COVID-19 Epidemic in Bangladesh among Rural and Urban Residents: An Online Cross-Sectional Survey of Knowledge, Attitudes, and Practices

 ,
, 


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Respondents
2.2. Instrument
2.3. Data Collection
2.4. Sampling
2.5. Data Management and Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics
3.2. Correct Knowledge of Respondents on COVID-19
3.3. Attitudes of the Respondents towards COVID-19
3.4. Good Preventive Practices against COVID-19
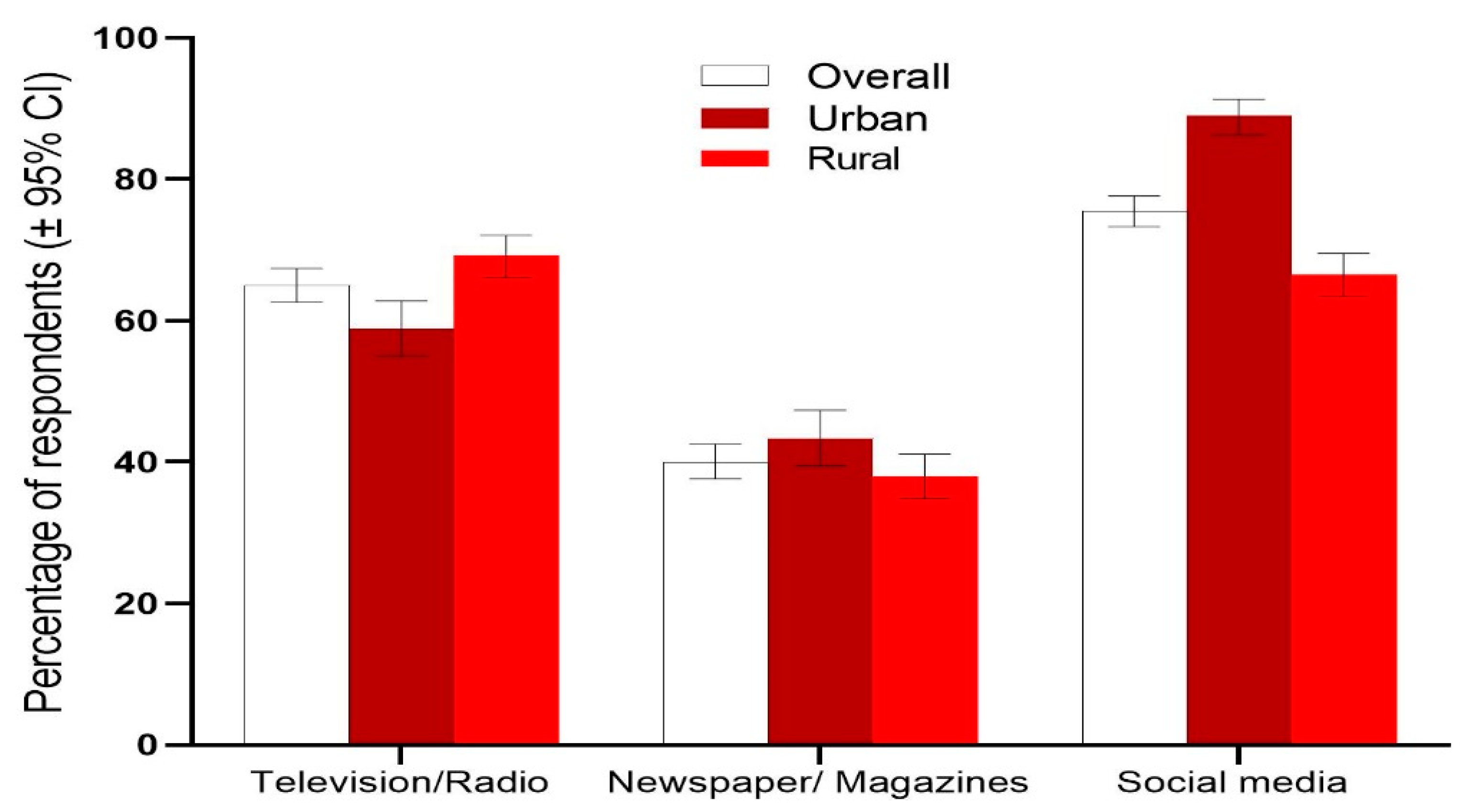
3.5. Sources of Information on COVID-19
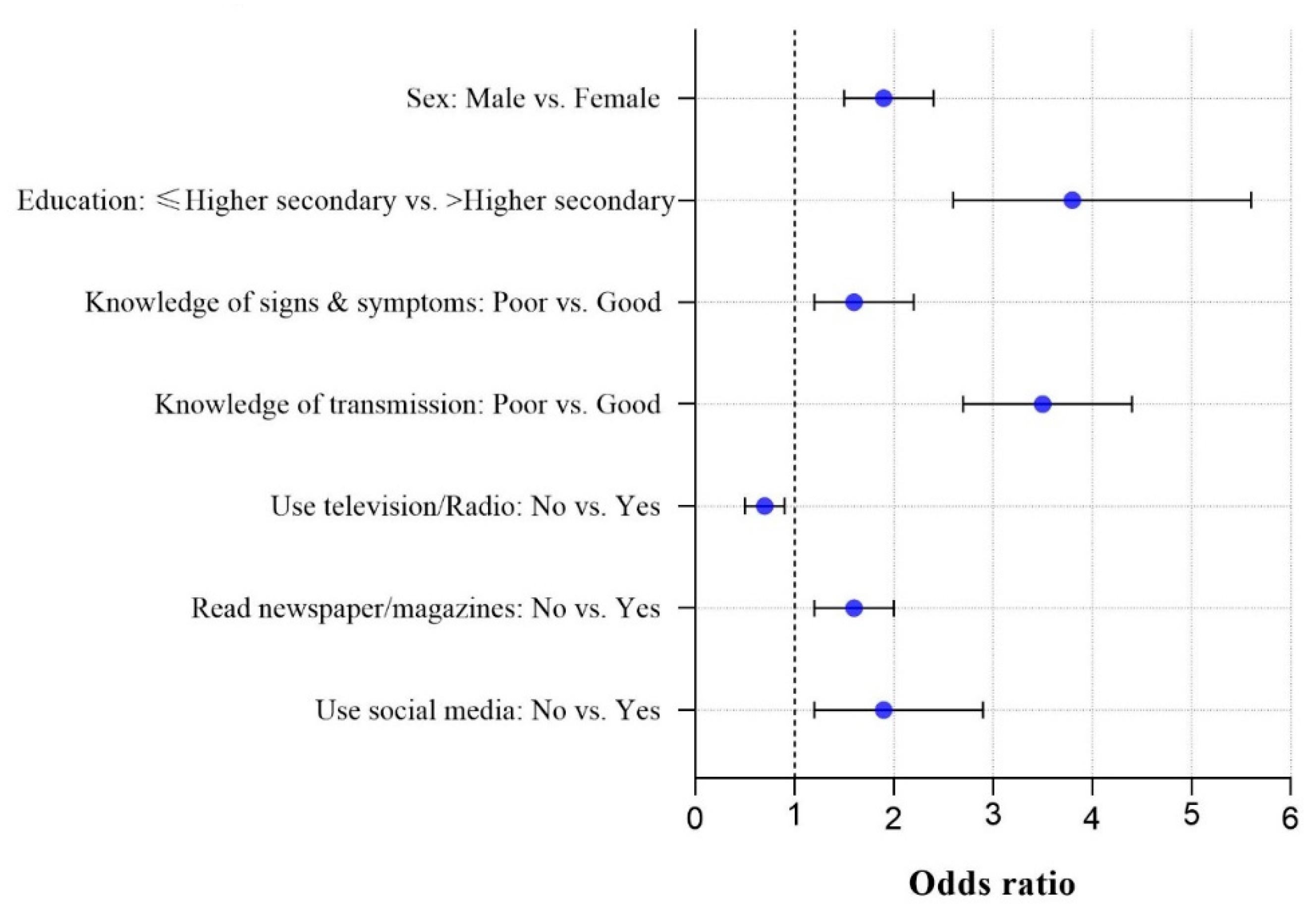
3.6. Analysis of Demographic Factors, Knowledge, and Attitudes Associated with Preventive Practices against COVID-19
4. Discussion
5. Study Limitations
6. Conclusions and Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745. [Google Scholar] [CrossRef] [PubMed]
- Ruan, S. Likelihood of survival of coronavirus disease 2019. Lancet Infect. Dis. 2020, 20, 630–631. [Google Scholar] [CrossRef]
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int. J. Epidemiol. 2020, 49, 717–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, P.; Wang, X. COVID-19: A new challenge for human beings. Cell. Mol. Immunol. 2020, 17, 555–557. [Google Scholar] [CrossRef] [Green Version]
- Mahase, E. Coronavirus: Covid-19 Has Killed More People than SARS and MERS Combined, Despite Lower Case Fatality Rate. BMJ 2020. [Google Scholar] [CrossRef] [Green Version]
- Al-Omari, A.; Rabaan, A.A.; Salih, S.; Al-Tawfiq, J.A.; Memish, Z.A. MERS coronavirus outbreak: Implications for emerging viral infections. Diagn. Microbiol. Infect. Dis. 2019, 93, 265–285. [Google Scholar] [CrossRef]
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 9, e238–e244. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 9 November 2020).
