


Post-Viral Fatigue Following SARS-CoV-2 Infection during Pregnancy: A Longitudinal Comparative Study
 , , , , ,
, , , , ,
Abstract
:1. Introduction
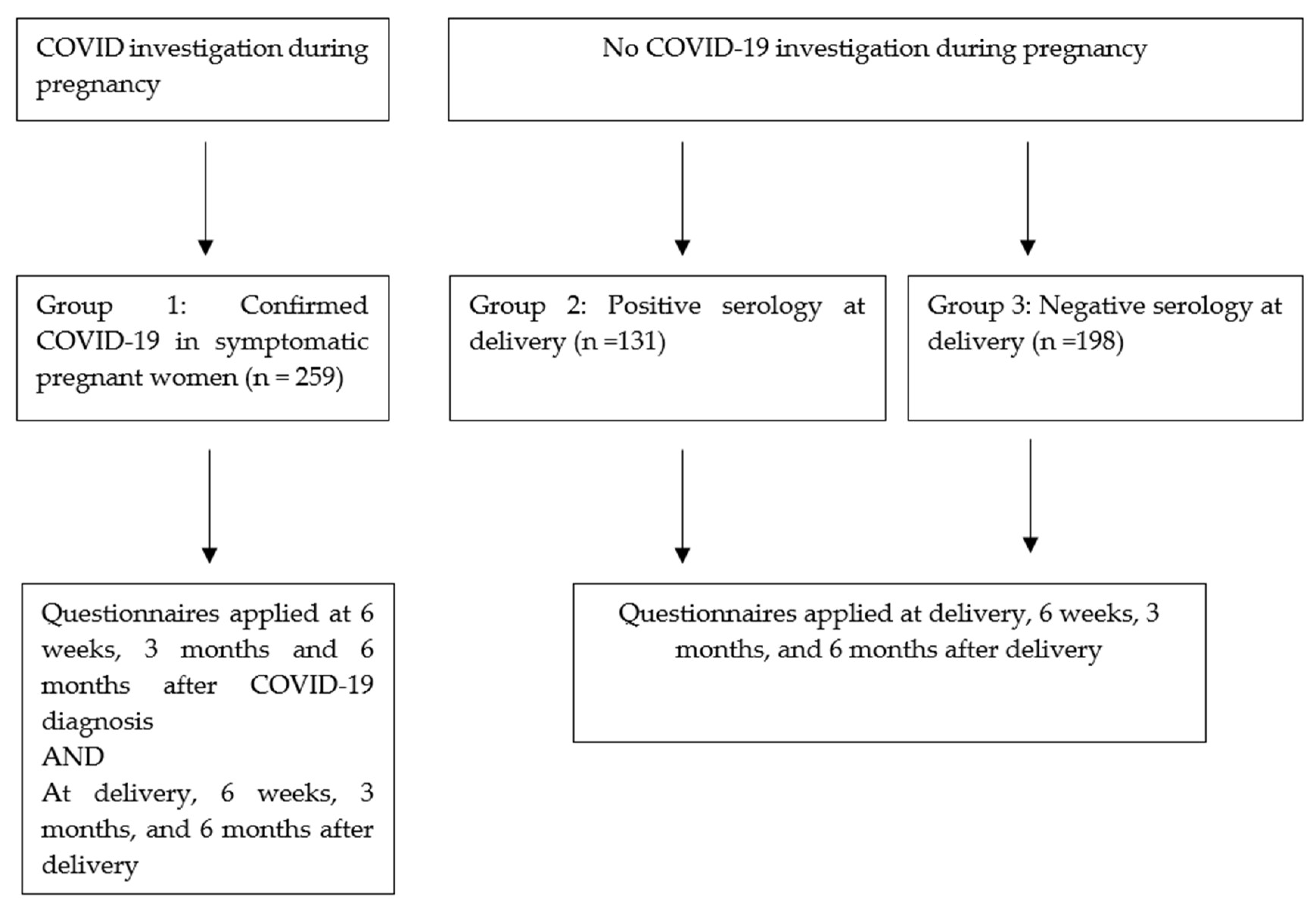
2. Materials and Methods
3. Results
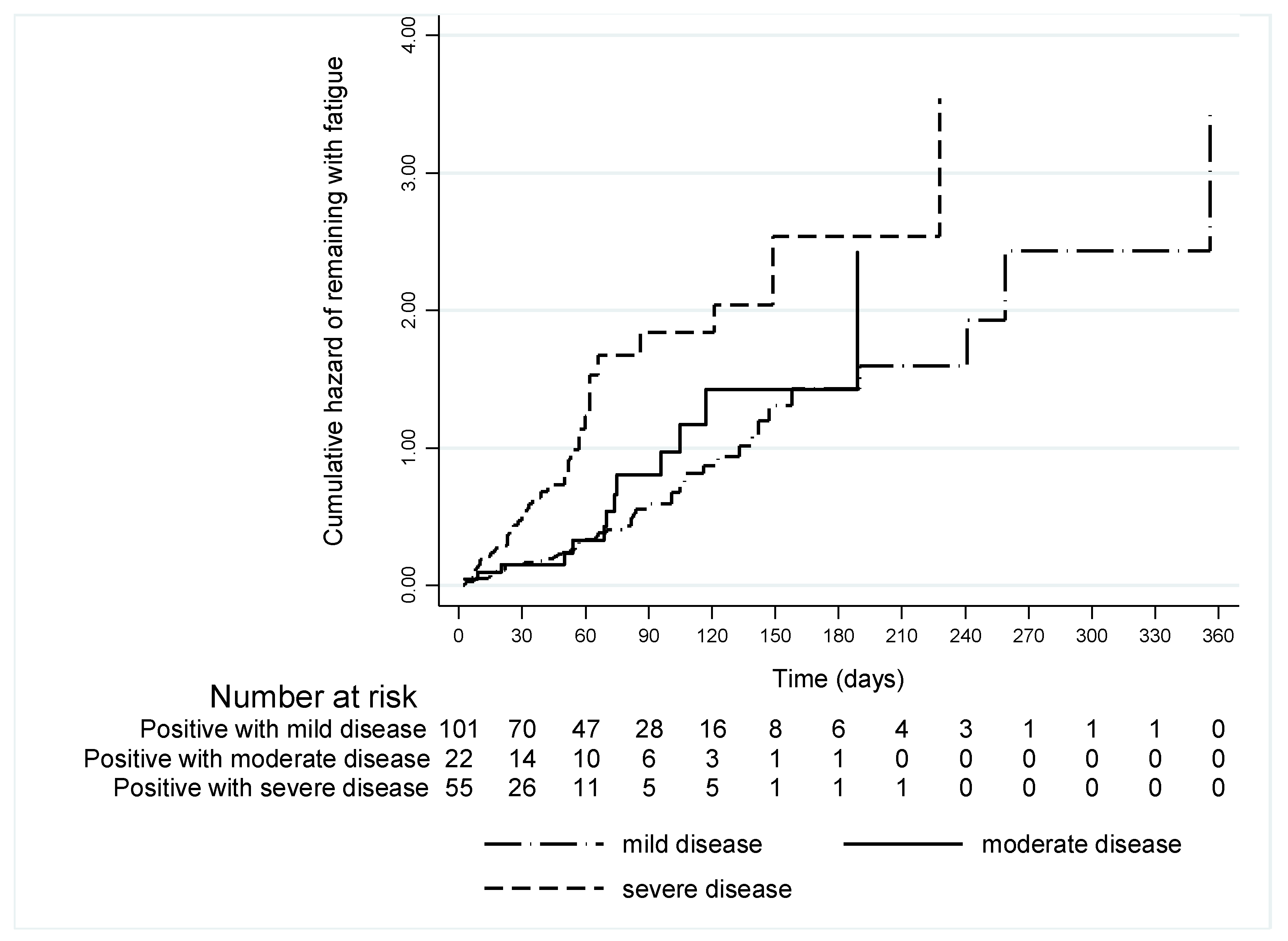
Prevalence over Time of Post-Viral Fatigue
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAAE | Certificate of Presentation of Ethical Appreciation |
| COVID-19 | CoronaVirus-associated Disease 2019 |
| IQR | Interquartile Range |
| ME/CFS | Myalgic Encephalomyelitis or Chronic Fatigue Syndrome |
| RT-PCR | Real-time polymerase chain reaction |
| SARS-CoV-2 | Respiratory Syndrome Coronavirus type-2 |
| SpO2 | Oxygen Saturation |
| SPSS | Statistical Package for the Social Sciences |
| USP | University of Sao Paulo |
References
- Stoecklin, S.B.; Rolland, P.; Yassoungolue, S.; Mailles, A.; Campese, C.; Simondon, A.; Mechain, M.; Meurice, L.; Nguyen, M.; Bassi, C.; et al. First cases of coronavirus disease 2019 (COVID-19) in France: Surveillance, investigations and control measures, January 2020. Eurosurveillance 2020, 25, 2000094. [Google Scholar]
- Xu, X.W.; Wu, X.X.; Jiang, X.G.; Xu, K.J.; Ying, L.J.; Ma, C.L.; Li, S.B.; Wang, H.Y.; Zhang, S.; Gao, H.N.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, m606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrin, R.; Riste, L.; Hann, M.; Walther, A.; Mukherjee, A.; Heald, A. Into the looking glass: Post-viral syndrome post COVID-19. Med. Hypotheses 2020, 144, 110055. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Goërtz, Y.M.J.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.C.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.E.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542. [Google Scholar] [CrossRef]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Negro, F.D.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- North American Nursing Diagnosis Association (NANDA). Nursing Diagnoses: Definitions and Classification 2003–2004; NANDA International: Philadelphia, PA, USA, 2003; p. 74. [Google Scholar]
