Nutritional Factors, Physical Health and Immigrant Status Are Associated with Anxiety Disorders among Middle-Aged and Older Adults: Findings from Baseline Data of The Canadian Longitudinal Study on Aging (CLSA)

 ,
, _Lin.jpg) , , , and
, , , and
Abstract
:1. Introduction
- (1)
- Is immigrant status associated with anxiety disorders among Canadians aged 45 to 85?
- (2)
- Is the association between immigrant status and anxiety disorders attenuated by a wide range of socio-demographic, health, and nutritional correlates?
- (3)
- What specific dietary intakes are associated with anxiety disorders among Canadians 45–85 years after adjusting for immigrant status?
- (4)
- What other factors are significantly associated with anxiety disorders after controlling for immigrant status?
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Analysis
3. Results
3.1. Sample Description and Bivariate Analysis
3.2. Logistic Regression Analysis
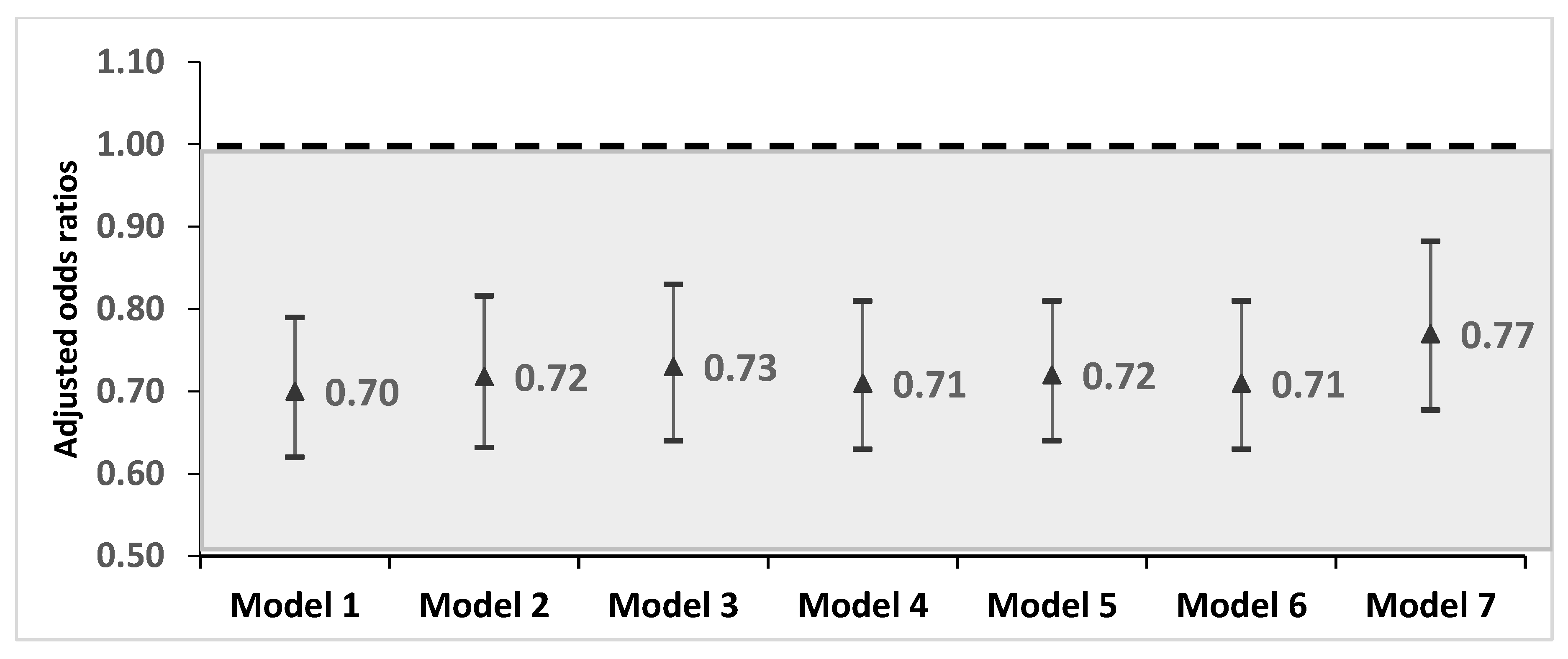
3.2.1. Research Question 1 & 2: Is Immigrant Status Associated with Anxiety Disorders and Is This Association Attenuated by a Wide Range of Health Determinants?
3.2.2. Research Question 3: What Specific Dietary Intakes Are Associated with Anxiety Disorders after Adjusting for Immigrant Status?
3.2.3. Research Question 4: What Other Factors Are Significantly Associated with Anxiety Disorders after Controlling for Immigrant Status?
3.3. Sensitivity Analysis
4. Discussion
4.1. Research Questions 1 & 2: Is Immigrant Status Associated with Anxiety Disorders and Is Any Immigration-Anxiety Association Attenuated When Other Health Determinants Are Taken into Account?
4.2. Research Question 3: What Specific Dietary Intakes Are Associated with Anxiety Disorders after Adjusting for Immigrant Status?
4.3. Research Question 4: What Other Factors Are Significantly Associated with Anxiety Disorders after Controlling for Immigrant Status?
