Proton Pump Inhibitors and Fracture Risk: A Review of Current Evidence and Mechanisms Involved



Abstract
:1. Introduction
2. The Relationship between PPIs and Fracture Risk
2.1. General Population
2.2. Patients with Comorbidities
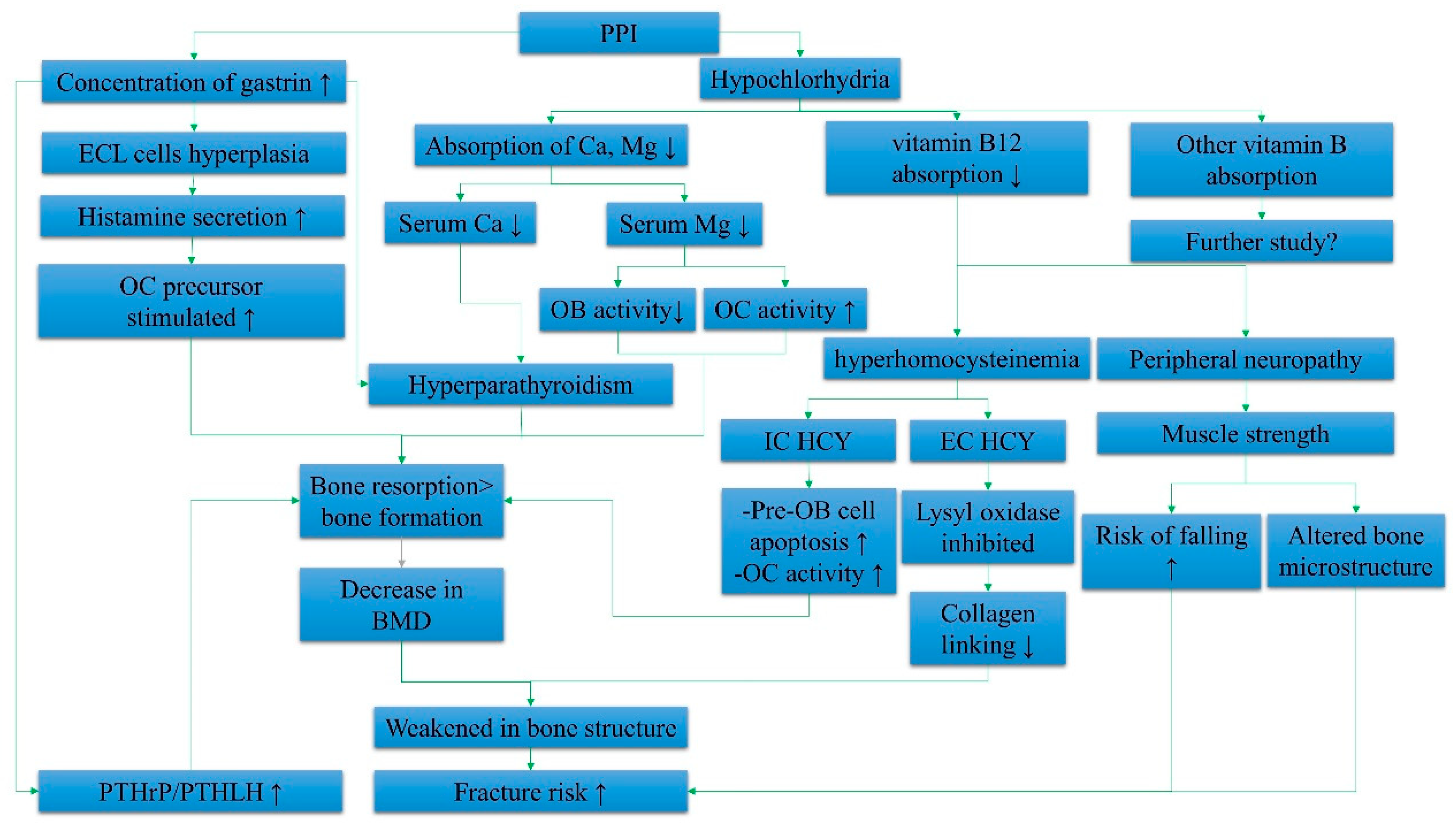
3. Mechanism of Bone Fractures induced by PPI
3.1. Hormones and PPIs
3.2. Micronutrients and PPIs
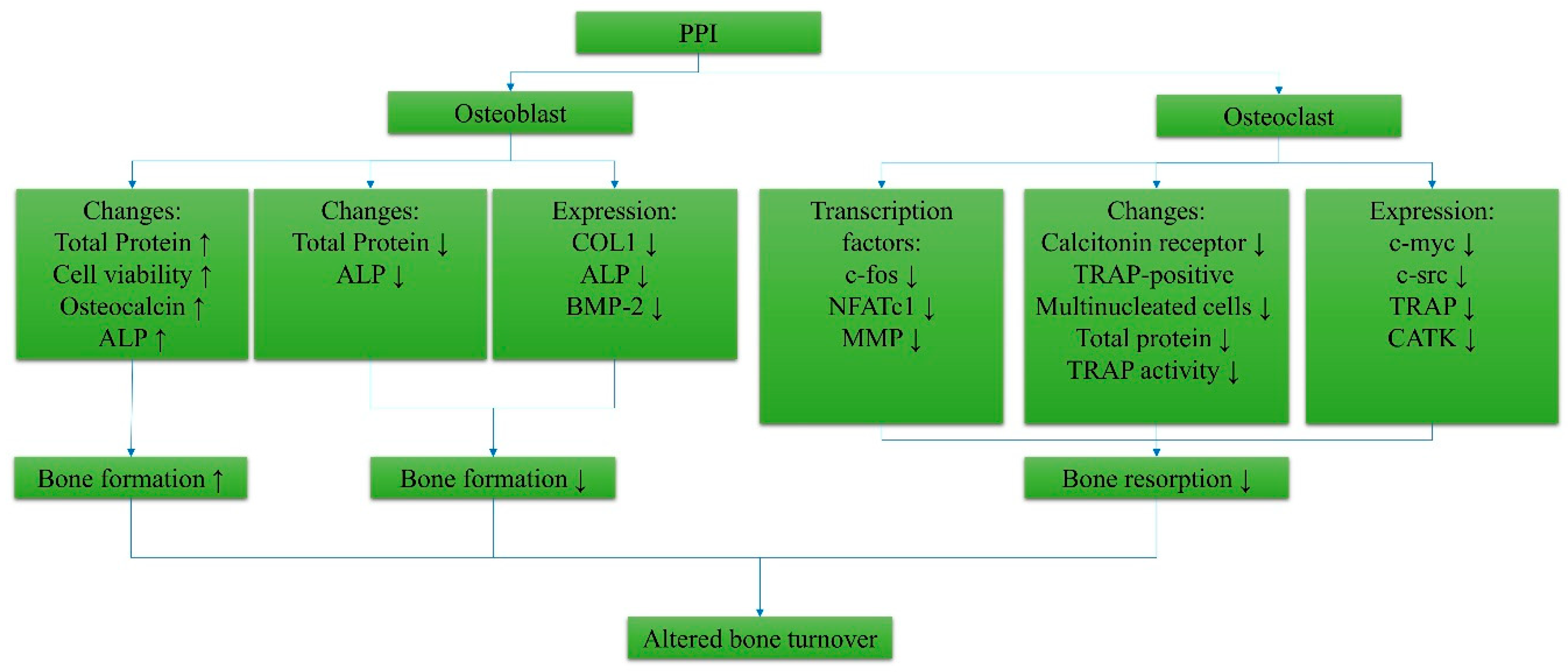
3.3. Effects of PPIs on Bone Cells
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shin, J.M.; Kim, N. Pharmacokinetics and Pharmacodynamics of the Proton Pump Inhibitors. J. Neurogastroenterol. Motil. 2013, 19, 25–35. [Google Scholar] [CrossRef] [Green Version]
- Leontiadis, G.I.; McIntyre, L.; Sharma, V.K.; Howden, C.W. Proton pump inhibitor treatment for acute peptic ulcer bleeding. In Cochrane Database of Systematic Reviews; Howden, C., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2004. [Google Scholar]
- Leontiadis, G.I.; Sharma, V.K.; Howden, C.W. Systematic review and meta-analysis of proton pump inhibitor therapy in peptic ulcer bleeding. BMJ 2005, 330, 568. [Google Scholar] [CrossRef]
- Vergara, M.; Catalan, M.; Gisbert, J.P.; Calvet, X. Meta-analysis: Role of Helicobacter pylori eradication in the prevention of peptic ulcer in NSAID users. Aliment. Pharmacol. Ther. 2005, 21, 1411–1418. [Google Scholar] [CrossRef] [PubMed]
- Heidelbaugh, J.J.; Kim, A.H.; Chang, R.; Walker, P.C. Overutilization of proton-pump inhibitors: What the clinician needs to know. Therap. Adv. Gastroenterol. 2012, 5, 219–232. [Google Scholar] [CrossRef]
