
The Neutrophil/Lymphocyte Ratio at Diagnosis Is Significantly Associated with Survival in Metastatic Pancreatic Cancer Patients

Abstract
:1. Introduction
2. Results
2.1. Patient General Features and Circulating Markers of Inflammation
2.2. Risk Factor Analysis for Overall Survival
3. Discussion
4. Patients and Methods
4.1. Study Design and Population
4.2. Measured Biochemical Parameters
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; Jiang, Y.; Pillarisetty, V.G. Role of immune cells in pancreatic cancer from bench to clinical application: An updated review. Med. Baltim. 2016, 95, e5541. [Google Scholar] [CrossRef] [PubMed]
- Neesse, A.; Algül, H.; Tuveson, D.A.; Gress, T.M. Stromal biology and therapy in pancreatic cancer: A changing paradigm. Gut 2015, 64, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Inman, K.S.; Francis, A.A.; Murray, N.R. Complex role for the immune system in initiation and progression of pancreatic cancer. World J. Gastroenterol. 2014, 20, 11160–11181. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Geng, Y.; Sun, M.; Wang, P.; Chen, Z. Clinical implications of systemic inflammatory response markers as independent prognostic factors for advanced pancreatic cancer. Pancreatology 2015, 15, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.J.; Hu, Z.G.; Shi, W.X.; Deng, T.; He, S.Q.; Yuan, S.G. Prognostic significance of neutrophil to lymphocyte ratio in pancreatic cancer: A meta-analysis. World J. Gastroenterol. 2015, 21, 2807–2815. [Google Scholar] [CrossRef] [PubMed]
- Szkandera, J.; Stotz, M.; Absenger, G.; Stojakovic, T.; Samonigg, H.; Kornprat, P.; Schaberl-Moser, R.; Alzoughbi, W.; Lackner, C.; Ress, A.L.; et al. Validation of C-reactive protein levels as a prognostic indicator for survival in a large cohort of pancreatic cancer patients. Br. J. Cancer 2014, 110, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Stotz, M.; Gerger, A.; Eisner, F.; Szkandera, J.; Loibner, H.; Ress, A.L.; Kornprat, P.; AlZoughbi, W.; Seggewies, F.S.; Lackner, C.; et