Recent Advances in Treatment of Coronary Artery Disease: Role of Science and Technology


Radiologic Sciences and Respiratory Therapy Division, School of Health and Rehabilitation Sciences, The Ohio State University College of Medicine, Columbus, OH 43210, USA
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2018, 19(2), 424; https://doi.org/10.3390/ijms19020424
Submission received: 10 November 2017
/
Revised: 6 January 2018
/
Accepted: 15 January 2018
/
Published: 31 January 2018
(This article belongs to the Special Issue Ischemic Heart Disease: From Bench to Bedside)
Abstract
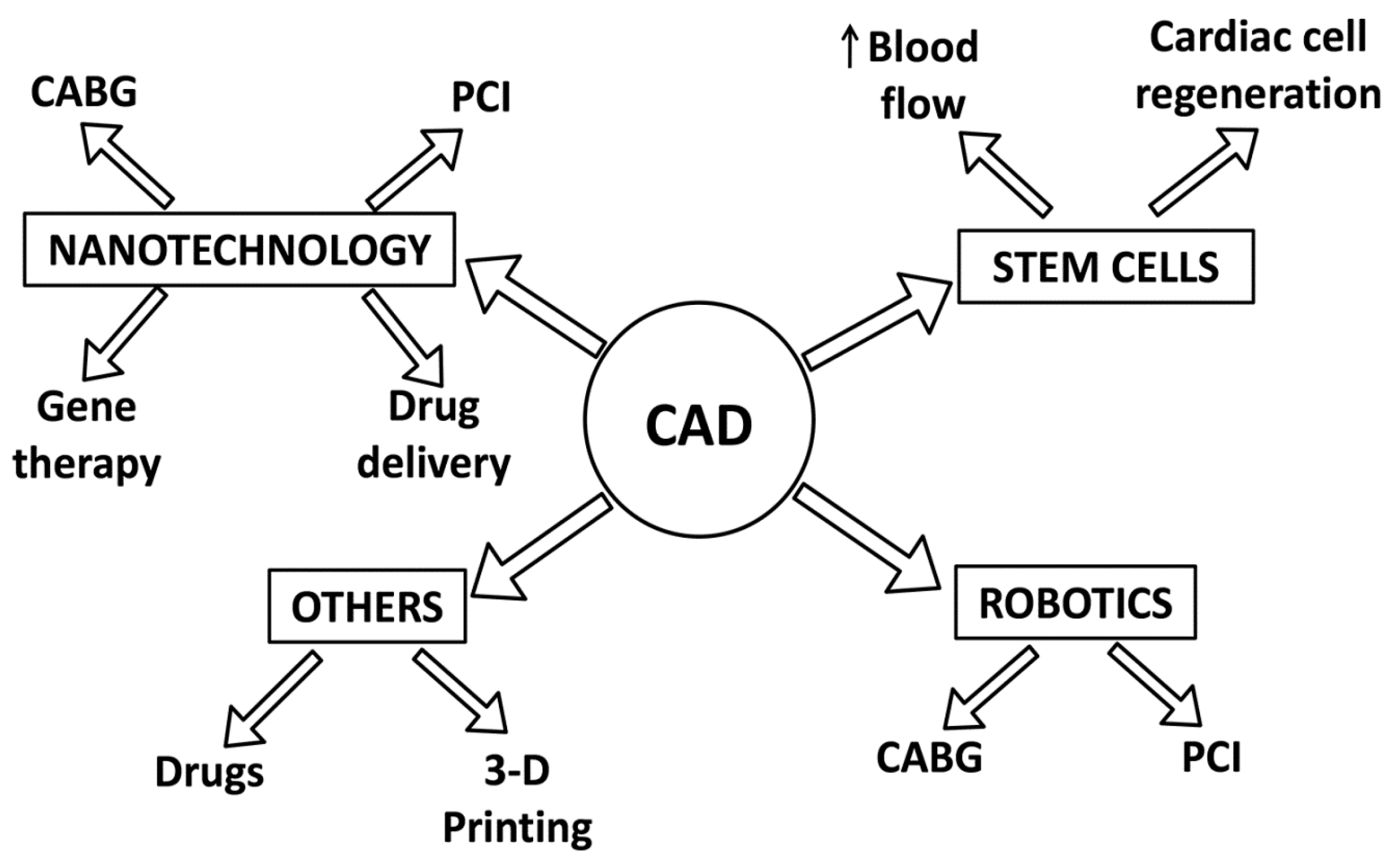
:Coronary artery disease (CAD) is one of the most common causes of death worldwide. In the last decade, significant advancements in CAD treatment have been made. The existing treatment is medical, surgical or a combination of both depending on the extent, severity and clinical presentation of CAD. The collaboration between different science disciplines such as biotechnology and tissue engineering has led to the development of novel therapeutic strategies such as stem cells, nanotechnology, robotic surgery and other advancements (3-D printing and drugs). These treatment modalities show promising effects in managing CAD and associated conditions. Research on stem cells focuses on studying the potential for cardiac regeneration, while nanotechnology research investigates nano-drug delivery and percutaneous coronary interventions including stent modifications and coatings. This article aims to provide an update on the literature (in vitro, translational, animal and clinical) related to these novel strategies and to elucidate the rationale behind their potential treatment of CAD. Through the extensive and continued efforts of researchers and clinicians worldwide, these novel strategies hold the promise to be effective alternatives to existing treatment modalities.
1. Introduction
The scientific advancements in the understanding of the pathophysiology of coronary artery disease (CAD) have led to a decrease in the mortality (in age-adjusted subjects) towards the turn of the 20th century [1]. However, CAD remains one of the leading cause of death in the world [2]. CAD is responsible for one-third of deaths in developing and developed countries in people over 35 years of age, with the percentage reaching close to 50% (according to some estimates) in western countries [3,4]. The worldwide burden is set to reach 47 million disability adjusted life years (years lost due to disability, ill-health or death) by the year 2020 as projected by World Health Organization [5]. In the United States alone, there are estimated to be 900,000 subjects who suffeedr or die from CAD and its complications in 2016 [6].
There has been a greater focus in research aimed at all aspects of CAD in the last decade. Due to exhaustive efforts from clinicians and researchers worldwide, there has been significant progress made in developing novel strategies for patients suffering from CAD and its associated complications. These strategies have ranged from drugs to robotic surgery to nanotechnology. This article will summarize the literature on the recent advances in coronary artery disease research in respect to therapeutics and biomarkers. This article will cover topics under the following headings: robotic surgery, nanotechnology, stem cells and other related advancements.
2. Robotics
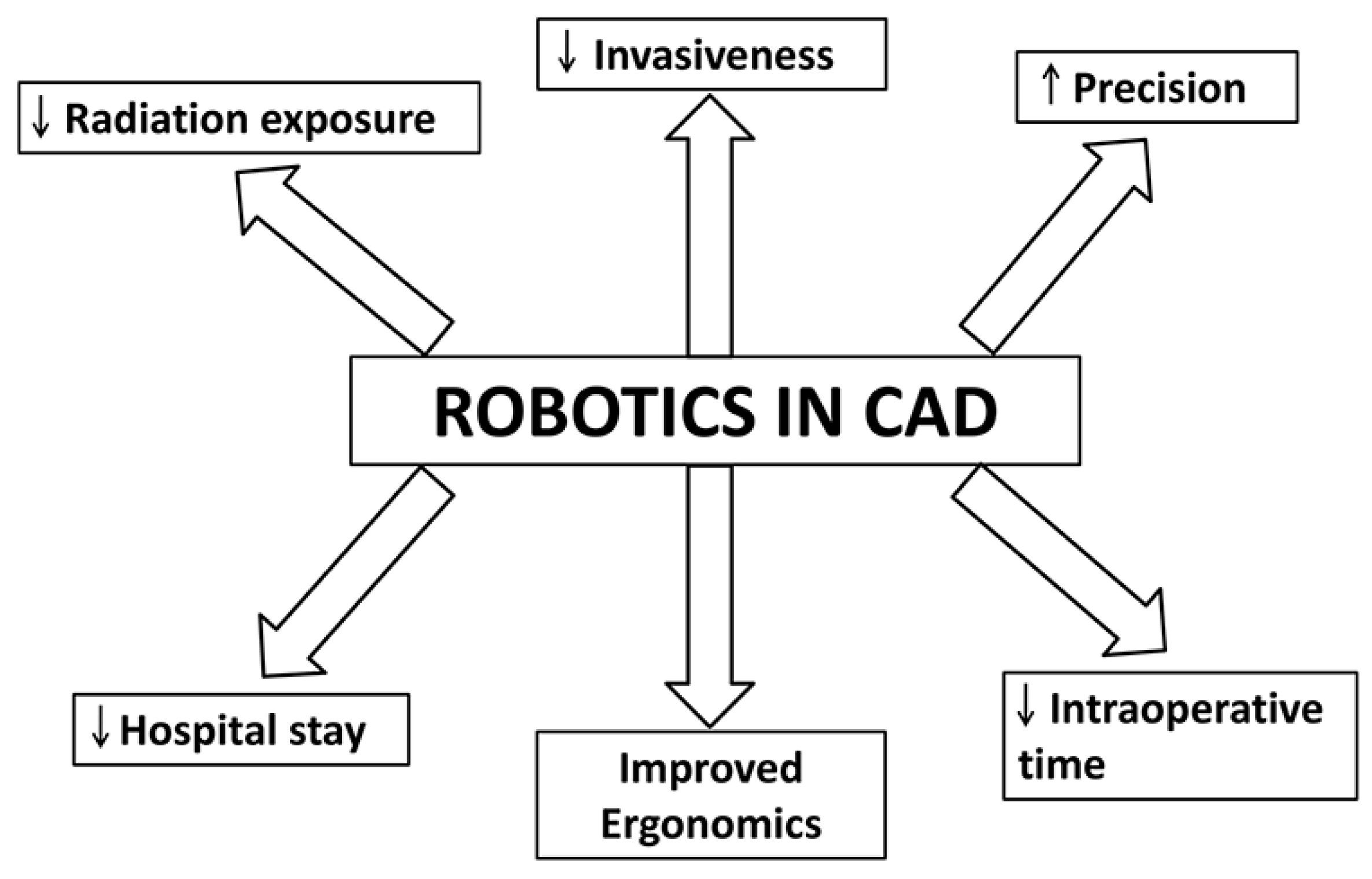
Robots have been in place in mass production industries for many years. However, their introduction in medicine was fairly recent and started in the fields of surgery and radiotherapy. In cardiology, they have been in use for more than a decade for surgeries like mitral valve repair, coronary artery bypass graft and septal defect closure. The technology is fast evolving with reports emerging about their potential applications in percutaneous coronary intervention (Figure 1) and atrial fibrillation ablation [7]. Robotics provide the operator with advantages such as improved ergonomics, precision and sometimes shortening of intraoperative time (Figure 2) [7]. There have been reports that robot-assisted surgery can shorten patient hospital stay and improve patient perception (Figure 2) [8].