4.4. Limitations and New Contributions to The Research Literature
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Somers, J.M.; Goldner, E.M.; Waraich, P.; Hsu, L. Prevalence and incidence studies of anxiety disorders: A systematic review of the literature. Can. J. Psychiatry 2006, 51, 100–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baxter, A.J.; Scott, K.M.; Vos, T.; Whiteford, H.A. Global prevalence of anxiety disorders: A systematic review and meta-regression. Psychol. Med. 2013, 43, 897–910. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Mental illness surveillance among adults in the United States. MMWR 2011, 60, 1–32. [Google Scholar]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [CrossRef] [Green Version]
- Zaider, T.I.; Heimberg, R.G.; Iida, M. Anxiety disorders and intimate relationships: A study of daily processes in couples. J. Abnorm. Psychol. 2010, 119, 163–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramkisson, S.; Pillay, B.J.; Sartorius, B. Anxiety, depression and psychological well-being in a cohort of South African adults with type 2 diabetes mellitus. S. Afr. J. Psychiatr. 2016, 22, 935. [Google Scholar] [CrossRef] [Green Version]
- De Beurs, E.; Beekman, A.T.F.; van Balkom, A.J.L.M.; Deeg, D.J.H.; van Dyck, R.; van Tilburg, W. Consequences of anxiety in older persons: Its effect on disability, well-being and use of health services. Psychol. Med. 1999, 29, 583–593. [Google Scholar] [CrossRef] [Green Version]
- Sareen, J.; Cox, B.J.; Afifi, T.O.; de Graaf, R.; Asmundson, G.J.; ten Have, M.; Stein, M.B. Anxiety disorders and risk for suicidal ideation and suicide attempts: A population-based longitudinal study of adults. Arch. Gen. Psychiatry 2005, 62, 1249–1257. [Google Scholar] [CrossRef] [Green Version]
- Sareen, J.; Cox, B.J.; Stein, M.B.; Afifi, T.O.; Fleet, C.; Asmundson, G.J. Physical and mental comorbidity, disability, and suicidal behavior associated with posttraumatic stress disorder in a large community sample. Psychosom. Med. 2007, 69, 242–248. [Google Scholar] [CrossRef]
- Sutherland, G.; Stonebridge, C. Healthy Brains at Work: Estimating the Impact of Workplace Mental Health Benefits and Programs; The Conference Board of Canada: Ottawa, ON, Canada, 2016. [Google Scholar]
- Sutherland, G.; Stonebridge, C. Healthy Brains at Work: Creating the Conditions for Healthy Brains in the Workplace; The Conference Board of Canada: Ottawa, ON, Canada, 2017. [Google Scholar]
- Shirneshan, E. Cost of illness Study of Anxiety Disorders for the Ambulatory Adult Population of the United States. Ph.D. Thesis, University of Tennessee Health Science Center, Knoxville, TN, USA, 2013. [Google Scholar]
- Shirneshan, E.; Bailey, J.; Relyea, G.; Franklin, B.E.; Solomon, D.K.; Brown, L.M. Incremental direct medical expenditures associated with anxiety disorders for the U.S. adult population: Evidence from the Medical Expenditure Panel Survey. J. Anxiety Disord. 2013, 27, 720–727. [Google Scholar] [CrossRef]
- Bandelow, B.; Michaelis, S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin. Neurosci. 2015, 17, 327–335. [Google Scholar] [PubMed]
- National Institute of Mental Health. Any Anxiety Disorder. 2017. Available online: https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder.shtml (accessed on 11 January 2020).
- McLaughlin, K.A.; Costello, E.J.; Leblanc, W.; Sampson, N.A.; Kessler, R.C. Socioeconomic status and adolescent mental disorders. Am. J. Public Health 2012, 102, 1742–1750. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Krokstad, S.; Mykletun, A.; Dahl, A.A.; Tell, G.S.; Tambs, K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc. Sci. Med. 2008, 66, 1334–1345. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.M.; Wells, J.E.; Angermeyer, M.; Brugha, T.S.; Bromet, E.; Demyttenaere, K.; de Girolamo, G.; Gureje, O.; Haro, J.M.; Jin, R.; et al. Gender and the relationship between marital status and first onset of mood, anxiety and substance use disorders. Psychol. Med. 2010, 40, 1495–1505. [Google Scholar] [CrossRef] [Green Version]
- Strine, T.W.; Mokdad, A.H.; Dube, S.R.; Balluz, L.S.; Gonzalez, O.; Berry, J.T.; Manderscheid, R.; Kroenke, K. The association of depression and anxiety with obesity and unhealthy behaviors among community-dwelling US adults. Gen. Hosp. Psychiatry 2008, 30, 127–137. [Google Scholar] [CrossRef]
- Fuller-Thomson, E.; Jayanthikumar, J.; Agbeyaka, S.K. Untangling the association between migraine, pain, and anxiety: Examining migraine and generalized anxiety disorders in a Canadian population based study. Headache 2017, 57, 375–390. [Google Scholar] [CrossRef]
- Fuller-Thomson, E.; Lateef, R.; Sulman, J. Robust association between inflammatory bowel disease and generalized anxiety disorder: Findings from a nationally representative Canadian study. Inflamm. Bowel. Dis. 2015, 21, 2341–2348. [Google Scholar] [CrossRef]
- DeJean, D.; Giacomini, M.; Vanstone, M.; Brundisini, F. Patient experiences of depression and anxiety with chronic disease: A systematic review and qualitative meta-synthesis. Ont. Health Technol. Assess Ser. 2013, 13, 1–33. [Google Scholar]
- Peltzer, K.; Pengpid, S. Anxiety and depressive features in chronic disease patients in Cambodia, Myanmar and Vietnam. [Anxiety; depression; chronic diseases; comorbidity; Cambodia; Myanmar; Vietnam]. S. Afr. J. Psychiatr. 2016, 22, 940. [Google Scholar] [CrossRef] [Green Version]
- Conn, V.S. Anxiety outcomes after physical activity interventions: Meta-analysis findings. Nurs. Res. 2010, 59, 224–231. [Google Scholar] [CrossRef] [Green Version]
- De Moor, M.H.; Beem, A.L.; Stubbe, J.H.; Boomsma, D.I.; De Geus, E.J. Regular exercise, anxiety, depression and personality: A population-based study. Prev. Med. 2006, 42, 273–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stonerock, G.L.; Hoffman, B.M.; Smith, P.J.; Blumenthal, J.A. Exercise as treatment for anxiety: Systematic review and analysis. Ann. Behav. Med. 2015, 49, 542–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacka, F.N.; Mykletun, A.; Berk, M.; Bjelland, I.; Tell, G.S. The association between habitual diet quality and the common mental disorders in community-dwelling adults: The Hordaland Health study. Psychosom. Med. 2011, 73, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Jacka, F.N.; Pasco, J.A.; Mykletun, A.; Williams, L.J.; Hodge, A.M.; O’Reilly, S.L.; Nicholson, G.C.; Kotowicz, M.A.; Berk, M. Association of Western and traditional diets with depression and anxiety in women. Am. J. Psychiatry 2010, 167, 305–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, K.P.; Tseng, P.T.; Lin, P.Y.; Okubo, R.; Chen, T.Y.; Chen, Y.W.; Matsuoka, Y.J. Association of use of omega-3 polyunsaturated fatty acids with changes in severity of anxiety symptoms: A systematic review and meta-analysis. JAMA Netw. Open 2018, 1, e182327. [Google Scholar] [CrossRef] [PubMed]
