Using a Developmental-Relational Approach to Understand the Impact of Interpersonal Violence in Women Who Struggle with Substance Use


Abstract
:1. Introduction
2. A Developmental-Relational Approach to Understand the Impact of IPV for Women
All of the things I witnessed at home really affected me in my early teenage years…and at that point I became addicted myself. And so, even though I kind of had a realization that I was following in my mom’s footsteps, I wasn’t really able to do anything about it, and my own cycle of addiction kind of took over at that point.[22] (p. 98)
It creates a lifetime of fear because you’ve spent a lifetime like that, walking on eggshells, not knowing…just expected to duck the next blow…It’s something that’s been one of the hardest things in my life to challenge and attempt to change, because it’s something that I’ve been formed like…I have, you know, severe reactionary issues when it comes to safety, and conversely overreactive sense of safety.[23] (p. 22)
There was all this violence in our house, and I thought that was normal, and I thought that’s what I was supposed to be growing up. And I was receiving violence from whomever, and I just let that happen…[27] (p. 15)
[It] de-sensitized you a little bit…my parents were so abusive towards each other, and there was no respect or love or affection, and there was always turmoil, turmoil, turmoil – we were moving, there was fighting, there was police, there was violence – that I found out even as an adult, because that was so normal for me, if my life was going along smoothly and calmly, it’s like unfamiliar so I create this chaos, this craziness, because that feels more comfortable to me.[27] (p. 16)
3. Origins of Substance Use in Women Exposed to IPV
3.1. IPV and Neurological Development
3.1.1. Physiological Mechanisms
3.1.2. Brain Structure and Functioning
3.1.3. Neuropsychological Development
3.2. IPV and the Development of Relational Capacity
3.2.1. Attachment
3.2.2. Internal Working Models
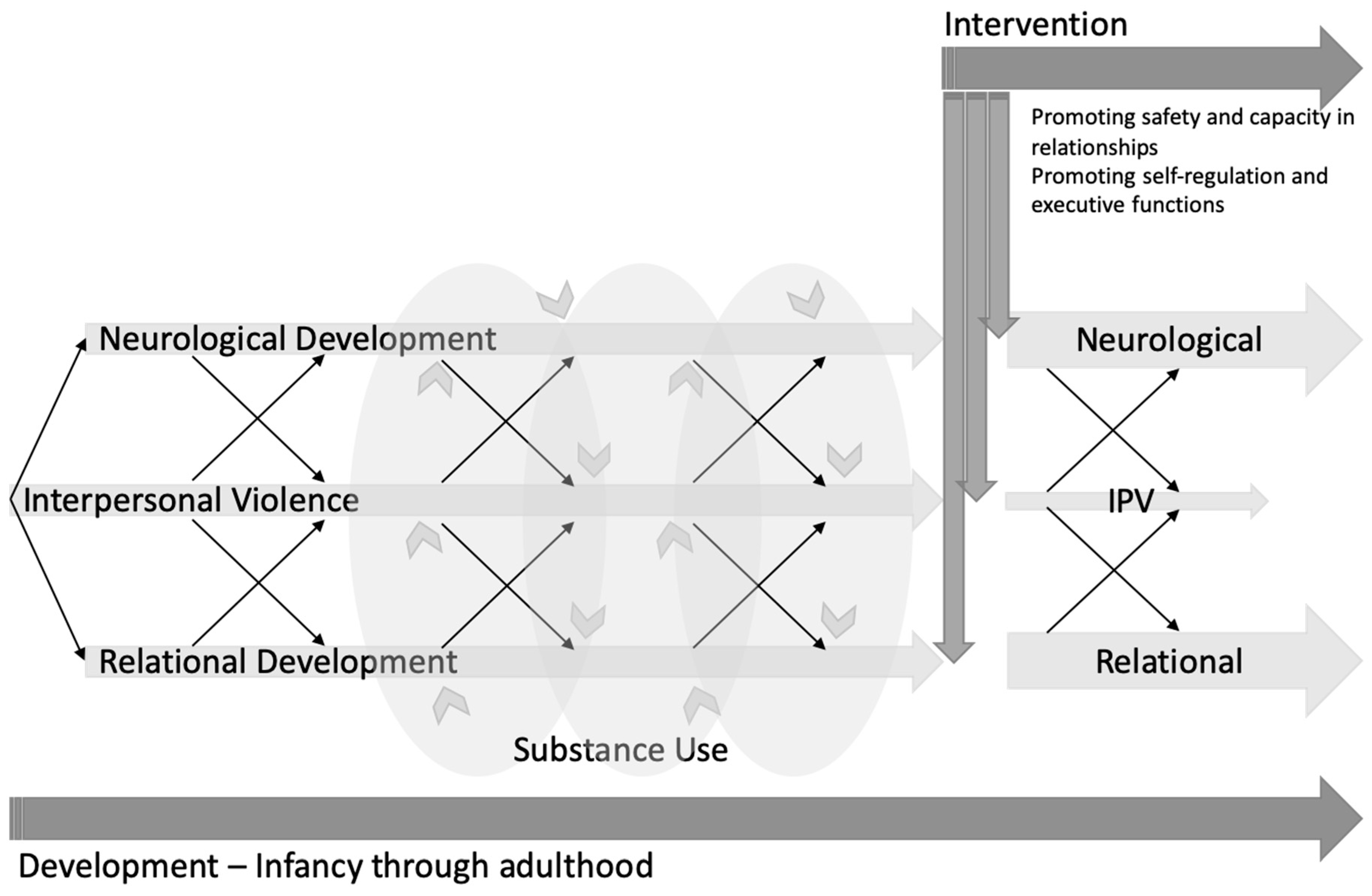
3.3. A Model of IPV and Substance Use Across the Lifespan
