A randomized clinical trial. JAMA 2020, 324, 1298–1306. [Google Scholar] [CrossRef]
- Edalatifard, M.; Akhtari, M.; Salehi, M.; Naderi, Z.; Jamshidi, A.; Mostafaei, S.; Najafizadeh, S.R.; Farhadi, E.; Jalili, N.; Esfahani, M.; et al. Intravenous methylprednisolone pulse as a treatment for hospitalised severe COVID-19 patients: Results from a randomized controlled clinical trial. Eur. Respir. J. 2020, 56, 2002808. [Google Scholar] [CrossRef]
- Corral-Gudino, L.; Bahamonde, A.; Arnaiz-Revillas, F.; Gomez-Barquero, J.; Abadia-Otero, J.; Garcia-Ibarbia, C.; Mora, V.; Hernandez, J.L.; Lopez-Muniz, G.; Hernandez-Blanco, F.; et al. GLUCOCOVID: A controlled trial of methylprednisolone in adults hospitalized with COVID-19 pneumonia. Wien. Klin. Wochenschr. 2021, 133, 303–311. [Google Scholar] [CrossRef]
- Fadel, R.; Morrison, A.R.; Vahia, A.; Smith, Z.R.; Chaudhry, Z.; Bhargava, P.; Miller, J.; Kenney, R.M.; Alangaden, G.; Ramesh, M.S. Early short-course corticosteroids in hospitalized patients with COVID-19. Clin. Infect. Dis. 2020, 71, 2114–2120. [Google Scholar] [CrossRef]
- Juul, S.; Nielsen, E.E.; Feinberg, J.; Siddiqui, F.; Jørgensen, C.K.; Barot, E.; Holgersson, J.; Nielsen, N.; Bentzer, P.; Veroniki, A.A.; et al. Interventions for treatment of COVID-19: Second edition of a living systematic review with meta-analyses and trial sequential analyses (The LIVING Project). PLoS ONE 2021, 16, e0248132. [Google Scholar] [CrossRef]
- Cano, E.J.; Fonseca, X.; Corsini, C.; O’Horo, J.C.; Saleh, O.A.; Odeyemi, Y.; Yadav, H.; Temesgen, Z. Impact of corticosteroids in coronavirus disease 2019 outcomes: Systematic review and meta-analysis. Chest 2021, 159, 1019–1040. [Google Scholar] [CrossRef] [PubMed]
- Siemieniuk, R.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Qasim, A.; Martinez, J.P.D.; Rochwerg, B.; et al. Drug treatments for COVID-19: Living systematic review and network meta-analysis. BMJ 2020, 370, m2980. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Corticosteroids for COVID-19. World Health Organization Website. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoVCorticosteroids-2020.1 (accessed on 8 June 2021).
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America guidelines on the treatment and management of patients with COVID-19. Infectious Diseases Society of America Website. Available online: https://www.idsociety.org/practice-guideline/COVID-19-guideline-treatment-and-management/ (accessed on 8 June 2021).
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 8 June 2021).