- Welage, L.S.; Berardi, R.R. Evaluation of Omeprazole, Lansoprazole, Pantoprazole, and Rabeprazole in the Treatment of Acid-Related Diseases. J. Am. Pharm. Assoc. 2000, 40, 52–62. [Google Scholar] [CrossRef]
- Internal Clinical Guidelines Team (UK) Gastro-Oesophageal Reflux Disease and Dyspepsia in Adults: Investigation and Management. Available online: https://www.nice.org.uk/guidance/cg184/resources/gastrooesophageal-reflux-disease-and-dyspepsia-in-adults-investigation-and-management-pdf-35109812699845 (accessed on 30 April 2019).
- Freedberg, D.E.; Kim, L.S.; Yang, Y.X. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology 2017, 152, 706–715. [Google Scholar] [CrossRef]
- Lanza, F.L.; Chan, F.K.L.; Quigley, E.M.M.; Inadomi, J.; Baroni, D.; Bernstein, D.; Brugge, W.; Chang, L.; Cunningham, J.; Dendrinos, K.G.; et al. Guidelines for prevention of NSAID-related ulcer complications. Am. J. Gastroenterol. 2009, 104, 728–738. [Google Scholar] [CrossRef] [PubMed]
- McGowan, B.; Bennett, K.; Barry, M. Prescribing of anti-osteoporotic therapies following the use of proton pump inhibitors in general practice. Pharmacoepidemiol. Drug Saf. 2010, 19, 763–769. [Google Scholar] [CrossRef]
- Tables of Prescription Volumes and Government Costs (Expenditures) under the Pharmaceutical Benefits Scheme (PBS). Available online: http://www.pbs.gov.au/info/statistics/expenditure-and-prescriptions-30- 06-2014 (accessed on 15 July 2014).