- De Souza, R.G.M.; Schincaglia, R.M.; Pimentel, G.D.; Mota, J.F. Nuts and human health outcomes: A systematic review. Nutrients 2017, 9, 1311. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, K.; Cowen, P.J.; Harmer, C.J.; Tzortzis, G.; Errington, S.; Burnet, P.W. Prebiotic intake reduces the waking cortisol response and alters emotional bias in healthy volunteers. Psychopharmacology 2015, 232, 1793–1801. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.M.; Holscher, H.D. A review of dietary and microbial connections to depression, anxiety, and stress. Nutr. Neurosci. 2018, 23, 237–250. [Google Scholar] [CrossRef]
- Leshem, M. Low dietary sodium is anxiogenic in rats. Physiol. Behav. 2011, 103, 453–458. [Google Scholar] [CrossRef]
- Davison, K.M.; Lung, Y.; Lin, S.L.; Tong, H.; Kobayashi, K.M.; Fuller-Thomson, E. Depression in middle and older adulthood: The role of immigration, nutrition, and other determinants of health in the Canadian longitudinal study on aging. BMC Psychiatry 2019, 19, 329. [Google Scholar] [CrossRef] [Green Version]
- Davison, K.M.; Lung, Y.; Lin, S.; Tong, H.; Kobayashi, K.; Fuller-Thomson, E. Psychological distress in older adults linked to immigrant status, dietary intake, and physical health conditions in the Canadian Longitudinal Study on Aging (CLSA). J. Affect. Disord. 2020, 265, 526–537. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Yip, T.; Gee, G. The physical and mental health effects of age of immigration, age, and perceived difference in social status among first generation Asian Americans. Asian Am. J. Psychol. 2012, 3, 29–43. [Google Scholar] [CrossRef]
- Creese, G.; Wiebe, B. ‘Survival Employment’: Gender and deskilling among African immigrants in Canada. Int. Migr. 2012, 50, 56–76. [Google Scholar] [CrossRef]
- Quillian, L.; Pager, D.; Hexel, O.; Midtboen, A.H. Meta-analysis of field experiments shows no change in racial discrimination in hiring over time. Proc. Natl. Acad. Sci. USA 2017, 114, 10870–10875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, K.M.; Gondara, L. A comparison of mental health, food insecurity and diet quality indicators between foreign-born immigrants of Canada and Native-born Canadians. J. Hunger Environ. Nutr. 2019. [Google Scholar] [CrossRef]
- Tiikkaja, S.; Sandin, S.; Malki, N.; Modin, B.; Sparen, P.; Hultman, C.M. Social class, social mobility and risk of psychiatric disorder--a population-based longitudinal study. PLoS ONE 2013, 8, e77975. [Google Scholar] [CrossRef] [PubMed]
- Szaflarski, M.; Cubbins, L.A.; Meganathan, K. Anxiety disorders among US immigrants: The role of immigrant background and social-psychological factors. Issues Ment. Health Nurs. 2017, 38, 317–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, A.; Tsai, W.; Shih, J.; Liu, L.; Hwang, W.; Takeuchi, D. The immigrant paradox among Asian American women: Are disparities in the burden of depression and anxiety paradoxical or explicable? J. Consult. Clin. Psychol. 2013, 81, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Watterson, R.A.; Williams, J.V.; Lavorato, D.H.; Patten, S.B. Descriptive epidemiology of generalized anxiety disorder in Canada. Can. J. Psychiatry 2017, 62, 24–29. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, S.; Kidd, M.P.; McDonald, J.T.; Biddle, N. The healthy immigrant effect: Patterns and evidence from four countries. J. Int. Migr. Integr. 2014, 16, 317–332. [Google Scholar] [CrossRef]
- Baum, F.; Lawless, A.; Williams, C. Health in All Policies from International Ideas to Local Implementation: Policies, Systems, and Organizations. In Health Promotion and the Policy Process; Clavier, C., de Leeuw, E., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 188–217. [Google Scholar]
- Davison, K.M.; D’Andreamatteo, C.; Mitchell, S.; Vanderkooy, P. The development of a national nutrition and mental health research agenda with comparison of priorities among diverse stakeholders. Public Health Nutr. 2017, 20, 712–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raina, P.S.; Wolfson, C.; Kirkland, S.A.; Griffith, L.E.; Oremus, M.; Patterson, C.; Tuokko, H.; Penning, M.; Balion, C.M.; Hogan, D.; et al. The Canadian Longitudinal Study on Aging (CLSA). Can. J. Aging 2009, 28, 221–229. [Google Scholar] [CrossRef]
- Stinchcombe, A.; Wilson, K.; Kortes-Miller, K.; Chambers, L.; Weaver, B. Physical and mental health inequalities among aging lesbian, gay, and bisexual Canadians: Cross-sectional results from the Canadian Longitudinal Study on Aging (CLSA). Can. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Aglipay, M.; Colman, I.; Chen, Y. Does the healthy immigrant effect extend to anxiety disorders? Evidence from a nationally representative study. J. Immigr. Minor. Health 2013, 15, 851–857. [Google Scholar] [CrossRef]
- Nabalamba, A.; Patten, S.B. Prevalence of mental disorders in a Canadian household population with dementia. Can. J. Neurol. Sci. 2010, 37, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller-Thomson, E.; Baker, T.M.; Brennenstuhl, S. Evidence supporting an independent association between childhood physical abuse and lifetime suicidal ideation. Suicide Life Threat. Behav. 2012, 42, 279–291. [Google Scholar] [CrossRef]
- Sanchez-Villegas, A.; Schlatter, J.; Ortuno, F.; Lahortiga, F.; Pla, J.; Benito, S.; Martinez-Gonzalez, M.A. Validity of a self-reported diagnosis of depression among participants in a cohort study using the Structured Clinical Interview for DSM-IV (SCID-I). BMC Psychiatry 2008, 8, 43. [Google Scholar] [CrossRef] [Green Version]
- Herva, A.; Laitinen, J.; Miettunen, J.; Veijola, J.; Karvonen, J.T.; Läksy, K.; Joukamaa, M. Obesity and depression: Results from the longitudinal Northern Finland 1966 Birth Cohort Study. Int. J. Obes. 2006, 30, 520–527. [Google Scholar] [CrossRef] [Green Version]
- Statistics Canada. Heavy Drinking. 2016. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2017001/article/54861-eng.htm (accessed on 16 November 2018).