In the field of interventional cardiology, robotics are being used for catheter-based surgical procedures. Conventional angiography radiation exposure for CAD patients is estimated at 7 mSV, and this exposure can be increased by up to 5 times in complicated surgeries [9]. Robotic guided surgery has potential to limit this radiation exposure. In addition, they can also reduce contrast induced nephrotoxicity and associated mortality in patients (Figure 2) [9]. In terms of patient related outcomes, the robotic assisted surgery has potential benefits as it can accurately measure the size of the lesions (which can be miscalculated using 2D angiography) which could improve long-term health. Hence, they reduce radiation exposure for the surgeon and the patient as well as improve precision by rendering accurate measurements of lesions (Figure 2) [7]. Granada et al. published the first robotic interventions for cardiac patients [10]. They performed coronary angioplasty and reported 100% success rate (measured in terms of less than 30% residual stenosis along with the absence of major cardiac complications) in all of their patients (80 subjects) [10]. In a multicenter study published by Weisz et al., a percutaneous coronary intervention was performed for patients with coronary artery disease [11]. They used similar success criteria (measured in terms of less than 30% residual stenosis along with absence of major cardiac complications) and reported a 97.6% rate of success (164 patients) [11]. They also reported a significant reduction (95%) in operator radiation exposure [11].
Robotics has also been used to perform coronary artery bypass grafting in CAD patients (Figure 1). The procedure, including the harvesting of the mammary arteries and anastomosis, can be performed endoscopically [7]. The results of the clinical studies are summarized in Table 1. Although there are reported benefits for robotically assisted bypass grafting, high costs and long learning curves have slowed down its progress towards becoming used routinely [12]. Robotically assisted hybrid coronary revascularization, which involves coronary artery bypass graft as well as percutaneous coronary intervention, has also been developed as a treatment modality for CAD. There have been reported benefits such as reduced morbidity and shortened hospital stays due to the minimally invasive nature of the procedure [13,14,15,16].
The current state of robotic surgery is promising in the treatment of CAD. These systems are of excellent quality with high-end technology. Their proposed benefits in the form of improved precision, increased visibility, improved ergonomics and reduced radiation exposure have been documented, which have translated into improved patient recovery times with reduced hospital stays [7,20,21]. They also provide a distinct advantage for procedures that are difficult to be performed using endoscopy or catheters [7]. However, their translation into full-fledged clinical usage is inhibited by high cost and the learning curve needed to master these procedures [22]. It remains to be determined, with further technological advancement, whether this technology will be accepted into routine clinical practice and replace conventional technologies.
3. Nanotechnology
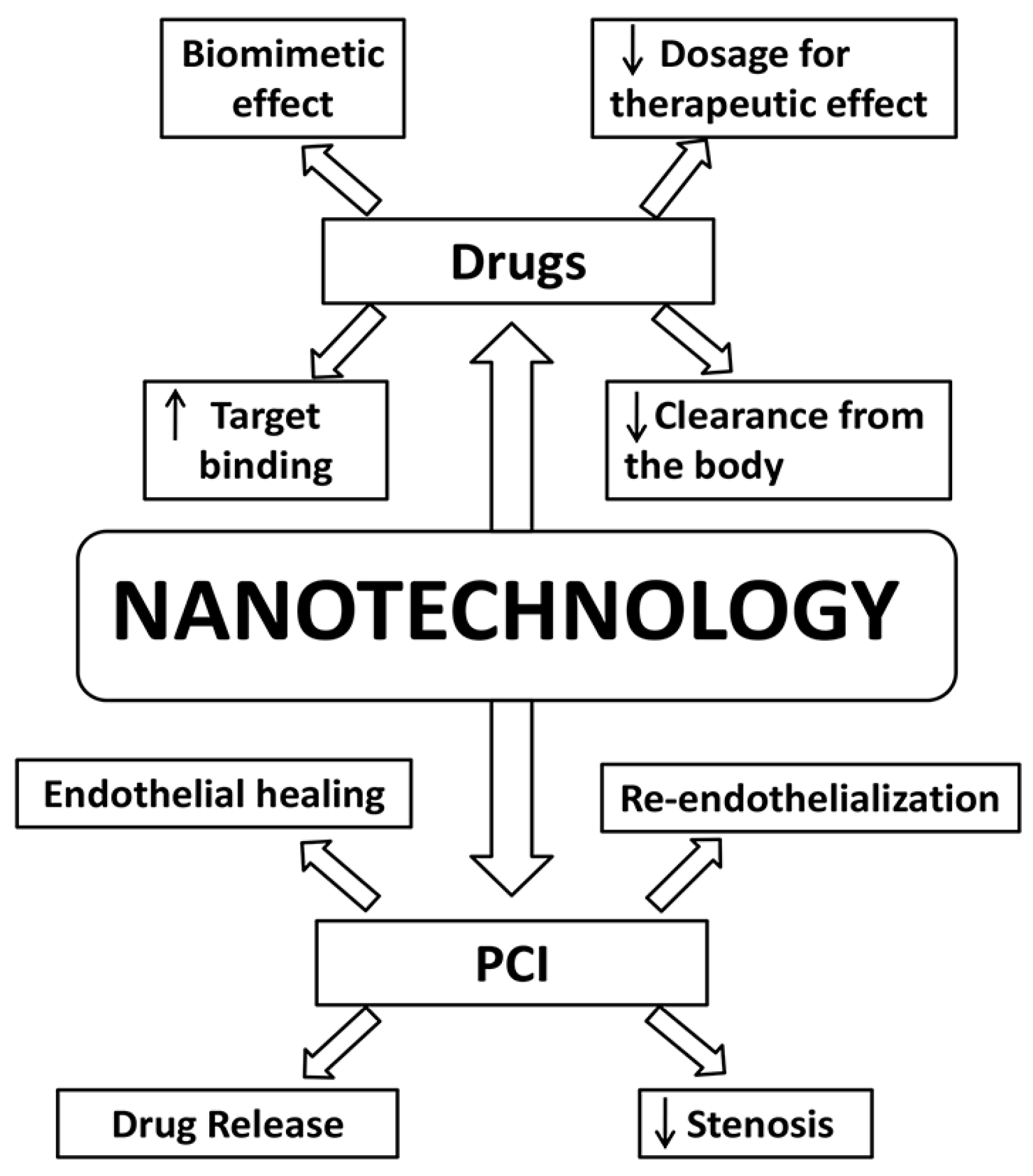
Nanotechnology has been revolutionizing several fields including medicine. It involves the engineering of nanoscale molecules with distinctly different properties than bulk molecules of the same composition. These inherent differences provide distinct benefits which are strong reasons for the boom in nanotechnology research. This technology has been studied in CAD for its potential benefits in medical (non-invasive) and invasive treatment modalities, drug delivery applications, percutaneous coronary interventions, gene therapy, and coronary artery bypass graft (Figure 1).
Cholesterol is an important factor involved in the pathogenesis of coronary artery disease. High levels of low-density lipoproteins (LDL) are implicated in coronary artery disease whereas high-density lipoproteins (HDL) are thought to have a protective role since they are involved in transportation of cholesterol away from the peripheral tissues. Nanotechnology has been used in the synthesis of a dimyristoyl phosphatidylcholine, which mimics the surface characteristics of HDL (Figure 3) by mediating the removal of cholesterol from the peripheral tissues and transport it to the liver. In an animal model study, mice fed with a cholesterol-rich diet showed significantly lower plaque volume and cholesterol content in the aorta when treated with dimyristoyl phosphatidylcholine liposomes [23]. Fumagillin is an anti-angiogenic drug that has been shown to inhibit angiogenesis thereby promoting plaque regression in coronary arteries. One of the disadvantages that has prevented Fumagillin application is its ability to cause adverse neurocognitive effects at high doses, which is required to achieve a therapeutic effect. Winter et al. demonstrated that the Fumagillin can be delivered through αvβ3 integrin targeted nano-delivery system, and is able to achieve significant antiplaque effects at one-third of the usual dose (Figure 3) [24]. Several nanoparticle-based antithrombotic agents have been tested for their potency. d-phenylalanyl-l-prolyl-Larginyl-chloromethyl ketone is a potent antithrombotic agent that is rapidly cleared from the body, thus limiting its clinical use [25]. When combined with a perfluorocarbon-core nanoparticle, it has been shown to have improved antithrombotic action, as shown by Myerson et al. in an animal model study (Figure 3) [26]. Peters et al. on the other hand used hirudin with fibrin binding micellar nanoparticles which exhibited greater targeting of fibrin clots in vivo (Figure 3) [27]. Collagen IV nanoparticles have been tried in an animal model study and were shown to improve collagen formation while reducing oxidative stress by mimicking Annexin A1 (glucocorticoid regulatory protein) [28].
The studied modifications were in the form of liposomal glucocorticoid carrier (to deliver anti-inflammatory hormones thereby reducing arterial wall inflammation), lipid nanoparticles (to deliver siRNA antagonistic to the C-C chemokine type 2 pro-inflammatory receptor), and HDL nanoparticles (to deliver simvastatin to inhibit monocyte recruitments) [29,30,31]. Gel-based nanoparticles combined with rapamycin (antiproliferative and antiapoptotic effect) were studied in an animal model, which were found to re-endothelialize injured arteries and reduce hyperplasia [32]. Smart nanoparticles such as a pH-dependent delivery of antioxidants as developed by Tang et al. has shown promise in treating cardiac diseases [33].
Nanotechnology has shown potential benefits when used in percutaneous coronary intervention. They have been studied for their ability to release drugs as well as promote healing and reduce restenosis (Figure 3) [25]. Nano-sized hydroxyapatite coating for controlled release of sirolimus (an immunosuppressive drug) performed satisfactorily in clinical trials [34]. Similarly, the release of sirolimus was studied using carbon nanoparticle coated stents with consistent drug release, as reported in an in-vitro study [35]. The sirolimus-releasing stents were compared with pitavastatin nanoparticle-eluting stents. The latter were found to be more efficient in terms of faster endothelial healing while being comparable in other parameters (Figure 3) [36]. Magnetic silica nanoparticles were loaded with rapamycin, coated onto the stent and exhibited rapid endothelialization in in vivo studies [37]. Endothelial healing and re-endothelialization help to restore the injured vessel back to health. Polycaprolactone was found to be an effective carrier for nitric oxide to prevent restenosis (Figure 3) [38]. In animal model studies, it has been proven that liposome encapsulated alendronate (a bisphosphonate) can reduce restenosis and neointimal formations (Figure 3) [39]. Similarly, paclitaxel (antimitotic drug) in the form of albumin-based nanoparticles have shown to have significant antiproliferative and restenosis effects without significant toxicity even when administered systemically [40,41]. The nanoparticles in these cases were either used to improve cell membrane permeability (alendronate) or binding capacity to the targeted tissues (paclitaxel) [42]. Polymeric stent coatings in the form of poly(lactic-co-glycolic acid) were proven to have a controlled release of the drug paclitaxel (nanocoatings-64) and polyethylene glycol was proven to reduce platelet adhesion [38,43]. Nanomodifications have also helped scientists in targeting specific delivery of medications such as collagen IV, chondroitin sulfate, tissue factor, or stents [44,45,46,47].