- Bhutta, Z.A.; Basnyat, B.; Saha, S.; Laxminarayan, R. Covid-19 Risks and Response in South Asia. BMJ 2020. [Google Scholar] [CrossRef] [Green Version]
- Vince, G. The world’s largest refugee camp prepares for covid-19. BMJ 2020. [Google Scholar] [CrossRef] [Green Version]
- IEDCR. COVID-19. Available online: https://iedcr.gov.bd/covid-19/covid-19-situation-updates (accessed on 9 November 2020).
- Shrestha, N.; Shad, M.Y.; Ulvi, O.; Khan, M.H.; Karamehic-Muratovic, A.; Nguyen, U.-S.D.; Baghbanzadeh, M.; Wardrup, R.; Aghamohammadi, N.; Cervantes, D. The impact of COVID-19 on globalization. One Health 2020. [Google Scholar] [CrossRef]
- Hossain, M.A.; Jahid, M.I.K.; Hossain, K.M.A.; Walton, L.M.; Uddin, Z.; Haque, M.O.; Kabir, M.F.; Arafat, S.Y.; Sakel, M.; Faruqui, R. Knowledge, attitudes, and fear of COVID-19 during the Rapid Rise Period in Bangladesh. PLoS ONE 2020, 15, e0239646. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, M.S.; Karamehic-Muratovic, A.; Baghbanzadeh, M.; Amrin, M.; Zafar, S.; Rahman, N.N.; Shirina, S.U.; Haque, U. Climate change and dengue fever knowledge, attitudes and practices in Bangladesh: A social media–based cross-sectional survey. Trans. R. Soc. Trop. Med. Hyg. 2020. [CrossRef]
- Watkins, J. Preventing a Covid-19 Pandemic. BMJ 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, B.R.; Villegas Botero, A.; Grijalva, M.J. Knowledge, attitudes, and practices towards COVID-19 among Colombians during the outbreak: An online cross-sectional survey. J. Commun. Healthc. 2020. [Google Scholar] [CrossRef]
- CDC. Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/faq.html?fbclid=IwAR2JI-KU-CoGsuDRieR03ylVLebWmwPa9RDCVo2oG-5ssyeM9-8pBLZIRNM (accessed on 9 March 2020).
- Ministry of Health and Family Welfare, Government of the People’s Republic of Bangladesh. Information of COVID-19. Available online: http://www.mohfw.gov.bd/ (accessed on 8 March 2020).
- WHO. COVID-19. Available online: http://www.emro.who.int/health-topics/corona-virus/questions-and-answers.html?fbclid=IwAR2NdMuuV57Ytr3vblTTwuCK0BdXenzfEDoti8LWYdeOT3rZqY6oiLhKtlE (accessed on 9 March 2020).
- Raosoft, I. Raosoft Sample Size Calculator. Available online: http://www.raosoft.com/samplesize.html (accessed on 5 March 2020).
