Post-Traumatic Stress Symptoms in Healthcare Workers Dealing with the COVID-19 Pandemic: A Systematic Review

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
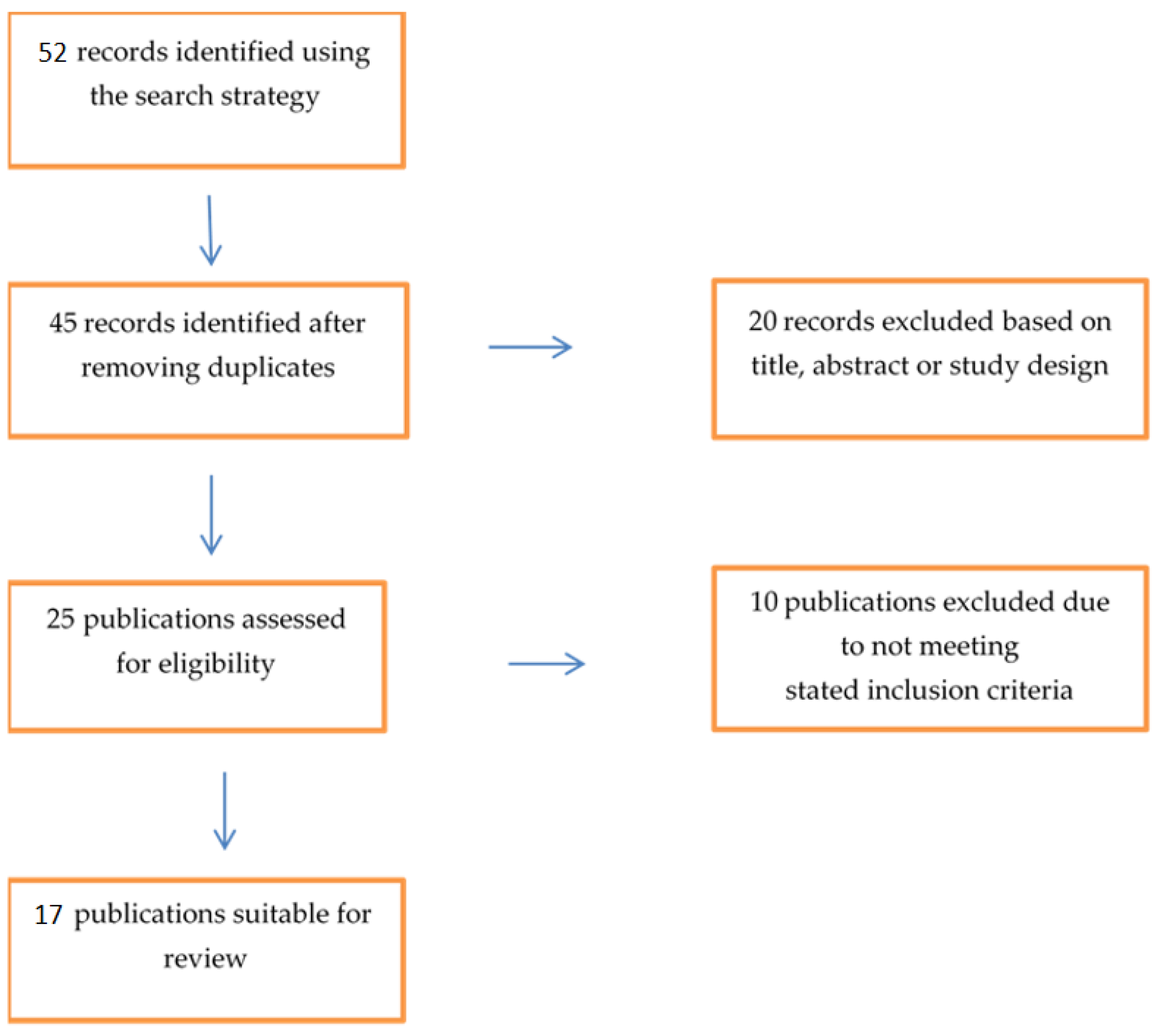
2.1. Search Strategy
2.2. Data Extraction
2.3. Categorization of Selected Articles
3. Results
4. Discussion
4.1. Risk Assessment of Work-Related PTSS
4.2. Risk Management of PTSS
4.3. Occurrence of PTSS
4.4. A Call for Action
5. Limits of the Study
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Garzaro, G.; Clari, M.; Ciocan, C.; Grillo, E.; Mansour, I.; Godono, A.; Borgna, L.G.; Sciannameo, V.; Costa, G.; Raciti, I.M.; et al. COVID-19 infection and diffusion among the healthcare workforce in a large university-hospital in northwest Italy. Med. Lav. 2020, 111, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Ying, Y.; Ruan, L.; Kong, F.; Zhu, B.; Ji, Y.; Lou, Z. Mental health status among family members of health care workers in Ningbo, China, during the coronavirus disease 2019 (COVID-19) outbreak: A cross-sectional study. BMC Psychiatry 2020, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.R.; Wang, K.; Yin, L.; Zhao, W.F.; Xue, Q.; Peng, M.; Min, B.Q.; Tian, Q.; Leng, H.X.; Du, J.L.; et al. Mental health and psychosocial problems of medical health workers during the COVID-19 epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef]
- Carmassi, C.; Cerveri, G.; Bui, E.; Gesi, C.; Dell’Osso, L. Defining Effective Strategies to Prevent Post-Traumatic Stress in Healthcare Emergency Workers Facing the COVID-19 Pandemic in Italy. CNS Spectr. 2020, 25, 293–294. [Google Scholar] [CrossRef]
- Bai, Y.; Lin, C.C.; Lin, C.Y.; Chen, J.Y.; Chue, C.M.; Chou, P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr. Serv. 2004, 55, 1055–1057. [Google Scholar] [CrossRef]
- Lee, S.M.; Kang, W.S.; Cho, A.R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Xiao, X.; Zhu, X.; Fu, S.; Hu, Y.; Li, X.; Xiao, J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: A multi-center cross-sectional survey investigation. J. Affect. Disord. 2020, 274, 405–410. [Google Scholar] [CrossRef]
- Dutheil, F.; Mondillon, L.; Navel, V. PTSD as the second tsunami of the SARS-Cov-2 pandemic. Psychol. Med. 2020, 33, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Peters, L.; Slade, T.; Andrews, G. A comparison of ICD10 and DSM-IV criteria for posttraumatic stress disorder. J. Trauma Stress. 1999, 12, 335–343. [Google Scholar] [CrossRef]
- American Pyschiatric Association. Sleep-Wake Disorders. Available online: http://www.dsm5.org/ (accessed on 10 November 2020).
- WHO. Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide. 2017. Available online: https://www.who.int/alliance-hpsr/resources/publications/rapid-review-guide/en/ (accessed on 10 November 2020).
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 October 2020).
- Moher, D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264. [Google Scholar] [CrossRef] [Green Version]