- Burlington, M. Declining Medicine Use and Costs: For Better or Worse? A Review of the Use of Medicines in the United States in 2012; IMS Institute for Healthcare Informatics: Danbury, CT, USA, 2013. [Google Scholar]
- Savarino, V.; Dulbecco, P.; de Bortoli, N.; Ottonello, A.; Savarino, E. The appropriate use of proton pump inhibitors (PPIs): Need for a reappraisal. Eur. J. Int. Med. 2017, 37, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bahtiri, E.; Islami, H.; Hoxha, R.; Qorraj-Bytyqi, H.; Rexhepi, S.; Hoti, K.; Thaci, K.; Thaci, S.; Karakulak, C. Esomeprazole use is independently associated with significant reduction of BMD: 1-year prospective comparative safety study of four proton pump inhibitors. J. Bone Min. Metab. 2016, 34, 571–579. [Google Scholar] [CrossRef]
- Romdhane, H.; Ayadi, S.; Elleuch, N.; Abdelghani, K. Effect of long-term proton pump inhibitors on bone mineral density. Tunis Med. 2018, 96, 193–197. [Google Scholar] [PubMed]
- Arj, A.; Razavi Zade, M.; Yavari, M.; Akbari, H.; Zamani, B.; Asemi, Z. Proton pump inhibitors use and change in bone mineral density. Int. J. Rheum. Dis. 2016, 19, 864–868. [Google Scholar] [CrossRef]
- Glaser, D. Frederick Kaplan Osteoporosis: Definition and Clinical Presentation. Spine (Phila. Pa. 1976). 1997, 22, 12S–16S. [Google Scholar] [CrossRef]
- Kiebzak, G.M.; Beinart, G.A.; Perser, K.; Ambrose, C.G.; Siff, S.J.; Heggeness, M.H. Undertreatment of osteoporosis in men with hip fracture. Arch. Int. Med. 2002, 162, 2217–2222. [Google Scholar] [CrossRef]
- Penrod, J.D.; Litke, A.; Hawkes, W.G.; Magaziner, J.; Doucette, J.T.; Koval, K.J.; Silberzweig, S.B.; Egol, K.A.; Siu, A.L. The association of race, gender, and comorbidity with mortality and function after hip fracture. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 867–872. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef]
- Keene, G.S.; Parker, M.J.; Pryor, G.A. Mortality and morbidity after hip fractures. BMJ 1993, 307, 1248–1250. [Google Scholar] [CrossRef] [PubMed]
- Hasserius, R.; Karlsson, M.K.; Nilsson, B.E.; Redlund-Johnell, I.; Johnell, O. Prevalent vertebral deformities predict increased mortality and increased fracture rate in both men and women: A 10-year population-based study of 598 individuals from the Swedish cohort in the European Vertebral Osteoporosis Study. Osteoporos. Int. 2003, 14, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Campion, G.; Melton, L.J. Hip fractures in the elderly: A world-wide projection. Osteoporos. Int. 1992, 2, 285–289. [Google Scholar] [CrossRef]
- Panula, J.; Pihlajamäki, H.; Mattila, V.M.; Jaatinen, P.; Vahlberg, T.; Aarnio, P.; Kivelä, S.L. Mortality and cause of death in hip fracture patients aged 65 or older—A population-based study. BMC Musculoskelet. Disord. 2011, 12. [Google Scholar] [CrossRef]
- Gu, Q.; Koenig, L.; Mather, R.C.; Tongue, J. Surgery for Hip Fracture Yields Societal Benefits That Exceed the Direct Medical Costs. Clin. Orthop. Relat. Res. 2014, 472, 3536–3546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopic, S.; Geibel, J.P. Gastric Acid, Calcium Absorption, and Their Impact on Bone Health. Physiol. Rev. 2013, 93, 189–268. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.N.; Tomizza, M.; Wong-Pack, M.; Papaioannou, A.; Adachi, J.D. The relationship between long-term proton pump inhibitor therapy and skeletal frailty. Endocrine 2015, 49, 606–610. [Google Scholar] [CrossRef] [Green Version]
- Leontiadis, G.I.; Moayyedi, P. Proton Pump Inhibitors and Risk of Bone Fractures. Curr. Treat. Options Gastroenterol. 2014, 12, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Torio, T.; Miyajima, T.; Kim, Y.T.; Oda, H. Calcium, proton pump inhibitors, and fracture risk. Osteoporos. Int. 2016, 27, 349–350. [Google Scholar] [CrossRef]
- Lai, S.W.; Lin, C.H.; Lin, C.L.; Liao, K.F. Proton pump inhibitors therapy and the risk of hip fracture in older people in Taiwan. Eur. Geriatr. Med. 2018, 9, 169–174. [Google Scholar] [CrossRef]
- Reyes, C.; Formiga, F.; Coderch, M.; Hoyo, J.; Ferriz, G.; Casanovas, J.; Monteserín, R.; Brotons, C.; Rojas, M.; Moral, I. Use of proton pump inhibitors and risk of fragility hip fracture in a Mediterranean region. Bone 2013, 52, 557–561. [Google Scholar] [CrossRef]
- Adams, A.L.; Black, M.H.; Zhang, J.L.; Shi, J.M.; Jacobsen, S.J. Proton-pump inhibitor use and hip fractures in men: A population-based case-control study. Ann. Epidemiol. 2014, 24, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Lin, C.-L.; Kao, C.-H. Gastroesophageal reflux disease with proton pump inhibitor use is associated with an increased risk of osteoporosis: A nationwide population-based analysis. Osteoporos. Int. 2016, 27, 2117–2126. [Google Scholar] [CrossRef]
- Fraser, L.; Leslie, W.D.; Targownik, L.E.; Papaioannou, A.; Adachi, J.D. The effect of proton pump inhibitors on fracture risk: Report from the Canadian Multicenter Osteoporosis Study. Osteoporos. Int. 2013, 24, 1161–1168. [Google Scholar] [CrossRef]
- Cea Soriano, L.; Ruigõmez, A.; Johansson, S.; García Rodríguez, L.A. Study of the association between hip fracture and acid-suppressive drug use in a UK primary care setting. Pharmacotherapy 2014, 34, 570–581. [Google Scholar] [CrossRef] [PubMed]