- Hsieh, F.; Liu, A.A. Adequacy of sample size in health studies. Stanley Lemeshow, David W. Hosmer Jr., Janelle Klar and Stephen K. Lwanga published on behalf of WHO by Wiley, Chichester, 1990. No. of pages: Xii+ 233. Price:£ D17. 50. Stat. Med. 1990, 9, 1382. [Google Scholar] [CrossRef]
- Ferdous, M.Z.; Islam, M.S.; Sikder, M.T.; Mosaddek, A.S.M.; Zegarra-Valdivia, J.; Gozal, D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: An online-based cross-sectional study. PLoS ONE 2020, 15, e0239254. [Google Scholar] [CrossRef]
- Paul, A.; Sikdar, D.; Hossain, M.M.; Amin, M.R.; Deeba, F.; Mahanta, J.; Jabed, M.A.; Islam, M.M.; Noon, S.J.; Nath, T.K. Knowledge, attitudes, and practices toward the novel coronavirus among Bangladeshis: Implications for mitigation measures. PLoS ONE 2020, 15, e0238492. [Google Scholar] [CrossRef]
- Yue, S.; Zhang, J.; Cao, M.; Chen, B. Knowledge, Attitudes and Practices of COVID-19 Among Urban and Rural Residents in China: A Cross-sectional Study. J. Community Health 2020. [Google Scholar] [CrossRef]
- Alyousefi, T.A.; Abdul-Ghani, R.; Mahdy, M.A.; Al-Eryani, S.M.; Al-Mekhlafi, A.M.; Raja, Y.A.; Shah, S.A.; Beier, J.C. A household-based survey of knowledge, attitudes and practices towards dengue fever among local urban communities in Taiz Governorate, Yemen. BMC Infect. Dis. 2016, 16, 543. [Google Scholar] [CrossRef] [Green Version]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.-T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Yao, H.; Chen, J.-H.; Xu, Y.-F. Rethinking online mental health services in China during the COVID-19 epidemic. Asian J. Psychiatry 2020, 50, 102015. [Google Scholar] [CrossRef]
- Rahman, M.S.; Peeri, N.C.; Shrestha, N.; Zaki, R.; Haque, U.; Ab Hamid, S.H. Defending against the Novel Coronavirus (COVID-19) Outbreak: How Can the Internet of Things (IoT) help to save the World? Health Policy Technol. 2020, 9, 136–138. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Rural | Urban | |||||
|---|---|---|---|---|---|---|
| Variables | n | % (95% C.I.) | n | % (95% C.I.) | Total n (%) | p-Value |
| Total respondents | 911 | 59.9 | 609 | 40.1 | 1520 (100.0) | |
| Age group (years) | <0.01 | |||||
| <30 | 398 | 43.7 (40.5–46.9) | 327 | 53.7 (49.7–57.6) | 725 (47.7) | |
| 30–40 | 213 | 23.4 (20.7–26.2) | 206 | 33.8 (30.2–37.7) | 419 (27.6) | |
| >40 | 300 | 32.9 (29.9–36.0) | 76 | 12.5 (10.0–15.3) | 376 (24.7) | |
| Sex | <0.01 * | |||||
| Female | 304 | 33.4 (30.4–36.5) | 271 | 45.5 (40.6–48.5) | 575 (37.8) | |
| Male | 607 | 66.6 (63.5–69.6) | 338 | 55.5 (51.5–59.4) | 945 (62.1) | |
| Education | <0.01 * | |||||
| ≤ higher secondary | 309 | 33.9 (30.9–37.0) | 49 | 8.0 (6.1–10.4) | 358 (23.6) | |
| > higher secondary | 602 | 66.1 (63.0–69.1) | 560 | 92.0 (89.6–93.9) | 1162 (76.4) | |
| Marital status | <0.01 | |||||
| Unmarried | 595 | 65.3 (62.2–68.4) | 534 | 87.7 (84.9–90.1) | 1129 (74.2) | |