Nanotechnology has the potential to promote healing by inducing endothelialization of the stent (Figure 3) [25]. These nano-modifications have been in the form of nanofibrous matrix (attracts endothelial cells), polyhedral oligomericsilsesquioxanepoly-(carbonate-urea) urethane (improved adherence and proliferation of human endothelial cells), peptide amphiphile-nanofiber coating (for promotion of endothelial cell adhesion), and magnetic nanoparticles (for preferential movement of cells towards the stent) [48,49,50,51]. Nanotechnology also has potential applications in finding synthetic alternatives for coronary artery bypass grafts. Researchers have studied the potential of electrospunnanosized fibrous scaffolds, which may prove to be an alternative synthetic graft for coronary artery bypass graft procedures [52,53]. Targeting drug-eluting stents in gene therapy is another area where nanotechnology holds promise. Gene eluting stents can be used to overcome restenosis, in-stent thrombosis, and delayed endothelialisation [54,55]. Several nano-coatings in the form of hyaluronic acid (to carry pDNA), nanobiohybrid hydrogel (to carry Tat peptide and DNA), and poly(lactic-co-glycolic acid) nanoparticles (carrying PDGF receptor-β antisense RNA) have been studied in animal models and have shown promising results [56,57,58]. Other gene targets that have been studied extensively include antisense oligonucleotide, chitosan-plasmid DNA, Akt1 siRNA, vascular endothelial growth factor, prostacyclin synthase, and endothelial nitric oxide synthase [54].
Nanotechnology has led to an interesting and promising direction in the treatment of CAD. It has valuable potential in delivering drugs that are otherwise limited by their pharmacokinetics. Its applications in stent and gene therapy are potentially useful for future therapeutics based on these modalities. Further randomized controlled trials need to be conducted to establish strong evidence to support the use of these newer technologies for CAD treatments. This needs to be carried out with strong collaboration between researchers, engineers, biomedical engineers, nanotechnologists and clinicians. As the technology and evidence develops, we will soon enter an era where existing established treatment modalities could be questioned and eventually replaced by nanotherapeutics.
4. Stem Cells
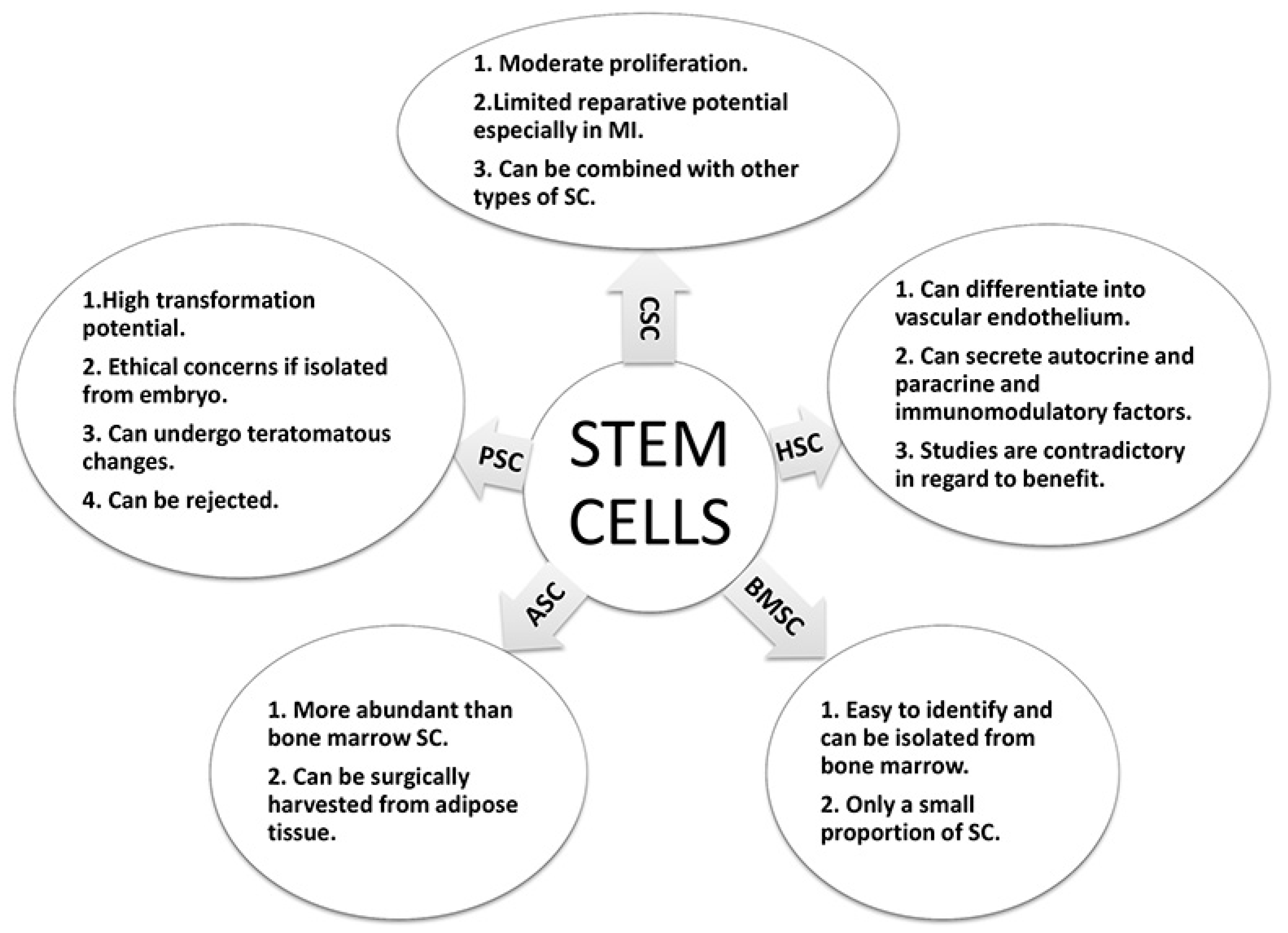
Research in cardiovascular disease has sought to repair myocardial damage and increase blood supply in ischemic conditions of the heart, thereby reversing the effects of CAD. In this respect, both vascular growth factors and stem cells have generated a lot of interest as a mode of treatment in patients with CAD [59]. The rationale behind such therapy is to improve the blood supply to ischemic areas of the heart by stem cells, as well as promote cardiac cell regeneration (Figure 1). This can be achieved in one of two ways: by a direct effect of the stem cells, or by paracrine factors secreted by these stem cells [60]. In this regard, hematopoietic stem cells have been of great interest, especially for mononuclear cells and endothelial progenitor cells (Figure 4). Studies conducted using these cells for various forms of ischemic heart disease (such as acute myocardial infarction (MI) and chronic ischemic heart disease) have been contradictory, although some studies have demonstrated a beneficial effect in such patients [61,62,63,64]. This has led to the inclusion of other types of stem cells, such as adipose derived stem cells, into such studies. A novel alternative is the creation of induced pluripotent stem cells, for which adult cells are transformed into pluripotent stem cells, similar to embryonic stem cells [65,66]. Although it offers a promising alternative, concerns of cancerous transformation of the undifferentiated stem cells have to be taken into account before they can be tried in human subjects.
The stem cells studied in cardiovascular research ranged from bone marrow to adipose tissue to skeletal muscle stem cells. Bone marrow-derived mononuclear cells are the most readily available cells for transplantation in the body. They are easy to identify based on their cell surface markers and can be isolated from the bone marrow [60]. However, their therapeutic potential is low since the harvested cells contain a multitude of cells with a small proportion of stem cells (Figure 4) [63,67]. The bone marrow-derived mesenchymal stem cells are found in even lower concentrations than that of mononuclear cells thus requiring several weeks of maturation with different growth factors in the lab prior to clinical usage. The adipose derived stem cells can be surgically harvested from adipose tissues. They are more abundant in comparison to the bone marrow-derived cells. This drastically reduces the time and cost involved in laboratory procedures to culture them for clinical use (Figure 4) [68]. The pluripotent stem cells have a high potential for transformation. Although embryos represent the most obvious source of stem cells, their use has ethical concerns and is in debate. Additionally, these cells could potentially face rejection when transplanted to a recipient. However, it is possible to reprogram adult cells and transform them into pluripotent cells (similar properties as embryonic stem cells), thereby being called induced pluripotent stem cells. These cells can be auto-transplanted and therefore would not be rejected. However, due to their transformation potential, unless closely regulated, they can undergo teratomatous (derived from all three germ layers) changes in the body (Figure 4) [65,69]. Due to the risk of teratomatous changes, this area of research requires more work before they can be considered safe for human trials. Another interesting source of stem cells are cardiac stem cells. Although the heart was considered as a static organ (with little or no potential to undergo mitosis during adulthood) [70,71,72], recent evidence has shown a different perspective. The heart is now believed to have intrinsic regenerative potential and undergoes constant turnover throughout adult life (Figure 4) [73]. Beltrami et al. showed that the heart possesses cardiac stem cells that could be responsible for the intrinsic regeneration and turnover throughout adult life [70]. These cells are more numerous in the apices of the atrium and ventricles [74]. Although these cells are known to be involved in tissue homeostasis, their reparative potential is limited, especially in conditions with extensive damage such as myocardial infarction (MI) [72,75,76,77]. More recently, there has been an interest to develop and inject multiple stem cells that can communicate with each other, termed as a “Cardiocluster”. These clusters are cocktails of cells that include cardiac progenitor cells, mesenchymal stem cells, endothelial progenitor cells and fibroblasts (Figure 4). They have the potential to promote cardiac cell regeneration in disease states where cell function is reduced such as CAD [78].
The clinical data for stem cell therapy is in its early days with reported literature covering both non-randomized and randomized trials. One non-randomized trial reported improved left ventricular ejection fraction (LVEF) function following injection of mononuclear stem cells in patients with MI within three months [79]. Improved exercise capacity, reduced mortality and scar tissue are shown in a 5-year follow up [80]. Several other studies showed similar effects following treatments with mononuclear stem cells after MI [64,81,82,83]. An earlier meta-analysis reported an improvement in LVEF function by 2.99% following bone marrow stem cell transplantation in patients after MI [84]. However, the meta-analysis did not include recent studies that reported no improvement in left ventricular function [61,62]. In patients suffering from chronic ischemic heart disease, there is reported evidence towards improved cardiac function following the use of bone marrow derived-stem cells [85,86,87,88]. There have been several trials that have studied the clinical efficacy of mesenchymal stem cells. They have reported an improvement in cardiac function and relative safety in the use of mesenchymal stem cells [89,90,91,92]. Cardiac derived stem cells have also undergone clinical testing and have shown promising results [93,94,95]. They reported an improvement in LVEF [93], an improvement in the left ventricular mass that was viable [94], improved quality of life [93], reduced scar mass, improved regional contractility [95] and safety of the procedure [93,94]. Interestingly, a patient that was treated with cardiac stem cells 14 months after MI had similar therapeutic benefit as someone treated earlier, suggesting that cardiac stem cells could be beneficial in chronic ischemia patients [96]. However, it should be noted that the observed clinical benefit was less than the expected clinical benefit based on prior in vitro and animal studies [97] (for a more in-depth review on this topic, the reader can refer to Kastrup [60], Quijada and Sussman [98] and Dixit and Katare [99]).