- van der Hoorn, M.M.C.; Tett, S.E.; de Vries, O.J.; Dobson, A.J.; Peeters, G.M.E.E.G. The effect of dose and type of proton pump inhibitor use on risk of fractures and osteoporosis treatment in older Australian women: A prospective cohort study. Bone 2015, 81, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Harding, B.N.; Weiss, N.S.; Walker, R.L.; Larson, E.B.; Dublin, S. Proton pump inhibitor use and the risk of fractures among an older adult cohort. Pharmacoepidemiol. Drug Saf. 2018, 27, 596–603. [Google Scholar] [CrossRef]
- Wang, L.; Li, M.; Cao, Y.; Han, Z.; Wang, X.; Atkinson, E.J.; Liu, H.; Amin, S. Proton Pump Inhibitors and the Risk for Fracture at Specific Sites: Data Mining of the FDA Adverse Event Reporting System. Sci. Rep. 2017, 7, 5527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, J.; Heller, D.A.; Ahern, F.M.; Brown, T.V. The relationship between proton pump inhibitor adherence and fracture risk in the elderly. Calcif. Tissue Int. 2014, 94, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Moberg, L.M.E.; Nilsson, P.M.; Samsioe, G.; Borgfeldt, C. Use of proton pump inhibitors (PPI) and history of earlier fracture are independent risk factors for fracture in postmenopausal women the WHILA study. Maturitas 2014, 78, 310–315. [Google Scholar] [CrossRef]
- Freedberg, D.E.; Haynes, K.; Denburg, M.R.; Zemel, B.S.; Leonard, M.B.; Abrams, J.A.; Yang, Y.-X. Use of proton pump inhibitors is associated with fractures in young adults: A population-based study. Osteoporos. Int. 2015, 26, 2501–2507. [Google Scholar] [CrossRef]
- Lewis, J.R.; Barre, D.; Zhu, K.; Ivey, K.L.; Lim, E.M.; Hughes, J.; Prince, R.L. Long-term proton pump inhibitor therapy and falls and fractures in elderly women: A prospective cohort study. J. Bone Miner. Res. 2014, 29, 2489–2497. [Google Scholar] [CrossRef]
- Lee, J.; Youn, K.; Choi, N.-K.; Lee, J.-H.; Kang, D.; Song, H.-J.; Park, B.-J. A population-based case-control study: Proton pump inhibition and risk of hip fracture by use of bisphosphonate. J. Gastroenterol. 2013, 48, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Torvinen-Kiiskinen, S.; Tolppanen, A.M.; Koponen, M.; Tanskanen, A.; Tiihonen, J.; Hartikainen, S.; Taipale, H. Proton pump inhibitor use and risk of hip fractures among community-dwelling persons with Alzheimer’s disease—A nested case-control study. Aliment. Pharmacol. Ther. 2018, 47, 1135–1142. [Google Scholar] [CrossRef]
- Vangala, C.; Niu, J.; Lenihan, C.R.; Mitch, W.E.; Navaneethan, S.D.; Winkelmayer, W.C. Proton Pump Inhibitors, Histamine-2 Receptor Antagonists, and Hip Fracture Risk among Patients on Hemodialysis. Clin. J. Am. Soc. Nephrol. 2018, 13, 1534–1541. [Google Scholar] [CrossRef]
- Lenihan, C.R.; Sukumaran Nair, S.; Vangala, C.; Ramanathan, V.; Montez-Rath, M.E.; Winkelmayer, W.C. Proton Pump Inhibitor Use and Risk of Hip Fracture in Kidney Transplant Recipients. Am. J. Kidney Dis. 2017, 69, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-M.; Yang, S.-H.; Liang, C.-C.; Huang, H.-K. Proton pump inhibitor use and the risk of osteoporosis and fracture in stroke patients: A population-based cohort study. Osteoporos. Int. 2018, 29, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Dammann, H.G.; Burkhardt, F.; Wolf, N. The effects of oral rabeprazole on endocrine and gastric secretory function in healthy volunteers. Aliment Pharmacol. Ther. 1999, 13, 1195–1203. [Google Scholar] [CrossRef]
- Walsh, J.H.; Richardson, C.T.; Fordtran, J.S. pH dependence of acid secretion and gastrin release in normal and ulcer subjects. J. Clin. Investig. 1975, 55, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Campos, R.V.; Buchan, A.M.; Meloche, R.M.; Pederson, R.A.; Kwok, Y.N.; Coy, D.H. Gastrin Secretion From Human Antral G Cells in Culture. Gastroenterology 1990, 99, 36–44. [Google Scholar] [CrossRef]
- Solcia, E.; Vassallo, G.; Capella, C. Studies on the G cells of the pyloric mucosa, the probable site of gastrin secretion. Gut 1969, 10, 379–388. [Google Scholar] [CrossRef]
- Hersey, S.J.; Sachs, G. Gastric acid secretion. Physiol. Rev. 1995, 75, 155–189. [Google Scholar] [CrossRef] [PubMed]
- Arroyo Villarino, M.T.; Lanas Arbeloa, A.; Esteva Diaz, F.; Ortego Fernandez de Retana, J.; Sainz Samitier, R. Effects of long-term treatment with lansoprazole and omeprazole on serum gastrin and the fundic mucosa. Rev. Esp. Enferm. Dig. 1997, 89, 347–356. [Google Scholar] [PubMed]
- Sanduleanu, S.; Stridsberg, M.; Jonkers, D.; Hameeteman, W.; Biemond, I.; Lundqvist, G.; Lamers, C.; Stockbrugger, R.W. Serum gastrin and chromogranin A during medium- and long-term acid suppressive therapy: A case-control study. Aliment Pharmacol. Ther. 1999, 13, 145–153. [Google Scholar] [CrossRef]
- Nakamura, S.; Watanabe, H.; Yokota, T.; Matsui, H.; Onji, M.; Maeyama, K. Effect of rabeprazole on histamine synthesis in enterochromaffin-like cells of mast cell-deficient (Ws/Ws) rats. Eur. J. Pharmacol. 2000, 394, 9–16. [Google Scholar] [CrossRef]
- Tanabe, T.; Murata, I.; Karasuyama, M.; Shin, M.; Ueoka, R.; Fujiwara, K. Immunoelectron microscopic study for histamine in the gastric enterochromaffin-like cells of rats treated with the proton pump inhibitor lansoprazole. Histochem. Cell Biol. 2003, 120, 401–408. [Google Scholar] [CrossRef]
