
Bioprinting Technology in Skin, Heart, Pancreas and Cartilage Tissues: Progress and Challenges in Clinical Practice

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Identifying the Research Question
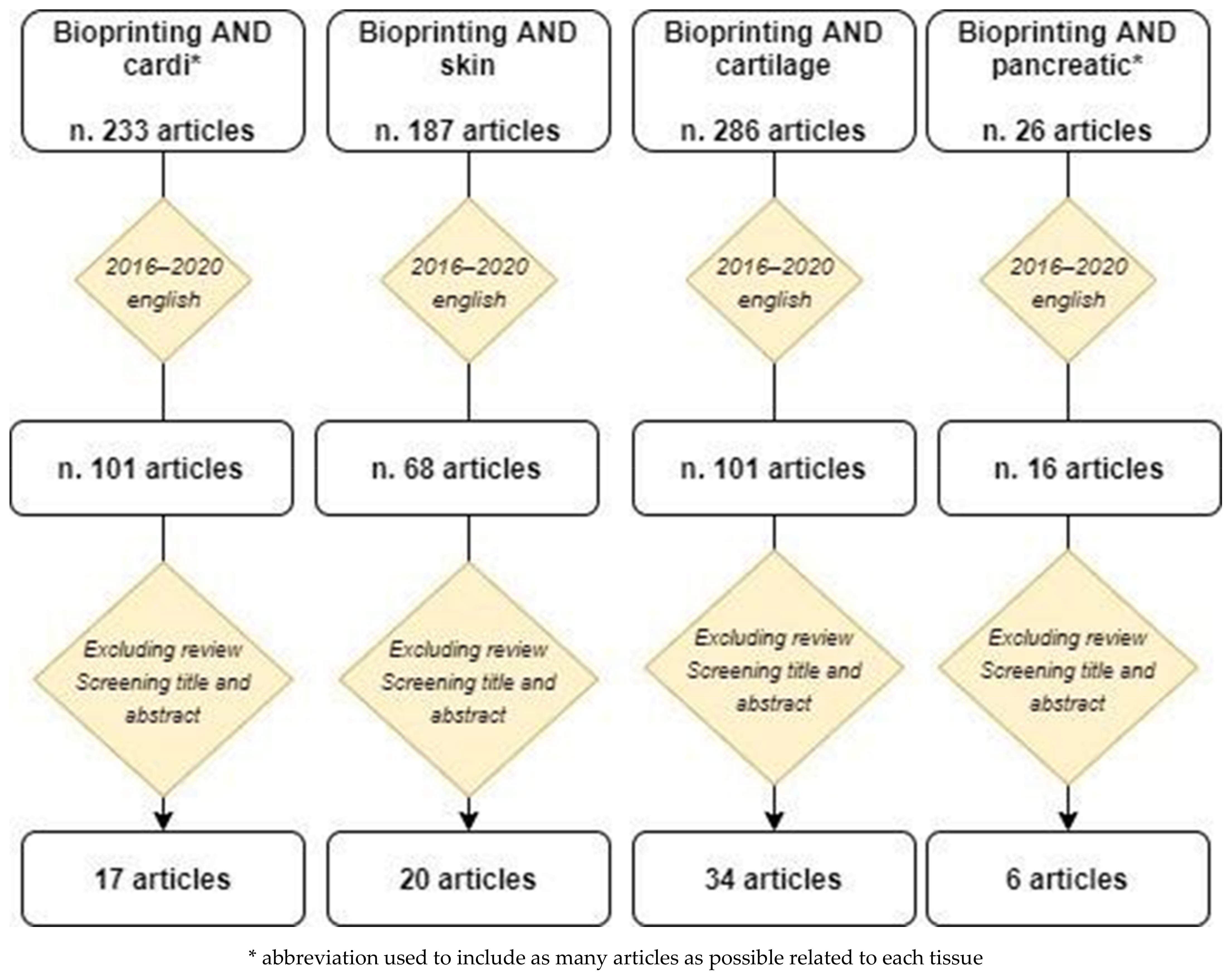
2.2. Identifying Relevant Studies
2.3. Selecting Studies
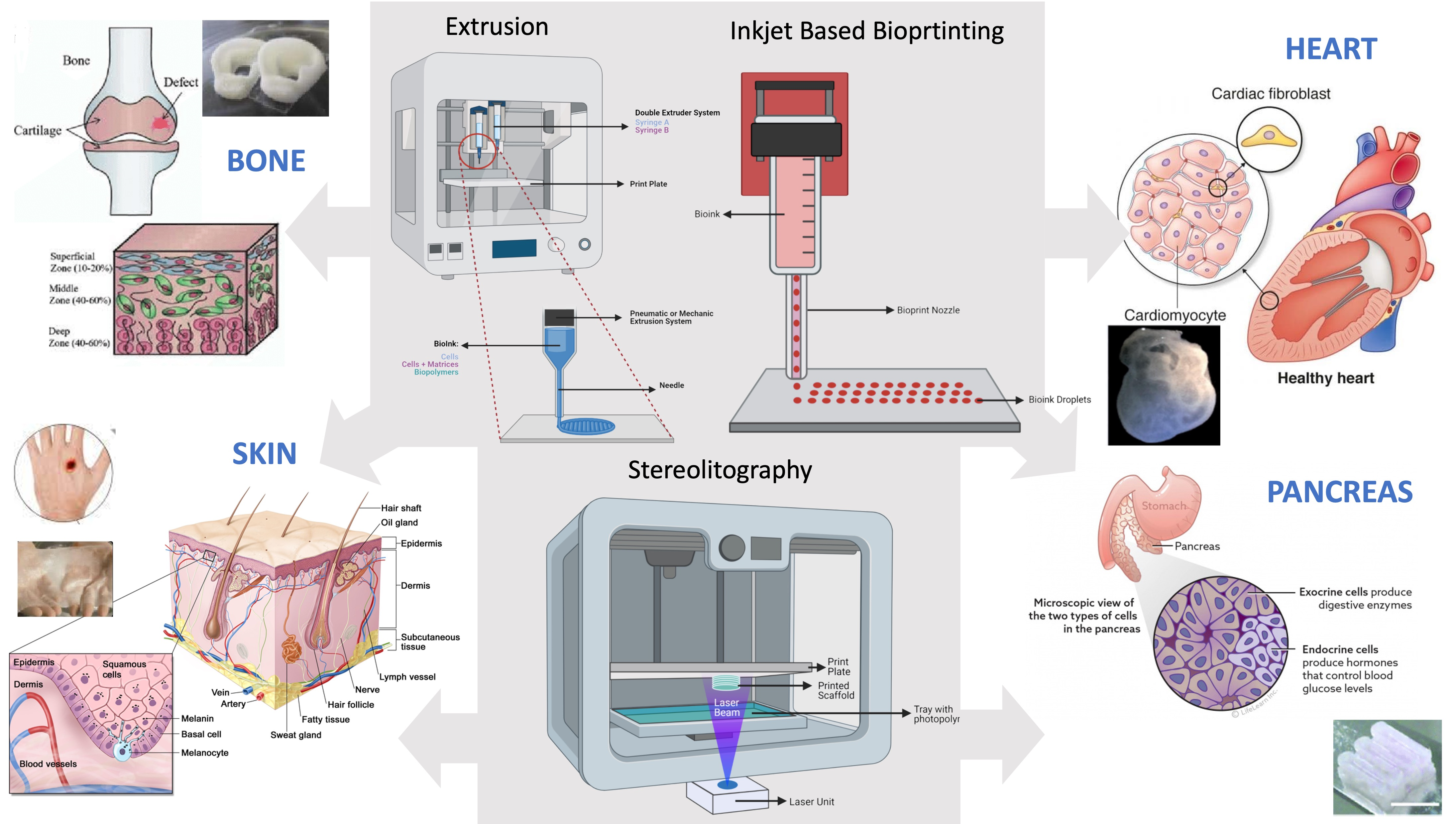
3. Main Bioprinting Techniques
3.1. Extrusion Printing
3.2. Inkjet—Based Bioprinting
3.3. Laser—Assisted Bioprinting (LAB)
3.4. Microvalve—Based Bioprinting
3.5. Stereolithography (SLA)
4. 3D Bioprinting of Skin
4.1. Background
4.2. Current Applications and Future Perspectives
5. 3D Bioprinting in Cardiovascular Disease
5.1. Background
5.2. Current Applications and Future Perspectives
6. 3D Bioprinting of Pancreatic Tissue
6.1. Background
6.2. Current Applications and Future Perspectives
7. 3D Bioprinting of Cartilage
7.1. Background
7.2. Current Applications and Future Perspectives
8. Hurdles and Promises of Bioprinting in the Clinical Routine
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Matai, I.; Kaur, G.; Seyedsalehi, A.; McClinton, A.; Laurencin, C.T. Progress in 3D bioprinting technology for tissue/organ regenerative engineering. Biomaterials 2020, 226, 119536. [Google Scholar] [CrossRef]
- Ma, X.; Liu, J.; Zhu, W.; Tang, M.; Lawrence, N.; Yu, C.; Goud, M.; Chen, S. 3D bioprinting of functional tissue models for personalized drug screening and in vitro disease modeling. Adv. Drug Deliv. Rev. 2018, 132, 235–251. [Google Scholar] [CrossRef]
- Vijayavenkataraman, S.; Yan, W.-C.; Lu, W.F.; Wang, C.-H.; Fuh, J.Y.H. 3D bioprinting of tissues and organs for regenerative medicine. Adv. Drug Deliv. Rev. 2018, 132, 296–332. [Google Scholar] [CrossRef]
- Ozbolat, I.T.; Peng, W.; Ozbolat, V. Application areas of 3D bioprinting. Drug Discov. Today 2016, 21, 1257–1271. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.V.; Atala, A. 3D bioprinting of tissues and organs. Nat. Biotechnol. 2014, 32, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Hospodiuk, M.; Dey, M.; Sosnoski, D.; Ozbolat, I.T. The bioink: A comprehensive review on bioprintable materials. Biotechnol. Adv. 2017, 35, 217–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, W.L.; Lee, J.M.; Yeong, W.Y.; Win Naing, M. Microvalve-based bioprinting—Process, bio-inks and applications. Biomater. Sci. 2017, 5, 632–647. [Google Scholar] [CrossRef] [Green Version]
- Tiberio, F.; Cacciotti, I.; Frassanito, P.; Nocca, G.; Tamburrini, G.; Arcovito, A.; Lattanzi, W. Personalized Bone Reconstruction and Regeneration in the Treatment of Craniosynostosis. Appl. Sci. 2021, 11, 2649. Available online: https://www.mdpi.com/2076-3417/11/6/2649 (accessed on 1 September 2021). [CrossRef]
- Seoane-Viaño, I.; Januskaite, P.; Alvarez-Lorenzo, C.; Basit, A.W.; Goyanes, A. Semi-solid extrusion 3D printing in drug delivery and biomedicine: Personalised solutions for healthcare challenges. J. Control. Release 2021, 332, 367–389. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Diggle, B.; Tan, M.L.; Viktorova, J.; Bennett, C.W.; Connal, L.A. Extrusion 3D Printing of Polymeric Materials with Advanced Properties. Adv. Sci. 2020, 7, 2001379. [Google Scholar] [CrossRef]
- Sodupe Ortega, E.; Sanz-Garcia, A.; Pernia-Espinoza, A.; Escobedo-Lucea, C. Efficient Fabrication of Polycaprolactone Scaffolds for Printing Hybrid Tissue-Engineered Constructs. Materials 2019, 12, 613. [Google Scholar] [CrossRef] [Green Version]
- Nurdillayeva, R.N.; Oshido, A.B.; Bamford, T.A.; El-Zubir, O.; Houlton, A.; Hedley, J.; Pike, A.R.; Horrocks, B.R. Inkjet printing and electrical characterisation of DNA-templated cadmium sulphide nanowires. Nanotechnology 2018, 29, 135704. [Google Scholar] [CrossRef] [PubMed]
- Tse, C.C.W.; Smith, P.J. Inkjet Printing for Biomedical Applications. Methods Mol. Biol. 2018, 1771, 107–117. [Google Scholar]
- Capulli, A.K.; Emmert, M.Y.; Pasqualini, F.S.; Kehl, D.; Caliskan, E.; Lind, J.U.; Sheehya, S.P.; Park, S.J.; Ahn, S.; Weber, B.; et al. JetValve: Rapid manufacturing of biohybrid scaffolds for biomimetic heart valve replacement. Biomaterials 2017, 133, 229–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakobyan, D.; Kerouredan, O.; Remy, M.; Dusserre, N.; Medina, C.; Devillard, R.; Fricain, J.-C.; Oliveira, H. Laser-Assisted Bioprinting for Bone Repair. Methods Mol. Biol. 2020, 2140, 135–144. [Google Scholar]
- Kérourédan, O.; Hakobyan, D.; Rémy, M.; Ziane, S.; Dusserre, N.; Fricain, J.-C.; Delmond, S.; Thébaud, N.B.; Devillard, R. In situ prevascularization designed by laser-assisted bioprinting: Effect on bone regeneration. Biofabrication 2019, 11, 045002. [Google Scholar] [CrossRef] [PubMed]