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mandavia, A.; Robinson, G.G.N.; Bradley, B.; Ressler, K.J.; Power, A. Exposure to Childhood Abuse and Later Substance Use: Indirect Effects of Emotion Dysregulation and Exposure to Trauma. J. Trauma. Stress 2016, 29, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.; Ordean, A.; Kahan, M. Substance Use in Pregnancy. Int. J. Gynecol. Obstet. 2011, 114, 190–202. [Google Scholar] [CrossRef]
- Canadian Centre for Justice Statistics. Family Violence in Canada: A Statistical Profile; Minister of Industry: Ottawa, ON, Canada, 2014. [Google Scholar]
- Sameroff, A. The Transactional Model. In The Transactional Model of Development: How Children and Contexts Shape Each Other; Sameroff, A., Ed.; American Psychological Association: Washington, DC, USA, 2009; pp. 3–21. [Google Scholar] [CrossRef]
- Jordan, J.V.; Walker, M.; Hartling, L.M. (Eds.) The Complexity of Connection; The Guildford Press: New York, NY, USA, 2004. [Google Scholar]
- Walker, M.; Rosen, W.B. (Eds.) How Connections Heal: Stories from Relational-Cultural Therapy; Guilford Press: New York, NY, USA, 2004. [Google Scholar]
- Motz, M.; Leslie, M.; Pepler, D.; Moore, T.; Freeman, P. Breaking the Cycle: Measures of Progress 1995–2005. J. Fas Int. 2006, 4, 1–134. [Google Scholar]
- Motz, M.; Leslie, M.; Pepler, D.J. Breaking the Cycle: A Comprehensive, Early Intervention Program Supporting Substance-Exposed Infants, Young Children, and Their Mothers. In Healthy Development, Healthy Communities; Pepler, D.J., Cummings, J., Craig, W.M., Eds.; PREVNet Series Volume IV: Kingston, ON, Canada, 2016; pp. 115–134. [Google Scholar]
- Van der Kolk, B.A. This Issue: Child Abuse and Victimization. Psychiatr. Ann. 2005, 35, 374–379. [Google Scholar] [CrossRef]
- Leslie, M.; Reynolds, W.; Motz, M.; Pepler, D.J. Building Connections: Supporting Community-Based Programs to Address Interpersonal Violence and Child Maltreatment; Mothercraft Press: Toronto, ON, Canada, 2016. [Google Scholar]
- Katz, E. Beyond the Physical Incident Model: How Children Living with Domestic Violence Are Harmed by and Resist Regimes of Coercive Control. Child Abus. Rev. 2016, 25, 46–59. [Google Scholar] [CrossRef] [Green Version]