- Arnetz, J.E.; Goetz, C.M.; Sudan, S.; Arble, E.; Janisse, J.; Arnetz, B.B. Personal Protective Equipment and Mental Health Symptoms Among Nurses During the COVID-19 Pandemic. J. Occup. Environ. Med. 2020, 62, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, L.P.G.; Arriaga, R.J.M.; Hernández-Gonzalez, M.A.; De la Roca-Chiapas, J.M. Psychological Distress and Signs of Post-Traumatic Stress in Response to the COVID-19 Health Emergency in a Mexican Sample. Psychol. Res. Behav. Manag. 2020, 13, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.; Ngiam, J.N.; Tan, B.Y.Q.; Tham, S.M.; Tan, C.Y.; Jing, M.; Sagayanathan, R.; Chen, J.T.; Wong, L.Y.H.; Ahmad, A.; et al. Asian-Pacific perspective on the psychological well-being of healthcare workers during the evolution of the COVID-19 pandemic. BJPsych. Open 2020, 6, e116. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.Y.Q.; Chew, N.W.S.; Lee, G.K.H.; Jing, M.; Goh, Y.; Yeo, L.L.L.; Zhang, K.; Chin, H.K.; Ahmad, A.; Khan, F.A.; et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 2020, 173, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Khasne, R.W.; Dhakulkar, B.S.; Mahajan, H.C.; Kulkarni, A.P. Burnout among Healthcare Workers during COVID-19 Pandemic in India: Results of a Questionnaire-based Survey. Indian J. Crit. Care Med. 2020, 24, 664–671. [Google Scholar] [CrossRef]
- Song, X.; Fu, W.; Liu, X.; Luo, Z.; Wang, R.; Zhou, N.; Yan, S.; Lv, C. Mental health status of medical staff in emergency departments during the Coronavirus disease 2019 epidemic in China. Brain Behav. Immun. 2020, 88, 60–65. [Google Scholar] [CrossRef]
- Wang, Y.X.; Guo, H.T.; Du, X.W.; Song, W.; Lu, C.; Hao, W.N. Factors associated with post-traumatic stress disorder of nurses exposed to corona virus disease 2019 in China. Medicine 2020, 99, e20965. [Google Scholar] [CrossRef]
- Si, M.; Su, X.; Jiang, Y.; Wang, W.; Gu, X.F.; Ma, L.; Li, J.; Zhang, S.K.; Ren, Z.F.; Ren, R.; et al. Psychological impact of COVID-19 on medical care workers in China. Infect. Dis. Poverty 2020, 9, 113. [Google Scholar] [CrossRef]
- Wang, Y.; Ma, S.; Yang, C.; Cai, Z.; Hu, S.; Zhang, B.; Tang, S.; Bai, H.; Guo, X.; Wu, J.; et al. Acute psychological effects of Coronavirus Disease 2019 outbreak among healthcare workers in China: A cross-sectional study. Transl. Psychiatry 2020, 13, 348. [Google Scholar] [CrossRef]
- Asaoka, H.; Koido, Y.; Kawashima, Y.; Ikeda, M.; Miyamoto, Y.; Nishi, D. Post-traumatic stress symptoms among medical rescue workers exposed to COVID-19 in Japan. Psychiatry Clin. Neurosci. 2020, 74, 503–505. [Google Scholar] [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Coping With COVID-19: Emergency Stress, Secondary Trauma and Self-Efficacy in Healthcare and Emergency Workers in Italy. Front. Psychol. 2020, 11, 566912. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Ángel Castellanos, M.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in spanish health personnel during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef] [PubMed]
- Caillet, A.; Coste, C.; Sanchez, R.; Allaouchiche, B. Psychological Impact of COVID-19 on ICU Caregivers. Anaesth. Crit. Care Pain Med. 2020, 39, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, G.J.; Ślusarska, B.; Tucholska, K.; Naylor, K.; Chrzan-Rodak, A.; Niedorys, B. The Severity of Traumatic Stress Associated with COVID-19 Pandemic, Perception of Support, Sense of Security, and Sense of Meaning in Life among Nurses: Research Protocol and Preliminary Results from Poland. Int. J. Environ. Res. Public Health 2020, 17, 6491. [Google Scholar] [CrossRef] [PubMed]