Stem cell therapy continues to be a promising treatment modality for coronary artery disease (both acute and chronic). The experimental and clinical studies have shown promising results. However, further research is needed to understand the exact mechanisms of action and the ideal source of stem cells to derive optimum benefit and to further our understanding. Several challenges have to be overcome (such as long term safety and route of administration), but the direction of current research looks promising.
5. Other Advancements
5.1. 3-D Printing
Cardiac conditions often require 3-D imaging such as magnetic resonance imaging, computerized tomography, and 3-D echography to diagnose and treat these conditions. The limitations to this are that though these images are in 3-D, they are viewed on a 2-D computer screen or films. Although it could be sufficient for some cardiac procedures, the current imaging modalities are not effective for more complex interventions [100,101]. 3-D printing has a potential role in CAD (Figure 1) as it cannot only overcome these limitations but also allow for complete visualization, tactile sense, education and surgical planning as well as simulation [102]. 3-D printing involves additive manufacturing of a model using 3-D data from imaging modalities. Scientists are starting to see the full potential of 3-D printing as the technology continues to evolve. In the field of cardiology it has tremendous potential in the treatment of congenital defects, cardiac tumors, cardiomyopathy, functional flow models, valvular heart diseases, stent placement for CAD and other cardiac surgeries [103,104,105,106]. 3-D printing allows the visualization of 3-D printed heart with coronary arteries in order to visualize the extent of occlusion and stenosis in CAD patients [107]. These models can be used in a pulsatile flow loop environment, not only to visualize and understand complex flow patterns but also to simulate interventions [105]. 3-D printed models are also useful in CAD research to compare imaging and treatment modalities [105,108]. One in vitro study mimicking a clinical scenario proved that 3-D printing could be more effective in planning and treating complex situations (bifurcation lesions) that require stent placement [106]. Tissue engineering models are now being tested to fabricate stem cells along with extracellular matrix (tissue printing) for implantation in the body [109]. In vitro studies have been successful in tissue printing cardiac cells in different scaffolds [109,110]. In animal model studies, the implantation of printed tissue in epicardial tissues showed beneficial effects including reduced adverse remodeling and improved perfusion in myocardial infarct models [109,110].
5.2. Drugs
CAD patients are often on supportive, therapeutic, and lifelong medication for the condition itself and co-morbidities (such as hypercholesterolemia). There have been recent advances in drug developments for CAD patients (Figure 1). One class of drugs taken by patients suffering from CAD are oral antithrombotic medications such as aspirin and clopidogrel. A few years ago a group of drugs collectively termed as novel oral anti-coagulants were discovered. This group consists of the following drugs: ximelagatran, darexaban, dabigatran, rivaroxaban, and apixaban [111]. Of which, dabigatran, edoxaban, rivaroxaban, apixaban are approved for clinical use. Dabigatran is a competitive inhibitor of thrombin while edoxaban, rivaroxaban, and apixaban are inhibitors of clotting factor Xa. Use of dabigatran in CAD patients was studied in a phase 2 trial. The results revealed that ischemic events in patients were significantly reduced at higher doses of the drug (110 and 150 mg), but this benefit was counteracted with a four-fold increase in bleeding risk. However, the trials concluded that lower dose therapy could be used without a significant increase in bleeding risk [112].
An important protein that controls the regulation of LDL is proprotein convertase subtilisin/kexin type 9 (PCSK9) [113,114,115]. They function to reduce the number of LDL receptors thereby decreasing LDL cholesterol levels in the blood [115]. Another important drug which could block the action of PCSK9 is Alirocumab. The drug itself is a monoclonal antibody produced by recombinant DNA technology [114]. The first studies reported a reduction in LDL cholesterol levels ranging from 28% to 65% depending on the route of administration (subcutaneous or intravenous) [116]. In phase II studies (randomized controlled double blinded trials) it was reported that LDL cholesterol reduction ranged from 18.2% to 67% (depending on the dosage) compared to placebo [116,117]. When combined with atorvastatin, Alirocumab brought about a LDL cholesterol reduction of 66–73% whereas placebo and atorvastatin brought about a reduction of 17% [118]. These results were confirmed in several phase III trials [119,120,121,122,123,124,125,126,127,128,129,130]. Since high LDL levels are linked to CAD, the use of Alirocumab reduced adverse cardiovascular events by 15–48% [127,131,132]. Another drug that was recently developed for the treatment of heart failure is the angiotensin receptor-neprilysin inhibitor (ARNi). This drug contains a combination of sacubitril and valsartan, commonly referred to as the LCZ696 or ARNi [133,134]. The valsartan portion is a drug of the angiotensin receptor blocker family as well as angiotensin II receptor antagonist, while the sacubitril component is neprilysin inhibitor [135]. This drug has proven to be more effective in the treatment of heart failure than traditional Angiotensin-converting enzyme (ACE) inhibitors [136]. Although initial trials are promising, the results of phase III clinical trials are being awaited [136,137,138,139,140]
6. Conclusions
Despite great progress in cardiovascular research, CAD remains one of the most common causes of morbidity and mortality worldwide. However, significant inter-collaborative efforts between researchers, clinicians and other related professionals have led to multi-faceted and novel strategies to be developed to treat CAD and its associated conditions. Though some of these strategies have strong evidence supporting their clinical use, some others are still in the experimental stage. Despite only early evidence being available on some of these novel treatment modalities, the results are promising and hold the potential to become alternatives to current treatment options in the future. Since we live in the era of evidence-based medicine, further evidence in the form of clinical trials and long term follow up studies are required before these novel treatment strategies enter into mainstream practice. With sustained continued efforts, the future for CAD therapeutics looks substantially promising.
Acknowledgments
We thank Chia-Chen Chuang, Mykola Stetskiv, James Meade, Alicia Simpson and Evan Prather for their assistance during the manuscript preparation.
Author Contributions
Eswar Kandaswamy and Li Zuo wrote, edit and approve the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ACE | Angio-tensin-converting enzyme |
| ARNi | Angiotensin receptor-neprilysin inhibitor |
| CAD | Coronary artery disease |
| CABG | Coronary artery bypass graft |
| HDL | High-density lipoprotein |
| LCZ696 | Combination of sacubitril and valsartan |
| LVEF | Left ventricular ejection fraction |
| LDL | Low-density lipoprotein |
| MI | Acute myocardial infarction |
| PCI | Percutaneous coronary intervention |
| PCSK9 | Proprotein convertase subtilisin/kexin type 9 |
| TECAB | Totally endoscopic coronary bypass surgery |
References
- Ford, E.S.; Ajani, U.A.; Croft, J.B.; Critchley, J.A.; Labarthe, D.R.; Kottke, T.E.; Giles, W.H.; Capewell, S. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N. Engl. J. Med. 2007, 356, 2388–2398. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.; Adams, R.J.; Brown, T.M.; Carnethon, M.; Dai, S.; de Simone, G.; Ferguson, T.B.; Ford, E.; Furie, K.; Gillespie, C.; et al. Executive summary: Heart disease and stroke statistics 2010 update: A report from the American Heart Association. Circulation 2010, 121, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Nichols, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe 2014: Epidemiological update. Eur. Heart J. 2014, 35, 2950–2959. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Srivastava, S.; Velmurugan, M. Newer perspectives of coronary artery disease in young. World J. Cardiol. 2016, 8, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Writing Group Members; Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Despres, J.P.; et al. Heart disease and stroke statistics-2016 Update: A report from the American Heart Association. Circulation 2016, 133, e38. [Google Scholar] [CrossRef] [PubMed]
- Bonatti, J.; Vetrovec, G.; Riga, C.; Wazni, O.; Stadler, P. Robotic technology in cardiovascular medicine. Nat. Rev. Cardiol. 2014, 11, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Suri, R.M.; Antiel, R.M.; Burkhart, H.M.; Huebner, M.; Li, Z.; Eton, D.T.; Topilsky, T.; Sarano, M.E.; Schaff, H.V. Quality of life after early mitral valve repair using conventional and robotic approaches. Ann. Thorac. Surg. 2012, 93, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Weisz, G. Robotic-assisted angioplasty: Current status and future possibilities. Curr. Cardiol. Rep. 2012, 14, 642–646. [Google Scholar] [CrossRef] [PubMed]
- Granada, J.F.; Delgado, J.A.; Uribe, M.P.; Fernandez, A.; Blanco, G.; Leon, M.B.; Weisz, G. First-in-human evaluation of a novel robotic-assisted coronary angioplasty system. JACC Cardiovasc. Interv. 2011, 4, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Weisz, G.; Metzger, D.C.; Caputo, R.P.; Delgado, J.A.; Marshall, J.J.; Vetrovec, G.W.; Reisman, M.; Waksman, R.; Granada, J.F.; Novack, V.; et al. Safety and feasibility of robotic percutaneous coronary intervention: PRECISE (Percutaneous Robotically-Enhanced Coronary Intervention) Study. J. Am. Coll. Cardiol. 2013, 61, 1596–1600. [Google Scholar] [CrossRef] [PubMed]