- Brooks, K.; Webster, K.; Smith, E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Lerner, A.M.; Robinson, D.A.; Yang, L.; Williams, C.F.; Newman, L.M.; Breen, J.J.; Eisinger, R.W.; Schneider, J.S.; Adimora, A.A.; Erbelding, E.J. Toward Understanding COVID-19 Recovery: National Institutes of Health Workshop on Postacute COVID-19. Ann. Intern. Med. 2021, 174, 999–1003. [Google Scholar] [CrossRef]
- Collins, F. Study Finds 1 in 10 Healthcare Workers with Mild COVID Have Lasting Symptoms. Posted on 20 April 2021. Available online: https://directorsblog.nih.gov/2021/04/20/study-finds-1-in-10-healthcare-workers-with-mild-covid-have-lasting-symptoms/ (accessed on 2 May 2022).
- Brodaty, H.; Altendorf, A.; Withall, A.; Sachdev, P. Do people become more apathetic as they grow older? A longitudinal study in healthy individuals. Int. Psychogeriatr. 2010, 22, 426–436. [Google Scholar] [CrossRef]
- Lacerda, E.M.; Geraghty, K.; Kingdon, C.C.; Palla, L.; Nacul, L. A logistic regression analysis of risk factors in ME/CFS pathogenesis. BMC Neurol. 2019, 19, 275. [Google Scholar] [CrossRef]
- del Rio, C.; Malani, P.N. New insights on a rapidly changing epidemic. JAMA 2020, 323, 1339–1340. [Google Scholar] [CrossRef] [Green Version]
- Lawrie, S.M.; Manders, D.N.; Geddes, J.R.; Pelosi, A.J. A population-based incidence study of chronic fatigue. Psychol. Med. 1997, 27, 343–353. [Google Scholar] [CrossRef]
- Bates, D.W.; Schmitt, W.; Buchwald, D.; Ware, N.C.; Lee, J.; Thoyer, E.; Kornish, R.J.; Komaroff, A.L. Prevalence of fatigue and chronic fatigue syndrome in a primary care practice. Arch. Intern. Med. 1993, 153, 2759–2765. [Google Scholar] [CrossRef] [PubMed]
- Cullen, W.; Kearney, Y.; Bury, G. Prevalence of fatigue in general practice. Ir. J. Med. Sci. 2002, 171, 10–12. [Google Scholar] [CrossRef]