- Yokota, T.; Matsui, H.; Matsuura, B.; Maeyama, K.; Onji, M. Direct effects of proton pump inhibitors on histamine release from rat enterochromaffin-like cells. Eur. J. Pharmacol. 2003, 481, 233–240. [Google Scholar] [CrossRef]
- Rindi, G.; Fiocca, R.; Morocutti, A.; Jacobs, A.; Miller, N.; Thjodleifsson, B. Effects of 5 years of treatment with rabeprazole or omeprazole on the gastric mucosa. Eur. J. Gastroenterol. Hepatol. 2005, 17, 559–566. [Google Scholar] [CrossRef]
- Nishi, T.; Makuuchi, H.; Weinstein, W.M. Changes in gastric ECL cells and parietal cells after long-term administration of high-dose omeprazole to patients with Barrett’s esophagus. Tokai J. Exp. Clin. Med. 2005, 30, 117–121. [Google Scholar]
- Bektas, M.; Sarac, N.; Cetinkaya, H.; Toruner, M.; Erdemli, E.; Keskin, O.; Soykan, I.; Oktay, E.I.; Korkut, E.; Ustun, Y.; et al. Effects of Helicobacter pylori infection and long-term proton pump inhibitor use on enterochromaffin-like cells. Ann. Gastroenterol. 2012, 25, 123–127. [Google Scholar]
- Schayer, R.W. Enzymatic formation of histamine from histidine. In Histamine and Anti-histaminics; Springer: Berlin, Germany, 1966; pp. 688–725. [Google Scholar]
- Schayer, R.W. Biogenesis of histamine. Handb. Exp. Pharmacol. 1952, 18, 109–128. [Google Scholar]
- Biosse-Duplan, M.; Baroukh, B.; Dy, M.; De Vernejoul, M.C.; Saffar, J.L. Histamine promotes osteoclastogenesis through the differential expression of histamine receptors on osteoclasts and osteoblasts. Am. J. Pathol. 2009, 174, 1426–1434. [Google Scholar] [CrossRef]
- Gagnemo-Persson, R.; Hakanson, R.; Sundler, F.; Persson, P. Growth of the parathyroid glands in omeprazole-treated chickens. Scand. J. Gastroenterol. 1994, 29, 493–497. [Google Scholar] [CrossRef]
- Gagnemo-Persson, R.; Samuelsson, A.; Hakanson, R.; Persson, P. Chicken parathyroid hormone gene expression in response to gastrin, omeprazole, ergocalciferol, and restricted food intake. Calcif. Tissue Int. 1997, 61, 210–215. [Google Scholar] [CrossRef]
- Mizunashi, K.; Furukawa, Y.; Katano, K.; Abe, K. Effect of omeprazole, an inhibitor of H+,K(+)-ATPase, on bone resorption in humans. Calcif. Tissue Int. 1993, 53, 21–25. [Google Scholar] [CrossRef]
- Grimelius, L.; Johansson, H.; Lundqvist, G.; Olazabal, A.; Polak, J.H.; Pearse, G.E. The parathyroid glands in experimentally induced hypergastrinemia in the rat. Scand. J. Gastroenterol. 1977, 12, 739–744. [Google Scholar] [CrossRef]
- Yang, Y.-X. Chronic proton pump inihibitor therapy and calcium metabolism. Curr. Gastroenterol. Rep. 2012, 14, 473–479. [Google Scholar] [CrossRef]
- Hinson, A.M.; Wilkerson, B.M.; Rothman-Fitts, I.; Riggs, A.T.; Stack, B.C., Jr.; Bodenner, D.L. Hyperparathyroidism Associated with Long-Term Proton Pump Inhibitors Independent of Concurrent Bisphosphonate Therapy in Elderly Adults. J. Am. Geriatr. Soc. 2015, 63, 2070–2073. [Google Scholar] [CrossRef]
- Selking, Ö; Borch, K.; Johansson, H.; Ljunghall, S.; Wide, L. Evaluation of Parathyroid Function in Patients with Hypergastrinaemia and Pernicious Anaemia. Upsala J. Med. Sci. 1982, 87, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Al Menhali, A.; Keeley, T.M.; Demitrack, E.S.; Samuelson, L.C. Gastrin induces parathyroid hormone-like hormone expression in gastric parietal cells. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G649–G657. [Google Scholar] [CrossRef]
- Karaplis, A.C.; Vautour, L. Parathyroid hormone-related peptide and the parathyroid hormone/parathyroid hormone-related peptide receptor in skeletal development. Curr. Opin. Nephrol. Hypertens. 1997, 6, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Amizuka, N.; Ozawa, H.; Sasaki, T. The biological action of parathyroid hormone-related peptide (PTHrP) and fibroblast growth factor receptor 3 (FGFR3) on bone and cartilage. Kaibogaku Zasshi 2000, 75, 415–425. [Google Scholar]
- Chung, U.; Kronenberg, H.M. Parathyroid hormone-related peptide and Indian hedgehog. Curr. Opin. Nephrol. Hypertens 2000, 9, 357–362. [Google Scholar] [CrossRef]
- Grill, V.; Rankin, W.; Martin, T.J. Parathyroid hormone-related protein (PTHrP) and hypercalcaemia. Eur. J. Cancer 1998, 34, 222–229. [Google Scholar] [CrossRef]
- Inoue, D.; Matsumoto, T. Parathyroid hormone-related peptide and bone: Pathological and physiological aspects. Biomed. Pharmacother. 2000, 54, 32s–41s. [Google Scholar] [CrossRef]
- Juppner, H. Role of parathyroid hormone-related peptide and Indian hedgehog in skeletal development. Pediatr. Nephrol. 2000, 14, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Suda, N. Parathyroid hormone-related protein (PTHrP) as a regulating factor of endochondral bone formation. Oral. Dis. 1997, 3, 229–231. [Google Scholar] [CrossRef] [PubMed]
- New, S.A. Bone health: The role of micronutrients. Br. Med. Bull. 1999, 55, 619–633. [Google Scholar] [CrossRef] [PubMed]
- Nieves, J.W. Osteoporosis: The role of micronutrients. Am. J. Clin. Nutr. 2005, 81, 1232S–1239S. [Google Scholar] [CrossRef]
- Goltzman, D.; Mannstadt, M.; Marcocci, C. Physiology of the Calcium-Parathyroid Hormone-Vitamin D Axis. Front. Horm. Res. 2018, 50, 1–13. [Google Scholar]