- Kypson, A.P. Recent trends in minimally invasive cardiac surgery. Cardiology 2007, 107, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, M.C.; Vesely, M.R.; Lee, J.D.; Lehr, E.J.; Wehman, B.; Bonaros, N.; Schachner, T.; Friedrich, G.J.; Zimrin, D.A.; Bonatti, J.O. Robotically assisted hybrid coronary revascularization: Does sequence of intervention matter? Innovations 2013, 8, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.R.; Van Praet, F.; de Canniere, D.; Murphy, D.; Siwek, L.; Seshadri-Kreaden, U.; Friedrich, G.; Bonatti, J. Integrated coronary revascularization: Percutaneous coronary intervention plus robotic totally endoscopic coronary artery bypass. Circulation 2006, 114 (Suppl. 1), 473–476. [Google Scholar] [CrossRef] [PubMed]
- Reicher, B.; Poston, R.S.; Mehra, M.R.; Joshi, A.; Odonkor, P.; Kon, Z.; Reyes, P.A.; Zimrin, D.A. Simultaneous “hybrid” percutaneous coronary intervention and minimally invasive surgical bypass grafting: Feasibility, safety, and clinical outcomes. Am. Heart J. 2008, 155, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Fitchett, D.H.; Gupta, M.; Farkouh, M.E.; Verma, S. Cardiology Patient Page: Coronary artery revascularization in patients with diabetes mellitus. Circulation 2014, 130, e104–e106. [Google Scholar] [CrossRef] [PubMed]
- Dogan, S.; Aybek, T.; Andressen, E.; Byhahn, C.; Mierdl, S.; Westphal, K.; Matheis, G.; Moritz, A.; Wimmer-Greinecker, G. Totally endoscopic coronary artery bypass grafting on cardiopulmonary bypass with robotically enhanced telemanipulation: Report of forty-five cases. J. Thorac. Cardiovasc. Surg. 2002, 123, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Kappert, U.; Schneider, J.; Cichon, R.; Gulielmos, V.; Tugtekin, S.M.; Nicolai, J.; Matschke, K.; Schueler, S. Development of robotic enhanced endoscopic surgery for the treatment of coronary artery disease. Circulation 2001, 104 (Suppl. 1), 102–107. [Google Scholar] [CrossRef]
- Mohr, F.W.; Falk, V.; Diegeler, A.; Walther, T.; Gummert, J.F.; Bucerius, J.; Jacobs, S.; Autschbach, R. Computer-enhanced “robotic” cardiac surgery: Experience in 148 patients. J. Thorac. Cardiovasc. Surg. 2001, 121, 842–853. [Google Scholar] [CrossRef] [PubMed]
- Bonaros, N.; Schachner, T.; Wiedemann, D.; Oehlinger, A.; Ruetzler, E.; Feuchtner, G.; Kolbitsch, C.; Velik-Salchner, C.; Friedrich, G.; Pachinger, O.; et al. Quality of life improvement after robotically assisted coronary artery bypass grafting. Cardiology 2009, 114, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Mihaljevic, T.; Jarrett, C.M.; Gillinov, A.M.; Williams, S.J.; deVilliers, P.A.; Stewart, W.J.; Svensson, L.G.; Sabik, J.F., III; Blackstone, E.H. Robotic repair of posterior mitral valve prolapse versus conventional approaches: Potential realized. J. Thorac. Cardiovasc. Surg. 2011, 141, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Schachner, T.; Bonaros, N.; Wiedemann, D.; Weidinger, F.; Feuchtner, G.; Friedrich, G.; Laufer, G.; Bonatti, J. Training surgeons to perform robotically assisted totally endoscopic coronary surgery. Ann. Thorac. Surg. 2009, 88, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.H.; Park, J.R.; Nakamura, M.T.; Odintsov, B.M.; Wallig, M.A.; Chung, B.H. Synthetic dimyristoylphosphatidylcholine liposomes assimilating into high-density lipoprotein promote regression of atherosclerotic lesions in cholesterol-fed rabbits. Exp. Biol. Med. 2010, 235, 1194–1203. [Google Scholar] [CrossRef] [PubMed]
- Winter, P.M.; Neubauer, A.M.; Caruthers, S.D.; Harris, T.D.; Robertson, J.D.; Williams, T.A.; Schmieder, A.H.; Hu, G.; Allen, J.S.; Lacy, E.K.; et al. Endothelial alpha(v)beta3 integrin-targeted fumagillin nanoparticles inhibit angiogenesis in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Rhee, J.W.; Wu, J.C. Advances in nanotechnology for the management of coronary artery disease. Trends Cardiovasc. Med. 2013, 23, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Myerson, J.; He, L.; Lanza, G.; Tollefsen, D.; Wickline, S. Thrombin-inhibiting perfluorocarbon nanoparticles provide a novel strategy for the treatment and magnetic resonance imaging of acute thrombosis. J. Thromb. Haemost. 2011, 9, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Peters, D.; Kastantin, M.; Kotamraju, V.R.; Karmali, P.P.; Gujraty, K.; Tirrell, M.; Ruoslahti, E. Targeting atherosclerosis by using modular, multifunctional micelles. Proc. Natl. Acad. Sci. USA 2009, 106, 9815–9819. [Google Scholar] [CrossRef] [PubMed]
- Fredman, G.; Kamaly, N.; Spolitu, S.; Milton, J.; Ghorpade, D.; Chiasson, R.; Kuriakose, G.; Perretti, M.; Farokhzad, O.; Tabas, I. Targeted nanoparticles containing the proresolving peptide Ac2-26 protect against advanced atherosclerosis in hypercholesterolemic mice. Sci. Transl. Med. 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Leuschner, F.; Dutta, P.; Gorbatov, R.; Novobrantseva, T.I.; Donahoe, J.S.; Courties, G.; Lee, K.M.; Kim, J.I.; Markmann, J.F.; Marinelli, B.; et al. Therapeutic siRNA silencing in inflammatory monocytes in mice. Nat. Biotechnol. 2011, 29, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Lobatto, M.E.; Fayad, Z.A.; Silvera, S.; Vucic, E.; Calcagno, C.; Mani, V.; Dickson, S.D.; Nicolay, K.; Banciu, M.; Schiffelers, R.M.; et al. Multimodal clinical imaging to longitudinally assess a nanomedical anti-inflammatory treatment in experimental atherosclerosis. Mol. Pharm. 2010, 7, 2020–2029. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Lobatto, M.E.; Hassing, L.; van der Staay, S.; van Rijs, S.M.; Calcagno, C.; Braza, M.S.; Baxter, S.; Fay, F.; Sanchez-Gaytan, B.L.; et al. Inhibiting macrophage proliferation suppresses atherosclerotic plaque inflammation. Sci. Adv. 2015, 1. [Google Scholar] [CrossRef] [PubMed]
- Reddy, M.K.; Vasir, J.K.; Sahoo, S.K.; Jain, T.K.; Yallapu, M.M.; Labhasetwar, V. Inhibition of apoptosis through localized delivery of rapamycin-loaded nanoparticles prevented neointimal hyperplasia and reendothelialized injured artery. Circ. Cardiovasc. Interv. 2008, 1, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Amin, D.; Messersmith, P.B.; Anthony, J.E.; Prud’homme, R.K. Polymer directed self-assembly of pH-responsive antioxidant nanoparticles. Langmuir 2015, 31, 3612–3620. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.R., Jr.; Abizaid, A.; Costa, R.; Feres, F.; Tanajura, L.F.; Abizaid, A.; Maldonado, G.; Staico, R.; Siqueira, D.; Sousa, A.G.; et al. 1-year results of the hydroxyapatite polymer-free sirolimus-eluting stent for the treatment of single de novo coronary lesions: The VESTASYNC I trial. JACC Cardiovasc. Interv. 2009, 2, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Rajender, G.; Narayanan, N.G. Liquid chromatography-tandem mass spectrometry method for determination of Sirolimus coated drug eluting nano porous carbon stents. Biomed. Chromatogr. 2010, 24, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Tsukie, N.; Nakano, K.; Matoba, T.; Masuda, S.; Iwata, E.; Miyagawa, M.; Zhao, G.; Meng, W.; Kishimoto, J.; Sunagawa, K.; et al. Pitavastatin-incorporated nanoparticle-eluting stents attenuate in-stent stenosis without delayed endothelial healing effects in a porcine coronary artery model. J. Atheroscler. Thromb. 2013, 20, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Liong, M.; Li, Z.; Zink, J.I.; Tamanoi, F. Biocompatibility, biodistribution, and drug-delivery efficiency of mesoporous silica nanoparticles for cancer therapy in animals. Small 2010, 6, 1794–1805. [Google Scholar] [CrossRef] [PubMed]
- Acharya, G.; Lee, C.H.; Lee, Y. Optimization of cardiovascular stent against restenosis: Factorial design-based statistical analysis of polymer coating conditions. PLoS ONE 2012, 7, e43100. [Google Scholar] [CrossRef] [PubMed]
- Danenberg, H.D.; Golomb, G.; Groothuis, A.; Gao, J.; Epstein, H.; Swaminathan, R.V.; Seifert, P.; Edelman, E.R. Liposomal alendronate inhibits systemic innate immunity and reduces in-stent neointimal hyperplasia in rabbits. Circulation 2003, 108, 2798–2804. [Google Scholar] [CrossRef] [PubMed]
- Kolodgie, F.D.; John, M.; Khurana, C.; Farb, A.; Wilson, P.S.; Acampado, E.; Desai, N.; Soon-Shiong, P.; Virmani, R. Sustained reduction of in-stent neointimal growth with the use of a novel systemic nanoparticle paclitaxel. Circulation 2002, 106, 1195–1198. [Google Scholar] [CrossRef] [PubMed]
- Margolis, J.; McDonald, J.; Heuser, R.; Klinke, P.; Waksman, R.; Virmani, R.; Desai, N.; Hilton, D. Systemic nanoparticle paclitaxel (nab-paclitaxel) for in-stent restenosis I (SNAPIST-I): A first-in-human safety and dose-finding study. Clin. Cardiol. 2007, 30, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Stinchcombe, T.E. Nanoparticle albumin-bound paclitaxel: A novel Cremphor-EL-free formulation of paclitaxel. Nanomedicine 2007, 2, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Joo, J.R.; Nam, H.Y.; Nam, S.H.; Baek, I.; Park, J.S. Thermal process for enhancing mechanical strength of PLGA nanoparticle layers on coronary stents. Bull. Korean Chem. Soc. 2009, 30, 1985–1988. [Google Scholar]
- Chan, J.M.; Rhee, J.W.; Drum, C.L.; Bronson, R.T.; Golomb, G.; Langer, R.; Farokhzad, O.C. In vivo prevention of arterial restenosis with paclitaxel-encapsulated targeted lipid-polymeric nanoparticles. Proc. Natl. Acad. Sci. USA 2011, 108, 19347–19352. [Google Scholar] [CrossRef] [PubMed]
- Chorny, M.; Fishbein, I.; Yellen, B.B.; Alferiev, I.S.; Bakay, M.; Ganta, S.; Adamo, R.; Amiji, M.; Friedman, G.; Levy, R.J. Targeting stents with local delivery of paclitaxel-loaded magnetic nanoparticles using uniform fields. Proc. Natl. Acad. Sci. USA 2010, 107, 8346–8351. [Google Scholar] [CrossRef] [PubMed]
- Joner, M.; Morimoto, K.; Kasukawa, H.; Steigerwald, K.; Merl, S.; Nakazawa, G.; John, M.C.; Finn, A.V.; Acampado, E.; Kolodgie, F.D.; et al. Site-specific targeting of nanoparticle prednisolone reduces in-stent restenosis in a rabbit model of established atheroma. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Lanza, G.M.; Yu, X.; Winter, P.M.; Abendschein, D.R.; Karukstis, K.K.; Scott, M.J.; Chinen, L.K.; Fuhrhop, R.W.; Scherrer, D.E.; Wickline, S.A. Targeted antiproliferative drug delivery to vascular smooth muscle cells with a magnetic resonance imaging nanoparticle contrast agent: Implications for rational therapy of restenosis. Circulation 2002, 106, 2842–2847. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, R.; Darbyshire, A.; Evans, J.E.; You, Z.; Lu, J.; Seifalian, A.M. Polymeric coating of surface modified nitinol stent with POSS-nanocomposite polymer. Colloids Surf. B Biointerfaces 2011, 86, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, H.; Tekinay, A.B.; Guler, M.O. Selective adhesion and growth of vascular endothelial cells on bioactive peptide nanofiber functionalized stainless steel surface. Biomaterials 2011, 32, 8797–8805. [Google Scholar] [CrossRef] [PubMed]