- Lacerda, E.M.; Bowman, E.W.; Cliff, J.M.; Kingdon, C.C.; King, E.C.; Lee, J.S.; Clark, T.G.; Dockrell, H.M.; Riley, E.M.; Curran, H.; et al. The UK ME/CFS Biobank for biomedical research on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Multiple Sclerosis. Open J. Bioresour. 2017, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Freyd, M. The Graphic Rating Scale. J. Educ. Psychol. 1923, 14, 83–102. [Google Scholar] [CrossRef]
- Lacerda, E.M.; Mudie, K.; Kingdon, C.C.; Butterworth, J.D.; O’Boyle, S.; Nacul, L. The UK ME/CFS Biobank: A Disease-Specific Biobank for Advancing Clinical Research Into Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Neurol. 2018, 9, 1026. [Google Scholar] [CrossRef] [Green Version]
- Maeda, M.d.Y.; Brizot, M.d.; Gibelli, M.A.B.C.; Ibidi, S.M.; de Carvalho, W.B.; Hoshida, M.S.; Machado, C.M.; Sabino, E.C.; da Silva, L.C.d.; Jaenisch, T.; et al. Vertical transmission of SARS-CoV2 during pregnancy: A high-risk cohort. Prenat. Diagn. 2021, 41, 998–1008. [Google Scholar] [CrossRef]
- González-Hermosillo, J.A.; Martínez-López, J.P.; Carrillo-Lampón, S.A.; Ruiz-Ojeda, D.; Herrera-Ramírez, S.; Amezcua-Guerra, L.M.; Martínez-Alvarado, M.D.R. Post-Acute COVID-19 Symptoms, a Potential Link with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A 6-Month Survey in a Mexican Cohort. Brain Sci. 2021, 11, 760. [Google Scholar] [CrossRef] [PubMed]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Prevalence and Determinants of Fatigue after COVID-19 in Non-Hospitalized Subjects: A Population-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 2030. [Google Scholar] [CrossRef] [PubMed]
- Nacul, L.; Authier, F.J.; Scheibenbogen, C.; Lorusso, L.; Helland, I.B.; Martin, J.A.; Sirbu, C.A.; Mengshoel, A.M.; Polo, O.; Behrends, U.; et al. European Network on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (EUROMENE): Expert Consensus on the Diagnosis, Service Provision, and Care of People with ME/CFS in Europe. Medicina 2021, 57, 510. [Google Scholar] [CrossRef] [PubMed]
- Ceban, F.; Ling, S.; Lui, L.M.W.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Matura, L.A.; Malone, S.; Jaime-Lara, R.; Riegel, B. A Systematic Review of Biological Mechanisms of Fatigue in Chronic Illness. Biol Res Nurs. 2018, 20, 410–421. [Google Scholar] [CrossRef]