- Chaudhuri, D.; Sasaki, K.; Karkar, A.; Sharif, S.; Lewis, K.; Mammen, M.J.; Alexander, P.; Ye, Z.; Lozano, L.E.C.; Munch, M.W.; et al. Corticosteroids in COVID-19 and non-COVID-19 ARDS: A systematic review and meta-analysis. Intensive Care Med. 2021, 47, 521–537. [Google Scholar] [CrossRef] [PubMed]
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Sternea, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19 a meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar]
- Rodríguez-Baño, J.; Pachón, J.; Carratalà, J.; Ryan, P.; Jarrín, I.; Yllescas, M.; Arribas, J.R.; Berenguer, J.; Munoz, E.A.; Divasson, P.G.; et al. Treatment with tocilizumab or corticosteroids for COVID-19 patients with hyperinflammatory state: A multicentre cohort study (SAMCOVID-19). Clin. Microbiol. Infect. 2021, 27, 244–252. [Google Scholar] [CrossRef]
- García Muñoz, S.; Santos, M.; Cebolla, T.; Boso, V.; Ferrando, R. High-Dose Versus Low-Dose Corticosteroid Treatment Strategy in Hospitalized COVID-19 Patients: Effect on the ICU Admission Rate. Rev. OFIL·ILAPHAR 2020, 31, 13–17. [Google Scholar] [CrossRef]
- López-Zúñiga, M.A.; Moreno-Moral, A.; Ocaña-Granados, A.; Padilla-Moreno, F.A.; Castillo-Fernández, A.M.; Guillamón-Fernández, D.; Ramírez-Sánchez, C.; Sanchez-Palop, M.; Martínez-Colmenero, J.; Pimentel-Villar, M.A.; et al. High-dose corticosteroid pulse therapy increases the survival rate in COVID-19 patients at risk of hyper-inflammatory response. PLoS ONE 2021, 16, e0243964. [Google Scholar] [CrossRef]
- Ruiz-Irastorza, G.; Pijoan, J.I.; Bereciartua, E.; Dunder, S.; Dominguez, J.; Garcia-Escudero, P.; Rodrigo, A.; Gomez-Carballo, C.; Varona, J.; Guio, L.; et al. Second week methyl-prednisolone pulses improve prognosis in patients with severe coronavirus disease 2019 pneumonia: An observational comparative study using routine care data. PLoS ONE 2020, 15, e0239401. [Google Scholar] [CrossRef]
- Meduri, G.U.; Annane, D.; Chrousos, G.P.; Marik, P.E.; Sinclair, S.E. Activation and regulation of systemic inflammation in ARDS: Rationale for prolonged glucocorticoid therapy. Chest 2009, 136, 1631–1643. [Google Scholar] [CrossRef]
- Annane, D.; Pastores, S.M.; Arlt, W.; Balk, R.A.; Beishuizen, A.; Briegel, J.; Carcillo, J.; Christ-Crain, M.; Cooper, M.S.; Marik, P.E.; et al. Critical illness-related corticosteroid insufficiency (CIRCI): A narrative review from a Multispecialty Task Force of the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM). Intensive Care Med. 2017, 43, 1781–1792. [Google Scholar] [CrossRef]
- Buttgereit, F.; Da Silva, J.P.A.; Boers, M.; Burmester, G.R.; Cutolo, M.; Jacobs, J.; Kirwan, J.; Köhler, L.; van Riel, P.L.C.M.; Vischer, T.; et al. Standardised nomenclature for glucocorticoid dosages and glucocorticoid treatment regimens: Current questions and tentative answers in rheumatology. Ann. Rheum. Dis. 2002, 61, 718–722. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Whole Cohort | Matched Sample | |||||