- Kushwaha, M.; Anderson, J.M.; Bosworth, C.A.; Andukuri, A.; Minor, W.P.; Lancaster, J.R., Jr.; Anderson, P.G.; Brott, B.C.; Jun, H.W. A nitric oxide releasing, self assembled peptide amphiphile matrix that mimics native endothelium for coating implantable cardiovascular devices. Biomaterials 2010, 31, 1502–1508. [Google Scholar] [CrossRef] [PubMed]
- Polyak, B.; Fishbein, I.; Chorny, M.; Alferiev, I.; Williams, D.; Yellen, B.; Friedman, G.; Levy, R.J. High field gradient targeting of magnetic nanoparticle-loaded endothelial cells to the surfaces of steel stents. Proc. Natl. Acad. Sci. USA 2008, 105, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Hashi, C.K.; Zhu, Y.; Yang, G.Y.; Young, W.L.; Hsiao, B.S.; Wang, K.; Chu, B.; Li, S. Antithrombogenic property of bone marrow mesenchymal stem cells in nanofibrous vascular grafts. Proc. Natl. Acad. Sci. USA 2007, 104, 11915–11920. [Google Scholar] [CrossRef] [PubMed]
- Stankus, J.J.; Soletti, L.; Fujimoto, K.; Hong, Y.; Vorp, D.A.; Wagner, W.R. Fabrication of cell microintegrated blood vessel constructs through electrohydrodynamic atomization. Biomaterials 2007, 28, 2738–2746. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.X.; Yang, D.Z.; Wu, J.Z. Nanoparticle drug- and gene-eluting stents for the prevention and treatment of coronary restenosis. Theranostics 2014, 4, 175–200. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.; Zheng, Y.; Yin, T.; Tang, C.; Yu, Q.; Wang, G. Coronary drug-eluting stents: From design optimization to newer strategies. J. Biomed. Mater. Res. A 2014, 102, 1625–1640. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.G.; Lee, Y.; Park, T.G. Controlled gene-eluting metal stent fabricated by bio-inspired surface modification with hyaluronic acid and deposition of DNA/PEI polyplexes. Int. J. Pharm. 2010, 384, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Egashira, K.; Masuda, S.; Funakoshi, K.; Zhao, G.; Kimura, S.; Matoba, T.; Sueishi, K.; Endo, Y.; Kawashima, Y.; et al. Formulation of nanoparticle-eluting stents by a cationic electrodeposition coating technology: Efficient nano-drug delivery via bioabsorbable polymeric nanoparticle-eluting stents in porcine coronary arteries. JACC Cardiovasc. Interv. 2009, 2, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Paul, A.; Shao, W.; Shum-Tim, D.; Prakash, S. The attenuation of restenosis following arterial gene transfer using carbon nanotube coated stent incorporating TAT/DNA(Ang1+Vegf) nanoparticles. Biomaterials 2012, 33, 7655–7664. [Google Scholar] [CrossRef] [PubMed]
- Kastrup, J. Gene therapy and angiogenesis in patients with coronary artery disease. Expert Rev. Cardiovasc. Ther. 2010, 8, 1127–1138. [Google Scholar] [CrossRef] [PubMed]
- Kastrup, J. Stem cells therapy for cardiovascular repair in ischemic heart disease: How to predict and secure optimal outcome? EPMA J. 2011, 2, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Janssens, S.; Dubois, C.; Bogaert, J.; Theunissen, K.; Deroose, C.; Desmet, W.; Kalantzi, M.; Herbots, L.; Sinnaeve, P.; Dens, J.; et al. Autologous bone marrow-derived stem-cell transfer in patients with ST-segment elevation myocardial infarction: Double-blind, randomised controlled trial. Lancet 2006, 367, 113–121. [Google Scholar] [CrossRef]
- Lunde, K.; Solheim, S.; Aakhus, S.; Arnesen, H.; Abdelnoor, M.; Egeland, T.; Endresen, K.; Ilebekk, A.; Mangschau, A.; Fjeld, J.G.; et al. Intracoronary injection of mononuclear bone marrow cells in acute myocardial infarction. N. Engl. J. Med. 2006, 355, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Perin, E.C.; Dohmann, H.F.; Borojevic, R.; Silva, S.A.; Sousa, A.L.; Mesquita, C.T.; Rossi, M.I.; Carvalho, A.C.; Dutra, H.S.; Dohmann, H.J.; et al. Transendocardial, autologous bone marrow cell transplantation for severe, chronic ischemic heart failure. Circulation 2003, 107, 2294–2302. [Google Scholar] [CrossRef] [PubMed]
- Schachinger, V.; Erbs, S.; Elsasser, A.; Haberbosch, W.; Hambrecht, R.; Holschermann, H.; Yu, J.; Corti, R.; Mathey, D.G.; Hamm, C.W.; et al. Intracoronary bone marrow-derived progenitor cells in acute myocardial infarction. N. Engl. J. Med. 2006, 355, 1210–1221. [Google Scholar] [CrossRef] [PubMed]
- Gunaseeli, I.; Doss, M.X.; Antzelevitch, C.; Hescheler, J.; Sachinidis, A. Induced pluripotent stem cells as a model for accelerated patient- and disease-specific drug discovery. Curr. Med. Chem. 2010, 17, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piuzzi, N.S.; Chahla, J.; Jiandong, H.; Chughtai, M.; LaPrade, R.F.; Mont, M.A.; Muschler, G.F.; Pascual-Garrido, C. Analysis of cell therapies used in clinical trials for the treatment of osteonecrosis of the femoral head: A systematic review of the literature. J. Arthroplast. 2017, 32, 2612–2618. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.; Matsubara, Y.; Masuda, Y.; Togashi, K.; Ohno, T.; Tamura, T.; Toyoshima, Y.; Sugimachi, K.; Toyoda, M.; Marc, H.; et al. Characterization of adipose tissue-derived cells isolated with the Celution system. Cytotherapy 2008, 10, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Y.; Christophersen, N.S.; Hall, V.; Soulet, D.; Brundin, P. Critical issues of clinical human embryonic stem cell therapy for brain repair. Trends Neurosci. 2008, 31, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Beltrami, A.P.; Barlucchi, L.; Torella, D.; Baker, M.; Limana, F.; Chimenti, S.; Kasahara, H.; Rota, M.; Musso, E.; Urbanek, K.; et al. Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell 2003, 114, 763–776. [Google Scholar] [CrossRef]
- Ellison, G.M.; Waring, C.D.; Vicinanza, C.; Torella, D. Physiological cardiac remodelling in response to endurance exercise training: Cellular and molecular mechanisms. Heart 2012, 98, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.S.K.; Shueh, Y.Z.; Liu, Y.W.; Hsieh, P.C.H. Harnessing endogenous intra- and extra-cardiac stem cells for cardiac regeneration—Hope or hype? Drug Discov. Today Ther. Strateg. 2009, 6, 127–133. [Google Scholar] [CrossRef]
- Barile, L.; Messina, E.; Giacomello, A.; Marban, E. Endogenous cardiac stem cells. Prog. Cardiovasc. Dis. 2007, 50, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Leri, A. Human cardiac stem cells: The heart of a truth. Circulation 2009, 120, 2515–2518. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.R.; Barile, L.; Messina, E.; Marban, E. Stem cells in the heart: What’s the buzz all about?—Part 1: Preclinical considerations. Heart Rhythm 2008, 5, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Hatzistergos, K.E.; Quevedo, H.; Oskouei, B.N.; Hu, Q.; Feigenbaum, G.S.; Margitich, I.S.; Mazhari, R.; Boyle, A.J.; Zambrano, J.P.; Rodriguez, J.E.; et al. Bone marrow mesenchymal stem cells stimulate cardiac stem cell proliferation and differentiation. Circ. Res. 2010, 107, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Martins, J.; Ogorek, B.; Cappetta, D.; Matsuda, A.; Signore, S.; D’Amario, D.; Kostyla, J.; Steadman, E.; Ide-Iwata, N.; Sanada, F.; et al. Cardiomyogenesis in the developing heart is regulated by c-kit-positive cardiac stem cells. Circ. Res. 2012, 110, 701–715. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.; Sussman, M.A. Rejuvenating the senescent heart. Curr. Opin. Cardiol. 2015, 30, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Stamm, C.; Westphal, B.; Kleine, H.; Petzsch, M.; Kittner, C.; Klinge, H.; Schümichen, C.; Nienaber, C.; Freund, M.; Steinhoff, P.G. Autologous bone-marrow stem-cell transplantation for myocardial regeneration. Lancet 2003, 361, 45–46. [Google Scholar] [CrossRef]
- Yousef, M.; Schannwell, C.M.; Kostering, M.; Zeus, T.; Brehm, M.; Strauer, B.E. The BALANCE Study: Clinical benefit and long-term outcome after intracoronary autologous bone marrow cell transplantation in patients with acute myocardial infarction. J. Am. Coll. Cardiol. 2009, 53, 2262–2269. [Google Scholar] [CrossRef] [PubMed]
- Assmus, B.; Schachinger, V.; Teupe, C.; Britten, M.; Lehmann, R.; Dobert, N.; Grunwald, F.; Aicher, A.; Urbich, C.; Martin, H.; et al. Transplantation of progenitor cells and regeneration enhancement in acute myocardial infarction (TOPCARE-AMI). Circulation 2002, 106, 3009–3017. [Google Scholar] [CrossRef] [PubMed]
- Schachinger, V.; Assmus, B.; Britten, M.B.; Honold, J.; Lehmann, R.; Teupe, C.; Abolmaali, N.D.; Vogl, T.J.; Hofmann, W.K.; Martin, H.; et al. Transplantation of progenitor cells and regeneration enhancement in acute myocardial infarction: Final one-year results of the TOPCARE-AMI Trial. J. Am. Coll. Cardiol. 2004, 44, 1690–1699. [Google Scholar] [CrossRef] [PubMed]
- Schachinger, V.; Erbs, S.; Elsasser, A.; Haberbosch, W.; Hambrecht, R.; Holschermann, H.; Yu, J.; Corti, R.; Mathey, D.G.; Hamm, C.W.; et al. Improved clinical outcome after intracoronary administration of bone-marrow-derived progenitor cells in acute myocardial infarction: Final 1-year results of the REPAIR-AMI trial. Eur. Heart J. 2006, 27, 2775–2783. [Google Scholar] [CrossRef] [PubMed]
- Martin-Rendon, E.; Brunskill, S.J.; Hyde, C.J.; Stanworth, S.J.; Mathur, A.; Watt, S.M. Autologous bone marrow stem cells to treat acute myocardial infarction: A systematic review. Eur. Heart J. 2008, 29, 1807–1818. [Google Scholar] [CrossRef] [PubMed]
- Beeres, S.L.; Bax, J.J.; Kaandorp, T.A.; Zeppenfeld, K.; Lamb, H.J.; Dibbets-Schneider, P.; Stokkel, M.P.; Fibbe, W.E.; de Roos, A.; van der Wall, E.E.; et al. Usefulness of intramyocardial injection of autologous bone marrow-derived mononuclear cells in patients with severe angina pectoris and stress-induced myocardial ischemia. Am. J. Cardiol. 2006, 97, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Beeres, S.L.; Lamb, H.J.; Roes, S.D.; Holman, E.R.; Kaandorp, T.A.; Fibbe, W.E.; de Roos, A.; van der Wall, E.E.; Schalij, M.J.; Bax, J.J.; et al. Effect of intramyocardial bone marrow cell injection on diastolic function in patients with chronic myocardial ischemia. J. Magn. Reson. Imaging 2008, 27, 992–997. [Google Scholar] [CrossRef] [PubMed]