- Shepherd, C.; Chaudhury, A. ME/CFS/PVFS—An Exploration of the Clinical Issues; MEA: Gawcott, UK, 2022. [Google Scholar]
- Sigera, P.C.; Rajapakse, S.; Weeratunga, P.; de Silva, N.L.; Gomes, L.; Malavige, G.N.; Rodrigo, C.; Fernando, S.D. Dengue and post-infection fatigue: Findings from a prospective cohort-the Colombo Dengue Study. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 669–676. [Google Scholar] [CrossRef]
- Gérardin, P.; Fianu, A.; Malvy, D.; Mussard, C.; Boussaïd, K.; Rollot, O.; Michault, A.; Gaüzere, B.; Bréart, G.; Favier, F. Perceived morbidity and community burden after a Chikungunya outbreak: The TELECHIK survey, a population-based cohort study. BMC Med. 2011, 9, 5. [Google Scholar] [CrossRef] [Green Version]
- Nacul, L.; O’Boyle, S.; Palla, L.; Nacul, F.E.; Mudie, K.; Kingdon, C.C.; Cliff, J.M.; Clark, T.G.; Dockrell, H.M.; Lacerda, E.M. How Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Progresses: The Natural History of ME/CFS. Front. Neurol. 2020, 11, 826. [Google Scholar] [CrossRef]
- Saleh, J.; Peyssonnaux, C.; Singh, K.K.; Edeas, M. Mitochondria and microbiota dysfunction in COVID-19 pathogenesis. Mitochondrion 2020, 54, 1–7. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Maternal Characteristics | n (%) or Median (IQR) | ||
|---|---|---|---|
| Group 1 (n = 259) | Group 2 (n = 131) | Group 3 (n = 198) | |
| Age, years, median | 31.0 (26–36) | 27.0 (23–75) | 30.5 (24–36) |
| Parity | |||
| Nulliparous | 78/256 (30.1) | 59/131 (44.7) | 75/198 (37.9) |
| Multiparous | 178/256 (68.7) | 73/131 (55.3) | 123/198 (62.1) |
| Ethnicity | |||
| White | 124/257 (48.2) | 44/131 (33.6) | 74/196 (37.8) |
| Other | 133/257 (51.8) | 87/131 (66.4) | 122/196 (62.2) |
| Current smoking | 19/248 (7.7) | 9/131 (6.9) | 19/197 (9.6) |
| Comorbidities | |||
| Diabetes mellitus | 10/258 (3.9) | 5/131 (3.8) | 5/197 (2.5) |
| Hypertension | 40/258 (15.5) | 5/131 (3.8) | 18/197 (9.1) |
| Heart disease | 13/258 (5.0) | 2/131 (1.5) | 6/197 (3.0) |
| Lung disease | 29/258 (11.2) | 3/131 (2.3) | 12/197 (6.1) |
