Recommendations for Lung Ultrasound in Internal Medicine

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
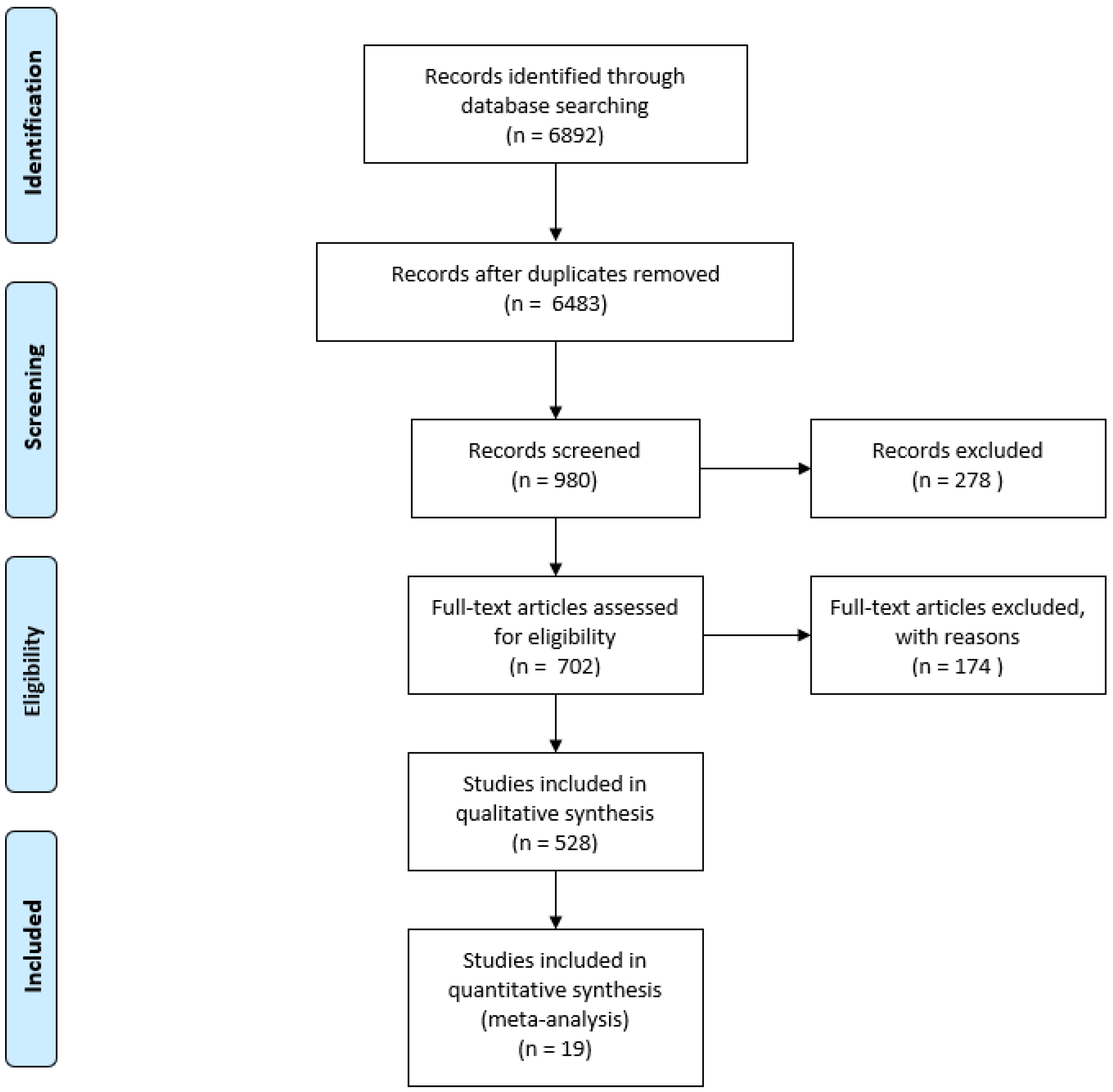
2. Materials and Methods
3. Recommendations
3.1. Pleural Cavity:
3.1.1. Pneumothorax
- The sonographic features of pneumothorax are as follows: absence of lung sliding, absence of vertical reverberation artifacts, absence of the lung pulse sign, and the presence of the lung point. (A1)
- The presence of lung sliding and/or vertical reverberation artifacts rising from the pleural line and/or the lung pulse excludes pneumothorax. (A1)
- In a patient with acute respiratory failure and with a significant suspicion of pneumothorax, it is not necessary to search for the lung point. (A1)
- Lung ultrasound is a superior diagnostic imaging technique to chest X-ray for patients with pneumothorax; however, lung ultrasound is less useful than chest X-ray for making therapeutic decisions, such as chest drainage. (A1)
- Convex and linear transducers are recommended for the diagnosis of pneumothorax. (A1)
- (a)
- The absence of the lung point with the simultaneous presence of pneumothorax occurs in cases of critical or mantle pneumothorax.
- (b)
- Prior pleurodesis affects the presence of lung sliding (the sign will be absent or limited) and of vertical reverberation artifacts (artifacts emerge due to pleural line abnormalities). The presence of vertical artifacts excludes pneumothorax in patients who underwent pleurodesis.
- (c)
- Loculated pneumothorax—a pocket of pleural air can be visualized; the air in the pleural cavity does not move with the change of the patient’s position.
- (d)
- The lung point is the border between the pocket of pleural air and the normal pleural cavity; this sign can be visualized in the B or M-mode.
- (e)
- The lung pulse is the pulse of the lung resulting from cardiac motion transferred to the lung; the lung pulse is best visualized in the M-mode and/or power/color Doppler options.
- (f)
- The recommended position during the examination is the supine position (except for patients with orthopnea).
3.1.2. Pleural Effusion
- Chest ultrasound is a more sensitive and more specific diagnostic imaging technique for pleural effusion than chest X-ray. (A1)
- The sensitivity of chest ultrasound, when determining the volume of pleural fluid, is similar to that of chest computed tomography. (B1)
- Chest ultrasound is a good method for chest imaging that allows for the finding of an optimal place to perform a puncture. (A1)
- Chest ultrasound allows for the minimization of post-puncture complications. (A1)
- Sonomorphology of pleural fluid in combination with clinical data may suggest its type. (C1)
- (a)
- If available, lung ultrasound should be performed for each patient with a clinical suspicion of pleural effusion and/or in the case when a classical X-ray result indicates the presence of pleural effusion, especially when thoracentesis is required.
- (b)
- Parietal pleural thickening (more than 2 mm) and/or detection of focal lesions within the parietal pleura may suggest a metastatic fluid type.
- (c)
- Ultrasound estimation of the volume of free fluid in the pleural cavity is possible using mathematical formulas. Below are some examples of formulas, dependent on body position:
- (d)
- Sitting position: V (ml) = LH (cm) × 90 or V (ml) = [LH (cm) + SH (cm)] × 70; measurement in posterior axillary line, LH—height of fluid layer, SH—average distance between diaphragm and lung base
- (e)
- Prone position: V (ml) = T (mm) × 20; measurement on exhalation; T—thickness of the fluid layer
3.2. LUNGS
3.2.1. Pulmonary Pathologies Associated with Interstitial Pulmonary Lesions
- The sonographic features of interstitial syndrome are as follows: the presence of lung sliding and ≥3 B-line artifacts in one intercostal space in a single longitudinal scan plane (in relation to the body axis). (A1)
- Lung ultrasound may be a superior diagnostic strategy to chest X-ray for detecting interstitial lesions. (A1)
- Interstitial syndrome may be caused by various conditions, including cardiogenic pulmonary edema, non-cardiogenic pulmonary edema, interstitial lung disease, infections and prior bronchoalveolar lavage. (A1)
- Convex/micro-convex or sector transducers, and, in some cases, a linear transducer, are recommended for the differential diagnosis of the causes of interstitial syndrome. (A1)
- (a)
- B-line artifacts are laser-like vertical reverberation artifacts arising from the pleural line, extending to the bottom of the screen, and moving along with the movements of the pleural line. The definition of a B-line artifact is based on the use of convex/micro-convex transducers.
- (b)
- The lung sliding sign may be limited or absent in the case of prior pleurodesis or the so-called stiff lung.
- (c)
- A linear transducer is recommended for the differential diagnosis of the causes of “interstitial syndrome”. This is particularly important in the case of bilateral asymmetric interstitial lesions, in the presence of the so-called spared areas, and also in the case of suspected respiratory tract infections, as well as in any clinically ambiguous cause of interstitial pulmonary lesions.