- McTavish, J.R.; MacGregor, J.C.D.; Wathen, C.N.; MacMillan, H.L. Children’s Exposure to Intimate Partner Violence: An Overview. Int. Rev. Psychiatry 2016, 28, 504–518. [Google Scholar] [CrossRef]
- Crouch, E.; Probst, J.C.; Radcliff, E.; Bennett, K.J.; McKinney, S.H. Prevalence of Adverse Childhood Experiences (ACEs) among US Children. Child Abus. Negl. 2019, 92, 209–218. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Fuller-Thomson, E.; Baird, S.L.; Dhrodia, R.; Brennenstuhl, S. The Association between Adverse Childhood Experiences (ACEs) and Suicide Attempts in a Population-Based Study. Child Care Health Dev. 2016, 42, 725–734. [Google Scholar] [CrossRef]
- Kalmakis, K.A.; Chandler, G.E. Health Consequences of Adverse Childhood Experiences: A Systematic Review. J. Am. Assoc. Nurse Pract. 2015, 27, 457–465. [Google Scholar] [CrossRef]
- Fusco, R.A. Socioemotional Problems in Children Exposed to Intimate Partner Violence: Mediating Effects of Attachment and Family Supports. J. Interpers. Violence 2017, 32, 2515–2532. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, H.C.; Brown, G.L.; Mills-Koonce, W.R.; Cox, M.J. Intimate Partner Violence and Children’s Attachment Representations during Middle Childhood. J. Marriage Fam. 2017, 79, 865–878. [Google Scholar] [CrossRef] [PubMed]
- Oshri, A.; Sutton, T.E.; Clay-Warner, J.; Miller, J.D. Child Maltreatment Types and Risk Behaviors: Associations with Attachment Style and Emotion Regulation Dimensions. Pers. Individ. Dif. 2015, 73, 127–133. [Google Scholar] [CrossRef]
- Widom, C.S.; Czaja, S.J.; Kozakowski, S.S.; Chauhan, P. Does Adult Attachment Style Mediate the Relationship between Childhood Maltreatment and Mental and Physical Health Outcomes? Child Abus. Negl. 2018, 76, 533–545. [Google Scholar] [CrossRef]
- Leslie, M.; DeMarchi, G.; Motz, M. Breaking the Cycle: An Essay in Three Voices. In With Child—Substance Use During Pregnancy: A Woman-Centered Approach; Boyd, S., Marcellus, L., Eds.; Fernwood Publishing: Peterborough, UK, 2007; pp. 91–104. [Google Scholar]
- BTC Client; Toronto, ON, Canada. Personal Communication, 2006.