- Shi, P.; Tan, Y.S.E.; Yeong, W.Y.; Li, H.Y.; Laude, A. A bilayer photoreceptor-retinal tissue model with gradient cell density design: A study of microvalve-based bioprinting. J. Tissue Eng. Regen. Med. 2018, 12, 1297–1306. [Google Scholar] [CrossRef]
- Melchels, F.P.W.; Feijen, J.; Grijpma, D.W. A review on stereolithography and its applications in biomedical engineering. Biomaterials 2010, 31, 6121–6130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickett, R.R. and Visscher, M.O. Structure and Function of the Epidermal Barrier. Am. J. Infect. Control 2006, 34, S98–S110. Available online: https://doi.org/10.1016/j.ajic.2006.05.295 (accessed on 1 September 2021). [CrossRef]
- Abdo, J.; Ortman, H. Biologic and Synthetic Cellular and/or Tissue-Based Products and Smart Wound Dressings/Coverings. Surg. Clin. N. Am. 2020, 100, 741–756. [Google Scholar] [CrossRef]
- Coyer, F.; Gardner, A.; Doubrovsky, A.; Cole, R.; Ryan, F.M.; Allen, C.; McNamara, G. Reducing pressure injuries in critically ill patients by using a patient skin integrity care bundle (InSPiRE). Am. J. Crit. Care 2015, 24, 199–209. [Google Scholar] [CrossRef] [Green Version]
- Chocarro-Wrona, C.; López-Ruiz, E.; Perán, M.; Gálvez-Martín, P.; Marchal, J.A. Therapeutic strategies for skin regeneration based on biomedical substitutes. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 484–496. [Google Scholar] [CrossRef]
- Peirce, S.C.; Carolan-Rees, G. ReCell® Spray-On Skin System for Treating Skin Loss, Scarring and Depigmentation after Burn Injury: A NICE Medical Technology Guidance. Appl. Health Econ. Health Policy 2019, 17, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.-C.; Davoodi, P.; Vijayavenkataraman, S.; Tian, Y.; Ng, W.C.; Fuh, J.Y.H.; Robinson, K.S.; Wang, C.H. 3D bioprinting of skin tissue: From pre-processing to final product evaluation. Adv. Drug Deliv. Rev. 2018, 132, 270–295. [Google Scholar] [CrossRef] [PubMed]
- Cubo, N.; Garcia, M.; Del Cañizo, J.F.; Velasco, D.; Jorcano, J.L. 3D bioprinting of functional human skin: Production and in vivo analysis. Biofabrication 2016, 9, 015006. [Google Scholar] [CrossRef] [Green Version]
- Pourchet, L.J.; Thepot, A.; Albouy, M.; Courtial, E.J.; Boher, A.; Blum, L.J.; Marquette, C.A. Human Skin 3D Bioprinting Using Scaffold-Free Approach. Adv. Healthc. Mater. 2017, 6, 1601101. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Yoo, J.J.; Lee, S.J. Three-dimensional cell-based bioprinting for soft tissue regeneration. Tissue Eng. Regen. Med. 2016, 13, 647–662. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.S.; Kwon, Y.W.; Kong, J.-S.; Park, G.T.; Gao, G.; Han, W.; Kim, M.-B.; Lee, H.; Kim, J.H.; Choa, D.-W. 3D cell printing of in vitro stabilized skin model and in vivo pre-vascularized skin patch using tissue-specific extracellular matrix bioink: A step towards advanced skin tissue engineering. Biomaterials 2018, 168, 38–53. [Google Scholar] [CrossRef]
- Xiong, R.; Zhang, Z.; Chai, W.; Chrisey, D.B.; Huang, Y. Study of gelatin as an effective energy absorbing layer for laser bioprinting. Biofabrication 2017, 9, 024103. [Google Scholar] [CrossRef]
- Hossain, M.R.; Ansary, T.M.; Komine, M.; Ohtsuki, M. Diversified Stimuli-Induced Inflammatory Pathways Cause Skin Pigmentation. Int. J. Mol. Sci. 2021, 22, 3970. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, A.M.; Varkey, M.; Gorkun, A.; Clouse, C.; Xu, L.; Chou, Z.; Murphy, S.V.; Molnar, J.; Lee, S.J.; Yoo, J.J.; et al. Bioprinted Skin Recapitulates Normal Collagen Remodeling in Full-Thickness Wounds. Tissue Eng. Part A 2020, 26, 512–526. [Google Scholar] [CrossRef]
- Min, D.; Lee, W.; Bae, I.-H.; Lee, T.R.; Croce, P.; Yoo, S.-S. Bioprinting of biomimetic skin containing melanocytes. Exp. Dermatol. 2018, 27, 453–459. [Google Scholar] [CrossRef]
- Shi, Y.; Xing, T.L.; Zhang, H.B.; Yin, R.X.; Yang, S.M.; Wei, J.; Zhang, W.J. Tyrosinase-doped bioink for 3D bioprinting of living skin constructs. Biomed. Mater. 2018, 13, 035008. [Google Scholar] [CrossRef]
- Ng, H.Y.; Lee, K.-X.A.; Kuo, C.-N.; Shen, Y.-F. Bioprinting of artificial blood vessels. Int. J. Bioprinting 2018, 4, 140. [Google Scholar] [CrossRef]
- Di Bella, C.D.; Duchi, S.; O’Connell, C.D.; Blanchard, R.; Augustine, C.; Yue, Z.; Thompson, F.; Richards, C.; Beirne, S.; Onofrillo, C.; et al. In situ handheld three-dimensional bioprinting for cartilage regeneration. J. Tissue Eng. Regen. Med. 2018, 12, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-H.; Jung, C.S.; Min, B.-H. Advances in three-dimensional bioprinting for hard tissue engineering. Tissue Eng. Regen. Med. 2016, 13, 622–635. [Google Scholar] [CrossRef] [PubMed]