- Guruge, S.; Thomson, M.S.; Seifi, S.G. Mental health and service issues faced by older immigrants in Canada: A scoping review. Can. J. Aging 2015, 34, 431–444. [Google Scholar] [CrossRef]
- Bauldry, S.; Szaflarski, M. Immigrant-based disparities in mental health care utilization. Socius 2017, 3. [Google Scholar] [CrossRef]
- Thomson, M.S.; Chaze, F.; George, U.; Guruge, S. Improving immigrant populations’ access to mental health services in Canada: A Review of Barriers and Recommendations. J. Immigr. Minor. Health 2015, 17, 1895–1905. [Google Scholar] [CrossRef] [PubMed]
- Derr, A.S. Mental health service use among immigrants in the United States: A systematic review. Psychiatr. Serv. 2016, 67, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Morales, B.; Cueto-Escobedo, J.; Guillen-Ruiz, G.; Rodriguez-Landa, J.F.; Contreras, C.M. A fatty acids mixture reduces anxiety-like behaviors in infant rats mediated by GABAA receptors. Biomed Res. Int. 2017, 2017, 8798546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clouard, C.; Gerrits, W.J.; van Kerkhof, I.; Smink, W.; Bolhuis, J.E. Dietary linoleic and alpha-linolenic acids affect anxiety-related responses and exploratory activity in growing pigs. J. Nutr. 2015, 145, 358–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Y.; Xia, J.; Ke, Y.; Cheng, J.; Yuan, J.; Wu, S.; Lv, Z.; Huang, S.; Kim, J.H.; Wong, S.Y.; et al. Effects of nut consumption on selected inflammatory markers: A systematic review and meta-analysis of randomized controlled trials. Nutrition 2018, 54, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Torabi, M.; Kesmati, M.; Harooni, H.E.; Varzi, H.N. Effects of nano and conventional zinc oxide on anxiety-like behavior in male rats. Indian J. Pharm. 2013, 45, 508–512. [Google Scholar] [CrossRef]
- Sartori, S.B.; Whittle, N.; Hetzenauer, A.; Singewald, N. Magnesium deficiency induces anxiety and HPA axis dysregulation: Modulation by therapeutic drug treatment. Neuropharmacology 2012, 62, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Carroll, D.; Ring, C.; Suter, M.; Willemsen, G. The effects of an oral multivitamin combination with calcium, magnesium, and zinc on psychological well-being in healthy young male volunteers: A double-blind placebo-controlled trial. Psychopharmacology 2000, 150, 220–225. [Google Scholar] [CrossRef]
- Yannakoulia, M.; Panagiotakos, D.B.; Pitsavos, C.; Tsetsekou, E.; Fappa, E.; Papageorgiou, C.; Stefanadis, C. Eating habits in relations to anxiety symptoms among apparently healthy adults. A pattern analysis from the ATTICA Study. Appetite 2008, 51, 519–525. [Google Scholar] [CrossRef]
- Rezzi, S.; Ramadan, Z.; Martin, F.P.; Fay, L.B.; van Bladeren, P.; Lindon, J.C.; Nicholson, J.K.; Kochhar, S. Human metabolic phenotypes link directly to specific dietary preferences in healthy individuals. J. Proteome Res. 2007, 6, 4469–4477. [Google Scholar] [CrossRef] [Green Version]
- Niccolai, E.; Boem, F.; Russo, E.; Amedei, A. The gut(-)brain axis in the neuropsychological disease model of obesity: A classical movie revised by the emerging director “Microbiome”. Nutrients 2019, 11, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, K.M.; Kaplan, B.J. Nutrient intakes are correlated with overall psychiatric functioning in adults with mood disorders. Can. J. Psychiatry 2012, 57, 85–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlemmer, U.; Frolich, W.; Prieto, R.M.; Grases, F. Phytate in foods and significance for humans: Food sources, intake, processing, bioavailability, protective role and analysis. Mol. Nutr. Food Res. 2009, 53 (Suppl. 2), S330–S375. [Google Scholar] [CrossRef] [PubMed]
- Simpson, H.L.; Campbell, B.J. Review article: Dietary fibre-microbiota interactions. Aliment Pharm. 2015, 42, 158–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, G.B.; Keating, D.J.; Young, R.L.; Wong, M.L.; Licinio, J.; Wesselingh, S. From gut dysbiosis to altered brain function and mental illness: Mechanisms and pathways. Mol. Psychiatry 2016, 21, 738–748. [Google Scholar] [CrossRef] [Green Version]
- Harth, M.; Nielson, W.R. Pain and affective distress in arthritis: Relationship to immunity and inflammation. Expert Rev. Clin. Immunol. 2019, 15, 541–552. [Google Scholar] [CrossRef]
- Santo, E.C.; Vo, M.T.; Uratsu, C.S.; Grant, R.W. Patient-defined visit priorities in primary care: Psychosocial versus medically-related concerns. J. Am. Board Fam. Med. 2019, 32, 513–520. [Google Scholar] [CrossRef]
- Puhl, R.M.; Heuer, C.A. The stigma of obesity: A review and update. Obesity 2009, 17, 941–964. [Google Scholar] [CrossRef]