| Mental health condition | 24/257 (9.3) | 6/131 (4.6) | 19/197 (9.6) |
| Number of comorbidities | |||
| 0 | 158/258 (61.8) | 110/131 (84.0) | 142/197 (72.1) |
| 1 | 80/258 (28.1) | 17/131 (13.0) | 44/197 (22.3) |
| ≥2 | 20/258 (7.8) | 4/131 (3.1) | 12/197 (6.1) |
| Obstetrical outcomes | |||
| Vaginal delivery | 79/217 (36.4) | 49/129 (37.5) | 81/194 (41.7) |
| Cesarean delivery | 138/217 (63.6) | 79/129 (61.2) | 107/194 (55.2) |
| Curettage | 0/217 | 2/129 (1.5) | 6/194 (3.1) |
| Fatigue-Related Outcomes | Timepoint after COVID-19 | ||
|---|---|---|---|
| 6 Weeks (n = 175) n (%) | 3 Months (n = 125) n (%) | 6 Months (n = 79) n (%) | |
| Fatigue | 71 (40.6) | 42 (33.6) | 22 (27.8) |
| Fatigue most of the time # | 6 (3.4) | 5 (3.9) | 5 (6.3) |
| Significant fatigue ## | 2 (1.1) | 3 (2.4) | 1(1.3) |
| Variables | Hazard Ratio (HR) | 95% CI | p |
|---|---|---|---|
| Lower–Upper | |||
| SARS-CoV-2 infection | |||
| Positive with mild disease | Reference | ||
| Positive with moderate disease | 1.69 | 0.89–3.20 | 0.107 |
| Positive with severe disease | 2.43 | 1.49–3.95 | <0.001 |
| Age, years | |||
| ≤25 | Reference | ||
| 25 to 34 | 1.43 | 0.64–3.23 | 0.383 |
| ≥35 | 2.08 | 0.95–4.80 | 0.084 |
| Pregnancy trimester | |||
| 1st | Reference | ||
| 2nd | 1.09 | 0.31–3.79 | 0.890 |
| 3rd | 0.96 | 0.29–3.18 | 0.943 |
| Comorbidities * | |||
| 0 | Reference | ||
| 1 | 0.83 | 0.51–1.35 | 0.460 |
| ≥2 | 0.67 | 0.28–1.60 | 0.372 |
| Variables | Hazard Ratio (HR) | 95% CI | p |
|---|---|---|---|
| Lower–Upper | |||
| Cough | 1.80 | 1.08–2.99 | 0.024 |
| Myalgia | 1.51 | 0.98–2.33 | 0.060 |
| Dyspnea | 1.43 | 0.93–2.18 | 0.100 |
| Fever | 1.54 | 1.04–2.28 | 0.032 |
| Fatigue | 1.32 | 0.90–1.94 | 0.162 |
| Asthenia | 1.20 | 0.82–1.76 | 0.345 |
| Headache | 1.01 | 0.68–1.49 | 0.968 |
| Diarrhea | 1.33 | 0.82–2.15 | 0.245 |
| Runny nose | 0.72 | 0.49–1.06 | 0.092 |
| Anosmia | 0.66 | 0.45–0.97 | 0.033 |
| Sore throat | 0.76 | 0.49–1.18 | 0.218 |
| Dysgeusia | 0.67 | 0.46–0.99 | 0.042 |