|---|---|---|---|---|---|---|
| 3-Day MP | DXM | p-Value | 3-Day MP | DXM | p-Value | |
| n | 189 | 493 | 189 | 199 | ||
| Age, median (IQR) | 67 (56.6–76.5) | 66.6 (56.4–76.1) | 0.642 | 67 (56.6–76.5) | 67.8 (56.8–76.6) | 0.805 |
| Gender (males) | 140 (74.1) | 326 (66.1) | 0.046 | 140 (74.1) | 143 (71.9) | 0.624 |
| Race | 0.322 | 0.879 | ||||
| Caucasian | 156 (82.5) | 390 (79.1) | 156 (82.5) | 163 (81.9) | ||
| Hispanic | 27 (14.3) | 70 (14.2) | 27 (14.3) | 30 (15.1) | ||
| Others | 6 (3.2) | 33 (6.7) | 6 (3.2) | 6 (3) | ||
| Days from onset to admission, median (IQR) | 8 (5–10) | 7 (5–10) | 0.011 | 8 (5.5–10) | 8 (7–10) | 0.648 |
| BMI | 29.8 (26.2–32.4) | 29.6 (26.9–33.5) | 0.521 | 29.8 (26.2–32.4) | 29.6 (27–33.1) | 0.939 |
| Smoking behaviour | 0.578 | 0.886 | ||||
| Never smoker | 131 (69.3) | 321 (65.1) | 131 (69.3) | 134 (67.3) | ||
| Former smoker | 49 (25.9) | 144 (29.2) | 49 (25.9) | 56 (28.1) | ||
| Current smoker | 9 (4.8) | 28 (5.7) | 9 (4.8) | 9 (4.5) | ||
| Degree of dependency | 0.874 | 0.366 | ||||
| None or mild | 174 (92.1) | 451 (91.5) | 174 (92.1) | 182 (91.5) | ||
| Moderate | 9 (4.8) | 28 (5.7) | 9 (4.8) | 14 (7) | ||
| Severe | 6 (3.2) | 14 (2.8) | 6 (3.2) | 3 (1.5) | ||
| Arterial hypertension | 97 (51.3) | 279 (56.6) | 0.216 | 97 (51.3) | 97 (48.7) | 0.612 |
| Dyslipidemia | 86 (45.5) | 222 (45) | 0.912 | 86 (45.5) | 93 (43.7) | 0.808 |
| Diabetes mellitus | 41 (21.7) | 115 (23.3) | 0.649 | 41 (21.7) | 42 (21.1) | 0.888 |
| Ischaemic cardiopathy | 10 (5.3) | 35 (7.1) | 0.395 | 10 (5.3) | 12 (6) | 0.753 |
| Cerebrovascular disease | 4 (2.1) | 30 (6.1) | 0.031 | 4 (2.1) | 5 (2.5) | 1 |
| Dementia | 7 (3.7) | 20 (4.1) | 0.832 | 7 (3.7) | 11 (5.5) | 0.393 |
| Chronic heart failure | 6 (3.2) | 25 (5.1) | 0.287 | 6 (3.2) | 7 (3.5) | 0.851 |
| Chronic liver disease | 8 (4.2) | 12 (2.4) | 0.213 | 8 (4.2) | 7 (3.5) | 0.715 |
| Severe chronic renal failure | 4 (2.1) | 15 (3) | 0.612 | 4 (2.1) | 7 (3.5) | 0.544 |
| Cancer | 9 (4.8) | 29 (5.9) | 0.568 | 9 (4.8) | 6 (3) | 0.372 |
| COPD | 10 (5.3) | 39 (7.9) | 0.236 | 10 (5.3) | 13 (6.5) | 0.605 |
| Asthma | 3 (1.6) | 22 (4.5) | 0.108 | 3 (1.6) | 3 (1.5) | 1 |
| OSAS | 11 (5.8) | 43 (8.7) | 0.209 | 11 (5.8) | 15 (7.5) | 0.499 |
| Charlson index, median (IQR) | 0 (0–1) | 0 (0–2) | 0.105 | 0 (0–1) | 0 (0–1) | 0.918 |
| Whole Cohort | Matched Sample | |||||
|---|---|---|---|---|---|---|
| 3-Day MP | DXM | p-Value | 3-Day MP | DXM | p-Value | |
| Cough, n (%) | 149 (78.8) | 344 (69.8) | 0.018 | 149 (78.8) | 142 (71.4) | 0.089 |
| Arthromyalgias, n (%) | 57 (30.2) | 122 (24.7) | 0.150 | 57 (30.2) | 49 (24.6) | 0.221 |
| Ageusia, n (%) | 22 (11.6) | 87 (17.6) | 0.055 | 22 (11.6) | 37 (18.6) | 0.057 |
| Anosmia, n (%) | 19 (10.1) | 78 (15.8) | 0.054 | 19 (10.1) | 37 (18.6) | 0.017 |
| Sore throat, n (%) | 10 (5.3) | 39 (7.9) | 0.236 | 10 (5.3) | 20 (10.1) | 0.079 |
| Headache, n (%) | 22 (11.6) | 81 (16.4) | 0.118 | 22 (11.6) | 36 (18.1) | 0.075 |