- Ostbye, T.; Dement, J.M.; Krause, K.M. Obesity and workers’ compensation: Results from the Duke Health and Safety Surveillance System. Arch. Intern. Med. 2007, 167, 766–773. [Google Scholar] [CrossRef] [Green Version]
- Spencer, S.J.; Xu, L.; Clarke, M.A.; Lemus, M.; Reichenbach, A.; Geenen, B.; Kozicz, T.; Andrews, Z.B. Ghrelin regulates the hypothalamic-pituitary-adrenal axis and restricts anxiety after acute stress. Biol. Psychiatry 2012, 72, 457–465. [Google Scholar] [CrossRef]
- Aschbacher, K.; Rodriguez-Fernandez, M.; van Wietmarschen, H.; Tomiyama, A.J.; Jain, S.; Epel, E.; Doyle, F.J.; van der Greef, J. The hypothalamic-pituitary-adrenal-leptin axis and metabolic health: A systems approach to resilience, robustness and control. Interface Focus 2014, 4, 20140020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarouna, S.; Wozniak, G.; Papachristou, A.I. Mood disorders: A potential link between ghrelin and leptin on human body? World J. Exp. Med. 2015, 5, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.J.; Zhu, X.C.; Han, Q.Q.; Wang, Y.L.; Yue, N.; Wang, J.; Yu, R.; Li, B.; Wu, G.C.; Liu, Q.; et al. Ghrelin alleviates anxiety- and depression-like behaviors induced by chronic unpredictable mild stress in rodents. Behav. Brain Res. 2017, 326, 33–43. [Google Scholar] [CrossRef]
- Spencer, S.J.; Tilbrook, A. The glucocorticoid contribution to obesity. Stress 2011, 14, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Kirchner, J.E.; Zubritsky, C.; Cody, M.; Coakley, E.; Chen, H.; Ware, J.H.; Oslin, D.W.; Sanchez, H.A.; Durai, U.N.; Miles, K.M.; et al. Alcohol consumption among older adults in primary care. J. Gen. Intern. Med. 2007, 22, 92–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.-U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Reiss, S.; Peterson, R.A.; Gursky, D.M.; McNally, R.J. Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behav. Res. 1986, 24, 1–8. [Google Scholar] [CrossRef]
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef]
- Vu, H.T.T.; Lin, V.; Pham, T.; Pham, T.L.; Nguyen, A.T.; Nguyen, H.T.; Nguyen, T.X.; Nguyen, T.N.; Nguyen, H.T.T.; Nguyen, T.T.H.; et al. Determining risk for depression among older people residing in Vietnamese rural settings. Int. J. Environ. Res. Public Health 2019, 16, 2654. [Google Scholar] [CrossRef] [Green Version]
- Ho, R.C.M.; Chua, A.C.; Tran, B.X.; Choo, C.C.; Husain, S.F.; Vu, G.T.; McIntyre, R.S.; Ho, C.S.H. Factors associated with the risk of developing coronary artery disease in medicated patients with major depressive disorder. Int. J. Environ. Res. Public Health 2018, 15, 2073. [Google Scholar] [CrossRef] [Green Version]
- Vu, H.T.T.; Nguyen, T.X.; Nguyen, H.T.T.; Le, T.A.; Nguyen, T.N.; Nguyen, A.T.; Nguyen, T.T.H.; Nguyen, H.L.; Nguyen, C.T.; Tran, B.X.; et al. Depressive symptoms among elderly diabetic patients in Vietnam. Diabetes Metab. Syndr. Obes. 2018, 11, 659–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quek, Y.H.; Tam, W.W.S.; Zhang, M.W.B.; Zhang, M.W.B.; Ho, R.C.M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 2017, 18, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.S.H.; Tan, E.L.Y.; Ho, R.C.M.; Chiu, M.Y.L. Relationship of anxiety and depression with respiratory symptoms: Comparison between depressed and non-depressed smokers in Singapore. Int. J. Environ. Res. Public Health 2019, 16, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shepardson, R.L.; Buchholz, L.J.; Weisberg, R.B.; Funderburk, J.S. Psychological interventions for anxiety in adult p1rimary care patients: A review and recommendations for future research. J. Anxiety Disord. 2018, 54, 71–86. [Google Scholar]


{kind=link}
| Variables | Total (n = 26,991) | Immigration Status | Cases of Anxiety | X2 (df), p-Value a | |||
|---|---|---|---|---|---|---|---|
| CB | FB | Disorders | |||||
| (n = 22,258) | (n = 4733) | (n = 2286) | |||||
| n | % | CB% | FB% | n | Anxiety% | ||
| Core Block | |||||||
| Immigration status | |||||||
| Canadian born (CB) | 22,258 | 82.8% | -- | -- | 2007 | 9.3% | 40.8 (1), <0.001 |
| Foreign born (FB) | 4733 | 17.2% | -- | -- | 279 | 6.4% | |
| Sex | |||||||
| Men | 13,300 | 49.9% | 49.1% | 53.9% | 849 | 6.7% | 153.5 (1), |
| Women | 13,691 | 50.1% | 50.9% | 46.1% | 1437 | 11.0% | <0.001 |
| Age | |||||||
| 45–55 years | 6862 | 42.3% | 42.9% | 39.1% | 666 | 9.2% | 56.2 (3), <0.001 |
| 56–65 years | 8947 | 30.0% | 30.9% | 25.6% | 864 | 10.0% | |
| 66–75 years | 6628 | 17.1% | 16.1% | 22.0% | 523 | 8.0% | |