- Dodge, K.A.; Malone, P.S.; Lansford, J.E.; Miller, S.; Pettit, G.S.; Bates, J.E. A Dynamic Cascade Model of the Development of Substance-Use Onset. Monogr. Soc. Res. Child Dev. 2009, 74. [Google Scholar] [CrossRef]
- Eiden, R.D.; Lessard, J.; Colder, C.R.; Livingston, J.; Casey, M.; Leonard, K.E. Developmental Cascade Model for Adolescent Substance Use from Infancy to Late Adolescence. Dev. Psychol. 2016, 52, 1619–1633. [Google Scholar] [CrossRef] [Green Version]
- Otten, R.; Mun, C.J.; Shaw, D.S.; Wilson, M.N.; Dishion, T.J. A Developmental Cascade Model for Early Adolescent- Onset Substance Use: The Role of Early Childhood Stress. Addiction 2018, 114, 326–334. [Google Scholar] [CrossRef]
- Breaking the Cycle. Connections: A Group Intervention for Mothers and Children Experiencing Violence in Relationships; Mothercraft Press: Toronto, ON, Canada, 2014. [Google Scholar]
- Espinet, S.D.; Motz, M.; Jeong, J.J.; Jenkins, J.M.; Pepler, D. ‘Breaking the Cycle’ of Maternal Substance Use through Relationships: A Comparison of Integrated Approaches. Addict. Res. Theory 2016, 24, 375–388. [Google Scholar] [CrossRef]
- Andrews, N.C.Z.; Motz, M.; Pepler, D.J.; Jeong, J.J.; Khoury, J. Engaging Mothers with Substance Use Issues and Their Children in Early Intervention: Understanding Use of Service and Outcomes. Child Abus. Negl. 2018, 83, 10–20. [Google Scholar] [CrossRef]
- Appleyard, K.; Berlin, L.J.; Rosanbalm, K.D.; Dodge, K.A. Preventing Early Child Maltreatment: Implications from a Longitudinal Study of Maternal Abuse History, Substance Use Problems, and Offspring Victimization. Prev. Sci. 2011, 12, 139–149. [Google Scholar] [CrossRef] [Green Version]
- Widom, C.; Hiller-Sturmhofel, S. Alcohol Abuse as a Risk Factor for and Consequence of Child Abuse. Alcohol Res. Heal. 2001, 25, 52. [Google Scholar] [CrossRef]
- Widom, C.; Marmorstein, N.; White, R. Childhood Victimization and Illicit Drug Use in Middle Adulthood. Psychol. Addict. Behav. 2006, 20, 394. [Google Scholar] [CrossRef] [PubMed]
- Widom, C.; White, H.; Czaja, S.; Marmorstein, N. Long-Term Effects of Child Abuse and Neglect on Alcohol Use and Excessive Drinking in Middle Adulthood. J. Stud. Alcohol Drugs 2007, 68, 317–326. [Google Scholar] [CrossRef]
- Lansford, J.E.; Dodge, K.A.; Pettit, G.S.; Bates, J.E. Does Physical Abuse in Early Childhood Predict Substance Use in Adolescence and Early Adulthood? Child Maltreat. 2010, 15, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.M.; Teicher, M.H.; Polcari, A.; Renshaw, P.F. Abnormal T2 Relaxation Time in the Cerebellar Vermis of Adults Sexually Abused in Childhood: Potential Role of the Vermis in Stress-Enhanced Risk for Drug Abuse. Psychoneuroendocrinology 2002, 27, 231–244. [Google Scholar] [CrossRef]
- Repetti, R.L.; Taylor, S.E.; Seeman, T.E. Risky Families: Family Social Environments and the Mental and Physical Health of Offspring. Psychol. Bull. 2002, 128, 330. [Google Scholar] [CrossRef] [PubMed]
- Latuskie, K.A.; Andrews, N.C.Z.; Motz, M.; Leibson, T.; Austin, Z.; Ito, S.; Pepler, D.J. Reasons for Substance Use Continuation and Discontinuation during Pregnancy: A Qualitative Study. Women Birth 2019, 32, e57–e64. [Google Scholar] [CrossRef]
- McGee, R.A.; Wolfe, D.A.; Wilson, S.K. Multiple Maltreatment Experiences and Adolescent Behavior Problems: Adolescents’ Perspectives. Dev. Psychopathol. 1997, 9, 131–149. [Google Scholar] [CrossRef]