- d’Ettorre, G.; Pellicani, V.; Ceccarelli, G. Post-traumatic stress disorder symptoms in healthcare workers: A ten-year systematic review. Acta Biomed. Health Prof. 2020, 91, e2020009. [Google Scholar] [CrossRef]
- Haro, J.M.; Palacin, C.; Vilagut, G.; Martínez, M.; Bernal, M.; Luque, I.; Codony, M.; Dolz, M.; Alonso, J.; Grupo ESEMeD-España. Prevalence of mental disorders and associated factors: Results from the ESEMeD-Spain study. Med. Clin. 2006, 126, 445. [Google Scholar] [CrossRef] [Green Version]
- Neitzke, A.B. An illness of power: Sex and the social causes of depression. Cult. Med. Psychiatry 2016, 40, 59–73. [Google Scholar] [CrossRef]
- Bruine de Bruin, W. Age differences in COVID-19 risk perceptions and mental health: Evidence from a national U.S. survey conducted in March 2020. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J. Affect. Disord. 2010, 122, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Bambi, S.; Iozzo, P.; Lucchini, A. New issues in nursing management during the COVID-19 pandemic in Italy. Am. J. Crit. Care 2020, 122, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; González, A.D.; Gabani, F.L.; Andrade, S.M. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef] [PubMed]
- Adriaenssens, J.; De Gucht, V.; Maes, S. The impact of traumatic events on emergency room nurses: Findings from a questionnaire survey. Int. J. Nurs. Stud. 2012, 49, 1411–1422. [Google Scholar] [CrossRef] [PubMed]
- Somville, F.J.; De Gucht, V.; Maes, S. The impact of occupational hazards and traumatic events among Belgian emergency physicians. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 59. [Google Scholar] [CrossRef] [Green Version]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-Related Mental Health Effects in the Workplace: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef]
- Guay, S.; Beaulieu-Prévost, D.; Sader, J.; Marchand, A. A systematic literature review of early posttraumatic interventions for victims of violent crime. Aggress. Violent Behav. 2019, 46, 15–24. [Google Scholar] [CrossRef]
- Cao, J.; Wei, J.; Zhu, H.; Duan, Y.; Geng, W.; Hong, X.; Jiang, J.; Zhao, X.; Zhu, B. A study of basic needs and psychological wellbeing of medical workers in the fever clinic of a tertiary general hospital in Beijing during the COVID-19 outbreak. Psychother. Psychosom. 2020, 89, 252–254. [Google Scholar] [CrossRef]
- Theorell, T. COVID-19 and Working Conditions in Health Care. Psychother. Psychosom. 2020, 89, 193–194. [Google Scholar] [CrossRef]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [Green Version]
- Thibodeau, M.A.; Welch, P.G.; Sareen, J.; Asmundson, G.J.G. Anxiety disorders are independently associated with suicide ideation and attempts: Propensity score matching in two epidemiological samples. Depress. Anxiety 2013, 30, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Dutheil, F.; Aubert, C.; Pereira, B.; Dambrun, M.; Moustafa, F.; Mermillod, M.; Baker, J.S.; Trousselard, M.; Lesage, F.X.; Navel, V. Suicide among physicians and health-care workers: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0226361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuhr, D.C.; Acarturk, C.; McGrath, M.; Ilkkursun, Z.; Sondorp, E.; Sijbrandij, M.; Ventevogel, P.; Cuijpers, P.; McKee, M.; Roberts, B. Treatment gap and mental health service use among Syrian refugees in Sultanbeyli, Istanbul: A cross-sectional survey. Epidemiol. Psychiatr. Sci. 2019, 29, e70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovanetti, M.; Benedetti, F.; Campisi, G.; Ciccozzi, A.; Fabris, S.; Ceccarelli, G.; Tambone, V.; Caruso, A.; Angeletti, S.; Zella, D.; et al. Evolution patterns of SARS-CoV-2: Snapshot on its genome variants. Biochem. Biophys. Res. Commun. 2020. [Google Scholar] [CrossRef]