- Kroll, M. Parathyroid Hormone Temporal Effects on Bone Formation and Resorption. Bull. Math. Biol. 2000, 62, 163–188. [Google Scholar] [CrossRef] [PubMed]
- Moe, S.M. Disorders Involving Calcium, Phosphorus, and Magnesium. Prim. Care 2008, 35, 215–237. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, M.B.; Madden, D.M.; Murray, A.M.; Heaney, R.P.; Kerzner, L.J. Effects of proton pump inhibitors on calcium carbonate absorption in women: A randomized crossover trial. Am. J. Med. 2005, 118, 778–781. [Google Scholar] [CrossRef]
- Castiglioni, S.; Cazzaniga, A.; Albisetti, W.; Maier, J. Magnesium and Osteoporosis: Current State of Knowledge and Future Research Directions. Nutrients 2013, 5, 3022–3033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begley, J.; Smith, T.; Barnett, K.; Strike, P.; Azim, A.; Spake, C.; Richardson, T. Proton pump inhibitor associated hypomagnasaemia—A cause for concern? Br. J. Clin. Pharmacol. 2016, 81, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Cegla, J. The association between the use of proton pump inhibitors and the risk of hypomagnesemia: A systematic review and meta-analysis. Ann. Clin. Biochem. 2015, 52, 302. [Google Scholar] [CrossRef] [PubMed]
- Chowdhry, M.; Shah, K.; Kemper, S.; Zekan, D.; Carter, W.; McJunkin, B. Proton pump inhibitors not associated with hypomagnesemia, regardless of dose or concomitant diuretic use. J. Gastroenterol. Hepatol. 2018, 33, 1717–1721. [Google Scholar] [CrossRef] [PubMed]
- Bahtiri, E.; Islami, H.; Hoxha, R.; Gashi, A.; Thaci, K.; Karakulak, C.; Thaci, S.; Qorraj Bytyqi, H. Proton pump inhibitor use for 12 months is not associated with changes in serum magnesium levels: A prospective open label comparative study. Turk. J. Gastroenterol. 2017, 28, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.; Chiu, D.Y.; Kalra, P.A.; Green, D. Prevalence and outcomes of proton pump inhibitor associated hypomagnesemia in chronic kidney disease. PLoS ONE 2018, 13, e0197400. [Google Scholar] [CrossRef]
- Mikolasevic, I.; Milic, S.; Stimac, D.; Zaputovic, L.; Lukenda Zanko, V.; Gulin, T.; Jakopcic, I.; Klaric, D.; Gulin, M.; Orlic, L. Is there a relationship between hypomagnesemia and proton-pump inhibitors in patients on chronic hemodialysis? Eur. J. Int. Med. 2016, 30, 99–103. [Google Scholar] [CrossRef]
- Erdem, E. Proton pump inhibitors use in hemodialysis patients and serum magnesium levels. Int. J. Clin. Exp. Med. 2015, 8, 21689–21693. [Google Scholar]
- Hartman, B.; Donnelly-VanderLoo, M.; Watson, T.; O’Connor, C.; Madill, J. Proton-pump inhibitor therapy and vitamin B12 status in an inpatient hospital setting. Appl. Physiol. Nutr. Metab 2016, 41, 1071–1076. [Google Scholar] [CrossRef]
- Valuck, R.J.; Ruscin, J.M. A case-control study on adverse effects: H2 blocker or proton pump inhibitor use and risk of vitamin B12 deficiency in older adults. J. Clin. Epidemiol. 2004, 57, 422–428. [Google Scholar] [CrossRef]
- Herrmann, M.; Peter Schmidt, J.; Umanskaya, N.; Wagner, A.; Taban-Shomal, O.; Widmann, T.; Colaianni, G.; Wildemann, B.; Herrmann, W. The role of hyperhomocysteinemia as well as folate, vitamin B6 and B12 deficiencies in osteoporosis—A systematic review. Clin. Chem. Lab. Med. 2007, 45, 1621–1632. [Google Scholar] [CrossRef]
- Seshadri, S.; Beiser, A.; Selhub, J.; Jacques, P.F.; Rosenberg, I.H.; D’Agostino, R.B.; Wilson, P.W.F.; Wolf, P.A. Plasma Homocysteine as a Risk Factor for Dementia and Alzheimer’s Disease. N. Engl. J. Med. 2002, 346, 476–483. [Google Scholar] [CrossRef]
- Clarke, R.; Smith, A.D.; Jobst, K.A.; Refsum, H.; Sutton, L.; Ueland, P.M. Folate, Vitamin B12, and Serum Total Homocysteine Levels in Confirmed Alzheimer Disease. Arch. Neurol. 1998, 55, 1449. [Google Scholar] [CrossRef]
- Zhao, Y.; Shen, L.; Ji, H.-F. Alzheimer’s Disease and Risk of Hip Fracture: A Meta-Analysis Study. Sci. World J. 2012, 2012, 1–5. [Google Scholar] [CrossRef]
- Marcuard, S.P.; Albernaz, L.; Khazanie, P.G. Omeprazole therapy causes malabsorption of cyanocobalamin (vitamin B12). Ann. Int. Med. 1994, 120, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.B.; Nagaraja, V.; Kapur, A.; Eslick, G.D. Association between vitamin B12 deficiency and long-term use of acid-lowering agents: A systematic review and meta-analysis. Int. Med. J. 2015, 45, 409–416. [Google Scholar] [CrossRef]
- Dai, Z.; Koh, W.-P. B-Vitamins and Bone Health–A Review of the Current Evidence. Nutrients 2015, 7, 3322–3346. [Google Scholar] [CrossRef] [Green Version]
- Dai, Z.; Wang, R.; Ang, L.W.; Yuan, J.-M.; Koh, W.-P. Dietary B vitamin intake and risk of hip fracture: The Singapore Chinese Health Study. Osteoporos. Int. 2013, 24, 2049–2059. [Google Scholar] [CrossRef]
- Lapumnuaypol, K.; Thongprayoon, C.; Wijarnpreecha, K.; Tiu, A.; Cheungpasitporn, W. Risk of Fall in Patients Taking Proton Pump Inhibitors: A Meta-Analysis. QJM 2018, 112, 115–121. [Google Scholar] [CrossRef]
- Fratoni, V.; Brandi, M.L. B vitamins, Homocysteine and bone health. Nutrients 2015, 7, 2176–2192. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Gollhofer, A.; Hortobágyi, T.; Kressig, R.W.; Muehlbauer, T. The Importance of Trunk Muscle Strength for Balance, Functional Performance, and Fall Prevention in Seniors: A Systematic Review. Sport. Med. 2013, 43, 627–641. [Google Scholar] [CrossRef]