- Lansford, J.E.; Dodge, K.A.; Pettit, G.S.; Bates, J.E.; Crozier, J.; Kaplow, J. A 12-Year Prospective Study of the Long-Term Effects of Early Child Physical Maltreatment on Psychological, Behavioral, and Academic Problems in Adolescence. Arch. Pediatr. Adolesc. Med. 2002, 156, 824–830. [Google Scholar] [CrossRef]
- Macmillan, H.L.; Fleming, J.E.; Streiner, D.L.; Lin, E.; Boyle, M.H.; Jamieson, E.; Duku, E.K.; Walsh, C.A.; Wong, M.Y.Y.; Beardslee, W.R. Childhood Abuse and Lifetime Psychopathology in a Community Sample. Am. J. Psychiatry 2001, 158, 1878–1883. [Google Scholar] [CrossRef]
- Herringa, R.J.; Birn, R.M.; Ruttle, P.L.; Burghy, C.A.; Stodola, D.E.; Davidson, R.J.; Essex, M.J. Childhood Maltreatment Is Associated with Altered Fear Circuitry and Increased Internalizing Symptoms by Late Adolescence. Proc. Natl. Acad. Sci. USA 2013, 110, 19119–19124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cahill, L. Why Sex Matters for Neuroscience. Nat. Rev. Neurosci. 2006, 7, 477. [Google Scholar] [CrossRef] [PubMed]
- Widom, C.; Ireland, T.; Glynn, P.J. Alcohol Abuse in Abused and Neglected Children Followed-up: Are They at Increased Risk? J. Stud. Alcohol 1995, 56, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.Y.H.; Fong, D.Y.T.; Lai, V.; Tiwari, A. Bridging Intimate Partner Violence and the Human Brain: A Literature Review. Traumaviolenceabus. 2014, 15, 22–33. [Google Scholar] [CrossRef]
- Thomaes, K.; Dorrepaal, E.; Draijer, N.; De Ruiter, M.B.; Van Balkom, A.J.; Smit, J.H.; Veltman, D.J. Reduced Anterior Cingulate and Orbitofrontal Volumes in Child Abuse-Related Complex PTSD. J. Clin. Psychiatry 2010, 71, 1636–1644. [Google Scholar] [CrossRef]
- Cross, D.; Fani, N.; Powers, A.; Bradley, B. Neurobiological Development in the Context of Childhood Trauma. Clin. Psychol. Sci. Pract. 2017, 24, 111–124. [Google Scholar] [CrossRef]
- Carpenter, G.L.; Stacks, A.M. Developmental Effects of Exposure to Intimate Partner Violence in Early Childhood: A Review of the Literature. Child. Youth Serv. Rev. 2009, 31, 831–839. [Google Scholar] [CrossRef]
- Tarullo, A.R.; Gunnar, M.R. Child Maltreatment and the Developing HPA Axis. Horm. Behav. 2006, 50, 632–639. [Google Scholar] [CrossRef]
- Lupien, S.J.; Ouellet-Morin, I.; Herba, C.M.; Juster, R.; McEwen, B.S. From Vulnerability to Neurotoxicity: A Developmental Approach to the Effects of Stress on the Brain and Behavior. In Epigenetics and Neuroendocrinology; Springer: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- De Bellis, M.D.; Zisk, A. The Biological Effects of Childhood Trauma. Child Adolesc. Psychiatr. Clin. North Am. 2014, 23, 185–222. [Google Scholar] [CrossRef] [Green Version]
- Teicher, M.H. Wounds That Time Won’t Heal: The Neurobiology of Child Abuse. Cerebrum 2000, 2, 50–67. [Google Scholar]
- National Scientific Council on the Developing Child. Excessive Stress Disrupts the Architecture of the Developing Brain. Cent. Dev. Child Harv. Univ. 2005. [Google Scholar] [CrossRef]
- Shonkoff, J.P.; Garner, A.S. The Lifelong Effects of Early Childhood Adversity and Toxic Stress. Pediatrics 2012, 129, e232–e246. [Google Scholar] [CrossRef] [Green Version]