Cardiogenic Pulmonary Edema and Heart Failure
- The sonographic features of cardiogenic pulmonary edema are as follows: most frequently bilateral, gravitational and symmetrical interstitial syndrome, and/or alveolar-interstitial syndrome and/or the white lung sign. (A1)
- Lung ultrasound is a good diagnostic strategy for diagnosing cardiogenic pulmonary edema. (A1)
- The use of lung ultrasound in patients diagnosed with heart failure is an important monitoring method during periods of clinical stabilization and exacerbation. (A1)
- Lung ultrasound performed for patients diagnosed with heart failure allows for the identification of patients at high risk of hospitalization and mortality. (A1)
- In patients with heart failure, an increased number of B-lines is a predictor of serious cardiovascular events in the near future. (A1)
- The number of B-lines is a predictor of and correlates with the risk of adverse cardiovascular events, re-hospitalization and mortality for patients with heart failure. (A1)
- The number of B-lines correlates with an abnormal echocardiogram; hence the detection of B-lines is an indication for performing echocardiography, irrespective of the possible etiology of B-lines. (A1)
- When monitoring features of pulmonary edema in the context of therapeutic effectiveness, transducers of the same type should be used (convex–convex or sector–sector). (C1)
- B-line artifacts are a good biomarker that correlate with the level of hyperhydration in patients with heart failure. (B1)
- In cardiogenic pulmonary edema, the number of B-line artifacts correlates well with the severity of pulmonary edema, NYHA classification (New York Heart Association Classification) and pro-BNP level (pro B-type natriuretic peptide). (A1)
- An ultrasound image of the lungs of patients with heart failure is useful when deciding on the intensity of diuretic therapy. (A1)
- In a patient with dyspnea, the absence of B-line artifacts in lung ultrasound excludes the diagnosis of cardiogenic pulmonary edema, and indicates the necessity of searching for other causes of dyspnea. (B1)
- Lung ultrasound is a good and accurate method differentiating cardiogenic and pulmonary causes of dyspnea. (A1)
- Lung ultrasound is a superior technique to chest X-ray for imaging cardiogenic pulmonary edema, and is comparable to that of chest computed tomography. (A1)
- Lung ultrasound is complementary to echocardiography in a clinical assessment of clinically manifested and occult heart failure. (A1)
- (a)
- Interstitial syndrome, alveolar-interstitial syndrome and the white lung sign define successively occurring more advanced stages of interstitial lesions in the course of cardiogenic pulmonary edema. All three of these signs require that at least three B-line artifacts be found in one intercostal space in a single longitudinal scan plane (in relation to the body axis); however, the distance between individual B-line artifacts decreases with an increasing fluid volume in the interstitial space and in the alveoli.
- (b)
- The presence of free-flowing anechoic fluid in pleural cavities may result from heart failure.
- (c)
- The sum of B-lines correlates with the signs of heart failure and the level of natriuretic peptides. It is a predictor of serious cardiovascular events.
- (d)
- Several scales were used in the studies to assess the severity of pulmonary congestion. Examination, consisting of registering 28 scans of the anterolateral chest of a patient in a supine position and summing up the number of registered B-line artifacts, allows for the exclusion of congestion (B-line index <5), or for the revealing of mild (B-line index ≥5 and <15), moderate (B-line index ≥15 and <30) and severe (B-line index ≥30) congestion. This method, although applied in many studies, is, however, time-consuming and requires much experience.
- (e)
- For a quick assessment, the scheme of examining eight or six scans (four or three on each half of the chest, respectively) is suggested—the obtained data may be crucial for rapid diagnostic and therapeutic decisions, but they are qualitative rather than quantitative.
- (f)
- The use of the LuCUS (lung and cardiac ultrasound) protocol (four lung zones on each side of the chest, anterolateral scans, in combination with the assessment of the left ventricular ejection fraction and of the inferior vena cava) is characterized by a sensitivity of 83% and a specificity of 83% in diagnosing acute heart failure as the cause of dyspnea.
- (g)
- A positive correlation between the number of B-line artifacts, clinical signs (NYHA scores) and the level of natriuretic peptides was revealed in the studies. It was revealed that the reduction of the number of B-line artifacts in patients hospitalized due to acute heart failure is positively and linearly correlated with the change in NT-proBNP level (r = 0.44; p < 0.05), clinical signs (r = 0.87; p < 0.01) and radiologic factors (r = 0.62; p < 0.05) [65].
- (h)
- B-lines are defined by a normal pleural line, and are a typical hallmark of cardiogenic pulmonary edema after the exclusion of certain pathologies, including pneumonia or lung contusion, whereas comet-tail artifacts show an irregular pleural line representing a variety of parenchymal lung diseases.
Assessment and Monitoring of Dialysis Patients
- Lung ultrasound is useful for the assessment and monitoring of patients receiving hemodialysis. (C1)
- B-lines are a good biomarker for the assessment of the degree of pulmonary congestion, and correlate well with other referential methods. (B1)
- Lung ultrasound is a useful tool for establishing the setting of ultrafiltration volume in dialysis patients. (C1)
- The number of B-lines in patients receiving hemodialysis increases the risk of hospitalization due to heart failure and the risk of cardiovascular death. (C1)
- (a)
- Studies concerning dialysis patients most frequently follow the protocol of assessing 28 scans of the anterolateral chest, adapted from cardiologic examinations. The interpretation of the examination results is sometimes modified by resigning from the notion of “mild congestion”. In such cases, the detection of the sum of B-lines <15 is interpreted as the absence of congestion; terminology applying to other ranges remains unchanged.
- (b)
- Pulmonary congestion revealed in lung ultrasound in patients receiving hemodialysis is significantly, reversely correlated with the quality of life assessed according to the Kidney Disease Quality of Life Short Form (r = −0.22; p < 0.001). Pulmonary congestion is an independent factor decreasing the quality of life of these patients, including clinically asymptomatic patients.
- (c)
- Patients with ultrasonographic features of severe congestion, as compared to those with detected features of mild or moderate congestion, present a three-fold greater risk of a cardiovascular event, and a four-fold greater mortality risk (HR = 3.20, 95% CI = 1.75–5.88 for a cardiovascular event and HR = 4.20, 95% CI = 2.45–7.23 for mortality, respectively).
Interstitial Lung Disease Involving Pulmonary Fibrosis
- The sonographic features of interstitial lung disease involving pulmonary fibrosis are as follows: the lung sliding sign, the presence of ≥3 B-line artifacts in one intercostal space (a longitudinal scan plane in relation to the body axis) and pleural line abnormalities. (A1)
- The use of lung ultrasound may be a superior diagnostic strategy to chest X-ray for diagnosing interstitial lung disease involving pulmonary fibrosis. (A1)
- The use of lung ultrasound in the monitoring of interstitial lung disease involving pulmonary fibrosis may be helpful (C1)
- (a)
- Pleural line abnormalities found in patients with pulmonary fibrosis are described as irregular, coarse in appearance, fragmented or blurred.
- (b)
- The use of lung ultrasound in the diagnosis of interstitial pulmonary disease in the active phase is based on case reports, and refers to pulmonary vasculitis, sarcoidosis, hypersensitivity pneumonitis, diffuse alveolar hemorrhage secondary to systemic connective tissue diseases, pulmonary alveolar proteinosis, and interstitial pneumonia secondary to systemic connective tissue diseases.