- Research C for DE and Current Good Manufacturing Practice (CGMP) Regulations. 2020. Available online: https://www.fda.gov/drugs/pharmaceutical-quality-resources/current-good-manufacturing-practice-cgmp-regulations (accessed on 1 September 2021).
- Duan, B. State-of-the-Art Review of 3D Bioprinting for Cardiovascular Tissue Engineering. Ann. Biomed. Eng. 2016, 45, 195–209. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Li, Y.; Zeng, X.; Wang, H.; Yin, P.; Wang, L.; Liu, Y.; Liu, J.; Qi, J.; Ran, S.; et al. Burden of Cardiovascular Diseases in China, 1990–2016: Findings From the 2016 Global Burden of Disease Study. JAMA Cardiol. 2019, 4, 342–352. [Google Scholar] [CrossRef]
- UN General Assembly. General Assembly United Nations. Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases. 2021. Available online: https://documents-dds-ny.un.org/doc/UNDOC/LTD/N11/497/77/PDF/N1149777.pdf?OpenElement (accessed on 1 September 2021).
- Zhang, Y.S.; Arneri, A.; Bersini, S.; Shin, S.-R.; Zhu, K.; Goli-Malekabadi, Z.; Aleman, J.; Colosi, C.; Busignani, F.; Dell’Erba, V.; et al. Bioprinting 3D microfibrous scaffolds for engineering endothelialized myocardium and heart-on-a-chip. Biomaterials 2016, 110, 45–59. [Google Scholar] [CrossRef] [Green Version]
- Madonna, R.; Van Laake, L.W.; Botker, H.E.; Davidson, S.M.; De Caterina, R.; Engel, F.B.; Eschenhagen, T.; Fernandez-Aviles, F.; Hausenloy, D.J.; Hulot, J.S.; et al. ESC Working Group on Cellular Biology of the Heart: Position paper for Cardiovascular Research: Tissue engineering strategies combined with cell therapies for cardiac repair in ischaemic heart disease and heart failure. Cardiovasc. Res. 2019, 115, 488–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, G.; Cui, X. Three-dimensional bioprinting in tissue engineering and regenerative medicine. Biotechnol. Lett. 2016, 38, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Richardson, W.J.; Clarke, S.A.; Quinn, T.A.; Holmes, J.W. Physiological Implications of Myocardial Scar Structure. Compr. Physiol. 2015, 5, 1877–1909. [Google Scholar] [PubMed] [Green Version]
- Seymour, D.G.; Green, M.; Vaz, F.G.; Coles, E.C. Risk prediction in medicine and surgery: Ethical and practical considerations. J. R. Coll. Physicians Lond. 1990, 24, 173–177. [Google Scholar]
- Bishop, E.S.; Mostafa, S.; Pakvasa, M.; Luu, H.H.; Lee, M.J.; Wolf, J.M.; Ameer, G.A.; He, T.-C.; Reid, R.R. 3-D bioprinting technologies in tissue engineering and regenerative medicine: Current and future trends. Genes Dis. 2017, 4, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Hudson, A.R.; Shiwarski, D.J.; Tashman, J.W.; Hinton, T.J.; Yerneni, S.; Bliley, J.M.; Campbell, P.G.; Feinberg, A.W. 3D bioprinting of collagen to rebuild components of the human heart. Science 2019, 365, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Noor, N.; Shapira, A.; Edri, R.; Gal, I.; Wertheim, L.; Dvir, T. 3D Printing of Personalized Thick and Perfusable Cardiac Patches and Hearts. Adv. Sci. 2019, 6, 1900344. [Google Scholar] [CrossRef] [Green Version]
- Kupfer, M.E.; Lin, W.-H.; Ravikumar, V.; Qiu, K.; Wang, L.; Gao, L.; Bhuiyan, D.B.; Lenz, M.; Ai, J.; Mahutga, R.R.; et al. In Situ Expansion, Differentiation, and Electromechanical Coupling of Human Cardiac Muscle in a 3D Bioprinted, Chambered Organoid. Circ. Res. 2020, 127, 207–224. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Lee, S.J.; Cheng, H.-J.; Yoo, J.J.; Atala, A. 3D bioprinted functional and contractile cardiac tissue constructs. Acta Biomater. 2018, 70, 48–56. [Google Scholar] [CrossRef]
- Das, S.; Kim, S.-W.; Choi, Y.-J.; Lee, S.; Lee, S.-H.; Kong, J.-S.; Park, H.J.; Cho, D.W.; Jang, J. Decellularized extracellular matrix bioinks and the external stimuli to enhance cardiac tissue development in vitro. Acta Biomater. 2019, 95, 188–200. [Google Scholar] [CrossRef]
- Jang, J.; Park, H.-J.; Kim, S.-W.; Kim, H.; Park, J.Y.; Na, S.J.; Kim, H.J.; Park, M.N.; Choi, S.H.; Park, S.H.; et al. 3D printed complex tissue construct using stem cell-laden decellularized extracellular matrix bioinks for cardiac repair. Biomaterials 2017, 112, 264–274. [Google Scholar] [CrossRef]
- Pati, F.; Cho, D.-W. Bioprinting of 3D Tissue Models Using Decellularized Extracellular Matrix Bioink. Methods Mol. Biol. 2017, 1612, 381–390. [Google Scholar]