| Married | 311 | 34.1 (31.1–37.3) | 75 | 12.3 (9.9–15.1) | 386 (25.3) | |
| Divorced/Separated | 5 | 0.5 (0.2–1.2) | N/A | N/A | 5 (0.3) | |
| Monthly family income (BDT) | <0.01 | |||||
| <10,000 | 288 | 31.6 (28.7–34.7) | 52 | 8.5 (6.5–11.0) | 340 (22.3) | |
| 10,000–20,000 | 247 | 27.1 (24.3–30.1) | 104 | 17.1 (14.2–20.2) | 351 (23.0) | |
| 20,000–30,000 | 196 | 21.5 (18.9–24.3) | 146 | 24.0 (20.7–27.5) | 342 (22.5) | |
| >30,000 | 180 | 19.8 (17.3–22.4) | 307 | 50.4 (46.4–54.4) | 487 (32.0) | |
| COVID-19 is a global pandemic | 0.215 * | |||||
| No | 13 | 1.4 (0.8–2.4) | 4 | 0.7 (0.2–1.6) | 17 (1.1) | |
| Yes | 898 | 98.6 (97.6–99.2) | 605 | 99.3 (98.4–99.8) | 1503 (98.8) | |
| Use internet to learn about COVID-19 | <0.01 * | |||||
| No | 136 | 14.9 (12.7–17.4) | 28 | 4.6 (3.1–6.5) | 164 (10.7) | |
| Yes | 775 | 85.1 (82.6–87.3) | 581 | 95.4 (93.5–96.5) | 1356 (89.2) |
| Knowledge Items | Rural | Urban | ||||
|---|---|---|---|---|---|---|
| n | % (95% C.I) | n | % (95% C.I.) | Total n (%) | p-Value | |
| Total respondents | 911 | 59.9 | 609 | 40.1 | 1520 (100.0) | |
| Transmission modes | ||||||
| k1. Contact with respiratory droplets | 483 | 53.0 (49.8–56.2) | 405 | 66.5 (62.7–70.2) | 888 (58.4) | <0.01 * |
| k2. Touching and shaking hands with an infected person | 781 | 85.7 (83.3–87.9) | 565 | 92.8 (90.5–94.6) | 1346 (88.5) | <0.01 * |
| k3. The use of objects used by an infected person | 672 | 73.8 (70.8–76.5) | 501 | 82.3 (79.1–85.1) | 1173 (77.1) | <0.01 * |
| k4. Sexual route | 281 | 30.8 (27.9–33.9) | 201 | 33.0 (29.4–36.8) | 482 (31.7) | 0.399 * |
| k5. Person-to-person | 704 | 77.3 (74.5–79.9) | 479 | 78.7 (75.3–81.8) | 1183 (77.8) | 0.571 * |
| k6. Close contact | 632 | 69.4 (66.3–72.3) | 465 | 76.4 (71.9–79.6) | 1097 (72.1) | <0.01 * |
| Signs and symptoms | ||||||
| k7. Fever | 875 | 96.0 (94.9–97.2) | 587 | 96.4 (94.7–97.7) | 1462 (96.0) | 0.786 * |
| k8. Tiredness | 459 | 50.4 (47.1–53.1) | 339 | 55.7 (51.7–59.6) | 798 (52.5) | <0.05 * |
| k9. Dry cough | 780 | 85.6 (83.2–87.8) | 551 | 90.5 (88.0–92.6) | 1331 (87.5) | <0.01 * |
| k10. Shortness of breath/Breathing difficulties | 696 | 76.4 (73.6–79.1) | 544 | 89.3 (86.7–91.6) | 1240 (81.5) | <0.01 * |
| k11. Aches and pains | 433 | 47.5 (44.3–50.8) | 311 | 51.1 (47.1–55.0) | 744 (48.9) | 0.191 * |
| k12. Nasal congestion | 261 | 28.6 (25.8–31.7) | 223 | 36.6 (32.9–40.5) | 484 (31.8) | <0.01 * |
| k13. Running nose | 315 | 34.6 (31.5–37.7) | 216 | 35.5 (31.7–39.3) | 531 (35.0) | 0.742 * |
| k14. Sore throat | 348 | 38.2 (35.1–41.4) | 326 | 53.5 (49.6–57.5) | 674 (44.3) | <0.01 * |
| k15. Diarrhea | 447 | 49.1 (47.7–54.2) | 335 | 55.0 (51.0–58.9) | 782 (51.4) | <0.05 * |
| Treatments/prevention | ||||||
| k16. The incubation period (2 weeks) | 786 | 86.3 (83.9–88.4) | 561 | 92.1 (89.8–94.1) | 1347 (88.6) | <0.01 * |