3.2.2. Pulmonary Pathologies Associated with Consolidations
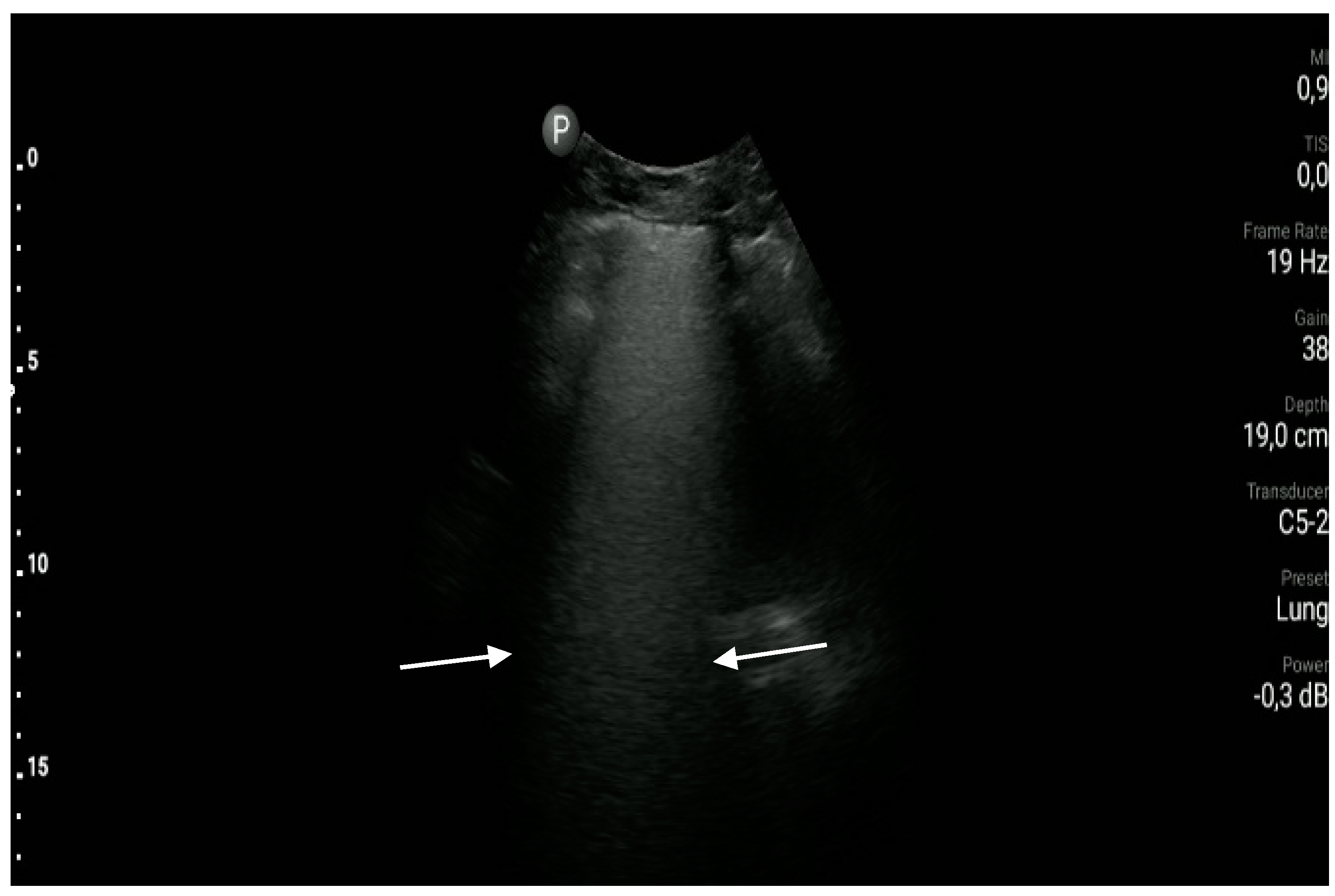
- The sonographic features of consolidations are as follows: a subpleural hypoechoic area with a liver-like structure. (A1)
- The use of lung ultrasound may be a superior diagnostic strategy to chest X-ray for confirming the presence of subpleural consolidations. (A1)
- Subpleural consolidations may have various underlying causes, most commonly pneumonia, atelectasis (compression- or resorption-related), pulmonary embolism, subpleural neoplastic lesions (primary or metastatic), and lung contusion. (A1)
- (a)
- Experts emphasize the coexistence of multiple morbidities within the respiratory system. The coexistence of more than one respiratory system disease, found in clinical practice, results in the overlapping of several abnormalities in the lung ultrasound scan. It should also be remembered that computed tomography performed according to a protocol suitable for an initial diagnosis is the reference examination in the assessment of pulmonary lesions.
Pneumonia
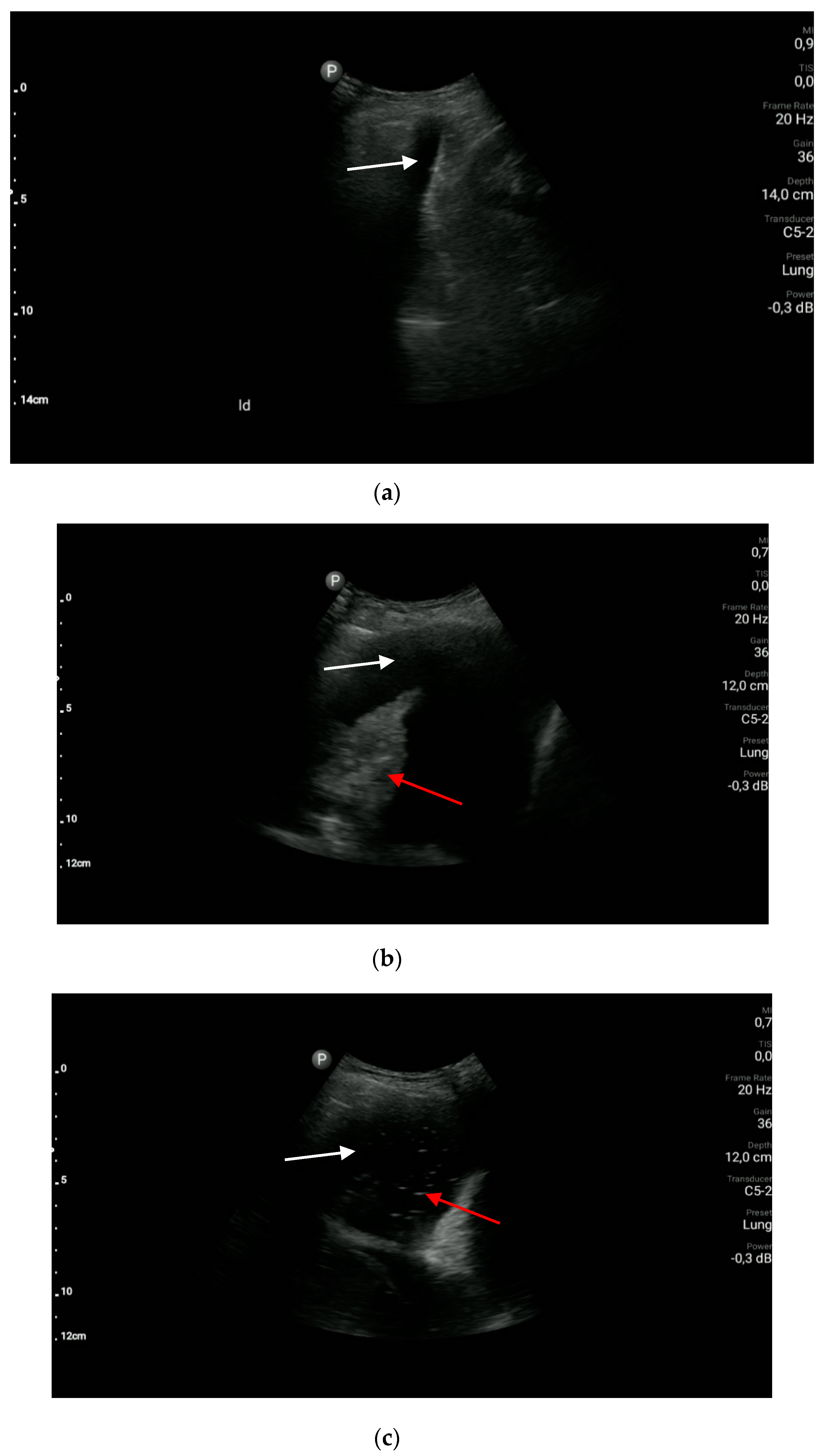
- The sonographic features of pneumonia are as follows: consolidation, irregular marginal contour, air bronchogram, the air trapping sign, comet-tail artifacts (B-lines), normal vascular pattern in CD and PD (color Doppler and power Doppler) options, and the presence of pleural effusion. (A1)
- The use of lung ultrasound may be a superior diagnostic strategy to chest X-ray for confirming the presence of pneumonia. (A1)
- When pneumonia is clinically suspected, the detection of typical inflammatory consolidations in lung ultrasound does not require further confirmation with chest X-ray. (A1)
- Lung ultrasound is more sensitive and more specific in the diagnosis of community-acquired pneumonia than chest X-ray, and is comparable to the effectiveness of chest computed tomography. (A1)
- Lung ultrasound is an accurate and quick diagnostic tool for differentiating the causes of acute dyspnea (including pneumonia, acute heart failure and exacerbation of chronic obstructive pulmonary disease (COPD)/asthma). (A1)
- (a)
- Inflammatory lesions are categorized as parenchymatous (consolidation with an irregular marginal contour, dynamic air bronchogram visible within the consolidation and/or the air trapping sign), vascular (normal flow pattern in CD and PD options) and pleural (pleural effusion). This description of lesions does not apply to bronchopneumonia.