- Zhu, K.; Shin, S.R.; van Kempen, T.; Li, Y.-C.; Ponraj, V.; Nasajpour, A.; Mandla, S.; Hu, N.; Liu, X.; Leijten, J.; et al. Gold Nanocomposite Bioink for Printing 3D Cardiac Constructs. Adv. Funct. Mater. 2017, 27, 1605352. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, N.I.; Hibino, N.; Nakayama, K. Principles of the Kenzan Method for Robotic Cell Spheroid-Based Three-Dimensional Bioprinting. Tissue Eng. Part B Rev. 2017, 23, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Ong, C.S.; Fukunishi, T.; Zhang, H.; Huang, C.Y.; Nashed, A.; Blazeski, A.; DiSilvestre, D.; Vricella, L.; Conte, J.; Tung, L.; et al. Biomaterial-Free Three-Dimensional Bioprinting of Cardiac Tissue using Human Induced Pluripotent Stem Cell Derived Cardiomyocytes. Sci. Rep. 2017, 7, 4566. [Google Scholar] [CrossRef] [Green Version]
- Yeung, E.; Fukunishi, T.; Bai, Y.; Bedja, D.; Pitaktong, I.; Mattson, G.; Jeyaram, A.; Lui, C.; Ong, C.S.; Inoue, T.; et al. Cardiac regeneration using human-induced pluripotent stem cell-derived biomaterial-free 3D-bioprinted cardiac patch in vivo. J. Tissue Eng. Regen. Med. 2019, 13, 2031–2039. [Google Scholar] [CrossRef]
- Liu, N.; Ye, X.; Yao, B.; Zhao, M.; Wu, P.; Liu, G.; Zhuang, D.; Jiang, H.; Chen, X.; He, Y.; et al. Advances in 3D bioprinting technology for cardiac tissue engineering and regeneration. Bioact. Mater. 2021, 6, 1388–1401. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, P.; Schweller, R.M.; Khademhosseini, A.; West, J.L.; Bashir, R. 3D biofabrication strategies for tissue engineering and regenerative medicine. Annu. Rev. Biomed. Eng. 2014, 16, 247–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Nuglozeh, E.; Touré, F.; Schmidt, A.M.; Vunjak-Novakovic, G. Controllable expansion of primary cardiomyocytes by reversible immortalization. Hum. Gene Ther. 2009, 20, 1687–1696. [Google Scholar] [CrossRef]
- Bejleri, D.; Streeter, B.W.; Nachlas, A.L.Y.; Brown, M.E.; Gaetani, R.; Christman, K.L.; Davis, M.E. A Bioprinted Cardiac Patch Composed of Cardiac-Specific Extracellular Matrix and Progenitor Cells for Heart Repair. Adv. Healthc. Mater. 2018, 7, e1800672. [Google Scholar] [CrossRef]
- Park, S.-J.; Kim, R.Y.; Park, B.-W.; Lee, S.; Choi, S.W.; Park, J.-H.; Choi, J.J.; Kim, S.-W.; Jang, J.; Cho, D.-W.; et al. Dual stem cell therapy synergistically improves cardiac function and vascular regeneration following myocardial infarction. Nat. Commun. 2019, 10, 3123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birla, R.K.; Williams, S.K. 3D bioprinting and its potential impact on cardiac failure treatment: An industry perspective. APL Bioeng. 2020, 4, 010903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doss, M.X.; Sachinidis, A. Current Challenges of iPSC-Based Disease Modeling and Therapeutic Implications. Cells 2019, 8, 403. [Google Scholar] [CrossRef] [Green Version]
- Roche, C.D.; Brereton, R.J.L.; Ashton, A.W.; Jackson, C.; Gentile, C. Current challenges in three-dimensional bioprinting heart tissues for cardiac surgery. Eur. J. Cardio-Thorac. Surg. 2020, 58, 500–510. [Google Scholar] [CrossRef]
- Ruiz-Alonso, S.; Villate-Beitia, I.; Gallego, I.; Lafuente-Merchan, M.; Puras, G.; Saenz-Del-Burgo, L.; Pedraz, J. Current Insights Into 3D Bioprinting: An Advanced Approach for Eye Tissue Regeneration. Pharmaceutics 2021, 13, 308. [Google Scholar] [CrossRef] [PubMed]
- Jakab, K.; Norotte, C.; Marga, F.; Murphy, K.; Vunjak-Novakovic, G.; Forgacs, G. Tissue engineering by self-assembly and bio-printing of living cells. Biofabrication 2010, 2, 022001. [Google Scholar] [CrossRef] [PubMed]
- Xin, Y.; Chai, G.; Zhang, T.; Wang, X.; Qu, M.; Tan, A.; Bogari, M.; Zhu, M.; Lin, L.; Hu, Q.; et al. Analysis of multiple types of human cells subsequent to bioprinting with electrospraying technology. Biomed. Rep. 2016, 5, 723–730. [Google Scholar] [CrossRef] [Green Version]
- Pina, S.; Ribeiro, V.P.; Marques, C.F.; Maia, F.R.; Silva, T.H.; Reis, R.L.; Oliveira, J.M. Scaffolding Strategies for Tissue Engineering and Regenerative Medicine Applications. Materials 2019, 12, 1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, B.; Liu, J.; Dvir, T.; Jin, L.; Tsui, J.H.; Qing, Q.; Suo, Z.; Langer, R.; Kohane, D.S.; Lieber, C.M. Macroporous nanowire nanoelectronic scaffolds for synthetic tissues. Nat. Mater. 2012, 11, 986–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.R.; Jung, S.M.; Zalabany, M.; Kim, K.; Zorlutuna, P.; Kim, S.B.; Nikkhah, M.; Khabiry, M.; Azize, M.; Kong, J. Carbon-nanotube-embedded hydrogel sheets for engineering cardiac constructs and bioactuators. ACS Nano 2013, 7, 2369–2380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, J.; Visintini, S.; Quay, T. An Overview of Clinical Applications of 3-D Printing and Bioprinting. In CADTH Issues in Emerging Health Technologies; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2016. Available online: http://www.ncbi.nlm.nih.gov/books/NBK542711/ (accessed on 1 September 2021).