al. Increased neutrophil-lymphocyte ratio is a poor prognostic factor in patients with primary operable and inoperable pancreatic cancer. Br. J. Cancer 2013, 109, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, N.B.; Glen, P.; McMillan, D.C.; McKay, C.J.; Foulis, A.K.; Carter, R.; Imrie, C.W. Systemic inflammatory response predicts outcome in patients undergoing resection for ductal adenocarcinoma head of pancreas. Br. J. Cancer 2005, 92, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, I.; Peacock, O.; Lloyd, G.; Larvin, M.; Hall, R.I. Preoperative hematologic markers as independent predictors of prognosis in resected pancreatic ductal adenocarcinoma: Neutrophil-lymphocyte versus platelet-lymphocyte ratio. Am. J. Surg. 2010, 200, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.S.; Luo, H.Y.; Qiu, M.Z.; Wang, Z.Q.; Zhang, D.S.; Wang, F.H.; Li, Y.H.; Xu, R.H. Comparison of the prognostic values of various inflammation based factors in patients with pancreatic cancer. Med. Oncol. 2012, 29, 3092–3100. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Fujii, T.; Yabusaki, N.; Murotani, K.; Iwata, N.; Kanda, M.; Tanaka, C.; Nakayama, G.; Sugimoto, H.; Koike, M.; et al. Clinical implication of inflammation-based prognostic score in pancreatic cancer: Glasgow prognostic score is the most reliable parameter. Med. Baltim. 2016, 95, e3582. [Google Scholar] [CrossRef] [PubMed]
- Szkandera, J.; Stotz, M.; Eisner, F.; Absenger, G.; Stojakovic, T.; Samonigg, H.; Kornprat, P.; Schaberl-Moser, R.; Alzoughbi, W.; Ress, A.L.; et al. External validation of the derived neutrophil to lymphocyte ratio as a prognostic marker on a large cohort of pancreatic cancer patients. PLoS ONE 2013, 8, e78225. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.M.; Yeo, C.J.; Brody, J.R. Diagnostic, prognostic, and predictive biomarkers in pancreatic cancer. J. Surg. Oncol. 