- (b)
- Consolidation means an airless area of the lung.
- (c)
- An air bronchogram is the air visible in the bronchial tree within the consolidation.
- (d)
- A dynamic air bronchogram is visible on inspiration and disappears on expiration.
- (e)
- A normal vascular pattern is one that is consistent with the anatomical standard—it is visible with the use of CD and/or PD options.
- (f)
- Experts emphasize that inflammatory lesions caused by tuberculosis, systemic mycosis, pneumocystosis, viral infection and pneumonia of an atypical etiology may present a different sonomorphology than the one described above. It should also be remembered that typical inflammatory lesions may overlap with those caused by less common pathogens.
- (g)
- The diagnostic sensitivity of lung ultrasound for the diagnosis of pneumonia amounts to 87–95%, and specificity to 80–96%. The interpretation of the examination results must account for clinical data. The significance of lung ultrasound results for diagnostic and therapeutic procedures may be particularly important in the following patient groups: geriatric patients, chronically immobile bedridden patients, and patients with chest deformities.
Atelectasis
- The sonographic features of compression atelectasis are as follows: pleural effusion, consolidation of a homogeneous echogenicity and echostructure, static air bronchogram, the air trapping sign, and normal vascular pattern in CD and PD options. (A1)
- The sonographic features of resorption atelectasis are as follows: consolidation of a homogeneous echogenicity and echostructure, fluid bronchogram, static air bronchogram, normal vascular pattern in CD and PD options, and possible visualization of a pathological mass at the top of the consolidation. (A1)
- The use of lung ultrasound may be a superior diagnostic strategy to chest X-ray for confirming compression atelectasis. (A1)
- The use of lung ultrasound may be a superior diagnostic strategy to chest X-ray for confirming resorption atelectasis. (A1)
- (a)
- Blood flow in CD and PD options is normal only within the area of compression atelectasis, or within the consolidation area constituting resorption atelectasis and not being a pathological mass associated with cancer.
- (b)
- A static air bronchogram represents the presence of air in the bronchial tree and is visible during all respiration phases.
Pulmonary Embolism
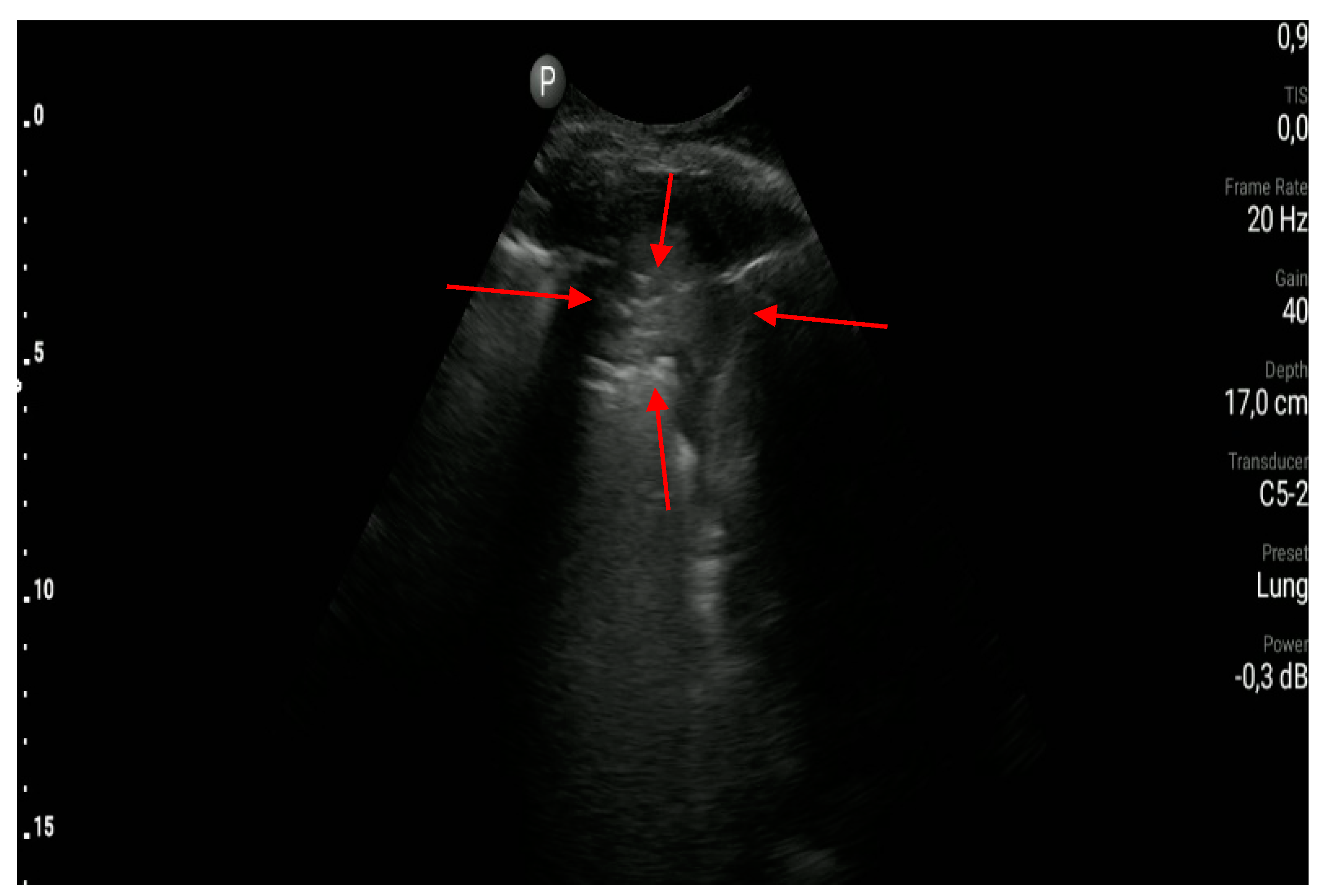
- The sonographic features of pulmonary embolism may be as follows: consolidation, mostly wedge-shaped or oval/rounded, centrally located echo, flow amputation in the CD option (the so-called vascular sign), local fluid immediately above the subpleural lesion, and local interstitial lesions. (A1)
- If pulmonary embolism is suspected, lung ultrasound may be a good diagnostic strategy to confirm the diagnosis. (A1)
- If pulmonary embolism is suspected (according to the Wells score), the combination of lung ultrasound, transthoracic echocardiography (ECHO) and compression ultrasound (CUS) venous imaging significantly increases the sensitivity and specificity of pulmonary embolism diagnosis, and consequently allows for limiting the number of angio-CT exams performed. (A1)
- Pulmonary embolism is diagnosed if ≥ 2 typical abnormalities are found in lung ultrasound. (B1)
- The diagnosis of pulmonary embolism is likely if one abnormality typical of pulmonary embolism is detected in lung ultrasound. (C1)
- The absence of abnormalities typical of pulmonary embolism does not rule out its diagnosis. (A1)
- (a)
- In the case of patients with acute respiratory failure and a high risk of death, it is recommended to follow the BLUE protocol and criteria for the diagnosis of pulmonary embolism designed therein as a potential cause of the patient’s acute status.
- (b)
- Lung ultrasound may be an alternative technique for the diagnosis of pulmonary embolism when angio-CT cannot be performed or is contraindicated, e.g., in pregnant women, patients with acute kidney failure, and patients allergic to contrast agents.
- (c)
- The use of lung ultrasound in the diagnosis of pulmonary embolism may increase the sensitivity and specificity of commonly applied assessment scores for the clinical risk of embolism (e.g., the Wells score); it does not, however, apply to the assessment of the patient’s prognosis.
- (d)
- Two thirds of the lung infarctions are located dorsally in the lower lobes of the lungs. Therefore, it is very important to examine the patients from the dorsal in the right- and left-side position.
- (e)
- In about 50% of the cases there are small pleural effusions, focally above the lesions in the pleural cavity.