| Outcome at Each Time Point | Group 1 (n = 259) n (%) | Group 2 (n = 131) n (%) | Group 3 (n = 198) n (%) | p-Value | |
|---|---|---|---|---|---|
| Fatigue | Delivery | 28/145 (19.3) | 1/125 (0.8) | 4/181 (2.2) | <0.001 * |
| Six weeks | 34/134 (25.4) | 2/56 (3.6) | 3/69 (4.3) | <0.001 * | |
| Three months | 18/78 (23.1) | 3/34 (8.8) | 2/44 (4.5) | 0.011 ** | |
| Six months | 9/55 (16.4) | 0/28 | 1/34 (2.9) | 0.011 ** | |
| Fatigue most of the time # | Delivery | 2/145 (1.4) | 0/125 | 2/181 (1.0) | NA |
| 6 weeks | 2/134 (1.5) | 1/56 (5.3) | 0/69 | NA | |
| 3 months | 2/78 (2.6) | 0/34 | 0/44 | NA | |
| 6 months | 1/55 (1.8) | NA | 0/34 | NA | |
| Significant fatigue ## | Delivery | 2/145 (1.4) | 0/125 | 1/181 (0.6) | NA |
| 6 weeks | 0/134 | 0/56 | 0/69 | NA | |
| 3 months | 1/78 (1.3) | 0/34 | 0/44 | NA | |
| 6 months | 0/55 | NA | 0/34 | NA | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, A.M.d.S.S.; Carvalho, M.A.; Nacul, L.; Cabar, F.R.; Fabri, A.W.; Peres, S.V.; Zaccara, T.A.; O’Boyle, S.; Alexander, N.; Takiuti, N.H.; et al. Post-Viral Fatigue Following SARS-CoV-2 Infection during Pregnancy: A Longitudinal Comparative Study. Int. J. Environ. Res. Public Health 2022, 19, 15735. https://doi.org/10.3390/ijerph192315735
Oliveira AMdSS, Carvalho MA, Nacul L, Cabar FR, Fabri AW, Peres SV, Zaccara TA, O’Boyle S, Alexander N, Takiuti NH, et al. Post-Viral Fatigue Following SARS-CoV-2 Infection during Pregnancy: A Longitudinal Comparative Study. International Journal of Environmental Research and Public Health. 2022; 19(23):15735. https://doi.org/10.3390/ijerph192315735
Chicago/Turabian StyleOliveira, Ana Maria da Silva Sousa, Mariana Azevedo Carvalho, Luis Nacul, Fábio Roberto Cabar, Amanda Wictky Fabri, Stela Verzinhasse Peres, Tatiana Assuncao Zaccara, Shennae O’Boyle, Neal Alexander, Nilton Hideto Takiuti, and et al. 2022. "Post-Viral Fatigue Following SARS-CoV-2 Infection during Pregnancy: A Longitudinal Comparative Study" International Journal of Environmental Research and Public Health 19, no. 23: 15735. https://doi.org/10.3390/ijerph192315735