2013, 107, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Kadokura, M.; Ishida, Y.; Tatsumi, A.; Takahashi, E.; Shindo, H.; Amemiya, F.; Takano, S.; Fukasawa, M.; Sato, T.; Enomoto, N. Performance status and neutrophil-lymphocyte ratio are important prognostic factors in elderly patients with unresectable pancreatic cancer. J. Gastrointest. Oncol. 2016, 7, 982–988. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; El-Maraghi, R.H.; Hammel, P.; Heinemann, V.; Kunzmann, V.; Sastre, J.; Scheithauer, W.; Siena, S.; Tabernero, J.; Teixeira, L.; et al. nab-Paclitaxel plus gemcitabine for metastatic pancreatic cancer: Long-term survival from a phase III trial. J. Natl. Cancer Inst. 2015, 107, dju413. [Google Scholar] [CrossRef] [PubMed]
- Vivaldi, C.; Caparello, C.; Musettini, G.; Pasquini, G.; Catanese, S.; Fornaro, L.; Lencioni, M.; Falcone, A.; Vasile, E. First-line treatment with FOLFOXIRI for advanced pancreatic cancer in clinical practice: Patients’ outcome and analysis of prognostic factors. Int. J. Cancer 2016, 139, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Formica, V.; Morelli, C.; Ferroni, P.; Nardecchia, A.; Tesauro, M.; Pellicori, S.; Cereda, V.; Russo, A.; Riondino, S.; Guadagni, F.; et al. Neutrophil/lymphocyte ratio helps select metastatic pancreatic cancer patients benefitting from oxaliplatin. Cancer Biomark. 2016, 17, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Guo, J.; Guo, L.; Zuo, Q. The C-reactive protein/albumin ratio predicts overall survival of patients with advanced pancreatic cancer. Tumour Biol. 2016, 37, 12525–12533. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Chen, W.; Xie, Z.; Shao, Z.; Xie, H.; Qin, G.; Zhao, N. Prognostic relevance of lactate dehydrogenase in advanced pancreatic ductal adenocarcinoma patients. BMC Cancer 2017, 17, 25. [Google Scholar] [CrossRef] [PubMed]
- Ji, F.; Fu, S.J.; Guo, Z.Y.; Pang, H.; Ju, W.Q.; Wang, D.P.; Hua, Y.P.; He, X.S. Prognostic value of combined preoperative lactate dehydrogenase and alkaline phosphatase levels in patients with resectable pancreatic ductal adenocarcinoma. Med. Baltim. 2016, 95, e4065. [Google Scholar] [CrossRef] [PubMed]