- McEwen, B.S.; Gianaros, P.J. Stress- and Allostasis-Induced Brain Plasticity. Annu. Rev. Med. 2010, 62, 431–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyce, W.T.; Ellis, B.J. Biological Sensitivity to Context: I. An Evolutionary-Developmental Theory of the Origins and Functions of Stress Reactivity. Dev. Psychopathol. 2005, 17, 271–301. [Google Scholar] [CrossRef] [PubMed]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [Green Version]
- Cowell, R.A.; Cicchetti, D.; Rogosch, F.A.; Toth, S.L. Childhood Maltreatment and Its Effect on Neurocognitive Functioning: Timing and Chronicity Matter. Dev. Psychopathol. 2015, 27, 521–533. [Google Scholar] [CrossRef] [Green Version]
- Tarter, R.E.; Kirisci, L.; Mezzich, A.; Cornelius, J.R.; Pajer, K.; Vanyukov, M.; Gardner, W.; Blackson, T.; Clark, D. Neurobehavioral Disinhibition in Childhood Predicts Early Age at Onset of Substance Use Disorder. Am. J. Psychiatry 2003, 160, 1078–1085. [Google Scholar] [CrossRef] [Green Version]
- Van Harmelen, A.L.; Van Tol, M.J.; Dalgleish, T.; Van der Wee, N.J.A.; Veltman, D.J.; Aleman, A.; Spinhoven, P.; Penninx, B.W.J.H.; Elzinga, B.M. Hypoactive Medial Prefrontal Cortex Functioning in Adults Reporting Childhood Emotional Maltreatment. Soc. Cogn. Affect. Neurosci. 2013, 9, 2026–2033. [Google Scholar] [CrossRef]
- Werner, K.; Gross, J.J. Emotion Regulation and Psychopathology: A Conceptual Framework. In Emotion Regulation and Psychopathology: A Transdiagnostic Approach to Etiology and Treatment; Guilford Press: New York, NY, USA, 2010. [Google Scholar] [CrossRef]
- Bariola, E.; Gullone, E.; Hughes, E.K. Child and Adolescent Emotion Regulation: The Role of Parental Emotion Regulation and Expression. Clin. Child Fam. Psychol. Rev. 2011, 14, 198. [Google Scholar] [CrossRef]
- Kober, H. Emotion Regulation in Substance Use Disorders. In Handbook of Emotion Regulation, 2nd ed.; Gross, J.J., Ed.; Guilford Press: New York, NY, USA, 2014. [Google Scholar]
- Wilcox, C.E.; Pommy, J.M.; Adinoff, B. Neural Circuitry of Impaired Emotion Regulation in Substance Use Disorders. Am. J. Psychiatry 2016, 173, 344–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Publications Office of the European Union. A Gender Perspective on Drug Use and Responding to Drug Problems; Publications Office of the European Union: Luxembourg, 2006. [Google Scholar]
- Arsova Netzelmann, T.; Dan, M.; Dreezens-Fuhrke, J.; Kalikov, J.; Karnite, A.; Kucharova, B.; Musat, G. Women Using Drugs: A Qualitative Situation and Needs Analysis. Cross-Country Rapid Assessment and Response (RAR Report); SPI Forschung gGmbH: Berlin, Germany, 2015. [Google Scholar]
- Jones, A.; Weston, S.; Moody, A.; Millar, T.; Dollin, L.; Anderson, T.; Donmall, M. The Drug Treatment Outcomes Research Study (DTORS): Baseline Report; Home Office: London, UK, 2007. [Google Scholar]
- Tuchman, E. Women and Addiction: The Importance of Gender Issues in Substance Abuse Research. J. Addict. Dis. 2010, 29, 127–138. [Google Scholar] [CrossRef] [PubMed]
- United Nations Office on Drugs and Crime (UNODC). World Drug Report 2016; United Nations Office on Drugs and Crime: Vienna, Austria, 2016. [Google Scholar]
- Bowlby, J. Attachment and Loss. Volume II: Separation; Basic Books: New York, NY, USA, 1973. [Google Scholar]
- Putnam, F.W. The Impact of Trauma on Child Development. Juv. Fam. Court J. 2006, 57, 1–11. [Google Scholar] [CrossRef]