- Russo, A.; Bellelli, V.; Ceccarelli, G.; Marincola Cattaneo, F.; Bianchi, L.; Pierro, R.; Russo, R.; Steffanina, A.; Pugliese, F.; Mastroianni, C.M.; et al. Comparison Between Hospitalized Patients Affected or Not Affected by Coronavirus Disease 2019. Clin. Infect. Dis. 2020, ciaa1745. [Google Scholar] [CrossRef]
- d’Ettorre, G.; Ceccarelli, G.; Marazzato, M.; Campagna, G.; Pinacchio, C.; Alessandri, F.; Ruberto, F.; Rossi, G.; Celani, L.; Scagnolari, C. Challenges in the Management of SARS-CoV2 Infection: The Role of Oral Bacteriotherapy as Complementary Therapeutic Strategy to Avoid the Progression of COVID-19. Front. Med. (Lausanne) 2020, 7, 389. [Google Scholar] [CrossRef]
- Violi, F.; Cangemi, R.; Romiti, G.F.; Ceccarelli, G.; Oliva, A.; Alessandri, F.; Pirro, M.; Pignatelli, P.; Lichtner, M.; Carraro, A.; et al. Is Albumin Predictor of Mortality in COVID-19? Antioxid Redox Signal. 2020. [Google Scholar] [CrossRef]
- Violi, F.; Ceccarelli, G.; Cangemi, R.; Alessandri, F.; D’Ettorre, G.; Oliva, A.; Pastori, D.; Loffredo, L.; Pignatelli, P.; Ruberto, F. Hypoalbuminemia, Coagulopathy, and Vascular Disease in COVID-19. Circ. Res. 2020, 127, 400–401. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Alessandri, F.; d’Ettorre, G.; Borrazzo, C.; Spagnolello, O.; Oliva, A.; Ruberto, F.; Mastroianni, C.M.; Pugliese, F.; Venditti, M.; et al. Is teicoplanin a complementary treatment option for COVID-19? The question remains. Int. J. Antimicrob. Agents 2020, 56, 106029. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Study Design | Study Location | Sample Size | Risk Assessment | Risk Management | Occurrence Rates | Measures | Quality Assessment NOS Score | |
|---|---|---|---|---|---|---|---|---|---|
| Arnetz et al. [14] | Cross sectional | America | United States | 695 | X | X | PCL-6 (*) | 7 | |
| Ramirez et al. [15] | Cross sectional | Mexico | 3932 | X | X | IES-R (**) | 6 | ||
| Chew et al. [16] | Cross sectional | Asia | India Singapore Indonesia Malaysia Vietnama | 384 277 250 175 60 | X | X | X | IES-R (**) | 5 |
| Tan et al. [17] | Cross sectional | Singapore | 470 | X | X | IES-R (**) | 5 | ||
| Khasne et al. [18] | Cross sectional | India | 2026 | X | X | CBI (***) | |||
| Ying et al. [2] | Cross sectional | China | 371 | X | X | PCL-5 (****) | 5 | ||
| Song et al. [19] | Cross sectional | China | 13.879 | X | X | X | PCL-5 (****) | 7 | |
| Wang XY et al. [20] | Cross sectional | China | 202 | X | X | PTSD Checklist-Civilian Version | 6 | ||
| Si et al. [21] | Cross sectional | China | 863 | X | X | IES-6 (*) | 6 | ||
| Wang Y et al. [22] | Cross sectional | China | 1257 | X | X | IES-R (**) | 7 | ||
| Asaoka et al. [23] | Cross sectional | Japan | 331 | X | IES-R (**) | 4 | |||
| Vagni et al. [24] | Cross sectional | Europe | Italy | 210 | X | X | STSS-I (*****) | 7 | |