- Nyga, A.; Cheema, U.; Loizidou, M. 3D tumour models: Novel in vitro approaches to cancer studies. J. Cell Commun. Signal. 2011, 5, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Ware, M.J.; Keshishian, V.; Law, J.J.; Ho, J.C.; Favela, C.A.; Rees, P.; Smith, B.; Mohammad, S.; Hwang, R.F.; Rajapakshe, K.; et al. Generation of an in vitro 3D PDAC stroma rich spheroid model. Biomaterials 2016, 108, 129–142. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kang, K.; Drogemuller, C.J.; Wallace, G.G.; Coates, P.T. Bioprinting an Artificial Pancreas for Type 1 Diabetes. Curr. Diab. Rep. 2019, 19, 53. [Google Scholar] [CrossRef] [PubMed]
- Gan, M.J.; Albanese-O’Neill, A.; Haller, M.J. Type 1 diabetes: Current concepts in epidemiology, pathophysiology, clinical care, and research. Curr. Probl. Pediatr. Adolesc. Health Care 2012, 42, 269–291. [Google Scholar] [CrossRef] [PubMed]
- Cibulskis, R.E.; Alonso, P.; Aponte, J.; Aregawi, M.; Barrette, A.; Bergeron, L.; Fergus, C.A.; Knox, T.; Lynch, M.; Patouillard, E.; et al. Malaria: Global progress 2000–2015 and future challenges. Infect. Dis. Poverty 2016, 5, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravnic, D.J.; Leberfinger, A.N.; Ozbolat, I.T. Bioprinting and Cellular Therapies for Type 1 Diabetes. Trends Biotechnol. 2017, 35, 1025–1034. [Google Scholar] [CrossRef]
- Holstein, A.; Plaschke, A.; Egberts, E.-H. Clinical characterisation of severe hypoglycaemia––A prospective population—Based study. Exp. Clin. Endocrinol. Diabetes 2003, 111, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Fong, E.L.S.; Harrington, D.A.; Farach–Carson, M.C.; Yu, H. Heralding a new paradigm in 3D tumor modeling. Biomaterials 2016, 108, 197–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, Y.; Mukohara, T.; Shimono, Y.; Funakoshi, Y.; Chayahara, N.; Toyoda, M.; Kiyota, N.; Takao, S.; Kono, S.; Nakatsura, T.; et al. Comparison of 2D- and 3D-culture models as drug—Testing platforms in breast cancer. Oncol. Rep. 2015, 33, 1837–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, L.; Shestov, A.A.; Swain, P.; Yang, C.; Parker, S.J.; Wang, Q.A.; Terada, L.S.; Adams, N.D.; McCabe, M.T.; Pietrak, B.; et al. Reductive carboxylation supports redox homeostasis during anchorage–independent growth. Nature 2016, 532, 255–258. [Google Scholar] [CrossRef]
- Langer, E.M.; Allen–Petersen, B.L.; King, S.M.; Kendsersky, N.D.; Turnidge, M.A.; Kuziel, G.M.; Riggers, R.; Samatham, R.; Amery, T.S.; Jacques, S.L.; et al. Modeling Tumor Phenotypes In Vitro with Three–Dimensional Bioprinting. Cell Rep. 2019, 26, 608–623.e6. [Google Scholar] [CrossRef] [Green Version]
- Noel, P.; Muñoz, R.; Rogers, G.W.; Neilson, A.; Von Hoff, D.D.; Han, H. Preparation and Metabolic Assay of 3-dimensional Spheroid Co-cultures of Pancreatic Cancer Cells and Fibroblasts. J. Vis. Exp. JoVE 2017, 126, 56081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, S.; Tiriac, H.; Sridharan, B.P.; Scampavia, L.; Madoux, F.; Seldin, J.; Souza, G.R.; Watson, D.; Tuveson, D.; Spicer, T.P.; et al. Advanced Development of Primary Pancreatic Organoid Tumor Models for High-Throughput Phenotypic Drug Screening. SLAS Discov. Adv. Life. Sci. R D 2018, 23, 574–584. [Google Scholar] [CrossRef] [Green Version]
- Hakobyan, D.; Médina, C.; Dusserre, N.; Stachowicz, M.-L.; Handschin, C.; Fricain, J.-C.; Guillermet-Guibert, J.; Oliveira, H. Laser-assisted 3D bioprinting of exocrine pancreas spheroid models for cancer initiation study. Biofabrication 2020, 12, 035001. [Google Scholar] [CrossRef] [PubMed]
- Farina, M.; Ballerini, A.; Fraga, D.W.; Nicolov, E.; Hogan, M.; Demarchi, D.; Scaglione, F.; Sabek, O.M.; Horner, P.; Thekkedath, U.; et al. 3D Printed Vascularized Device for Subcutaneous Transplantation of Human Islets. Biotechnol. J. 2017, 12, 1700169. [Google Scholar] [CrossRef]
- Baidal, D.A.; Ricordi, C.; Berman, D.M.; Alvarez, A.; Padilla, N.; Ciancio, G.; Linetsky, E.; Pileggi, A.; Alejandro, R. Bioengineering of an Intraabdominal Endocrine Pancreas. N. Engl. J. Med. 2017, 376, 1887–1889. [Google Scholar] [CrossRef] [Green Version]
- Xiongfa, J.; Hao, Z.; Liming, Z.; Jun, X. Recent advances in 3D bioprinting for the regeneration of functional cartilage. Regen. Med. 2018, 13, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Murray, I.R.; Benke, M.T.; Mandelbaum, B.R. Management of knee articular cartilage injuries in athletes: Chondroprotection, chondrofacilitation, and resurfacing. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1617–1626. [Google Scholar] [CrossRef]
- Wu, Y.; Kennedy, P.; Bonazza, N.; Yu, Y.; Dhawan, A.; Ozbolat, I. Three-Dimensional Bioprinting of Articular Cartilage: A Systematic Review. Cartilage 2021, 12, 76–92. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, A.; Kennedy, P.M.; Rizk, E.B.; Ozbolat, I.T. Three-dimensional Bioprinting for Bone and Cartilage Restoration in Orthopaedic Surgery. J. Am. Acad. Orthop. Surg. 2019, 27, e215–e226. [Google Scholar] [CrossRef]
- Kamran, A.; Jennings, R.W. Tracheomalacia and Tracheobronchomalacia in Pediatrics: An Overview of Evaluation, Medical Management, and Surgical Treatment. Front. Pediatr. 2019, 7, 512. [Google Scholar] [CrossRef] [Green Version]
- Galliger, Z.; Vogt, C.D.; Panoskaltsis-Mortari, A. 3D bioprinting for lungs and hollow organs. Transl. Res. 2019, 211, 19–34. [Google Scholar] [CrossRef]
- Jeong, H.-J.; Nam, H.; Jang, J.; Lee, S.-J. 3D Bioprinting Strategies for the Regeneration of Functional Tubular Tissues and Organs. Bioengineering 2020, 7, 32. [Google Scholar] [CrossRef] [Green Version]
- Frejo, L.; Grande, D.A. 3D-bioprinted tracheal reconstruction: An overview. Bioelectron. Med. 2019, 5, 15. [Google Scholar] [CrossRef] [Green Version]