| k17. COVID-19 vaccines, drugs, or treatments is available | 686 | 75.3 (72.4–78.0) | 477 | 78.3 (74.9–81.5) | 1163 (76.5) | 0.068 * |
| k18. Lock-down | 475 | 52.1 (48.9–55.4) | 415 | 68.1 (64.4–71.8) | 890 (58.5) | <0.01 * |
| k19. Self-isolation | 417 | 45.8 (42.6–49.0) | 355 | 58.3 (54.3–62.2) | 772 (50.7) | <0.01 * |
| k20. Home quarantine | 770 | 84.5 (82.1–86.8) | 505 | 82.9 (79.8–85.8) | 1275 (83.8) | 0.434 * |
| Summarized knowledge about COVID-19 | <0.01 * | |||||
| Good | 226 | 24.8 (22.1–27.7) | 218 | 35.8 (32.1–39.7) | 444 (29.2) | |
| Poor | 685 | 75.2 (72.3–77.9) | 391 | 64.2 (60.3–67.9) | 1076 (70.8) |
| Attitude Items | Rural | Urban | ||||
|---|---|---|---|---|---|---|
| n | % (95% C.I) | n | % (95% C.I.) | Total n (%) | p-Value | |
| Total respondents | 911 | 59.9 | 609 | 40.1 | 1520 (100.0) | |
| A1. The government should lock-down the travel areas to avoid the spread of COVID-19 | <0.01 | |||||
| Strongly agree | 639 | 70.1 (67.1–73.0) | 491 | 80.6 (77.3–83.6) | 1130 (74.3) | |
| Agree | 220 | 24.1 (21.5–27.0) | 97 | 15.9 (13.2–19.0) | 317 (20.8) | |
| Neutral | 30 | 3.3 (2.3–4.6) | 10 | 1.6 (0.8–2.9) | 40 (2.6) | |
| Disagree | 19 | 2.1 (1.3–3.2) | 10 | 1.6 (0.8–2.9) | 29 (1.9) | |
| Strongly disagree | 3 | 0.3 (0.1–0.9) | 1 | 0.2 (0.0–0.8) | 4 (0.2) | |
| A2. Home quarantine can reduce COVID-19 outbreaks | <0.05 | |||||
| Strongly agree | 449 | 49.3 (46.0–52.5) | 342 | 56.2 (52.2–60.1) | 791 (52.0) | |
| Agree | 359 | 39.4 (36.3–42.6) | 216 | 35.5 (31.7–39.3) | 575 (37.8) | |
| Neutral | 48 | 5.3 (4.0–6.9) | 25 | 4.1 (2.7–5.9) | 73 (4.8) | |
| Disagree | 45 | 4.9 (3.7–6.5) | 15 | 2.5 (1.4–3.9) | 60 (3.9) | |
| Strongly disagree | 10 | 1.1 (0.6–1.9) | 11 | 1.8 (1.0–3.1) | 21 (1.3) | |
| A3. Isolation and treatment of infected people are effective ways to reduce the spread of the virus | <0.01 | |||||
| Strongly agree | 426 | 46.8 (43.5–50.0) | 355 | 58.3 (54.3–62.2) | 781 (51.3) | |
| Agree | 390 | 42.8 (39.6–46.0) | 206 | 33.8 (30.2–37.7) | 596 (39.2) | |
| Neutral | 64 | 7.0 (5.5–8.8) | 39 | 6.4 (4.7–8.6) | 103 (6.7) | |
| Disagree | 27 | 3.0 (2.0–4.2) | 7 | 1.1 (0.5–2.2) | 34 (2.2) | |
| Strongly disagree | 4 | 0.4 (0.1–1.0) | 2 | 0.3 (.1–1.0) | 6 (0.3) | |
| A4. Personal hygiene is important in controlling the spread of COVID-19 | <0.01 | |||||
| Strongly agree | 545 | 59.8 (56.6–63.0) | 455 | 74.7 (71.1–78.0) | 1000 (65.7) | |
| Agree | 315 | 34.6 (31.5–37.7) | 134 | 24.0 (18.9–25.4) | 449 (29.5) | |
| Neutral | 40 | 4.4 (3.2–5.9) | 12 | 2.0 (1.1–3.3) | 52 (3.4) | |
| Disagree | 9 | 1.0 (0.5–1.8) | 7 | 1.1 (0.5–2.2) | 16 (1.0) | |
| Strongly disagree | 2 | 0.2 (0.0–0.7) | 1 | 0.2 (0.0–0.8) | 3 (0.1) | |
| Summarized attitude towards COVID-19 | <0.01 * | |||||
| Good | 683 | 75.0 (72.1–77.7) | 517 | 84.9 (81.9–87.6) | 1200 (78.9) | |
| Poor | 228 | 25.0 (22.3–27.9) | 92 | 15.1 (12.4–18.1) | 320 (21.1) |