- Faloppi, L.; Bianconi, M.; Giampieri, R.; Sobrero, A.; Labianca, R.; Ferrari, D.; Barni, S.; Aitini, E.; Zaniboni, A.; Boni, C.; et al. The value of lactate dehydrogenase serum levels as a prognostic and predictive factor for advanced pancreatic cancer patients receiving sorafenib. Oncotarget 2015, 6, 35087–35094. [Google Scholar] [PubMed]
- Tao, L.; Zhang, L.; Peng, Y.; Tao, M.; Li, L.; Xiu, D.; Yuan, C.; Ma, Z.; Jiang, B. Neutrophils assist the metastasis of circulating tumor cells in pancreatic ductal adenocarcinoma: A new hypothesis and a new predictor for distant metastasis. Med. Baltim. 2016, 95, e4932. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean Age (Years) | 69.9 (95% CI 68.5–71.4) |
|---|---|
| Male Sex | 112/206 (54.4%) |
| Disease Stage at diagnosis | |
| Potentially Resectable Disease | 76/206 (37%) |
| Locally Advanced Disease | 49/206 (24%) |
| Distant Metastasis | 81/206 (39%) |
| Mean primary Tumor Size (mm) | 39.4 (95% CI 37.4–41.4) |
| Patients with Ca 19.9 > 37 (U.I./mL) | 141/173 (81.5%) |
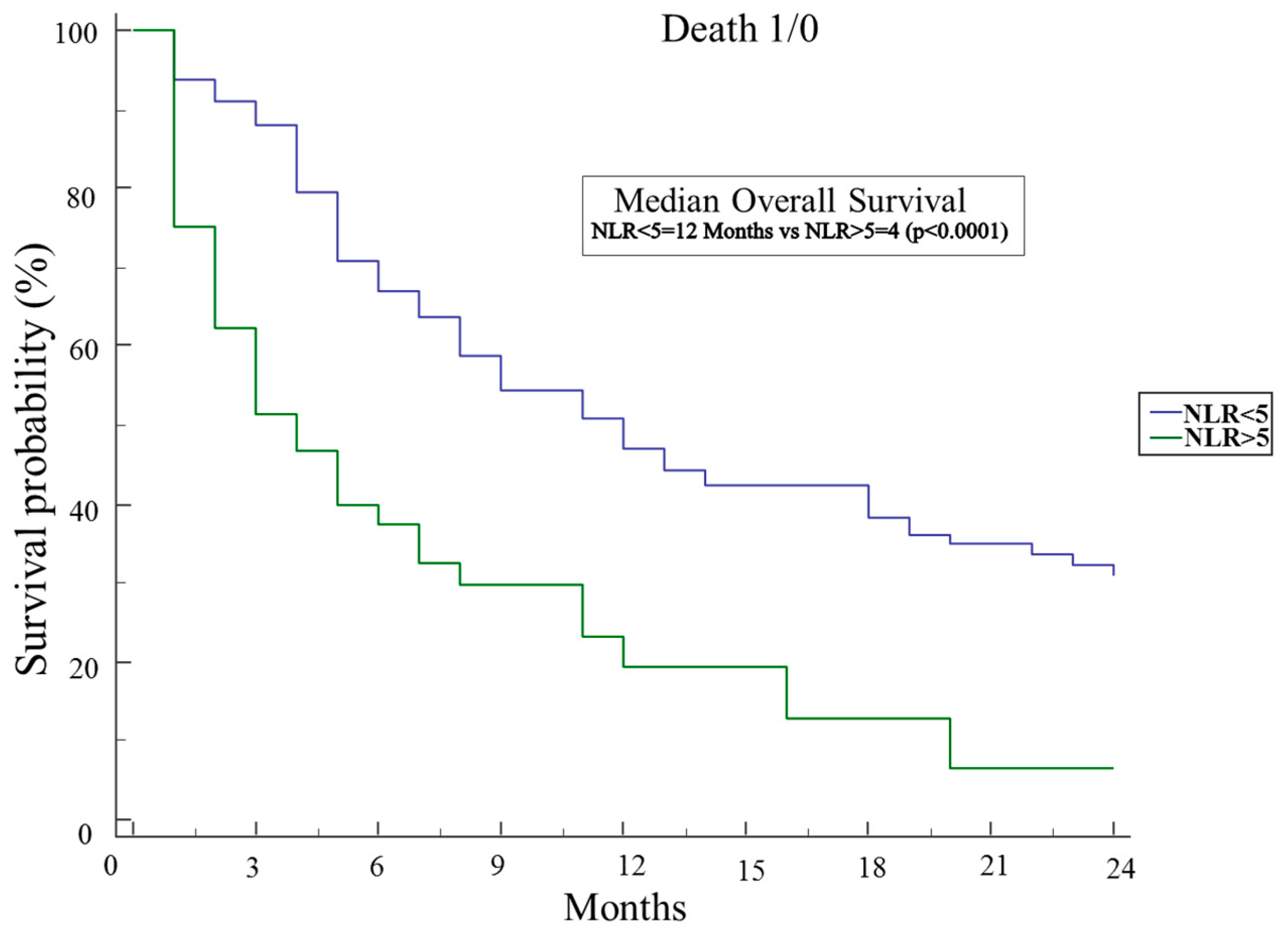
| Patients with an NLR > 5 | 60/206 (29.1%) |
| Patients with CRP levels > 1 mg/dL | 95/144 (65.9%) |
| Patients with Albumin levels < 3.5 g/dL | 110/189 (58.2%) |
| Patients with CRP/Albumin Ratio > 1 | 37/135 (27.4%) |
| Patients with Odonera PNI score < 35 | 110/189 (58.2%) |
| Glasgow Prognostic Score 0 | 26/136 (19.1%) |
| Glasgow Prognostic Score 1 | 44/136 (32.3%) |
| Glasgow Prognostic Score 2 | 66/136 (48.5%) |
| Patients Features | Univariate Analysis (HR 95% CI) | p-Value | Multivariate Analysis (HR 95% CI) | p-Value |
|---|---|---|---|---|
| Age (continuous variable) | 1.02 (1.006–1.04) | 0.007 | 1.02 (0.9–1.04) | 0.11 |
| Male Sex | 1.5 (1.1–2.1) | 0.02 | 1.2 (0.7–1.9) | 0.50 |
| Ca 19.9 (>37 U/mL) | 0.9 (0.6–1.5) | 0.82 | ||
| Primary Tumor Size (continuous variable) | 1.01 (1.004–1.03) | 0.009 | 1.02 (1.01–1.03) | 0.046 |
| Distant metastasis at diagnosis | 2.9 (2.1–4.3) | <0.0001 | 2.8 (1.7–4.7) | 0.0001 |