Subpleural Malignant Lesions
- The sonographic features of subpleural malignant lesions are as follows: infiltration of adjacent structures, diverse sonomorphology of the consolidation, chaotic vascular pattern in CD and PD options, and concomitant resorption atelectasis and/or fluid. (A1)
- The use of lung ultrasound is a good diagnostic strategy during invasive procedures (transthoracic biopsy) in the diagnosis of subpleural lesions suspected of being malignant. (A1)
- Lung ultrasound is a good imaging technique that allows for the localization of peripheral pulmonary tumors adjacent to the chest wall, or tumors within the consolidation area below the fluid in the pleural cavity. (B1)
- (a)
- Subpleural malignant lesions may be accompanied by accessory vascularization originating from intercostal vessels that can be visualized in CD and PD options.
- (b)
- The use of ultrasound guidance during a biopsy is applicable for both subpleural lesions and biopsies through the acoustic window formed by fluid or atelectasis.
3.3. Diaphragm
3.4. Other Indications
- The use of lung ultrasound may be a good diagnostic strategy for determining the causes of dyspnea. (A1)
- The use of lung ultrasound may be a good diagnostic strategy for the differential diagnosis of pleuritic chest pain. (A1)
- The use of lung ultrasound may be a good screening strategy for the differential diagnosis of acute cough (A1)
- A lung ultrasound examination performed by a trained clinician is at a comparable level to a lung ultrasound examination performed by a radiologist. (A1)
4. Experts’ Additional Suggestions
- Bedside examination is recommended for a clinically unstable patient with dyspnea.
- The lung ultrasound scanning technique depends on the patient’s clinical status and should cover the largest possible area of the lungs.
- Lung ultrasound performed by a trained clinician for a patient with respiratory failure is a good and safe diagnostic constituent for the differential diagnosis of pulmonary diseases.
- Basic training in the theoretical aspects and practical use of lung ultrasound is recommended for physicians during their specialty training programs, including internal medicine, cardiology, pulmonology and nephrology.
- The recommended basic course for clinicians during their specialty training programs should cover the diagnosis of pleural effusion, pneumothorax, cardiogenic and non-cardiogenic pulmonary edema, interstitial lung disease involving fibrosis, pneumonia, atelectasis, pulmonary embolism, subpleural malignant lesions, rib fracture as well as assistance during invasive diagnostic procedures and therapies.
- It is recommended to incorporate basic lung ultrasound training into the curriculum of students at faculties of medicine in medical universities.
5. Practical Aspects of Lung Ultrasound Examination
- When examining the patient, the protocol appropriate to the clinical situation should be selected each time;
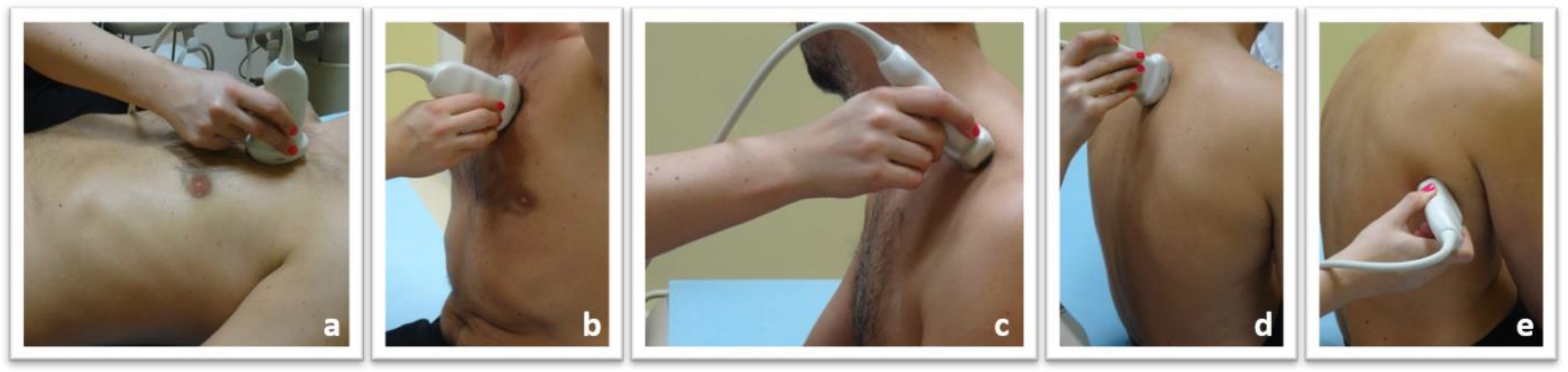
- If the patient’s condition allows it, assess the anterior, lateral and posterior surfaces of the chest in the vertical and supine positions of the patient, using a convex probe and then a linear probe (Figure 2);
- When analyzing the obtained ultrasound image, first of all, answer the following questions:
- (a)
- Was the pleural line visible on the entire lung fields during the examination?
- (b)
- is lung sliding present?
- (c)
- is the pleural line correct?
- (d)
- are there any pathological artifacts?
- (e)
- if pathological artifacts are found, their location should be determined (according to the anatomical topography of the chest)
- (f)
- if any subpleural consolidations are found, provide their location, dimensions, shape, echogenicity, and the degree of separation from the environment. If technically possible, an assessment of the vascularization (doppler) is also advisable.
- (g)
- are the pleural cavities free of fluid?
- (h)
- if fluid is found in the pleural cavity, its echogenicity should be determined and its volume should be estimated
- In everyday clinical practice, the results of the ultrasound examination of the lungs should be interpreted similarly to the results of other additional examinations, i.e., in relation to the overall clinical picture.
6. Conclusions
Funding
Conflicts of Interest
References
- Buda, N.; Kosiak, W.; Radzikowska, E.; Olszewski, R.; Jassem, E.; Grabczak, E.M.; Pomiecko, A.; Piotrkowski, J.; Piskunowicz, M.; Sołtysiak, M.; et al. Polish recommendations for lung ultrasound in internal medicine (POLLUS-IM). J. Ultrason. 2018, 18, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; the QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Reitsma, J.B.; Rutjes, A.W.; Whiting, P.; Vlassov, V.V.; Leeflang, M.M.; Deeks, J.J. Assessing methodological quality. In Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy Version 1.0.0; Deeks, J.J., Bossuyt, P.M., Gatsonis, C., Eds.; The Cochrane Collaboration: London, UK, 2009. [Google Scholar]
- Willis, B.H.; Quigley, M. Uptake of newer methodological developments and the deployment of meta-analysis in diagnostic test research: A systematic review. BMC Med. Res. Methodol. 2011, 11, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenstein, D.A.; Mezière, G.; Lascols, N.; Biderman, P.; Courret, J.P.; Gepner, A.; Goldstein, I.; Tenoudji-Cohen, M. Ultrasound diagnosis of occult pneumothorax. Crit. Care Med. 2005, 33, 1231–1238. [Google Scholar] [CrossRef] [Green Version]
- Blaivas, M.; Lyon, M.; Duggal, S. A prospective comparison of supine chest radiography and bedside ultrasound for the diagnosis of traumatic pneumothorax. Acad. Emerg. Med. 2005, 12, 844–849. [Google Scholar] [CrossRef] [Green Version]
- Sartori, S.; Tombesi, P.; Trevisani, L.; Nielsen, I.; Tassinari, D.; Abbasciano, V. Accuracy of transthoracic sonography in detection of pneumothorax after sonographically guided lung biopsy: Prospective comparison with chest radiography. AJR Am. J. Roentgenol. 2007, 188, 37–41. [Google Scholar] [CrossRef]
- Shostak, E.; Brylka, D.; Krepp, J.; Pua, B.; Sanders, A. Bedside sonography for detection of postprocedure pneumothorax. J. Ultrasound Med. 2013, 32, 1003–1009. [Google Scholar] [CrossRef] [Green Version]
- Soldati, G.; Testa, A.; Sher, S.; Pignataro, G.; La Sala, M.; Silveri, N.G. Occult traumatic pneumothorax: Diagnostic accuracy of lung ultrasonography in the emergency department. Chest 2008, 133, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Volpicelli, G.; Boero, E.; Sverzellati, N.; Cardinale, L.; Busso, M.; Boccuzzi, F.; Tullio, M.; Lamorte, A.; Stefanone, V.; Ferrari, G.; et al. Semi-quantification of pneumothorax volume by lung ultrasound. Intensive Care Med. 2014, 40, 1460–1467. [Google Scholar] [CrossRef]
- Viglietta, L.; Inchingolo, R.; Pavano, C.; Tomassetti, S.; Piciucchi, S.; Smargiassi, A.; Ravaglia, C.; Dubini, A.; Gurioli, C.; Gurioli, C.; et al. Ultrasonography for the Diagnosis of Pneumothorax after Transbronchial Lung Cryobiopsy in Diffuse Parenchymal Lung Diseases. Respiration 2017, 94, 232–236. [Google Scholar] [CrossRef]