- Kaye, R.; Goldstein, T.; Grande, D.A.; Zeltsman, D.; Smith, L.P. A 3-dimensional bioprinted tracheal segment implant pilot study: Rabbit tracheal resection with graft implantation. Int. J. Pediatr. Otorhinolaryngol. 2019, 117, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Ng, W.L.; Chua, C.K.; Shen, Y.-F. Print Me An Organ! Why We Are Not There Yet. Prog. Polym. Sci. 2019, 97, 101145. Available online: https://www.sciencedirect.com/science/article/pii/S007967001930156X (accessed on 1 September 2021). [CrossRef]
- Favreau, H.; Pijnenburg, L.; Seitlinger, J.; Fioretti, F.; Keller, L.; Scipioni, D.; Adriaensen, H.; Kuchler-Bopp, S.; Ehlinger, M.; Mainard, D.; et al. Osteochondral repair combining therapeutics implant with mesenchymal stem cells spheroids. Nanomed. Nanotechnol. Biol. Med. 2020, 29, 102253. [Google Scholar] [CrossRef]
- Francis, S.L.; Di Bella, C.; Wallace, G.G.; Choong, P.F.M. Cartilage Tissue Engineering Using Stem Cells and Bioprinting Technology-Barriers to Clinical Translation. Front. Surg. 2018, 5, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fellows, C.R.; Matta, C.; Zakany, R.; Khan, I.M.; Mobasheri, A. Adipose, Bone Marrow and Synovial Joint-Derived Mesenchymal Stem Cells for Cartilage Repair. Front. Genet. 2016, 7, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.H.; Tuan, R.S. Mesenchymal stem cells in arthritic diseases. Arthritis Res. Ther. 2008, 10, 223. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Choudhury, D.; Yu, F.; Mironov, V.; Naing, M.W. In situ bioprinting—Bioprinting from benchside to bedside? Acta Biomater. 2020, 101, 14–25. [Google Scholar] [CrossRef]
- O’Connell, C.D.; Di Bella, C.; Thompson, F.; Augustine, C.; Beirne, S.; Cornock, R.; Richards, C.J.; Chung, J.; Gambhir, S.; Yue, Z.; et al. Development of the Biopen: A handheld device for surgical printing of adipose stem cells at a chondral wound site. Biofabrication 2016, 8, 015019. [Google Scholar] [CrossRef]
- Ma, K.; Zhao, T.; Yang, L.; Wang, P.; Jin, J.; Teng, H.; Xia, D.; Zhu, L.; Li, L.; Jiang, Q.; et al. Application of robotic-assisted in situ 3D printing in cartilage regeneration with HAMA hydrogel: An in vivo study. J. Adv. Res. 2020, 23, 123–132. [Google Scholar] [CrossRef]
- You, F.; Chen, X.; Cooper, D.M.L.; Chang, T.; Eames, B.F. Homogeneous hydroxyapatite/alginate composite hydrogel promotes calcified cartilage matrix deposition with potential for three-dimensional bioprinting. Biofabrication 2018, 11, 015015. [Google Scholar] [CrossRef]
- Kosik-Kozioł, A.; Costantini, M.; Mróz, A.; Idaszek, J.; Heljak, M.; Jaroszewicz, J.; Kijeńska-Gawrońska, E.; Szöke, K.; Frerker, N.; Barbetta, A.; et al. 3D bioprinted hydrogel model incorporating β-tricalcium phosphate for calcified cartilage tissue engineering. Biofabrication 2019, 11, 035016. [Google Scholar] [CrossRef]
- Park, J.-H.; Yoon, J.-K.; Lee, J.B.; Shin, Y.M.; Lee, K.-W.; Bae, S.-W.; Lee, J.; Yu, J.; Jung, C.-R.; Youn, Y.-N.; et al. Experimental Tracheal Replacement Using 3-dimensional Bioprinted Artificial Trachea with Autologous Epithelial Cells and Chondrocytes. Sci. Rep. 2019, 9, 2103. [Google Scholar] [CrossRef]
- Ke, D.; Yi, H.; Est-Witte, S.; George, S.; Kengla, C.; Lee, S.J.; Atala, A.; Murphy, S.V. Bioprinted trachea constructs with patient-matched design, mechanical and biological properties. Biofabrication 2019, 12, 015022. [Google Scholar] [CrossRef]
- Jafarkhani, M.; Salehi, Z.; Aidun, A.; Shokrgozar, M.A. Bioprinting in Vascularization Strategies. Iran. Biomed. J. 2019, 23, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. Available online: https://www.mdpi.com/1420-3049/26/10/3007 (accessed on 1 September 2021). [CrossRef] [PubMed]
- Bisht, B.; Hope, A.; Mukherjee, A.; Paul, M.K. Advances in the Fabrication of Scaffold and 3D Printing of Biomimetic Bone Graft. Ann. Biomed. Eng. 2021, 49, 1128–1150. [Google Scholar] [CrossRef]
- Roseti, L.; Cavallo, C.; Desando, G.; Parisi, V.; Petretta, M.; Bartolotti, I.; Grigolo, B. Three-Dimensional Bioprinting of Cartilage by the Use of Stem Cells: A Strategy to Improve Regeneration. Materials 2018, 11, 1749. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6164915/ (accessed on 1 September 2021).
- Datta, P.; Dey, M.; Ataie, Z.; Unutmaz, D.; Ozbolat, I.T. 3D bioprinting for reconstituting the cancer microenvironment. NPJ Precis Oncol. 2020, 4, 18. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Tissue | Cell Type | Biomaterial | Printed Model | Outcome | Reference |
|---|---|---|---|---|---|
| Skin | |||||
| 2016–2018 | |||||
| Human dermal endothelial cells | Sodium alginate, chitosan, gelatin, gellan gum, collagen I (core materials), pure alginate (shell material) | Core/shell construct |
| Akkineni et al. 2016 | |
| Human fibroblasts (hFB) and keratinocytes (hKC) obtained from skin biopsies of healthy donors | Plasma-derived fibrin scaffold | Skin: dermis + epidermis |
| Cubo et al. 2016 | |
| Human primary dermal fibroblasts, human primary epidermal keratinocytes | Newly-developed ECM-like bioInk | Skin model |
| Rimann et al. 2016 | |
| Amniotic fluid-derived stem (AFS) cells | Photo-cross-linkable heparin-conjugated hyaluronic acid (HA-HP) hydrogel | In situ skin graft |
| Skardal et al. 2016 | |
| Fibroblasts | Collagen hydrogel | Dermal construct |
| Hou et al. 2017 | |
| Human fibroblasts and human keratinocytes | Unique bioink of alginate, gelatin, fibrinogen | Skin: dermis + epidermis |
| Pourchet et al. 2017 | |
| Human primary skin cells (fibroblasts and keratinocytes) | Collagen, gelatin. PCL (prevents collagen shrinkage) | Skin: dermis + epidermis |
| Kim et al. 2017 | |
| Keratinocytes (KCs), melanocytes (MCs) and fibroblasts (FBs) (from three different Caucasian skin donors) | Collagen, PVP (Polyvinylpyrrolidone) polymer | Pigmented skin: bioprinting vs. manual-cast approach |
| Ng et al. 2018 | |
| Endothelial progenitor cells (EPCs) and adipose-derived stem cells (ASCs) added to HDF (human dermal fibroblast) and HEK (human epidermal keratinocyte) | Skin-derived extracellular matrix (S-dECM) bioink, collagen I matrix (as a control) | Skin patch |
| Kim et al. 2018 | |
| Fibroblasts, melanocytes and keratinocytes | Collagen hydrogel | Pigmented skin model (dermal + epidermal layer) |