| Rossi et al. [25] | Cross sectional | Italy | 1379 | X | X | Italian version of the Global Psychotrauma Screen (GPS) | |||
| Gonzàlez-Sanguino et al. [26] | Cross-sectional | Spain | 3480 | X | X | PCL-C-2 (******) | 7 | ||
| Luceno-Moreno et al. [27] | Cross sectional | Spain | 1422 | X | X | IES-R (**) | 6 | ||
| Caillet et al. [28] | Cross sectional | French | 208 | X | X | X | IES-R (**) | 7 | |
| Nowicki et al. [29] | Cross sectional | Poland | 325 | X | X | IES-R (**) | 7 | ||
| Geo-Graphical area | Reference | Primary Outcome | Methods/Investigation Period/Setting | Occurrence Rate/Main Results/Risk Management |
|---|---|---|---|---|
| North and Central America | Arnetz et al. [14] | To evaluate the association between access to adequate PPE and mental health outcomes among U.S. nurses | Online questionnaire/May 2020/COVID-19: nurses |
|
| Ramirez et al. [15] | To evaluate the presence of psychological distress, signs of post-traumatic stress, and to identify the groups of subjects at highest risk | Online survey/March–April 2020/COVID-19: volunteers, mainly students and employees of a Mexican University, HCWs and their contacts |
| |
| South-East Asia | Chew et al. [16] | To compare the psychological outcomes during the COVID-19 pandemic and identify factors associated with adverse psychological outcomes | Self-administered survey/April–June 2020/COVID-19: HCWs | Ranges in analyzed countries:
Resources proposed to reduce PTSS:
|
| Tan et al. [17] | To examine the psychological distress, depression, anxiety, and stress experienced by healthcare workers | Self-administered survey/February–March 2020/COVID-19: HCWs |
| |
| Khasne et al. [18] | To evaluate the prevalence of burnout in HCWs involved in the care of COVID-19 patients | Questionnaire-based survey/date not reported/COVID-19: HCWs |
| |
| Ying et al. [2] | To investigate the mental health status and related factors in families of HCWs employed in hospital | Online self-administered questionnaires/February 2020/COVID-19: families of HCWs |
| |
| Song et al. [19] | To assess the mental health of emergency department medical staff during the SARS-CoV-2 epidemic | Electronic questionnaires/February–March 2020/COVID-19: HCWs |
Resources proposed to reduce PTSS:
| |
| Wang XY et al. [20] | To investigate the factors potentially involved in the level of PTSD of nurses exposed to COVID-19 | Questionnaires/February–March 2020/COVID-19: Nurses |
| |
| Si et al. [21] | To identify and evaluate the psychological impact of COVID-19 on medical care workers | Questionnaires/February–March 2020/COVID-19: medical care workers |
| |
| Wang Y et al. [22] | To evaluate the acute psychological effects of COVID-19 outbreak among HCWs | Survey/Early period of pandemic in China/COVID-19: HCWs |
Risk factors for PTSD were being a nurse, having an intermediate technical title, working at the frontline, and lacking confidence in protection measures. Protective factor for developing depression, anxiety, and PTSD was not worrying about infection. | |
| Asaoka et al. [23] | To evaluate factors associated with post-traumatic stress symptoms (PTSS) among HCWs highly involved in COVID-19-related activities outside hospitals | Internet-based survey/March–April 2020/COVID-19: HCWs | Anxiety about infection, exhaustion and being a Disaster Psychiatric Assistance Team member were associated with PTSS. | |