- Galbois, A.; Ait-Oufella, H.; Baudel, J.L.; Kofman, T.; Bottero, J.; Viennot, S.; Rabate, C.; Jabbouri, S.; Bouzeman, A.; Guidet, B.; et al. Pleural ultrasound compared with chest radiographic detection of pneumothorax resolution after drainage. Chest 2010, 138, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Patella, M.; Saporito, A.; Puligheddu, C.; Mongelli, F.; La Regina, D.; Pini, R.; Inderbitzi, R.; Cafarotti, S. Lung Ultrasound to Detect Residual Pneumothorax After Chest Drain Removal in Lung Resections. Ann. Thorac. Surg. 2018, 105, 1537–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sistrom, C.L.; Reiheld, C.T.; Gay, S.B.; Wallace, K.K. Detection and estimation of the volume of pneumothorax using real-time sonography: Efficacy determined by receiver operating characteristic analysis. AJR Am. J. Roentgenol. 1996, 166, 317–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, G.; Sandmann, W. Der akute arterielle Verschluss aus der Sicht des Chirurgen [Surgical aspects in arterial occlusion (author’s transl)]. Zentralbl. Chir. 1977, 102, 1097–1101. [Google Scholar]
- Matus, I.; Raja, H. Protocolized Thoracic Ultrasonography in Transbronchial Lung Cryobiopsies: A Potential Role as an Exclusion Study for Pneumothorax. J. Bronchol. Interv. Pulmonol. 2019, 26, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Sekine, K.; Funabiki, T.; Orita, T.; Shimizu, M.; Hayashida, K.; Kazamaki, T.; Suzuki, T.; Kishikawa, M.; Yamazaki, M.; et al. Diagnostic accuracy of oblique chest radiograph for occult pneumothorax: Comparison with ultrasonography. World J. Emerg. Surg. 2016, 11, 5. [Google Scholar] [CrossRef] [Green Version]
- Abdalla, W.; Elgendy, M.; Abdelaziz, A.A.; Ammar, M.A. Lung ultrasound versus chest radiography for the diagnosis of pneumothorax in critically ill patients: A prospective, single-blind study. Saudi J. Anaesth. 2016, 10, 265–269. [Google Scholar] [CrossRef]
- Karagöz, A.; Ünlüer, E.E.; Akçay, O.; Kadioğlu, E. Effectiveness of Bedside Lung Ultrasound for Clinical Follow-Up of Primary Spontaneous Pneumothorax Patients Treated With Tube Thoracostomy. Ultrasound Q. 2018, 34, 226–232. [Google Scholar] [CrossRef]
- Jalli, R.; Sefidbakht, S.; Jafari, S.H. Value of ultrasound in diagnosis of pneumothorax: A prospective study. Emerg. Radiol. 2013, 20, 131–134. [Google Scholar] [CrossRef]
- Alrajhi, K.; Woo, M.Y.; Vaillancourt, C. Test characteristics of ultrasonography for the detection of pneumothorax: A systematic review and meta-analysis. Chest 2012, 141, 703–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Agarwal, R.; Aggarwal, A.N.; Gupta, D.; Jindal, S.K. Role of ultrasonography in the diagnosis and management of pneumothorax following transbronchial lung biopsy. J. Bronchol. Interv. Pulmonol. 2015, 22, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.; Goldstein, I.; Mourgeon, E.; Cluzel, P.; Grenier, P.; Rouby, J.J. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004, 100, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Eibenberger, K.L.; Dock, W.I.; Ammann, M.E.; Dorffner, R.; Hörmann, M.F.; Grabenwöger, F. Quantification of pleural effusions: Sonography versus radiography. Radiology 1994, 191, 681–684. [Google Scholar] [CrossRef]
- Vignon, P.; Chastagner, C.; Berkane, V.; Chardac, E.; François, B.; Normand, S.; Bonnivard, M.; Clavel, M.; Pichon, N.; Preux, P.-M.; et al. Quantitative assessment of pleural effusion in critically ill patients by means of ultrasonography. Crit. Care Med. 2005, 33, 1757–1763. [Google Scholar] [CrossRef]
- Kelbel, C.; Börner, N.; Schadmand, S.; Klose, K.J.; Weilemann, L.S.; Meyer, J.; Thelen, M. Diagnosis of pleural effusions and atelectases: Sonography and radiology compared. Rofo 1991, 154, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Teichgräber, U.K.; Hackbarth, J. Sonographic Bedside Quantification of Pleural Effusion Compared to Computed Tomography Volumetry in ICU Patients. Ultrasound Int. Open 2018, 4, E131–E135. [Google Scholar] [CrossRef] [Green Version]
- Kurian, J.; Levin, T.L.; Han, B.K.; Taragin, B.H.; Weinstein, S. Comparison of ultrasound and CT in the evaluation of pneumonia complicated by parapneumonic effusion in children. AJR Am. J. Roentgenol. 2009, 193, 1648–1654. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, D.; Hulot, J.S.; Rabiller, A.; Tostivint, I.; Mezière, G. Feasibility and safety of ultrasound-aided thoracentesis in mechanically ventilated patients. Intensive Care Med. 1999, 25, 955–958. [Google Scholar] [CrossRef]
- Perazzo, A.; Gatto, P.; Barlascini, C.; Ferrari-Bravo, M.; Nicolini, A. Can ultrasound guidance reduce the risk of pneumothorax following thoracentesis? J. Bras. Pneumol. 2014, 40, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Mayo, P.H.; Goltz, H.R.; Tafreshi, M.; Doelken, P. Safety of ultrasound-guided thoracentesis in patients receiving mechanical ventilation. Chest 2004, 125, 1059–1062. [Google Scholar] [CrossRef] [Green Version]
- Salamonsen, M.; Dobeli, K.; McGrath, D.; Readdy, C.; Ware, R.; Steinke, K.; Fielding, D. Physician-performed ultrasound can accurately screen for a vulnerable intercostal artery prior to chest drainage procedures. Respirology 2013, 18, 942–947. [Google Scholar] [CrossRef]
- Salamonsen, M.; Ellis, S.; Paul, E.; Steinke, K.; Fielding, D. Thoracic ultrasound demonstrates variable location of the intercostal artery. Respiration 2012, 83, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Diacon, A.H.; Brutsche, M.H.; Solèr, M. Accuracy of pleural puncture sites: A prospective comparison of clinical examination with ultrasound. Chest 2003, 123, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Prina, E.; Torres, A.; Carvalho, C.R. Lung ultrasound in the evaluation of pleural effusion. J. Bras. Pneumol. 2014, 40, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brogi, E.; Gargani, L.; Bignami, E.; Barbariol, F.; Marra, A.; Forfori, F.; Vetrugno, L. Thoracic ultrasound for pleural effusion in the intensive care unit: A narrative review from diagnosis to treatment. Crit. Care 2017, 21, 325. [Google Scholar] [CrossRef]
- Chen, H.J.; Tu, C.Y.; Ling, S.J.; Chen, W.; Chiu, K.L.; Hsia, T.C.; Shih, C.M.; Hsu, W.H. Sonographic appearances in transudative pleural effusions: Not always an anechoic pattern. Ultrasound Med. Biol. 2008, 34, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.C.; Luh, K.T.; Chang, D.B.; Wu, H.D.; Yu, C.J.; Kuo, S.H. Value of sonography in determining the nature of pleural effusion: Analysis of 320 cases. AJR Am. J. Roentgenol. 1992, 159, 29–33. [Google Scholar] [CrossRef]
- Yuan, A.; Chang, D.B.; Yu, C.J.; Kuo, S.H.; Luh, K.T.; Yang, P.C. Color Doppler sonography of benign and malignant pulmonary masses. AJR Am. J. Roentgenol. 1994. [Google Scholar] [CrossRef] [Green Version]
- Bandi, V.; Lunn, W.; Ernst, A.; Eberhardt, R.; Hoffmann, H.; Herth, F.J. Ultrasound vs. CT in detecting chest wall invasion by tumor: A prospective study. Chest 2008, 133, 881–886. [Google Scholar] [CrossRef]