| Fever, n (%) | 167 (88.4) | 390 (79.1) | 0.005 | 167 (88.4) | 155 (77.9) | 0.006 |
| Dyspnea, n (%) | 127 (67.2) | 332 (67.3) | 0.971 | 127 (67.2) | 137 (68.8) | 0.728 |
| Diarrhea, n (%) | 63 (33.3) | 152 (30.8) | 0.529 | 63 (33.3) | 71 (35.7) | 0.627 |
| Vomiting, n (%) | 11 (5.8) | 26 (5.3) | 0.778 | 11 (5.8) | 9 (4.5) | 0.563 |
| Abdominal pain, n (%) | 4 (2.1) | 21 (4.3) | 0.255 | 4 (2.1) | 8 (4) | 0.382 |
| Heart rate, bpm median (IQR) | 93 (82–105) | 90 (80–102.5) | 0.100 | 93 (82–105) | 90 (80–105) | 0.262 |
| Respiratory rate > 20 bpm, n (%) | 116 (61.4) | 293 (59.4) | 0.643 | 116 (61.4) | 120 (60.3) | 0828 |
| Whole Cohort | Matched Sample | |||||
|---|---|---|---|---|---|---|
| 3-Day MP | DXM | p-Value | 3-Day MP | DXM | p-Value | |
| PaO2/FiO2 | 271.4 (206–323.6) | 304.8 (242.9–345.7) | <0.001 | 271.4 (206–323.6) | 290.6 (222.1–338.1) | 0.107 |
| Lymphocytes × 106/L, median (IQR) | 820 (600–1090) | 880 (630–1220) | 0.026 | 820 (600–1090) | 880 (630–1190) | 0.081 |
| CRP mg/L, median (IQR) | 126.4 (69.8–222.1) | 97.5 (56.1–162.8) | <0.001 | 126.4 (69.8–222.1) | 106 (64.7–177) | 0.039 |
| LDH U/L, median (IQR) | 393 (308.5–481) | 339 (266.5–438.8) | <0.001 | 393 (308.5–481) | 371 (282–459) | 0.052 |
| Ferritin mcg/L, median (IQR) | 1440 (712.3–2110.8) | 958.5 (454.9–1736.7) | <0.001 | 1440 (712.3–2110.8) | 1217.2 (573–1862.7) | 0.083 |
| D-dimer ng/mL, median (IQR) | 414 (250–828.5) | 339 (250–651.5) | 0.016 | 414 (250–828.5) | 388 (250–804) | 0.246 |
| Whole Cohort | Matched Sample | |||||
|---|---|---|---|---|---|---|
| 3-Day MP | DXM | p-Value | 3-Day MP | DXM | p-Value | |
| Remdesivir | 3 (1.6) | 177 (35.9) | <0.001 | 3 (1.6) | 8 (4) | 0.222 |
| Tocilizumab | 110 (58.2) | 89 (18.1) | <0.001 | 110 (58.2) | 55 (27.6) | <0.001 |
| LMWH | <0.001 | 0.001 | ||||
| No Low doses Intermediate doses Full doses | 6 (3.2) 106 (56.1) 36 (19) 41 (21.7) | 53 (10.8) 288 (58.4) 96 (19.5) 56 (11.4) | 6 (3.2) 106 (56.1) 36 (19) 41 (21.7) | 18 (9) 111 (55.8) 51 (25.6) 19 (9.5) | ||
| Whole Cohort | Matched Sample | |||||
|---|---|---|---|---|---|---|
| 3-Day MP | DXM | p-Value | 3-Day MP | DXM | p-Value | |
| Primary outcome n (%) | ||||||
| In-hospital mortality | 59 (31.2) | 88 (17.8) | <0.001 | 59 (31.2) | 35 (7.1) | 0.002 |
| Secondary outcomes n (%) | ||||||
| HFNC | 65 (34.4) | 186 (37.7) | 0.419 | 65 (34.4) | 84 (42.2) | 0.113 |
| NIMV | 50 (26.5) | 121 (24.5) | 0.606 | 50 (26.5) | 50 (25.1) | 0.765 |
| IMV | 49 (25.9) | 68 (13.8) | <0.001 | 49 (25.9) | 29 (14.6) | 0.005 |
| ICU admission | 55 (29.1) | 101 (20.5) | 0.017 | 55 (29.1) | 37 (18.6) | 0.015 |
| Composite variable | 118 (62.4) | 225 (45.6) | <0.001 | 118 (62.4) | 100 (50.3) | 0.016 |
| Length of stay (days), median (IQR) | 14 (8–24.5) | 11 (7–18.5) | <0.001 | 14 (8–24.5) | 11 (7–19) | 0.001 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | |
| Age/year | 1.06 (1.04–1.09) | <0.001 | 1.08 (1.05–1.10) | <0.001 |