| 76–85 years | 4554 | 10.7% | 10.1% | 13.3% | 233 | 5.6% | |
| Socio-Demographic Factors | |||||||
| Income | |||||||
| <$20,000 | 1237 | 3.9% | 4.1% | 3.2% | 247 | 22.0% | 312.8 (5), <0.001 |
| $20,000–$49,999 | 5514 | 17.1% | 16.9% | 18.0% | 523 | 10.1% | |
| $50,000–$99,999 | 9042 | 31.9% | 31.6% | 33.1% | 760 | 9.3% | |
| $100,000–$149,999 | 5069 | 21.4% | 21.7% | 19.8% | 372 | 7.7% | |
| ≥$150,000 | 4476 | 20.6% | 20.7% | 19.8% | 258 | 5.8% | |
| Not answered | 1653 | 5.2% | 5.1% | 6.1% | 126 | 9.2% | |
| Marital status | |||||||
| Single | 2300 | 3.9% | 8.7% | 5.0% | 288 | 13.9% | 131.1 (2), <0.001 |
| Live with a partner | 18,781 | 17.1% | 75.8% | 80.6% | 1397 | 7.8% | |
| Widowed/separated | 5910 | 31.9% | 15.5% | 14.4% | 601 | 11.4% | |
| Educational level | |||||||
| <High school | 1378 | 4.50 | 5.0% | 2.5% | 157 | 12.6% | 32.3 (3), <0.001 |
| High school | 4471 | 15.4% | 16.0% | 12.5% | 397 | 9.2% | |
| ≥Post-secondary | 21,099 | 80.0% | 79.0% | 84.7% | 1726 | 8.5% | |
| Non-response | 43 | 0.1% | 0.1% | 0.3% | 6 | 22.2% | |
| Physical Health | |||||||
| Morbidities | |||||||
| 0 health conditions | 4946 | 20.8% | 20.5% | 22.3% | 139 | 3.0% | 829.5 (3), <0.001 |
| 1 health condition | 7319 | 28.9% | 28.8% | 29.7% | 414 | 6.3% | |
| 2 health conditions | 6307 | 22.5% | 22.7% | 21.7% | 484 | 8.3% | |
| 3 health conditions | 8419 | 27.8% | 28.1% | 26.30% | 1249 | 16.4% | |
| Physical Health/cont’d. | |||||||
| Hypertension levels | |||||||
| Normal | 9826 | 42.5% | 42.5% | 42.3% | 817 | 8.5% | 7.5 (4), 0.11 |
| Elevated | 2578 | 8.7% | 8.6% | 9.2% | 198 | 8.3% | |
| Stage 1 hypertension | 4303 | 17.1% | 17.4% | 15.9% | 392 | 9.2% | |
| Stage 2 hypertension | 2835 | 9.7% | 9.5% | 10.5% | 240 | 8.6% | |
| Takes anti- hypertensives | 7449 | 22.0% | 22.0% | 22.2% | 639 | 9.6% | |
| Chronic pain | |||||||
| No reported pain | 21,257 | 79.8% | 79.7% | 80.1% | 1519 | 7.5% | 252.6 (2), <0.001 |
| Have pain | 5629 | 20.0% | 20.10% | 19.4% | 758 | 14.3% | |
| Refused | 105 | 0.2% | 0.2% | 0.5% | 9 | 9.7% | |
| Health Behaviors | |||||||
| Smoking lifetime | |||||||
| ≥100 cigarettes | 14,290 | 50.7% | 51.9% | 44.8% | 1376 | 10.5% | 91.5 (1), |
| <100 cigarettes | 12,701 | 49.3% | 48.1% | 55.2% | 910 | 7.2% | <0.001 |
| Binge drinking b | |||||||
| Non-binge drinking | 17,472 | 60.2% | 58.5% | 68.4% | 1495 | 9.2% | 16.7 (2), <0.001 |
| Occasional | 4224 | 22.2% | 23.0% | 18.7% | 380 | 9.2% | |
| Regular | 5295 | 17.6% | 18.5% | 12.90% | 411 | 7.5% | |
| Physical activity | |||||||
| Never or seldom | 24,101 | 89.7% | 89.8% | 89.5% | 2050 | 8.9% | 2.2 (2), 0.326 |
| Sometime or often | 2880 | 10.2% | 10.2% | 10.4% | 235 | 8.1% | |
| No answer /refused | 10 | 0.0% | 0.0% | 0.2% | 1 | 9.1% | |
| Family physician visits in the past year | |||||||
| Yes | 24,327 | 87.6% | 87.5% | 87.9% | 2114 | 9.2% | 29.8 (1) |
| No | 2664 | 12.4% | 12.5% | 12.1% | 172 | 6.3% | <0.001 |
| Anthropometric Measures | |||||||
| Body mass index (BMI) | |||||||
| Underweight: <18.5 | 185 | 0.7% | 0.7% | 0.7% | 26 | 16.8% | 43.8 (3), <0.001 |
| Normal: 18.5–24.9 | 8064 | 32.1% | 31.5% | 35.0% | 631 | 8.4% | |
| Overweight: 25–29.9 | 10,901 | 40.1% | 39.9% | 40.7% | 832 | 8.0% | |
| Obese: ≥30 | 7841 | 27.2% | 27.9% | 23.7% | 797 | 10.3% | |
| Anthropometric Measures /cont’d. | |||||||
| Waist-to-hip ratio | |||||||
| Low risk | 9290 | 36.5% | 36.5% | 36.8% | 827 | 9.2% | 2.9 (2), |
| High risk | 17,699 | 63.5% | 63.5% | 63.2% | 1458 | 8.6% | 0.228 |
| Waist-to-height ratio | |||||||
| < cut-off | 18,102 | 67.7% | 67.2% | 70.1% | 1399 | 8.3% | 20.7 (1), |
| ≥ cut-off | 8889 | 32.3% | 32.8% | 29.9% | 887 | 10.0% | <0.001 |
| Disease risk | |||||||
| Least risk | 7942 | 31.8% | 31.2% | 34.8% | 622 | 8.5% | 51.5 (3), <0.001 |
| Increased | 7070 | 28.0% | 27.5% | 30.1% | 494 | 7.3% | |
| High | 4659 | 15.4% | 15.7% | 13.8% | 414 | 9.6% | |
| Very high | 7320 | 24.9% | 25.6% | 21.3% | 756 | 10.6% | |
| Body fat percent | |||||||
| 0–26% | 4793 | 20.8% | 20.2% | 23.8% | 243 | 5.4% | 219.1 (5), <0.001 |
| 26%–31% | 5216 | 19.5% | 19.4% | 20.1% | 352 | 7.4% | |
| 31%–36% | 5248 | 18.7% | 18.5% | 20.1% | 407 | 8.0% | |
| 36%–41% | 4995 | 17.7% | 18.2% | 15.5% | 528 | 11.5% | |
| 41%–59% | 5815 | 19.6% | 20.3% | 15.9% | 671 | 12.2% | |
| Dietary Intakes | |||||||
| Average daily intake of fiber sources | |||||||
| <1 | 8655 | 34.5% | 35.1% | 31.3% | 781 | 8.9% | 3.3 (3), 0.338 |
| ≥1 & <2 | 12,780 | 46.9% | 46.8% | 47.4% | 1032 | 8.6% | |
| ≥2 & <3 | 4440 | 14.9% | 14.5% | 16.8% | 372 | 9.3% | |