- Pang, M.Y.C.; Eng, J.J. Muscle strength is a determinant of bone mineral content in the hemiparetic upper extremity: Implications for stroke rehabilitation. Bone 2005, 37, 103–111. [Google Scholar] [CrossRef] [Green Version]
- McMichael, K.A.; Vander Bilt, J.; Lavery, L.; Rodriguez, E.; Ganguli, M. Simple Balance and Mobility Tests Can Assess Falls Risk When Cognition Is Impaired. Geriatr. Nurs. (Minneap). 2008, 29, 311–323. [Google Scholar] [CrossRef] [Green Version]
- Oberlin, B.; Tangney, C.; Gustashaw, K.; Rasmussen, H. Vitamin B12 Deficiency in Relation to Functional Disabilities. Nutrients 2013, 5, 4462–4475. [Google Scholar] [CrossRef] [Green Version]
- Hadjidakis, D.J.; Androulakis, I.I. Bone remodeling. Ann. N. Y. Acad. Sci. 2006, 1092, 385–396. [Google Scholar] [CrossRef]
- Hyun, J.J.; Chun, H.J.; Keum, B.; Seo, Y.S.; Kim, Y.S.; Jeen, Y.T.; Lee, H.S.; Um, S.H.; Kim, C.D.; Ryu, H.S.; et al. Effect of omeprazole on the expression of transcription factors in osteoclasts and osteoblasts. Int. J. Mol. Med. 2010, 26, 877–883. [Google Scholar] [PubMed]
- Costa-Rodrigues, J.; Reis, S.; Teixeira, S.; Lopes, S.; Fernandes, M.H. Dose-dependent inhibitory effects of proton pump inhibitors on human osteoclastic and osteoblastic cell activity. FEBS J. 2013, 280, 5052–5064. [Google Scholar] [CrossRef] [Green Version]
- Prause, M.; Seeliger, C.; Unger, M.; Balmayor, E.R.; van Griensven, M.; Haug, A.T. Pantoprazole Decreases Cell Viability and Function of Human Osteoclasts In Vitro. Mediat. Inflamm 2015, 2015, 413097. [Google Scholar] [CrossRef]
- Prause, M.; Seeliger, C.; Unger, M.; van Griensven, M.; Haug, A.T. Pantoprazole increases cell viability and function of primary human osteoblasts in vitro. Injury 2014, 45, 1156–1164. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Study Design and Population Characteristics | Major Findings |
|---|---|---|
| POSITIVE ASSOCIATION | ||
| [34] | Design: population-based cohort, follow-up period: 10 years Subjects: Canadian PPI users (n = 261), non-users (n = 9162) Mean age in years (SD): PPI = 67.6 (11.1), without PPI = 61.9 (13.4) Gender, %: PPI male (M): 21.8, female (F): 78.2; without PPI M: 30.9, F: 69.1 | PPI use increased ten-year but not five-year risk of any fracture. PPI use did not increase hip fracture risk. |
| [43] | Design: case-control Subjects: Korean elderly ≥65 (mean: 77.7 ± 7.3 for both case and control) Sample: n = 24,710 (cases) n = 98,642 (control) Gender, %: M case and control: 26.6; F case: 73.5, control: 73.4 | Cumulative exposure or ever exposure to PPI increased hip fracture risk. Hip fracture risk increased even the last dose used was 90 days or more prior to index date. The use of pantoprazole, rabeprazole, and omeprazole increased the hip fracture risk, but not esomeprazole and lansoprazole. |
| [32] | Design: case-controlSubjects: USA men. n = 6774 (control) n = 6774 (case) Age (for both case, control): 14.7% <60, 85.3% ≥60 Race, %: White (71.4), Black (6.6), Hispanic (11.1), other (10.9) (for both case and control) | Ever use of omeprazole or medication possession ratio (MPR) >80% increased the hip fracture risk in a time-dependent manner. The most recent use (1–7 days) prior to index date (ID) increased the hip fracture risk. Ever use of pantoprazole or any MPR did not increase hip fracture risk. Pantoprazole use for 417–1931 days or if the last dose was 1–33 days prior to ID increased hip fracture risk. |
| [39] | Design: retrospective cohort study, follow-up (years): 5 Subjects: USA elderly (Caucasians and non-Caucasians) >64 years n = 1604 (PPI), n = 23,672 (without PPI) Gender, %: PPI: M: 17.1 F: 82.9; without PPI: M: 18.7 F: 81.3 | The use of PPI increased the risk of any fractures, major osteoporotic fractures, hip fracture, vertebral fracture and other fractures but not wrist and humerus fracture. For PPI adherence, proportion of days covered (PDC) ≥ 0.80 increased the risk of any fractures, major osteoporotic fracture and other fracture. While for PDC 0.40–0.79, the risk of any fracture also increased. |
| [42] | Design: prospective cohort study Subjects: Australian elderly woman n (without PPI) = 925, n (PPI) = 120 Mean age in years: 76.5 ± 2.6 (non), 77.5 ± 2.5 (PPI) | Risk of fracture increased with PPI therapy ≥1 year or ≥1.5 standard daily dose. |
| [40] | Design: Retrospective cohort, mean follow-up period: 14.4 years Subjects: 6917 Swedish women Mean age in years: 56.4 (50.0–64.0) | The use of PPI increased fracture risk. |
| [35] | Design: cohort with a nested case-control Subjects: UK men and women aged 40–89 n = 10,958 (cases) n = 20,000 (control) Age, %: Case: <60: 9, ≥60: 91; Control: <60: 9.7, ≥60: 90.3 Gender, %: case M: 24.8, F: 75.2; control: M: 25.6, F: 74.4 | Current use of single type PPI or the last dose of PPI 31–90 days prior to index date (ID) increased hip fracture risk. Medium and high PPI did increase the hip fracture risk. The relationship was not in a time-dependent manner. Only omeprazole increased the hip fracture risk while others such as lansoprazole, pantoprazole, rabeprazole, and esomeprazole did not. |