- Mathis, G. Thoraxsonography—Part II: Peripheral pulmonary consolidation. Ultrasound Med. Biol. 1997, 23, 1141–1153. [Google Scholar] [CrossRef]
- Sperandeo, M.; Varriale, A.; Sperandeo, G.; Polverino, E.; Feragalli, B.; Piattelli, M.L.; Maggi, M.M.; Palmieri, V.O.; De Sio, I.; Villella, M.; et al. Assessment of ultrasound acoustic artifacts in patients with acute dyspnea: A multicenter study. Acta Radiol. 2012, 53, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.; Mézière, G.; Biderman, P.; Gepner, A.; Barré, O. The comet-tail artifact. An ultrasound sign of alveolar-interstitial syndrome. Am. J. Respir. Crit. Care Med. 1997, 156, 1640–1646. [Google Scholar] [CrossRef] [PubMed]
- Palazzuoli, A.; Ruocco, G.; Beltrami, M.; Nuti, R.; Cleland, J.G. Combined use of lung ultrasound, B-type natriuretic peptide, and echocardiography for outcome prediction in patients with acute HFrEF and HFpEF. Clin. Res. Cardiol. 2018, 107, 586–596. [Google Scholar] [CrossRef] [Green Version]
- Curbelo, J.; Rodriguez-Cortes, P.; Aguilera, M.; Gil-Martinez, P.; Martín, D.; Suarez Fernandez, C. Comparison between inferior vena cava ultrasound, lung ultrasound, bioelectric impedance analysis, and natriuretic peptides in chronic heart failure. Curr. Med. Res. Opin. 2019, 35, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Scali, M.C.; Cortigiani, L.; Simionuc, A.; Gregori, D.; Marzilli, M.; Picano, E. Exercise-induced B-lines identify worse functional and prognostic stage in heart failure patients with depressed left ventricular ejection fraction. Eur. J. Heart Fail. 2017, 19, 1468–1478. [Google Scholar] [CrossRef] [Green Version]
- Garibyan, V.N.; Amundson, S.A.; Shaw, D.J.; Phan, J.N.; Showalter, B.K.; Kimura, B.J. Lung Ultrasound Findings Detected During Inpatient Echocardiography Are Common and Associated With Short- and Long-term Mortality. J. Ultrasound Med. 2018, 37, 1641–1648. [Google Scholar] [CrossRef] [Green Version]
- Pellicori, P.; Shah, P.; Cuthbert, J.; Urbinati, A.; Zhang, J.; Kallvikbacka-Bennett, A.; Clark, A.L.; Cleland, J.G.F. Prevalence, pattern and clinical relevance of ultrasound indices of congestion in outpatients with heart failure. Eur. J. Heart Fail. 2019, 21, 904–916. [Google Scholar] [CrossRef]
- Dwyer, K.H.; Merz, A.A.; Lewis, E.F.; Claggett, B.L.; Crousillat, D.R.; Lau, E.S.; Silverman, M.B.; Peck, J.; Rivero, J.; Cheng, S.; et al. Pulmonary Congestion by Lung Ultrasound in Ambulatory Patients with Heart Failure with Reduced or Preserved Ejection Fraction and Hypertension. J. Card. Fail. 2018, 24, 219–226. [Google Scholar] [CrossRef]
- Kobalava, Z.D.; Safarova, A.F.; Soloveva, A.E.; Cabello, F.E.; Meray, I.A.; Shavarova, E.K.; Villevalde, S.V. Pulmonary congestion by lung ultrasound in decompensated heart failure: Associations, in-hospital changes, prognostic value. Kardiologiia 2019, 59, 5–14. [Google Scholar] [CrossRef]
- Miglioranza, M.H.; Picano, E.; Badano, L.P.; Sant’Anna, R.; Rover, M.; Zaffaroni, F.; Sicari, R.; Kalil, R.K.; Leiria, T.L.; Gargani, L. Pulmonary congestion evaluated by lung ultrasound predicts decompensation in heart failure outpatients. Int. J. Cardiol. 2017, 240, 271–278. [Google Scholar] [CrossRef] [Green Version]
- Ye, X.J.; Li, N.; Li, J.H.; Wu, W.J.; Li, A.L.; Li, X.L. B-lines by lung ultrasound predict heart failure in hospitalized patients with acute anterior wall STEMI. Echocardiography 2019, 36, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Li, Y.D.; Zhu, W.W.; Kong, L.Y.; Ye, X.G.; Cai, Q.Z.; Sun, L.L.; Lu, X.Z. A Simplified Ultrasound Comet Tail Grading Scoring to Assess Pulmonary Congestion in Patients with Heart Failure. BioMed Res. Int. 2018, 2018, 8474839. [Google Scholar] [CrossRef] [Green Version]
- Buessler, A.; Chouihed, T.; Duarte, K.; Bassand, A.; Huot-Marchand, M.; Gottwalles, Y.; Penine, A.; Andre, E.; Nace, L.; Jaeger, D.; et al. Accuracy of Several Lung Ultrasound Methods for the Diagnosis of Acute Heart Failure in the ED: A Multicenter Prospective Study. Chest 2020, 157, 99–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlino, M.V.; Paladino, F.; Sforza, A.; Serra, C.; Liccardi, F.; de Simone, G.; Mancusi, C. Assessment of left atrial size in addition to focused cardiopulmonary ultrasound improves diagnostic accuracy of acute heart failure in the Emergency Department. Echocardiography 2018, 35, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Platz, E.; Merz, A.; Silverman, M.; Lewis, E.; Groarke, J.D.; Waxman, A.; Systrom, D. Association between lung ultrasound findings and invasive exercise haemodynamics in patients with undifferentiated dyspnoea. ESC Heart Fail. 2019, 6, 202–207. [Google Scholar] [CrossRef]
- Hubert, A.; Girerd, N.; Le Breton, H.; Galli, E.; Latar, I.; Fournet, M.; Mabo, P.; Schnell, F.; Leclercq, C.; Donal, E. Diagnostic accuracy of lung ultrasound for identification of elevated left ventricular filling pressure. Int. J. Cardiol. 2019, 281, 62–68. [Google Scholar] [CrossRef]
- Han, P.J.; Tsai, B.T.; Martin, J.W.; Keen, W.D.; Waalen, J.; Kimura, B.J. Evidence Basis for a Point-of-Care Ultrasound Examination to Refine Referral for Outpatient Echocardiography. Am. J. Med. 2019, 132, 227–233. [Google Scholar] [CrossRef]
- Sikdar, S.; Panja, A.; Das, A.; Dey, A.; Guha, S. Lung ultrasound evaluation of diabetic patients with acute onset dyspnea and its relationship with established markers of heart failure. Indian Heart J. 2018, 70 (Suppl. 3), S399–S402. [Google Scholar] [CrossRef]
- Öhman, J.; Harjola, V.P.; Karjalainen, P.; Lassus, J. Rapid cardiothoracic ultrasound protocol for diagnosis of acute heart failure in the emergency department. Eur. J. Emerg. Med. 2019, 26, 112–117. [Google Scholar] [CrossRef]
- Yang, F.; Wang, Q.; Zhi, G.; Zhang, L.; Huang, D.; Shen, D.; Zhang, M. The application of lung ultrasound in acute decompensated heart failure in heart failure with preserved and reduced ejection fraction. Echocardiography 2017, 34, 1462–1469. [Google Scholar] [CrossRef]
- Pivetta, E.; Baldassa, F.; Masellis, S.; Bovaro, F.; Lupia, E.; Maule, M.M. Sources of Variability in the Detection of B-Lines, Using Lung Ultrasound. Ultrasound Med. Biol. 2018, 44, 1212–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öhman, J.; Harjola, V.P.; Karjalainen, P.; Lassus, J. Focused echocardiography and lung ultrasound protocol for guiding treatment in acute heart failure. ESC Heart Fail. 2018, 5, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Mozzini, C.; Di Dio Perna, M.; Pesce, G.; Garbin, U.; Fratta Pasini, A.M.; Ticinesi, A.; Nouvenne, A.; Meschi, T.; Casadei, A.; Soresi, M.; et al. Lung ultrasound in internal medicine efficiently drives the management of patients with heart failure and speeds up the discharge time. Intern. Emerg. Med. 2018, 13, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Martindale, J.L.; Secko, M.; Kilpatrick, J.F.; deSouza, I.S.; Paladino, L.; Aherne, A.; Mehta, N.; Conigiliaro, A.; Sinert, R. Serial Sonographic Assessment of Pulmonary Edema in Patients with Hypertensive Acute Heart Failure. J. Ultrasound Med. 2018, 37, 337–345. [Google Scholar] [CrossRef]