| Gender (female) | 1.04 (0.62–1.75) | 0.881 | NS | |
| BMI | 0.99 (0.95–1.04) | 0.76 | ||
| Smoking behaviour | NS | |||
| Never smoker | 1 ref. | |||
| Former smoker | 1.56 (0.94–2.61) | 0.088 | ||
| Current smoker | 2.38 (0.88–6.41) | 0.088 | ||
| Degree of dependency | ||||
| None or mild | 1 ref. | 1 ref. | ||
| Moderate | 2.29 (0.96–5.49) | 0.063 | 1.37 (0.50–3.77) | 0.544 |
| Severe | 12.47 (2.54–61.3) | 0.002 | 8.77 (1.51–51.08) | 0.016 |
| Arterial hypertension | 1.99 (1.23–3.20) | 0.005 | NS | |
| Dyslipidemia | 1.54 (0.97–2.45) | 0.071 | NS | |
| Diabetes mellitus | 1.71 (1.01–2.92) | 0.048 | NS | |
| Ischaemic cardiopathy | 0.92 (0.33–2.55) | 0.866 | ||
| Cerebrovascular disease | 0.89 (0.18–4.37) | 0.887 | ||
| Dementia | 4.26 (1.63–11.13) | 0.003 | NS | |
| Chronic heart failure | 2.01 (0.64–6.30) | 0.232 | ||
| Chronic liver disease | 0.78 (0.21–2.81) | 0.697 | ||
| Severe chronic renal failure | 1.82 (0.52–6.37) | 0.347 | ||
| Cancer | 2.88 (1.01–8.16) | 0.047 | NS | |
| COPD | 2.57 (1.09–6.08) | 0.031 | NS | |
| Asthma | 1.58 (0.28–8.75) | 0.603 | ||
| OSAS | 1.43 (0.60–3.40) | 0.422 | ||
| PaO2/FiO2 | 0.99 (0.99–0.99) | <0.001 | 0.99 (0.99–0.99) | <0.001 |
| Respiratory rate > 20 bpm | 1.84 (1.11–3.04) | 0.018 | NS | |
| Lymphocytes/× 106/L | 1.00 (1.00–1.00) | 0.66 | ||
| CRP/mg/L | 1.01 (1.01–1.01) | 0.001 | NS | |
| LDH/U/L | 1.01 (1.01–1.01) | <0.001 | 1.01 (1.01–1.01) | 0.012 |
| Ferritin/mcg/L | 1.01 (1.01–1.01) | 0.774 | ||
| D-dimer/ng/mL | 1.01 (1.01–1.01) | 0.101 | ||
| Corticosteroids | ||||
| DXM | 1 ref. | 1 ref. | ||
| 3-day MP | 2.13 (1.32–3.43) | 0.002 | 2.30 (1.33–3.98) | 0.003 |
| Remdesivir | 0.31 (0.04–2.42) | 0.261 | ||
| Tocilizumab | 0.95 (0.59–1.51) | 0.815 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mora-Luján, J.M.; Tuells, M.; Montero, A.; Formiga, F.; Homs, N.A.; Albà-Albalate, J.; Corbella, X.; Rubio-Rivas, M. High-Dose Methylprednisolone Pulses for 3 Days vs. Low-Dose Dexamethasone for 10 Days in Severe, Non-Critical COVID-19: A Retrospective Propensity Score Matched Analysis. J. Clin. Med. 2021, 10, 4465. https://doi.org/10.3390/jcm10194465
Mora-Luján JM, Tuells M, Montero A, Formiga F, Homs NA, Albà-Albalate J, Corbella X, Rubio-Rivas M. High-Dose Methylprednisolone Pulses for 3 Days vs. Low-Dose Dexamethasone for 10 Days in Severe, Non-Critical COVID-19: A Retrospective Propensity Score Matched Analysis. Journal of Clinical Medicine. 2021; 10(19):4465. https://doi.org/10.3390/jcm10194465
Chicago/Turabian StyleMora-Luján, José María, Manel Tuells, Abelardo Montero, Francesc Formiga, Narcís A. Homs, Joan Albà-Albalate, Xavier Corbella, and Manuel Rubio-Rivas. 2021. "High-Dose Methylprednisolone Pulses for 3 Days vs. Low-Dose Dexamethasone for 10 Days in Severe, Non-Critical COVID-19: A Retrospective Propensity Score Matched Analysis" Journal of Clinical Medicine 10, no. 19: 4465. https://doi.org/10.3390/jcm10194465