| Practice Items | Rural | Urban | ||||
|---|---|---|---|---|---|---|
| n | % (95% C.I) | n | % (95% C.I) | Total n (%) | p-Value | |
| Total respondents | 911 | 59.9 | 609 | 40.1 | 1520 (100.0) | |
| Preventive practices | ||||||
| P1. Practice self-isolation/Home quarantine | 777 | 85.3 (82.9–87.5) | 561 | 92.1 (89.8–94.1) | 1338 (88.0) | <0.01* |
| P2. Ensure sufficient food stock | 297 | 32.3 (29.6–35.7) | 211 | 34.4 (30.9–38.5) | 508 (33.4) | 0.437 * |
| P3. Practice respiratory hygiene | 507 | 55.7 (52.4–58.9) | 371 | 60.9 (57.0–64.7) | 878 (57.7) | <0.05 * |
| P4. Wash hand frequently using hand sanitizer | 712 | 78.2 (75.4–80.7) | 554 | 91.0 (88.5–93.1) | 1266 (83.2) | <0.01 * |
| P5. Use face mask | 697 | 76.5 (73.7–79.2) | 484 | 79.5 (76.1–82.5) | 1181 (77.6) | 0.187 * |
| P6. Avoid touching nose, mouth and eyes | 688 | 75.5 (72.7–78.2) | 501 | 82.3 (79.1–85.1) | 1189 (78.2) | <0.01 * |
| P7. Maintain social distance (min 1 m) | 440 | 48.3 (45.1–51.5) | 418 | 68.6 (64.9–72.2) | 858 (56.4) | <0.01 * |
| P8. Avoid practice of handshake | 446 | 49.0 (45.7–52.2) | 319 | 52.4 (48.4–56.3) | 765 (50.3) | 0.209 * |
| P9. Avoid practice of handshake hug | 678 | 74.4 (71.5–77.2) | 474 | 77.8 (74.4–81.0) | 1152 (75.7) | 0.143 * |
| P10. Avoid visit to any public places | 413 | 45.3 (42.1–48.6) | 230 | 37.8 (34.0–41.7) | 643 (42.3) | <0.01 * |
| P11. Avoid contact with infected person | 796 | 87.4 (85.1–88.9) | 555 | 91.1 (88.7–93.2) | 1351 (88.8) | <0.05 * |
| P12. Seek immediate medical attention/treatment regarding primary symptoms | 556 | 61.0 (57.8–64.2) | 426 | 70.0 (66.2–73.5) | 982 (64.6) | <0.01* |
| Summarized preventive practices against COVID-19 | <0.01 * | |||||
| Good | 200 | 22.0 (19.4–24.7) | 198 | 32.5 (28.9–36.3) | 398 (26.2) | |
| Poor | 711 | 78.0 (75.3–80.6) | 411 | 67.5 (63.7–71.1) | 1122 (73.8) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.S.; Karamehic-Muratovic, A.; Amrin, M.; Chowdhury, A.H.; Mondol, M.S.; Haque, U.; Ali, P. COVID-19 Epidemic in Bangladesh among Rural and Urban Residents: An Online Cross-Sectional Survey of Knowledge, Attitudes, and Practices. Epidemiologia 2021, 2, 1-13. https://doi.org/10.3390/epidemiologia2010001
Rahman MS, Karamehic-Muratovic A, Amrin M, Chowdhury AH, Mondol MS, Haque U, Ali P. COVID-19 Epidemic in Bangladesh among Rural and Urban Residents: An Online Cross-Sectional Survey of Knowledge, Attitudes, and Practices. Epidemiologia. 2021; 2(1):1-13. https://doi.org/10.3390/epidemiologia2010001
Chicago/Turabian StyleRahman, Md. Siddikur, Ajlina Karamehic-Muratovic, Miftahuzzannat Amrin, Arman Hossain Chowdhury, Md. Selim Mondol, Ubydul Haque, and Parveen Ali. 2021. "COVID-19 Epidemic in Bangladesh among Rural and Urban Residents: An Online Cross-Sectional Survey of Knowledge, Attitudes, and Practices" Epidemiologia 2, no. 1: 1-13. https://doi.org/10.3390/epidemiologia2010001