| [41] | Design: case-control, mean follow-up period: 5 (SD 3.3) years Subjects: USA children, young adults (n = 124,799 cases and 605,643 controls) Age: case, %: <18: 69.8, ≥18: 30.2; Control, %:<18: 70, ≥18: 30 Gender, %: Case M: 65.6, F: 34.4; Control M: 65.4, F: 34.6 | Children (<18 years): maximal dose of PPI for daily use or less increased fracture risk but not in a cumulative exposure manner. Young adults (≥18 years): maximal dose of PPI was associated with increased fracture risk in a time-dependent manner. |
| [36] | Design: prospective cohort, mean follow-up period: 6.6 years Subjects: Australian elderly women n (PPI) = 1396, n (non-PPI users) = 1338 Mean age in years: 78.2 (1.4) (PPI users) 78.3 (1.5) (non-PPI users) | PPI use increased fracture risk when medication adherence increased. Only rabeprazole and multiple types of PPI were associated with increased fracture risk while others such as omeprazole, lansoprazole, pantoprazole, and esomeprazole were not associated. |
| [46] | Design: retrospective nested matched case-control, follow-up period: 6.9 ± 5.3 years. Subjects: Kidney transplant recipient (n = 231 for case, 15,575 for control) Mean age in years: 51.8 ± 12.9 (case), 51.2 ± 10.4 (control) Gender, %: Case: M: 56.8; Control: M: 49.8 Race, %: African American: 11.3 (case), 7.2 (control) Non-African American Hispanic: 19 (case), 33.4 (control) Missing: 4.3 (case), 1.2 (control) | Use of PPI in ≥80% of the time in one year increased hip fracture risk. |
| [38] | Design: retrospective study, using Food and Drug Administration Adverse Event Reporting System Data Mining Set with post-marketing surveillance data. Subjects: 169,563 entries in the database with PPI use. | Mean age of PPI users reporting fracture was 65.3 years, and with a gender ratio (F:M) of 3.4:1. Fractures reported to be associated with PPI use included bone sites rich in trabecular bones and atypical bone sites, like rib. PPI use (overall) and 5 generic ingredients (omeprazole, esomeprazole, pantoprazole, lansoprazole, rabeprazole) were reported to be associated with fractures. |
| [44] | Design: nested case-control Subjects: Finish elderly with Alzheimer’s diseasen (fracture) = 4818, n (control) = 19,235 Mean age in years: 84.1 (cases), 84.0 (control) Gender, %: Both: F: 75, M: 25 | Long-term or cumulative PPI use did not increase hip fracture risk, but risk of hip fracture was modestly increased during current short-term PPI use. |
| [47] | Design: retrospective cohort study mean follow-up period: 4.8 years Subjects: Taiwanese stroke patients n = 5298 (For both PPI and non-users) Mean age in years: Yes: 66.7 ± 12.7; No: 66.9 ± 13.1 Gender, %: Yes: M: 62.8, F: 37.2; No: M: 63.7, F: 36.3 | PPI use increased risk of hip and vertebral fracture. Cumulative exposure of PPI increased vertebral fracture. |
| [45] | Design: retrospective case-control Subjects: n = 4551 (cases), n = 45,510 (controls) Mean age in years: 71 (cases), 61 (controls) Gender, %: case F: 59, M: 41; control F: 52, M: 48 | End-stage kidney disease patients on hemodialysis and PPIs were associated with hip fracture events. |
| NIL RELATIONSHIP | ||
| [31] | Design: Retrospective multicenter case-control Subjects = Spanish elderly 82 (SD = 8.8) (n = 358 case, n = 698 controls) Mean age in years: 82 (SD = 8.8) (case), 81.9 (control) Gender, %: case F: 77.1, M: 22.9; control F: 76.9, M: 23.1 | Continuous/discontinuous exposure of PPI did not increase hip fracture risk. Types and dose of PPI was not related to increased hip fracture risk. |
| [33] | Design: retrospective cohort, mean follow-up period: 3.45 (GERD) 3.55 (control) Subjects: Taiwanese GERD patients on PPI (n = 10,620; men: 56.2%) and control (n = 20,738; men: 56%) Mean age in years: 46.6 (SD 14.1); (Control) 47.1 (SD 14.1) (GERD) | GERD patients using PPI did not have an increased hip fracture risk. |
| [30] | Design: case-control Subjects: Taiwanese elderly, n = 7208 Mean age in years: 79.8 ± 7.0 (cases) 79.7 ± 6.9 (control) Gender, %: F: 60.3, M: 39.7 (both) | When the last dose of PPI was ≥12 months prior to index date, hip fracture risk increased. The risk was not related to cumulative duration or cumulative dosage of PPI use. |
| [37] | Design: retrospective cohort; follow-up period: 6.1 years Sample: 4438 USA men (42%) and women (58%) Age in years: median = 74, IQR = 69.8–79.5 Gender, %: F: 58, M: 42 Race, %: White (89.7), Black (3.8) Asian (3.1), other (3.3) | Use of PPI was not associated with increased risk of fractures. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thong, B.K.S.; Ima-Nirwana, S.; Chin, K.-Y. Proton Pump Inhibitors and Fracture Risk: A Review of Current Evidence and Mechanisms Involved. Int. J. Environ. Res. Public Health 2019, 16, 1571. https://doi.org/10.3390/ijerph16091571
Thong BKS, Ima-Nirwana S, Chin K-Y. Proton Pump Inhibitors and Fracture Risk: A Review of Current Evidence and Mechanisms Involved. International Journal of Environmental Research and Public Health. 2019; 16(9):1571. https://doi.org/10.3390/ijerph16091571
Chicago/Turabian StyleThong, Benjamin Ka Seng, Soelaiman Ima-Nirwana, and Kok-Yong Chin. 2019. "Proton Pump Inhibitors and Fracture Risk: A Review of Current Evidence and Mechanisms Involved" International Journal of Environmental Research and Public Health 16, no. 9: 1571. https://doi.org/10.3390/ijerph16091571