| ≥3 | 1116 | 3.7% | 3.6% | 4.4% | 101 | 9.8% | |
| Average daily intake of pulses and nuts | |||||||
| <0.5 | 8625 | 31.3% | 32.0% | 28.4% | 835 | 10.1% | 24.6 (3), <0.001 |
| ≥0.5 & <1 | 6204 | 23.1% | 23.2% | 22.6% | 466 | 7.9% | |
| ≥1 & <2 | 10,353 | 38.8% | 38.4% | 40.4% | 831 | 8.4% | |
| ≥2 | 1809 | 6.8% | 6.4% | 8.7% | 154 | 8.7% | |
| Average daily intake of fat sources | |||||||
| <2.5 | 3304 | 12.1% | 11.2% | 16.2% | 277 | 9.0% | 8.6 (3), 0.035 |
| ≥2.5 & <5 | 10,202 | 37.7% | 37.2% | 39.9% | 821 | 8.4% | |
| ≥4 & <5 | 6587 | 24.7% | 25.1% | 22.5% | 554 | 8.6% | |
| ≥5 | 6898 | 25.5% | 26.4% | 21.4% | 634 | 9.6% | |
| Intake of fish in the past year | |||||||
| Never | 2240 | 8.2% | 8.5% | 6.8% | 250 | 11.5% | 21.4 (1), |
| Ever | 24,751 | 91.8% | 91.5% | 93.2% | 2036 | 8.6% | <0.001 |
| Intake of omega 3 eggs in the past year | |||||||
| Never | 19,916 | 72.7% | 73.3% | 69.8% | 1696 | 8.9% | 0.1 (1), |
| Ever | 7075 | 27.3% | 26.7% | 30.2% | 590 | 8.7% | 0.673 |
| Dietary Intakes /cont’d.. | |||||||
| Average daily intake of fruits and vegetables | |||||||
| <2 | 3817 | 13.1% | 13.5% | 11.3% | 389 | 10.5% | 21.3 (4), <0.001 |
| ≥2 & <3 | 6446 | 22.7% | 22.8% | 22.3% | 555 | 9.2% | |
| ≥3 & <4 | 6741 | 25.1% | 25.0% | 25.3% | 518 | 7.8% | |
| ≥4 & <6 | 7357 | 27.9% | 27.4% | 30.0% | 610 | 8.9% | |
| ≥6 | 2630 | 11.2% | 11.3% | 11.1% | 214 | 8.4% | |
| Average daily intake of pure fruit juice | |||||||
| No consumption | 8725 | 31.2% | 30.7% | 33.7% | 775 | 9.1% | 3.2 (2), 0.196 |
| ≤1 | 17,680 | 66.7% | 67.2% | 64.2% | 1455 | 8.7% | |
| >1 | 586 | 2.1% | 2.1% | 2.1% | 56 | 10.4% | |
| Average daily intake of salty snacks | |||||||
| No consumption | 5086 | 15.9% | 14.0% | 25.0% | 392 | 8.2% | 2.6 (2), 0.264 |
| >0 & ≤1 | 21,850 | 83.9% | 85.8% | 74.8% | 1890 | 9.0% | |
| >1 & ≤10 | 55 | 0.2% | 0.2% | 0.2% | 4 | 10.9% | |
| Average daily intake of calcium sources with high vitamin D content | |||||||
| <1 | 5945 | 22.5% | 22.2% | 23.7% | 500 | 8.8% | 19.6 (3), <0.001 |
| ≥1 & <2 | 12,233 | 45.6% | 45.3% | 46.9% | 983 | 8.3% | |
| ≥2 & <4 | 7839 | 28.4% | 28.9% | 26.5% | 692 | 9.3% | |
| ≥4 | 974 | 3.5% | 3.6% | 2.9% | 111 | 12.2% | |
| Average daily intake of calcium sources with low vitamin D content | |||||||
| No consumption | 4480 | 16.3% | 16.9% | 13.7% | 412 | 8.6% | 0.2 (1), |
| >0 | 20,225 | 83.7% | 83.1% | 86.3% | 1874 | 8.9% | 0.599 |
| Average daily intake of pastries | |||||||
| No consumption | 2733 | 10.0% | 9.5% | 12.1% | 253 | 9.5% | 10.0 (2), 0.007 |
| >0 & ≤1 | 23,794 | 88.3% | 88.6% | 86.9% | 1977 | 8.7% | |
| >1 | 464 | 1.7% | 1.8% | 1.0% | 56 | 12.6% | |
| Average weekly intake of chocolate bars | |||||||
| No consumption | 9354 | 34.0% | 34.7% | 30.4% | 784 | 8.9% | 2.7 (2), 0.252 |
| >0 & <0.6 | 16,420 | 61.7% | 61.40% | 63.3% | 1379 | 8.7% | |
| ≥0.6 | 1217 | 4.3% | 3.9% | 6.3% | 123 | 10.1% | |
| Variable | aOR (95% CI) | p-Value |
|---|---|---|
| Demographic, Social, and Economic Characteristics | ||
| Immigrant (Ref: Canadian born) | ||
| Immigrant | 0.77 (0.67–0.88) | <0.001 |
| Age (Ref: 76–85 years) | ||
| 45–55 years | 3.52 (2.88–4.29) | <0.001 |
| 56–65 years | 2.86 (2.36–3.46) | <0.001 |
| 66–75 years | 1.79 (1.47–2.18) | <0.001 |
| Sex (Ref: Male) | ||
| Female | 1.25 (1.07–1.46) | 0.006 |
| Income (Ref:≥$150,000) | ||
| < $20,000 | 2.68 (2.14–3.37) | <0.001 |
| $20,000–49,999 | 1.47 (1.23–1.74) | <0.001 |
| $50,000–99,999 | 1.43 (1.23–1.65) | <0.001 |
| $100,000–149,999 | 1.28 (1.09–1.49) | 0.002 |
| Not answered | 1.39 (1.10–1.75) | 0.005 |
| Marital status (Ref: Married/common law) | ||
| Single | 1.27 (1.09–1.48) | 0.002 |
| Widowed/divorced/separated | 1.08 (0.95–1.23) | 0.255 |
| Education level (Ref: < high school) | ||
| High school graduate | 0.83 (0.67–1.03) | 0.089 |
| Post-secondary degree/diploma | 0.92 (0.75–1.12) | 0.394 |
| Not answered | 2.22 (0.91–5.43) | 0.080 |
| Physical Health | ||
| Morbidities (Ref: No health conditions) | ||
| 1 health condition | 2.13 (1.78–2.56) | <0.001 |
| 2 health conditions | 2.79 (2.33–3.35) | <0.001 |
| 3 health conditions | 5.73 (4.81–6.82) | <0.001 |
| Hypertension levels (Ref: Normal blood pressure) | ||
| Elevated | 1.02 (0.86–1.21) | 0.823 |
| Stage 1 hypertension | 1.12 (0.99–1.28) | 0.081 |
| Stage 2 hypertension | 1.07 (0.90–1.26) | 0.444 |
| Taking anti-hypertensive | 1.04 (0.92–1.19) | 0.510 |
| Chronic pain (Ref: No pain) | ||
| Pain | 1.31 (1.18–1.44) | <0.001 |
| Not answered | 1.06 (0.44–2.57) | 0.894 |
| Health Behaviors | ||