| Min et al. 2018 | |
| Human melanocytes (HEM), human keratinocytes (HaCat) and human dermal fibroblasts (HDF) | Gelatin methacrylamide (GelMA) and collagen (Col)+ tyrosinase (Ty) | Living skin model |
| Shi et al. 2018 | |
| 2019–2020 | |||||
| Fibroblasts and keratinocytes | Hydrogel (fibrinogen, collagen I, trombin) | In situ skin bioprinting |
| Albanna et al. 2019 | |
| Neonatal human dermal fibroblasts and neonatal normal human epithelial keratinocytes | Gelatin, fibrinogen, collagen, elastin (dermal hydrogel) | Skin equivalent |
| Derr et al. 2019 | |
| Human fibroblasts, keratinocytes, human umbilical vein endothelial cells (HUVECs), preadipocytes | dECM-based bioinks, gelatin hydrogel. PCL transwell system (supportive mesh) | A vascularized tri-layered skin model (epidermis, dermis, and hypodermis) |
| Kim et al. 2019 | |
| Human amniotic epithelial cells (AECs), Wharton’s jelly-derived mesenchymal stem cells (WJMSCs) | Alginate/gelatin composite hydrogels | Skin bilayered construct |
| Liu et al. 2019 | |
| No cells | PCL and silk sericin for epidermis + CS_SA hydrogel for dermis (CS, chitosan; SA, sodium alginate) | Composite skin construct: three-dimensional skin asymmetric construct (3D_SAC) |
| Miguel et al. 2019 | |
| Human dermal fibroblasts (HDFs) | Skin decellularized extracellular matrix (dECM) | Bioprinted 3D construct |
| Won et al. 2019 | |
| Neonatal human dermal fibroblasts (NHDFs), immortalized human keratinocyte cell line (HaCaT) and human umbilical vein endothelial cells (HUVECs) | Methacrylated gelatin (GelMA) and succinylated chitosan/dextran aldehyde | Prevascularized core/shell construct for wound healing |
| Turner et al. 2020 | |
| Human-derived skin fibroblasts (hSF) | Bioink made of nanofibrillated cellulose (NFC), alginate (ALG) and carboxymethyl cellulose (CMC) | Dermal construct |
| Zidaric et al. 2020 | |
| Tissue | Cell Type | Biomaterial | Printed Model | Outcome | Reference |
|---|---|---|---|---|---|
| Heart | |||||
| 2016–2018 | |||||
| HUVECs, neonatal rat CMs/ hiPSCs-CMs | Alginate and GelMa | Endothelialized-myocardium-on-a-chip model |
| Zhang et al. 2016 | |
| Human adipose derived mesenchymal stem cells (HADMSC), aortic valve interstitial cells (HAVIC) and aortic valve sinus smooth muscle cells (HASSMC) | Mixture of methacrylated gelatin/polyethylene glycol diacrylate/alginate (MEGEL/PEGDA 3350/alginate) | 3D-bioprinted hydrogels for cardiac valve |
| Kang et al. 2017 | |
| Human coronary artery endothelial cells | Sodium alginate | Cardiac constructs (different architectures) |
| Izadifar et al. 2017 | |
| hiPSC-CMs, FBs, ECs | Scaffold-free | Patch |
| Ong et al. 2017 | |
| hiPSC-CMs, human dermal FB and EC (HUVECs) | Scaffold-free | Tubular cardiac constructs made of cardiac spheroid |
| Arai et al. 2018 | |
| Rat primary cardiomyocytes | Fibrin cell-laden hydrogel, sacrificial hydrogel and a PCL supporting frame | Patch |
| Wang et al. 2018 | |
| hCPCs, cECM | Decellularized cardiac extracellular matrix hydrogel (cECM) and gelatin methacrylate (GelMA) | Patch |
| Bejleri et al. 2018 | |
| Bone marrow- derived human mesenchymal stem cell (hMSCs), neonatal rat CMs | Gelatin hydrogel | Patterned gelatin hydrogel 3D bioprinted grid |
| Tijore et al. 2018 | |
| Human coronary artery endothelial cells (HCAECs) | Carboxyl functionalized carbon nanotubes (CNTs) incorporated alginate framework and cell-laden methacrylated collagen (MeCol) | Nanoreinforced hybrid cardiac patch |
| Izadifar et al. 2018 | |
| 2019–2020 | |||||
| iPSCs-derived CMs and ECs (patient-specific) | Patient-specific hydrogel (collagen/ECM) | Patient-specifically designed patch |
| Noor et al. 2019 | |
| hESC-CMs and cardiac FBs | Collagen | Left ventricle model, tricuspid heart valve |
| Lee et al. 2019 | |
| hiPSC-CMs, FB and EC | Scaffold-free | Patch |
| Yeung et al. 2019 | |
| hiPSC-CMs | Photo-cross-linkable cardiac dECM | Biomimetically patterned construct |
| Yu et al. 2019 | |
| Wnt-activated hiPSC-cardiomyocytes, hiPSC-cardiomyocytes | GelMA and 0.3% (wt/vol) lithium phenyl-2 4 6-trimethylbenzoylphosphinate (LAP) | hPSC-derived cardiomyocyte mini hearts |
| Ren et al. 2019 | |
| hiPSC-CM and normal human cardiac fibroblasts (NHCFs) coated with fibronectin and gelatin | Fibrinogen and hyaluronic acid | Layer-by-layer heart construct hiPSC-CM-derived |
| Chikae et al. 2019 | |
| iPSCs-derived CMs, ECs | Photo-cross-linkable bioink of ECM proteins and GelMa | Chambered cardiac pump |
| Kupfer et al. 2020 | |
| Tissue | Cell Type | Biomaterial | Printed Model | Outcome | Reference |
|---|---|---|---|---|---|
| Pancreas | |||||
| Human pancreatic islet cells | Polylactic acid functionalized with growth factor-enriched platelet gel | 3D printed construct |
| Farina et al. 2017 | |
| Pancreatic cancer cells (Patu8902) and activated pancreatic fibroblast cells (PS1) | Nanoshuttle (NS) composed of iron oxide, poly L-lysine and gold nanoparticles | In vitro pancreatic tumor model |
| Noel et al. 2017 | |
| Human colorectal adenocarcinoma cell line HT-29, human pancreatic epithelial carcinoma cell line PANC-1 | Nanoshuttle (NS) composed of iron oxide, poly L-lysine and gold nanoparticles | Primary pancreatic organoid tumor models |
| Hou et al. 2018 | |
| Pancreatic cancer cell lines, i.e., MIA PaCa-2 and PANC-1 | NanoShuttle nanoparticles (Nano3D Biosciences Inc., Houston, TX, USA) | Spheroids from MIA PaCa-2 and PANC-1 cells, mixed with human fibroblasts in a ratio of 1:1, and incubated with NanoShuttle nanoparticles |
| Daunys et al. 2019 | |
| Human primary pancreatic stellate cells (PSCs), human umbilical vein endothelial cells (HUVECs), HMF, subcutaneous preadipocytes(SPA), and MCF-7 cells | Alginate-containing hydrogel |
| Langer et al. 2019 | ||
| AR42J-B-13 rat acinar cell line | Methacrylated gelatin (GELMA) | Laser-assisted bioprinted 3D pancreatic cell spheroid arrays |
| Hakobyan et al. 2020 |