| Western Europe | Vagni et al. [24] | To explore the relationship between coping strategies used by HCWs and emergency workers to manage the stress factors related to the SARSC-CoV-2 epidemic | Questionnaires online/date not reported/COVID-19: HCWs and emergency workers | HCWs had greater levels of emergency stress and arousal and were more willing to use problem-focused coping compared with emergency workers. HCWs are exposed to a large degree of stress and could experience secondary trauma linked with their involvement in the treatment of SARS-CoV-2 infection. Resources proposed to reduce PTSS:
|
| Rossi et al. [25] | To evaluate mental health outcomes among HCWs | Online questionnaire/March 2020/COVID-19: HCWs |
Having a colleague who died was associated with PTSS, depression, and insomnia. | |
| Gonzàlez-Sanguino et al. [26] | To evaluate the psychological impact of the COVID-19 outbreak in a sample of the Spanish population | Survey/Early period of the pandemic in Spain/COVID-19: Spanish population and HCWs |
Factors negatively related to depression, anxiety, and PTSD: Being in the older age group, having economic stability, and the belief that adequate information had been provided about the pandemic. | |
| Luceno-Moreno et al. [27] | To analyze post-traumatic stress, anxiety, and depression during the SARS-CoV-2 pandemic To evaluate associations between COVID-19 and burnout, resilience, work | Online survey/April 2020/COVID-19: HCWs |
| |
| Caillet et al. [28] | To assess the psychological impact of COVID-19 on ICU caregivers at the peak of the “crisis period” | Survey/April 2020/COVID-19: ICU HCWs |
| |
| Nowicki et al. [29] | To investigates the level of post-traumatic stress, perceived social support, sense of security, and sense of meaning among nurses in the face of the SARS-CoV-2 epidemic. | Computer-assisted web interviews/May 2020/COVID-19: Nurses | An intensification of traumatic stress symptoms with particularly pronounced symptoms of avoidance was observed in subjects evaluated. Nurses characterized the experience of a pandemic with a reduced sense of security and an intense reflection on issues related to their personal safety. Resources proposed to reduce PTSS:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
d’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-Traumatic Stress Symptoms in Healthcare Workers Dealing with the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 601. https://doi.org/10.3390/ijerph18020601
d’Ettorre G, Ceccarelli G, Santinelli L, Vassalini P, Innocenti GP, Alessandri F, Koukopoulos AE, Russo A, d’Ettorre G, Tarsitani L. Post-Traumatic Stress Symptoms in Healthcare Workers Dealing with the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(2):601. https://doi.org/10.3390/ijerph18020601
Chicago/Turabian Styled’Ettorre, Gabriele, Giancarlo Ceccarelli, Letizia Santinelli, Paolo Vassalini, Giuseppe Pietro Innocenti, Francesco Alessandri, Alexia E. Koukopoulos, Alessandro Russo, Gabriella d’Ettorre, and Lorenzo Tarsitani. 2021. "Post-Traumatic Stress Symptoms in Healthcare Workers Dealing with the COVID-19 Pandemic: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 2: 601. https://doi.org/10.3390/ijerph18020601