- Tse, H.F.; Thambar, S.; Kwong, Y.L.; Rowlings, P.; Bellamy, G.; McCrohon, J.; Thomas, P.; Bastian, B.; Chan, J.K.; Lo, G.; et al. Prospective randomized trial of direct endomyocardial implantation of bone marrow cells for treatment of severe coronary artery diseases (PROTECT-CAD trial). Eur. Heart J. 2007, 28, 2998–3005. [Google Scholar] [CrossRef] [PubMed]
- Veltman, C.E.; Soliman, O.I.; Geleijnse, M.L.; Vletter, W.B.; Smits, P.C.; ten Cate, F.J.; Jordaens, L.J.; Balk, A.H.; Serruys, P.W.; Boersma, E.; et al. Four-year follow-up of treatment with intramyocardial skeletal myoblasts injection in patients with ischaemic cardiomyopathy. Eur. Heart J. 2008, 29, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Hare, J.M.; Fishman, J.E.; Gerstenblith, G.; DiFede Velazquez, D.L.; Zambrano, J.P.; Suncion, V.Y.; Tracy, M.; Ghersin, E.; Johnston, P.V.; Brinker, J.A.; et al. Comparison of allogeneic vs autologous bone marrow-derived mesenchymal stem cells delivered by transendocardial injection in patients with ischemic cardiomyopathy: The POSEIDON randomized trial. JAMA 2012, 308, 2369–2379. [Google Scholar] [CrossRef] [PubMed]
- Hare, J.M.; Traverse, J.H.; Henry, T.D.; Dib, N.; Strumpf, R.K.; Schulman, S.P.; Gerstenblith, G.; DeMaria, A.N.; Denktas, A.E.; Gammon, R.S.; et al. A randomized, double-blind, placebo-controlled, dose-escalation study of intravenous adult human mesenchymal stem cells (prochymal) after acute myocardial infarction. J. Am. Coll. Cardiol. 2009, 54, 2277–2286. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, S.H.; Youn, Y.J.; Ahn, M.S.; Kim, J.Y.; Yoo, B.S.; Yoon, J.; Kwon, W.; Hong, I.S.; Lee, K.; et al. A randomized, open-label, multicenter trial for the safety and efficacy of adult mesenchymal stem cells after acute myocardial infarction. J. Korean Med. Sci. 2014, 29, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, M.; DiFede, D.L.; Golpanian, S.; Khan, A.; Gomes, S.A.; Mendizabal, A.; Heldman, A.W.; Hare, J.M. Rationale and design of the Percutaneous Stem Cell Injection Delivery Effects on Neomyogenesis in Dilated Cardiomyopathy (the POSEIDON-DCM study): A phase I/II, randomized pilot study of the comparative safety and efficacy of transendocardial injection of autologous mesenchymal stem cell vs. allogeneic mesenchymal stem cells in patients with non-ischemic dilated cardiomyopathy. J. Cardiovasc. Transl. Res. 2014, 7, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Bolli, R.; Chugh, A.R.; D’Amario, D.; Loughran, J.H.; Stoddard, M.F.; Ikram, S.; Beache, G.M.; Wagner, S.G.; Leri, A.; Hosoda, T.; et al. Cardiac stem cells in patients with ischaemic cardiomyopathy (SCIPIO): Initial results of a randomised phase 1 trial. Lancet 2011, 378, 1847–1857. [Google Scholar] [CrossRef]
- Chugh, A.R.; Beache, G.M.; Loughran, J.H.; Mewton, N.; Elmore, J.B.; Kajstura, J.; Pappas, P.; Tatooles, A.; Stoddard, M.F.; Lima, J.A.; et al. Administration of cardiac stem cells in patients with ischemic cardiomyopathy: The SCIPIO trial: Surgical aspects and interim analysis of myocardial function and viability by magnetic resonance. Circulation 2012, 126, S54–S64. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Smith, R.R.; Cheng, K.; Malliaras, K.; Thomson, L.E.; Berman, D.; Czer, L.S.; Marban, L.; Mendizabal, A.; Johnston, P.V.; et al. Intracoronary cardiosphere-derived cells for heart regeneration after myocardial infarction (CADUCEUS): A prospective, randomised phase 1 trial. Lancet 2012, 379, 895–904. [Google Scholar] [CrossRef]
- Malliaras, K.; Makkar, R.R.; Smith, R.R.; Cheng, K.; Wu, E.; Bonow, R.O.; Marban, L.; Mendizabal, A.; Cingolani, E.; Johnston, P.V.; et al. Intracoronary cardiosphere-derived cells after myocardial infarction: Evidence of therapeutic regeneration in the final 1-year results of the CADUCEUS trial (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction). J. Am. Coll. Cardiol. 2014, 63, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Quijada, P.; Sussman, M.A. Making it stick: Chasing the optimal stem cells for cardiac regeneration. Expert Rev. Cardiovasc. Ther. 2014, 12, 1275–1288. [Google Scholar] [CrossRef] [PubMed]
- Dixit, P.; Katare, R. Challenges in identifying the best source of stem cells for cardiac regeneration therapy. Stem Cell Res. Ther. 2015, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- Leite, C.F.; Almeida, T.R.; Lopes, C.S.; Dias da Silva, V.J. Multipotent stem cells of the heart-do they have therapeutic promise? Front. Physiol. 2015, 6, 123. [Google Scholar] [CrossRef] [PubMed]
- Byrne, N.; Velasco Forte, M.; Tandon, A.; Valverde, I.; Hussain, T. A systematic review of image segmentation methodology, used in the additive manufacture of patient-specific 3D printed models of the cardiovascular system. JRSM Cardiovasc. Dis. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Kurup, H.K.; Samuel, B.P.; Vettukattil, J.J. Hybrid 3D printing: A game-changer in personalized cardiac medicine? Expert Rev. Cardiovasc. Ther. 2015, 13, 1281–1284. [Google Scholar] [CrossRef] [PubMed]
- Schmauss, D.; Haeberle, S.; Hagl, C.; Sodian, R. Three-dimensional printing in cardiac surgery and interventional cardiology: A single-centre experience. Eur. J. Cardiothorac. Surg. 2015, 47, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Bartel, T.; Rivard, A.; Jimenez, A.; Mestres, C.A.; Muller, S. Medical three-dimensional printing opens up new opportunities in cardiology and cardiac surgery. Eur. Heart J. 2017. [Google Scholar] [CrossRef] [PubMed]
- Valverde, I. Three-dimensional printed cardiac models: Applications in the field of medical education, cardiovascular surgery, and structural heart interventions. Rev. Esp. Cardiol. 2017, 70, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Vukicevic, M.; Mosadegh, B.; Min, J.K.; Little, S.H. Cardiac 3D printing and its future directions. JACC Cardiovasc. Imaging 2017, 10, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, J.; Zheng, X.; Rong, X.; Zheng, X.; Peng, H.; Silber-Li, Z.; Li, M.; Liu, L. Three-dimensional virtual surgery models for percutaneous coronary intervention (PCI) optimization strategies. Sci. Rep. 2015, 5, 10945. [Google Scholar] [CrossRef] [PubMed]
- Javan, R.; Herrin, D.; Tangestanipoor, A. Understanding spatially complex segmental and branch anatomy using 3D printing: Liver, lung, prostate, coronary arteries, and circle of willis. Acad. Radiol. 2016, 23, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Kolli, K.K.; Min, J.K.; Ha, S.; Soohoo, H.; Xiong, G. Effect of varying hemodynamic and vascular conditions on fractional flow reserve: An in vitro study. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Gaetani, R.; Doevendans, P.A.; Metz, C.H.; Alblas, J.; Messina, E.; Giacomello, A.; Sluijter, J.P. Cardiac tissue engineering using tissue printing technology and human cardiac progenitor cells. Biomaterials 2012, 33, 1782–1790. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Kupfer, M.E.; Jung, J.P.; Yang, L.; Zhang, P.; Da Sie, Y.; Tran, Q.; Ajeti, V.; Freeman, B.T.; Fast, V.G.; et al. Myocardial tissue engineering with cells derived from human-induced pluripotent stem cells and a native-like, high-resolution, 3-dimensionally printed scaffold. Circ. Res. 2017, 120, 1318–1325. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.R.; Brummel-Ziedins, K.; Schneider, D.J. Novel oral anticoagulants in the management of coronary artery disease. Coron. Artery Dis. 2016, 27, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Oldgren, J.; Budaj, A.; Granger, C.B.; Khder, Y.; Roberts, J.; Siegbahn, A.; Tijssen, J.G.; van de Werf, F.; Wallentin, L.; Investigators, R.-D. Dabigatran vs. placebo in patients with acute coronary syndromes on dual antiplatelet therapy: A randomized, double-blind, phase II trial. Eur. Heart J. 2011, 32, 2781–2789. [Google Scholar] [CrossRef] [PubMed]
- Abifadel, M.; Varret, M.; Rabes, J.P.; Allard, D.; Ouguerram, K.; Devillers, M.; Cruaud, C.; Benjannet, S.; Wickham, L.; Erlich, D.; et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat. Genet. 2003, 34, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.; Bozzetto, L.; Annuzzi, G.; Rivellese, A.A. Alirocumab for the treatment of hypercholesterolaemia. Expert Rev. Clin. Pharmacol. 2017, 10, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Graham, M.J.; Lemonidis, K.M.; Whipple, C.P.; Subramaniam, A.; Monia, B.P.; Crooke, S.T.; Crooke, R.M. Antisense inhibition of proprotein convertase subtilisin/kexin type 9 reduces serum LDL in hyperlipidemic mice. J. Lipid Res. 2007, 48, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.A.; Mellis, S.; Yancopoulos, G.D.; Stahl, N.; Logan, D.; Smith, W.B.; Lisbon, E.; Gutierrez, M.; Webb, C.; Wu, R.; et al. Effect of a monoclonal antibody to PCSK9 on LDL cholesterol. N. Engl. J. Med. 2012, 366, 1108–1118. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.A.; Gipe, D.; Bergeron, J.; Gaudet, D.; Weiss, R.; Dufour, R.; Wu, R.; Pordy, R. Effect of a monoclonal antibody to PCSK9, REGN727/SAR236553, to reduce low-density lipoprotein cholesterol in patients with heterozygous familial hypercholesterolaemia on stable statin dose with or without ezetimibe therapy: A phase 2 randomised controlled trial. Lancet 2012, 380, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Roth, E.M.; McKenney, J.M.; Hanotin, C.; Asset, G.; Stein, E.A. Atorvastatin with or without an antibody to PCSK9 in primary hypercholesterolemia. N. Engl. J. Med. 2012, 367, 1891–1900. [Google Scholar] [CrossRef] [PubMed]