- Stronach, E.P.; Toth, S.L.; Rogosch, F.; Oshri, A.; Manly, J.T.; Cicchetti, D. Child Maltreatment, Attachment Security, and Internal Representations of Mother and Mother-Child Relationships. Child Maltreat. 2011, 16, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, J.; Jackson, Y.; Huffhines, L.; Stone, K. Maltreatment, Coping, and Substance Use in Youth in Foster Care: Examination of Moderation Models. Child Maltreat. 2018, 23, 175–185. [Google Scholar] [CrossRef]
- Greger, H.K.; Myhre, A.K.; Klöckner, C.A.; Jozefiak, T. Childhood Maltreatment, Psychopathology and Well-Being: The Mediator Role of Global Self-Esteem, Attachment Difficulties and Substance Use. Child Abus. Negl. 2017, 70, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Hayre, R.S.; Goulter, N.; Moretti, M.M. Maltreatment, Attachment, and Substance Use in Adolescence: Direct and Indirect Pathways. Addict. Behav. 2019, 90, 196–203. [Google Scholar] [CrossRef]
- Lyons-Ruth, K. Contributions of the Mother–Infant Relationship to Dissociative, Borderline, and Conduct Symptoms in Young Adulthood. Infant Ment. Health J. 2008, 29, 203–218. [Google Scholar] [CrossRef] [Green Version]
- Lindberg, M.A.; Zeid, D. Interactive Pathways to Substance Abuse. Addict. Behav. 2017, 66, 76–82. [Google Scholar] [CrossRef]
- Schindler, A.; Bröning, S. A Review on Attachment and Adolescent Substance Abuse: Empirical Evidence and Implications for Prevention and Treatment. Subst. Abus. 2015, 36, 304–313. [Google Scholar] [CrossRef]
- Schindler, A.; Thomasius, R.; Sack, P.M.; Gemeinhardt, B.; Küstner, U.; Eckert, J. Attachment and Substance Use Disorders: A Review of the Literature and a Study in a Drug Dependent Adolescents. Attach. Hum. Dev. 2005, 7, 207–228. [Google Scholar] [CrossRef] [PubMed]
- Becoña Iglesias, E.; Del Río, E.F.; Calafat, A.; Fernández-Hermida, J.R. Attachment and Substance Use in Adolescence: A Review of Conceptual and Methodological Aspects. Adicciones 2014, 26, 77–86. [Google Scholar] [CrossRef] [Green Version]
- Unterrainer, H.F.; Hiebler-Ragger, M.; Rogen, L.; Kapfhammer, H.P. Addiction as an Attachment Disorder. Nervenarzt 2018, 89, 1043–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fairbairn, C.E.; Briley, D.A.; Kang, D.; Fraley, R.C.; Hankin, B.L.; Ariss, T. A Meta-Analysis of Longitudinal Associations between Substance Use and Interpersonal Attachment Security. Psychol. Bull. 2018, 144, 532. [Google Scholar] [CrossRef]
- Page, T. The Attachment Partnership as Conceptual Base for Exploring the Impact of Child Maltreatment. Child Adolesc. Soc. Work J. 1999, 16, 419–437. [Google Scholar] [CrossRef]
- Bretherton, I.; Munholland, K.A. Internal Working Models in Attachment Relationships: A Construct Revisited. In Handbook of Attachment: Theory, Research, and Clinical Applications; Cassidy, J., Shaver, P.R., Eds.; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Creeden, K. The Neurodevelopment Impact of Early Trauma and Insecure Attachment: Re-Thinking Our Understanding and Treatment of Sexual Behavior. Sex. Addict. Compulsivity 2004, 11, 223–247. [Google Scholar] [CrossRef]
- Cicchetti, D.; Cummings, E.M.; Greenberg, M.T.; Marvin, R. An Organizational Perspective on Attachment beyond Infancy: Implications for Theory, Measurement, and Research; University of Chicago Press: Chicago, IL, USA, 1990; pp. 3–49. [Google Scholar]
- Feeney, B.C.; Cassidy, J.; Ramos-Marcuse, F. The Generalization of Attachment Representations to New Social Situations: Predicting Behavior during Initial Interactions with Strangers. J. Pers. Soc. Psychol. 2008, 95, 1481. [Google Scholar] [CrossRef] [Green Version]