| Tissue | Cell Type | Biomaterial | Printed Model | Outcome | Reference |
|---|---|---|---|---|---|
| Cartilage | |||||
| 2016–2018 | |||||
| Rabbit ear chondrocytes | PCL, gelatin, fibrinogen, HA (hyaluronic acid) | PCL and chondrocytes laden scaffold |
| Kang HW et al. 2016 | |
| hMSC | Nanocrystalline hydroxyapatite | Scaffold |
| Nowicki et al. 2016 | |
| Human mesenchymal stem cell | 2D nanosilicate reinforced kappa-carrageenan (κCA) hydrogels | Hydrogel scaffold |
| Thakur et al. 2016 | |
| Human mesenchymal stem cells (hMSCs) | Poly(ethylene) glycol diacrylate (PEGDA)/acrylated peptides/I-2959 photoinitiator | bioprinted 3D construct |
| Gao et al. 2016 | |
| Human adipose stem cells | Gelatin–methacrylamide/hyaluronic acid–methacrylate (GelMa/HAMa) hydrogel | Hand-made 3D Scaffold |
| O’Connell et al. 2016 | |
| hMSCs and human nasal chondrocytes | Nanofibrillated cellulose and alginate | 5 × 5 × 1.2 m biological construct |
| Apelgren P. et al. 2017 | |
| iPSCs | Nanofibrillated cellulose and alginate (NFC/A) or hyaluronic acid (NFC/HA) | Scaffold |
| Nguyen D. et al. 2017 | |
| Chondrocytes | Methacrylated hyaluronic acid (HAMA) + methacrylated poly[N-(2-hydroxypropyl) methacrylamide mono/dilactate] (pHPMA-lac)/polyethylene glycol (PEG) + polycaprolactone (PCL) | Scaffold |
| Mouser et al. 2017 | |
| Human and equine mesenchymal stem cells (hMSCs) | Hyaluronic acid/poly(glycidol) and poly(ε-caprolactone) | Bioprinted 3D construct |
| Stichler et al. 2017 | |
| Human embryonic kidney (HEK) cells and ovine mesenchymal stem cells (oMSCs) | 8:1 v:v mixture of ULGT-agarose solution to Fmoc-dipeptide solution, with or without collagen | High-resolution patterned 3D cellular constructs |
| Graham et al. 2017 | |
| MSCs | GelMA + PEGDA + TGF-β1 embedded in nanospheres | Stereolithography Scaffold |
| Zhu et al. 2018 | |
| hADSCs | GelMa + hyaluronic acid methacrylate | Scaffold with Biopen |
| Onofrillo et al. 2018 | |
| hMSCs | Poly (l-lactide-co-caprolactone) + poly (lactic-co-glycolic acid) + Aggrecan | Scaffold |
| Guo et al. 2018 | |
| Human chondrocyte | Gelatin methacryloyl bioink | Three-dimensional disks |
| Gu et al. 2018 | |
| Mesenchymal stem cells (MSCs) | Gelatin methacrylamide (GelMa) and hyaluronic acid methacrylate (HAMA) hydrogel | Hand-made 3D Scaffold |
| Di Bella et al. 2018 | |
| 2019–2020 | |||||
| Human chondrocytes | Polylactic acid | Reticular layered scaffold |
| Baena J.M. et al. 2019 | |
| BM-MSCs | Scaffold-free | Spheroid |
| Breathwaite E.K. et al. 2019 | |
| Human mesenchymal stem cells (hMSCs) | Polycaprolactone (PCL) | Bioprinted 3D tracheal shape construct |
| Dongxu et al. 2019 | |
| hMSCs and hACs (human artificial chromosomes) | GelMa + CS-AEMA (chondroitin sulfate amino ethyl methacrylate) Hyaluronic acid (HC) + TCP (tricalcium phosphate) microparticles | Reticular layered scaffold |
| Idaszek J. et al. 2019 | |
| hMSC | PCL | Scaffold |
| Ke et al. 2019 | |
| ATDC5 cells | Oxidized hyaluronate (OHA), oxidized hyaluronate (OHA), oxidized hyaluronate (OHA) | Scaffold |
| Kim et al. 2019 | |
| BM-MSCs | β-tricalcium phosphate (TCP) | 3D biomimetic hydrogel scaffold |
| Kosik-Kozioł et al. 2019 | |
| hADSCs | hydroxybutyl chitosan (HBC) + oxidized chondroitin sulfate (OCS) Hydrogel | Macroporous hydrogel scaffold |
| Li et al. 2019 | |
| Human cartilage cells + human fibroblasts + human umbilical vein endothelial cells + human mesenchymal stem cells | Culture medium | Spheroid |
| Machino et al. 2019 | |
| MSCs | Cartilage extracellular matrix (cECM)-functionalized alginate bioink | Scaffold |
| Rathan et al. 2019 | |
| hMSCs | PEGDA | GDF5-conjugated BMSC laden scaffold |
| Sun et al. 2019 | |
| No cells used | CTGF (connective tissue growth factor) + TGFβ3 (transforming growth factor beta 3) + BMP2 (Bone Morphogenetic protein 2). All these growth factors are encapsulated in PLGA—poly(lactic-co-glycolic acid) scaffold | Thin membrane-like scaffold |
| Tarafder S et al. 2019 | |
| Human auricular chondrocytes (hACs) | poly(2-ethyl-2-oxazoline) (PEOXA)-peptide conjugates + sortase A (SA) + alginate + cellulose nanofibrils (CNF) | Scaffold |
| Trachsel et al. 2019 | |
| ADSCs | Alginate support | Spheroid |
| Ayan et al. 2020 | |
| Ovine fetal chondrocytes | Collagen I + fibrin glue | Scaffold |
| Dasargyri et al. 2020 | |
| hADSCs | 10%GelMa/2%HAMa Hydrogel | Core/shell bioscaffold |
| Duchi et al. 2020 | |
| hMSC | Calcium phosphate cement (CPC) + alginate-methylcellulose (algMC) | Scaffold |
| Kilian et al. 2020 | |
| Human adipose tissue-derived mesenchymal stem cells (hADMSCs) | Photo-cross-linkable alginate + gelatin and chondroitin sulfate + graphene oxide | Scaffold |
| Olate Moya et al. 2020 | |
| ADSCs | GelMA + PEGDA coated with lysine-rosette nanotubes (RNTK) | Lysine-functionalized rosette nanotubes scaffold |
| Zohu et al. 2020 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Piazza, E.; Pandolfi, E.; Cacciotti, I.; Del Fattore, A.; Tozzi, A.E.; Secinaro, A.; Borro, L. Bioprinting Technology in Skin, Heart, Pancreas and Cartilage Tissues: Progress and Challenges in Clinical Practice. Int. J. Environ. Res. Public Health 2021, 18, 10806. https://doi.org/10.3390/ijerph182010806
Di Piazza E, Pandolfi E, Cacciotti I, Del Fattore A, Tozzi AE, Secinaro A, Borro L. Bioprinting Technology in Skin, Heart, Pancreas and Cartilage Tissues: Progress and Challenges in Clinical Practice. International Journal of Environmental Research and Public Health. 2021; 18(20):10806. https://doi.org/10.3390/ijerph182010806
Chicago/Turabian StyleDi Piazza, Eleonora, Elisabetta Pandolfi, Ilaria Cacciotti, Andrea Del Fattore, Alberto Eugenio Tozzi, Aurelio Secinaro, and Luca Borro. 2021. "Bioprinting Technology in Skin, Heart, Pancreas and Cartilage Tissues: Progress and Challenges in Clinical Practice" International Journal of Environmental Research and Public Health 18, no. 20: 10806. https://doi.org/10.3390/ijerph182010806