| Access to any Chemotherapy | 0.4 (0.3–0.6) | <0.0001 | 0.45 (0.28–0.75) | 0.0022 |
| CRP levels (mg/dL) (continuous variable) | 1.04 (1.0009–1.1) | 0.046 | ||
| NLR (continuous variable) | 1.1 (1.01–1.1) | 0.014 | ||
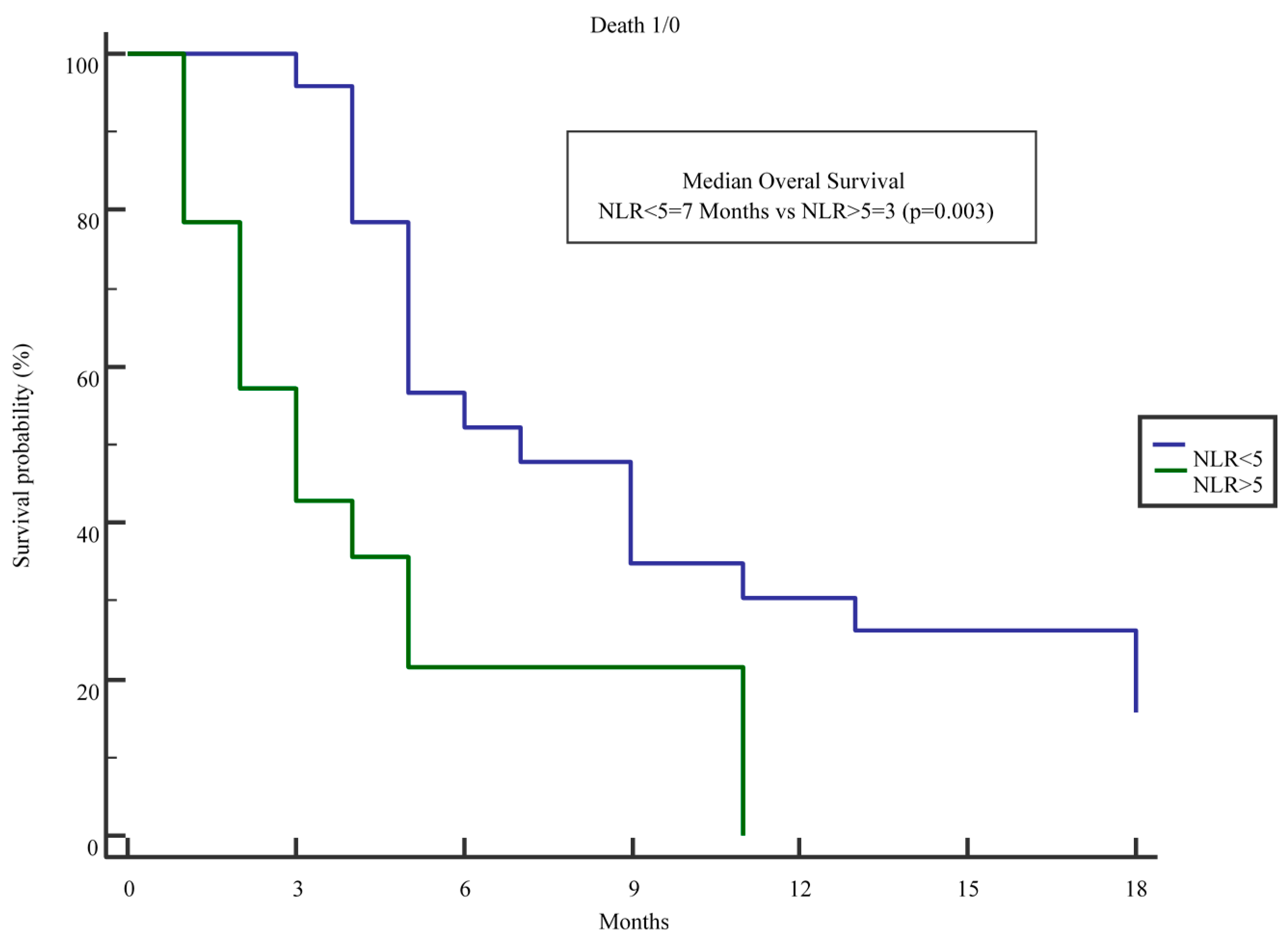
| NLR > 5 | 2.5 (1.7–3.7) | <0.0001 | 1.9 (1.1–3.3) | 0.027 |
| Odonera PNI score (continuous variable) | 0.96 (0.94–0.99) | 0.03 | ||
| Odonera < 35 | 1.6 (1.1–2.2) | 0.03 | ||
| CRP/Albumin (continuous variable) | 1.2 (1.02–1.3) | 0.03 | 1.1 (0.6–1.9) | 0.70 |
| CRP/Albumin > 1 | 2.02 (1.3–3.3) | 0.004 | ||
| GPS = 0 | 0.6 (0.4–1.2) | 0.17 | ||
| GPS = 1 | 0.8 (0.5–1.3) | 0.45 | ||
| GPS = 2 | 1.5 (0.9–2.4) | 0.06 | ||
| Plt/Lymphocyte Ratio | 1.001 (0.9–1.002) | 0.35 |
| Variable | Multivariate (OR 95% CI) | p-Value |
|---|---|---|
| Mean Age | 1.02 (0.99–1.04) | 0.09 |
| Access to Chemotherapy | 0.73 (0.42–1.26) | 0.26 |
| NLR > 5 | 1.75 (1.02–3.03) | 0.04 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piciucchi, M.; Stigliano, S.; Archibugi, L.; Zerboni, G.; Signoretti, M.; Barucca, V.; Valente, R.; Fave, G.D.; Capurso, G. The Neutrophil/Lymphocyte Ratio at Diagnosis Is Significantly Associated with Survival in Metastatic Pancreatic Cancer Patients. Int. J. Mol. Sci. 2017, 18, 730. https://doi.org/10.3390/ijms18040730
Piciucchi M, Stigliano S, Archibugi L, Zerboni G, Signoretti M, Barucca V, Valente R, Fave GD, Capurso G. The Neutrophil/Lymphocyte Ratio at Diagnosis Is Significantly Associated with Survival in Metastatic Pancreatic Cancer Patients. International Journal of Molecular Sciences. 2017; 18(4):730. https://doi.org/10.3390/ijms18040730
Chicago/Turabian StylePiciucchi, Matteo, Serena Stigliano, Livia Archibugi, Giulia Zerboni, Marianna Signoretti, Viola Barucca, Roberto Valente, Gianfranco Delle Fave, and Gabriele Capurso. 2017. "The Neutrophil/Lymphocyte Ratio at Diagnosis Is Significantly Associated with Survival in Metastatic Pancreatic Cancer Patients" International Journal of Molecular Sciences 18, no. 4: 730. https://doi.org/10.3390/ijms18040730