- Özcan, N.K.; Boyacioğlu, N.E.; Enginkaya, S.; Bilgin, H.; Tomruk, N.B. The Relationship between Attachment Styles and Childhood Trauma: A Transgenerational Perspective—A Controlled Study of Patients with Psychiatric Disorders. J. Clin. Nurs. 2016, 25, 2357–2366. [Google Scholar] [CrossRef]
- Sitko, K.; Bentall, R.P.; Shevlin, M.; O’Sullivan, N.; Sellwood, W. Associations between Specific Psychotic Symptoms and Specific Childhood Adversities Are Mediated by Attachment Styles: An Analysis of the National Comorbidity Survey. Psychiatry Res. 2014, 217, 202–209. [Google Scholar] [CrossRef]
- Finzi-Dottan, R.; Harel, G. Parents’ Potential for Child Abuse: An Intergenerational Perspective. J. Fam. Violence 2014, 29, 397–408. [Google Scholar] [CrossRef]
- Rada, C. Violence against Women by Male Partners and against Children within the Family: Prevalence, Associated Factors, and Intergenerational Transmission in Romania, a Cross-Sectional Study. BMC Public Health 2014, 14, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, J.C.; Allen, J.G.; Oldham, J.M.; Frueh, B.C. Exposure to Interpersonal Trauma, Attachment Insecurity, and Depression Severity. J. Affect. Disord. 2013, 149, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Milligan, K.; Usher, A.M.; Urbanoski, K.A. Supporting Pregnant and Parenting Women with Substance-Related Problems by Addressing Emotion Regulation and Executive Function Needs. Addict. Res. Theory 2017, 25, 251–261. [Google Scholar] [CrossRef]
- Motz, M.; Andrews, N.; Bondi, B.; Leslie, M.; Pepler, D. Addressing the Impact of Interpersonal Violence in Women Who Struggle with Substance Use through Developmental-Relational Strategies in a Community Program. Int. J. Environ. Res. Public Health 2019, 16, 4197. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Onset of Abuse | Physical Abuse (%) | Emotional Abuse (%) | Sexual Abuse (%) |
|---|---|---|---|
| Percentage of women reporting histories of abuse (total) | 88 | 89 | 76 |
| Onset (among women who reported abuse) | |||
| “As long as I can remember” | 5 | 10 | 0 |
| Early childhood | 9 | 7 | 22 |
| Childhood | 35 | 33 | 20 |
| Late childhood | 5 | 4 | 6 |
| Early adolescence | 6 | 6 | 13 |
| Adolescence | 15 | 24 | 12 |
| Late adolescence | 3 | 1 | 8 |
| Adulthood | 22 | 15 | 19 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrews, N.C.Z.; Motz, M.; Bondi, B.C.; Leslie, M.; Pepler, D.J. Using a Developmental-Relational Approach to Understand the Impact of Interpersonal Violence in Women Who Struggle with Substance Use. Int. J. Environ. Res. Public Health 2019, 16, 4861. https://doi.org/10.3390/ijerph16234861
Andrews NCZ, Motz M, Bondi BC, Leslie M, Pepler DJ. Using a Developmental-Relational Approach to Understand the Impact of Interpersonal Violence in Women Who Struggle with Substance Use. International Journal of Environmental Research and Public Health. 2019; 16(23):4861. https://doi.org/10.3390/ijerph16234861
Chicago/Turabian StyleAndrews, Naomi C. Z., Mary Motz, Bianca C. Bondi, Margaret Leslie, and Debra J. Pepler. 2019. "Using a Developmental-Relational Approach to Understand the Impact of Interpersonal Violence in Women Who Struggle with Substance Use" International Journal of Environmental Research and Public Health 16, no. 23: 4861. https://doi.org/10.3390/ijerph16234861