- Bays, H.; Gaudet, D.; Weiss, R.; Ruiz, J.L.; Watts, G.F.; Gouni-Berthold, I.; Robinson, J.; Zhao, J.; Hanotin, C.; Donahue, S. Alirocumab as add-on to atorvastatin versus other lipid treatment strategies: ODYSSEY OPTIONS I randomized trial. J. Clin. Endocrinol. Metab. 2015, 100, 3140–3148. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Cariou, B.; Blom, D.; McKenney, J.M.; Lorenzato, C.; Pordy, R.; Chaudhari, U.; Colhoun, H.M.; Investigators, O.C.I. Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated doses of statins: The ODYSSEY COMBO II randomized controlled trial. Eur. Heart J. 2015, 36, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Farnier, M.; Jones, P.; Severance, R.; Averna, M.; Steinhagen-Thiessen, E.; Colhoun, H.M.; Du, Y.; Hanotin, C.; Donahue, S. Efficacy and safety of adding alirocumab to rosuvastatin versus adding ezetimibe or doubling the rosuvastatin dose in high cardiovascular-risk patients: The ODYSSEY OPTIONS II randomized trial. Atherosclerosis 2016, 244, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, H.N.; Rader, D.J.; Raal, F.J.; Guyton, J.R.; Baccara-Dinet, M.T.; Lorenzato, C.; Pordy, R.; Stroes, E. Efficacy and safety of alirocumab in patients with heterozygous familial hypercholesterolemia and LDL-C of 160 mg/dL or higher. Cardiovasc. Drugs Ther. 2016, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Kastelein, J.J.; Ginsberg, H.N.; Langslet, G.; Hovingh, G.K.; Ceska, R.; Dufour, R.; Blom, D.; Civeira, F.; Krempf, M.; Lorenzato, C.; et al. ODYSSEY FH I and FH II: 78 week results with alirocumab treatment in 735 patients with heterozygous familial hypercholesterolaemia. Eur. Heart J. 2015, 36, 2996–3003. [Google Scholar] [CrossRef] [PubMed]
- Kereiakes, D.J.; Robinson, J.G.; Cannon, C.P.; Lorenzato, C.; Pordy, R.; Chaudhari, U.; Colhoun, H.M. Efficacy and safety of the proprotein convertase subtilisin/kexin type 9 inhibitor alirocumab among high cardiovascular risk patients on maximally tolerated statin therapy: The ODYSSEY COMBO I study. Am. Heart J. 2015, 169, 906–915. [Google Scholar] [CrossRef] [PubMed]
- Roth, E.M.; Moriarty, P.M.; Bergeron, J.; Langslet, G.; Manvelian, G.; Zhao, J.; Baccara-Dinet, M.T.; Rader, D.J.; ODYSSEY CHOICE I investigators. A phase III randomized trial evaluating alirocumab 300 mg every 4 weeks as monotherapy or add-on to statin: ODYSSEY CHOICE I. Atherosclerosis 2016, 254, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, P.M.; Thompson, P.D.; Cannon, C.P.; Guyton, J.R.; Bergeron, J.; Zieve, F.J.; Bruckert, E.; Jacobson, T.A.; Kopecky, S.L.; Baccara-Dinet, M.T.; et al. Efficacy and safety of alirocumab vs ezetimibe in statin-intolerant patients, with a statin rechallenge arm: The ODYSSEY ALTERNATIVE randomized trial. J. Clin. Lipidol. 2015, 9, 758–769. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.G.; Farnier, M.; Krempf, M.; Bergeron, J.; Luc, G.; Averna, M.; Stroes, E.S.; Langslet, G.; Raal, F.J.; El Shahawy, M.; et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N. Engl. J. Med. 2015, 372, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Roth, E.M.; Taskinen, M.R.; Ginsberg, H.N.; Kastelein, J.J.; Colhoun, H.M.; Robinson, J.G.; Merlet, L.; Pordy, R.; Baccara-Dinet, M.T. Monotherapy with the PCSK9 inhibitor alirocumab versus ezetimibe in patients with hypercholesterolemia: Results of a 24 week, double-blind, randomized Phase 3 trial. Int. J. Cardiol. 2014, 176, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroes, E.; Guyton, J.R.; Lepor, N.; Civeira, F.; Gaudet, D.; Watts, G.F.; Baccara-Dinet, M.T.; Lecorps, G.; Manvelian, G.; Farnier, M.; et al. Efficacy and safety of alirocumab 150 mg every 4 weeks in patients with hypercholesterolemia not on statin therapy: The ODYSSEY CHOICE II study. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, T.; Kobayashi, M.; Tasaki, H.; Yagyu, H.; Higashikata, T.; Takagi, Y.; Uno, K.; Baccara-Dinet, M.T.; Nohara, A. Efficacy and safety of alirocumab in japanese patients with heterozygous familial hypercholesterolemia or at high cardiovascular risk with hypercholesterolemia not adequately controlled with statins-ODYSSEY JAPAN randomized controlled trial. Circ. J. 2016, 80, 1980–1987. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Ginsberg, H.N.; Davidson, M.H.; Pordy, R.; Bessac, L.; Minini, P.; Eckel, R.H.; Cannon, C.P. Reductions in atherogenic lipids and major cardiovascular events: A pooled analysis of 10 ODYSSEY trials comparing alirocumab with control. Circulation 2016, 134, 1931–1943. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Pham, A.Q.; Patel, Y.; Gallagher, B. LCZ696 (angiotensin-neprilysin inhibition): The new kid on the heart failure block? J. Pharm. Pract. 2015, 28, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Seki, T.; Goto, K.; Kansui, Y.; Ohtsubo, T.; Matsumura, K.; Kitazono, T. Angiotensin II receptor-neprilysin inhibitor sacubitril/valsartan improves endothelial dysfunction in spontaneously hypertensive rats. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Desai, A.S. Angiotensin-neprilysin inhibition as a paradigm for All? Curr. Cardiol. Rep. 2016, 18, 115. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.S.; McMurray, J.J.; Packer, M.; Swedberg, K.; Rouleau, J.L.; Chen, F.; Gong, J.; Rizkala, A.R.; Brahimi, A.; Claggett, B.; et al. Effect of the angiotensin-receptor-neprilysin inhibitor LCZ696 compared with enalapril on mode of death in heart failure patients. Eur. Heart J. 2015, 36, 1990–1997. [Google Scholar] [CrossRef] [PubMed]
- Jhund, P.S.; Fu, M.; Bayram, E.; Chen, C.H.; Negrusz-Kawecka, M.; Rosenthal, A.; Desai, A.S.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; et al. Efficacy and safety of LCZ696 (sacubitril-valsartan) according to age: Insights from PARADIGM-HF. Eur. Heart J. 2015, 36, 2576–2584. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Claggett, B.; Desai, A.S.; Packer, M.; Zile, M.; Swedberg, K.; Rouleau, J.L.; Shi, V.C.; Starling, R.C.; Kozan, O.; et al. Influence of ejection fraction on outcomes and efficacy of sacubitril/valsartan (LCZ696) in heart failure with reduced ejection fraction: The prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure (PARADIGM-HF) trial. Circ. Heart Fail. 2016, 9, e002744. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.L.; Preiss, D.; Jhund, P.S.; Squire, I.; Cardoso, J.S.; Merkely, B.; Martinez, F.; Starling, R.C.; Desai, A.S.; Lefkowitz, M.P.; et al. Risk related to pre-diabetes mellitus and diabetes mellitus in heart failure with reduced ejection fraction: Insights from prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure trial. Circ. Heart Fail. 2016, 9. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
This schematic illustrates the potential applications by which nanotechnology, stem cells, robotics, new drugs and 3-D printing can be used in the treatment of coronary artery disease. Abbreviations: coronary artery bypass graft (CABG), coronary artery disease (CAD), percutaneous coronary intervention (PCI). The upward arrow represents an increase of blood flow.
Figure 1.
This schematic illustrates the potential applications by which nanotechnology, stem cells, robotics, new drugs and 3-D printing can be used in the treatment of coronary artery disease. Abbreviations: coronary artery bypass graft (CABG), coronary artery disease (CAD), percutaneous coronary intervention (PCI). The upward arrow represents an increase of blood flow.

Figure 2.
The schematic illustrates the potential advantages of using robotics in the treatment of CAD. The upward or downward arrows represent an increase or a decrease of blood flow, respectively.
Figure 2.
The schematic illustrates the potential advantages of using robotics in the treatment of CAD. The upward or downward arrows represent an increase or a decrease of blood flow, respectively.

Figure 3.
The schematic illustrates the potential advantages of using nanotechnology in the treatment of CAD. PCI—Percutaneous coronary intervention. Abbreviations: percutaneous coronary intervention (PCI). The upward or downward arrows represent an increase or a decrease of the referred parameters.
Figure 3.
The schematic illustrates the potential advantages of using nanotechnology in the treatment of CAD. PCI—Percutaneous coronary intervention. Abbreviations: percutaneous coronary intervention (PCI). The upward or downward arrows represent an increase or a decrease of the referred parameters.

Figure 4.
The schematic illustrates the potential of different types of stem cells in the treatment of CAD. Abbreviations: Adipose stem cells (ASC); bone-marrow stem cells (BMSC); cardiac stem cells (CSC); hematopoietic stem cells (HSC); pluripotent stem cells (PSC); stem cells (SC).
Figure 4.
The schematic illustrates the potential of different types of stem cells in the treatment of CAD. Abbreviations: Adipose stem cells (ASC); bone-marrow stem cells (BMSC); cardiac stem cells (CSC); hematopoietic stem cells (HSC); pluripotent stem cells (PSC); stem cells (SC).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of clinical studies for robotic assisted coronary artery bypass grafting.
| S. No. | Author’s Name | Results | Additional Comments |
|---|---|---|---|
| 1. | Dogan et al. [17] | They reported a patency rate of 100%. | TECAB was performed on hearts arrested intraoperatively. |
| 2. | Kappert et al. [18] | Reduced duration of surgery (down from 280 to 186 minutes); All of them had normal wound healing | TECAB was performed on a beating heart. 3 patients had to undergo re-exploration due to bleeding. |
| 3. | Mohr et al. [19] | Successful procedure in 22 patients (5 of them had to be converted to manual procedure); At discharge, patency was 100% and 95.4% at 3 months; In the TECAB group, success rate was 50%. | TECAB was performed on beating (n = 8) and arrested (n = 27) heart. |
TECAB: Totally endoscopic coronary artery bypass graft; S. No: Serial number.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kandaswamy, E.; Zuo, L. Recent Advances in Treatment of Coronary Artery Disease: Role of Science and Technology. Int. J. Mol. Sci. 2018, 19, 424. https://doi.org/10.3390/ijms19020424
AMA Style
Kandaswamy E, Zuo L. Recent Advances in Treatment of Coronary Artery Disease: Role of Science and Technology. International Journal of Molecular Sciences. 2018; 19(2):424. https://doi.org/10.3390/ijms19020424
Chicago/Turabian StyleKandaswamy, Eswar, and Li Zuo. 2018. "Recent Advances in Treatment of Coronary Artery Disease: Role of Science and Technology" International Journal of Molecular Sciences 19, no. 2: 424. https://doi.org/10.3390/ijms19020424
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.