| Smoking ≥100 cigarettes (Ref: <100) | 1.35 (1.23–1.48) | <0.001 |
| Binge drinking (No binge drinking) | ||
| Regular binge drinking | 1.04 (0.92–1.18) | 0.542 |
| Occasional binge drinking | 0.84 (0.75–0.94) | 0.003 |
| Physical activity (Ref: Sometimes or often) | ||
| Never or seldom | 1.10 (0.94–1.27) | 0.236 |
| No answer or refused | 1.27 (0.20–7.95) | 0.799 |
| Family physician visits (Ref: ≥1 visit in past 12 months) | ||
| No physician visits | 0.85 (0.73–0.99) | 0.039 |
| Anthropometric Measures | ||
| BMI (Ref: Normal weight: 18.5–24.99) | ||
| Underweight: <18.5 | 1.87 (1.20–2.92) | 0.006 |
| Overweight: 25–29.99 | 0.72 (0.48–1.07) | 0.100 |
| Obese: ≥30 | 0.63 (0.37–1.08) | 0.091 |
| Waist to hip categorical (Ref: Below cut–off; low risk) | ||
| Above cut-off; High risk | 1.11 (0.99–1.26) | 0.073 |
| Waist–to–height ratio (Below cut–off; low risk) | ||
| Above cut-off; High risk | 1.01 (0.88–1.15) | 0.932 |
| Disease risk (Ref: Least risk) | ||
| Increased | 1.09 (0.74–1.63) | 0.659 |
| High | 1.17 (0.76–1.82) | 0.478 |
| Very high | 1.09 (0.62–1.92) | 0.765 |
| Body fat percent (Ref: 0–26%) | ||
| 26%–31% | 1.32 (1.12–1.56) | 0.001 |
| 31%–36% | 1.28 (1.06–1.53) | 0.009 |
| 36%–41% | 1.79 (1.46–2.19) | <0.001 |
| 41%–59% | 1.72 (1.36–2.18) | <0.001 |
| Dietary Intakes | ||
| Average daily intakes of fiber sources (Ref: 0 to <1) | ||
| ≥1 to <2 | 1.02 (1.00–1.22) | 0.061 |
| ≥2 to <3 | 1.25 (1.09–1.44) | 0.001 |
| ≥3 | 1.34 (1.06–1.70) | 0.014 |
| Dietary Intakes /cont’d | ||
| Average daily intakes of pulses and nuts (Ref: 0 to <0.5) | ||
| ≥0.5 to <1 | 0.84 (0.74–0.95) | 0.004 |
| ≥1 to <2 | 0.89 (0.80–0.99) | 0.040 |
| ≥2 | 0.93 (0.77–1.12) | 0.438 |
| Average daily intakes of fat sources (Ref: 0 to <2.5) | ||
| ≥2.5 to <4 | 0.92 (0.79–0.08) | 0.306 |
| ≥4 to <5 | 0.90 (0.75–1.08) | 0.243 |
| ≥5 | 0.88 (0.73–1.07) | 0.203 |
| Average daily intakes of fish (Ref: No fish consumption) | ||
| Consumes fish | 1.08 (0.93–1.25) | 0.317 |
| Average daily intakes of omega-3 eggs (Ref: No omega–3 eggs) | ||
| Consumes omega-3 eggs | 0.91 (0.83–1.01) | 0.076 |
| Average daily intakes of fruits and vegetables (Ref: ≥6) | ||
| 0 to <2 | 1.26 (1.04–1.52) | 0.019 |
| ≥2 to <3 | 1.24 (1.05–1.46) | 0.012 |
| ≥3 to <4 | 1.04 (0.88–1.22) | 0.666 |
| ≥4 to <6 | 1.13 (0.96–1.32) | 0.142 |
| Average daily intakes of pure fruit juice (Ref: No consumption) | ||
| ≤1 | 1.04 (0.94–1.15) | 0.433 |
| >1 | 1.28 (0.95–1.72) | 0.101 |
| Average daily intakes of salty snacks (Ref: No consumption) | ||
| 0 to ≤1 | 1.08 (0.95–1.23) | 0.227 |
| >1 day | 1.23 (0.49–3.06) | 0.663 |
| Average daily intakes of calcium sources with high vitamin D content (Ref: ≥4) | ||
| 0 to <1 | 0.73 (0.56–0.95) | 0.018 |
| ≥1 to <2 | 0.73 (0.57–0.92) | 0.009 |
| ≥2 to <4 | 0.81 (0.65–1.01) | 0.066 |
| Average daily intakes of calcium sources with low vitamin D content (Ref: >0) | ||
| No consumption | 0.93 (0.82–1.05) | 0.236 |
| Average daily intakes of pastries (Ref: No consumption) | ||
| >0 to ≤1 | 1.06 (0.91–1.23) | 0.459 |
| >1 | 1.55 (1.12–1.15) | 0.008 |
| Average weekly intakes of chocolate bars (Ref: No consumption) | ||
| >0 to ≤0.6 | 1.01 (0.92–1.11) | 0.850 |
| >0.6 | 1.06 (0.86–1.32) | 0.582 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davison, K.M.; Lin, S.; Tong, H.; Kobayashi, K.M.; Mora-Almanza, J.G.; Fuller-Thomson, E. Nutritional Factors, Physical Health and Immigrant Status Are Associated with Anxiety Disorders among Middle-Aged and Older Adults: Findings from Baseline Data of The Canadian Longitudinal Study on Aging (CLSA). Int. J. Environ. Res. Public Health 2020, 17, 1493. https://doi.org/10.3390/ijerph17051493
Davison KM, Lin S, Tong H, Kobayashi KM, Mora-Almanza JG, Fuller-Thomson E. Nutritional Factors, Physical Health and Immigrant Status Are Associated with Anxiety Disorders among Middle-Aged and Older Adults: Findings from Baseline Data of The Canadian Longitudinal Study on Aging (CLSA). International Journal of Environmental Research and Public Health. 2020; 17(5):1493. https://doi.org/10.3390/ijerph17051493
Chicago/Turabian StyleDavison, Karen M., Shen (Lamson) Lin, Hongmei Tong, Karen M. Kobayashi, Jose G. Mora-Almanza, and Esme Fuller-Thomson. 2020. "Nutritional Factors, Physical Health and Immigrant Status Are Associated with Anxiety Disorders among Middle-Aged and Older Adults: Findings from Baseline Data of The Canadian Longitudinal Study on Aging (CLSA)" International Journal of Environmental Research and Public Health 17, no. 5: 1493. https://doi.org/10.3390/ijerph17051493