- Pardała, A.; Lupa, M.; Chudek, J.; Kolonko, A. Lung Ultrasound B-lines Occurrence in Relation to Left Ventricular Function and Hydration Status in Hemodialysis Patients. Medicina 2019, 55, 45. [Google Scholar] [CrossRef] [Green Version]
- Facchini, C.; Malfatto, G.; Giglio, A.; Facchini, M.; Parati, G.; Branzi, G. Lung ultrasound and transthoracic impedance for noninvasive evaluation of pulmonary congestion in heart failure. J. Cardiovasc. Med. 2016, 17, 510–517. [Google Scholar] [CrossRef]
- Trezzi, M.; Torzillo, D.; Ceriani, E.; Costantino, G.; Caruso, S.; Damavandi, P.T.; Genderini, A.; Cicardi, M.; Montano, N.; Cogliati, C. Lung ultrasonography for the assessment of rapid extravascular water variation: Evidence from hemodialysis patients. Intern. Emerg. Med. 2013, 8, 409–415. [Google Scholar] [CrossRef]
- Volpicelli, G.; Caramello, V.; Cardinale, L.; Mussa, A.; Bar, F.; Frascisco, M.F. Bedside ultrasound of the lung for the monitoring of acute decompensated heart failure. Am. J. Emerg. Med. 2008, 26, 585–591. [Google Scholar] [CrossRef]
- Saad, M.M.; Kamal, J.; Moussaly, E.; Karam, B.; Mansour, W.; Gobran, E.; Abbasi, S.H.; Mahgoub, A.; Singh, P.; Das, D.; et al. Relevance of B-Lines on Lung Ultrasound in Volume Overload and Pulmonary Congestion: Clinical Correlations and Outcomes in Patients on Hemodialysis. Cardiorenal Med. 2018, 8, 83–91. [Google Scholar] [CrossRef]
- Volpicelli, G.; Melniker, L.A.; Cardinale, L.; Lamorte, A.; Frascisco, M.F. Lung ultrasound in diagnosing and monitoring pulmonary interstitial fluid. Radiol. Med. 2013, 118, 196–205. [Google Scholar] [CrossRef]
- Rivas-Lasarte, M.; Álvarez-García, J.; Fernández-Martínez, J.; Maestro, A. Lopez-Lopez, L.; Sole-Gonzalez, E.; Pirla, M.J.; Mesado, N.; Mirabet, S.; Fluvia, P.; et al. Lung ultrasound-guided treatment in ambulatory patients with heart failure: A randomized controlled clinical trial (LUS-HF study). Eur. J. Heart Fail. 2019, 21, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Zanatta, M.; Benato, P.; De Battisti, S.; Pirozzi, C.; Ippolito, R.; Cianci, V. Pre-hospital lung ultrasound for cardiac heart failure and COPD: Is it worthwhile? Crit. Ultrasound J. 2018, 10, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajraktari, G.; Pugliese, N.R.; D’Agostino, A.; Rosa, G.M.; Ibrahimi, P.; Percuku, L.; Miccoli, M.; Galeotti, G.G.; Fabiani, J.; Pedrinelli, R.; et al. Echo- and B-Type Natriuretic Peptide-Guided Follow-Up versus Symptom-Guided Follow-Up: Comparison of the Outcome in Ambulatory Heart Failure Patients. Cardiol. Res. Pract. 2018, 2018, 3139861. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, M.; Gupta, M.; Vijan, V.; Vupputuri, A.; Chintamani, S.; Rajendran, B.; Thachathodiyal, R.; Chandrasekaran, R. Use of Lung Ultrasound for Diagnosing Acute Heart Failure in Emergency Department of Southern India. J. Clin. Diagn. Res. 2016, 10, TC05–TC08. [Google Scholar] [CrossRef] [PubMed]
- Coiro, S.; Porot, G.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Tritto, I.; Huttin, S.; Sadoul, N.; Donal, E.; Zannad, F.; et al. Prognostic value of pulmonary congestion assessed by lung ultrasound imaging during heart failure hospitalisation: A two-centre cohort study. Sci. Rep. 2016, 6, 39426. [Google Scholar] [CrossRef] [Green Version]
- Glöckner, E.; Christ, M.; Geier, F.; Otte, P.; Thiem, U.; Neubauer, S.; Kohfeldt, V.; Singler, K. Accuracy of Point-of-Care B-Line Lung Ultrasound in Comparison to NT-ProBNP for Screening Acute Heart Failure. Ultrasound Int. Open 2016, 2, E90–E92. [Google Scholar] [CrossRef] [Green Version]
- Miglioranza, M.H.; Gargani, L.; Sant’Anna, R.T.; Rover, M.M.; Martins, V.M.; Mantovani, A.; Weber, C.; Moraes, M.A.; Feldman, C.J.; Karam Kalil, R.A.; et al. Lung ultrasound for the evaluation of pulmonary congestion in outpatients: A comparison with clinical assessment, natriuretic peptides, and echocardiography. JACC Cardiovasc. Imaging 2013, 6, 1141–1151. [Google Scholar] [CrossRef] [Green Version]
- Zoccali, C.; Torino, C.; Tripepi, R.; Tripepi, G.; D’Arrigo, G.; Postorino, M. Pulmonary congestion predicts cardiac events and mortality in ESRD. J. Am. Soc. Nephrol. 2013, 24, 639–646. [Google Scholar] [CrossRef] [Green Version]
- Ang, S.H.; Andrus, P. Lung ultrasound in the management of acute decompensated heart failure. Curr. Cardiol. Rev. 2012, 8, 123–136. [Google Scholar] [CrossRef] [Green Version]
- Prosen, G.; Klemen, P.; Štrnad, M.; Grmec, S. Combination of lung ultrasound (a comet-tail sign) and N-terminal pro-brain natriuretic peptide in differentiating acute heart failure from chronic obstructive pulmonary disease and asthma as cause of acute dyspnea in prehospital emergency setting. Crit. Care 2011, 15, R114. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, L.; Priola, A.M.; Moretti, F.; Volpicelli, G. Effectiveness of chest radiography, lung ultrasound and thoracic computed tomography in the diagnosis of congestive heart failure. World J. Radiol. 2014, 6, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Staub, L.J.; Mazzali Biscaro, R.R.; Kaszubowski, E.; Maurici, R. Lung Ultrasound for the Emergency Diagnosis of Pneumonia, Acute Heart Failure, and Exacerbations of Chronic Obstructive Pulmonary Disease/Asthma in Adults: A Systematic Review and Meta-analysis. J. Emerg. Med. 2019, 56, 53–69. [Google Scholar] [CrossRef] [PubMed]
- McGivery, K.; Atkinson, P.; Lewis, D.; Taylor, L.; Harris, T.; Gadd, K.; Fraser, J.; Stoica, G. Emergency department ultrasound for the detection of B-lines in the early diagnosis of acute decompensated heart failure: A systematic review and meta-analysis. CJEM 2018, 20, 343–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laursen, C.B.; Hänselmann, A.; Posth, S.; Mikkelsen, S.; Videbæk, L.; Berg, H. Prehospital lung ultrasound for the diagnosis of cardiogenic pulmonary oedema: A pilot study. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 96. [Google Scholar] [CrossRef] [Green Version]
- Cibinel, G.A.; Casoli, G.; Elia, F.; Padoan, M.; Pivetta, E.; Lupia, E.; Goffi, A. Diagnostic accuracy and reproducibility of pleural and lung ultrasound in discriminating cardiogenic causes of acute dyspnea in the emergency department. Intern. Emerg. Med. 2012, 7, 65–70. [Google Scholar] [CrossRef]
- Koh, Y.; Chua, M.T.; Ho, W.H.; Lee, C.; Chan, G.W.H.; Sen Kuan, W. Assessment of dyspneic patients in the emergency department using point-of-care lung and cardiac ultrasonography-a prospective observational study. J. Thorac. Dis. 2018, 10, 6221–6229. [Google Scholar] [CrossRef]
- Wooten, W.M.; Shaffer, L.E.T.; Hamilton, L.A. Bedside Ultrasound Versus Chest Radiography for Detection of Pulmonary Edema: A Prospective Cohort Study. J. Ultrasound Med. 2019, 38, 967–973. [Google Scholar] [CrossRef]
- Farahmand, S.; Abdolhoseini, A.; Aliniagerdroudbari, E.; Babaniamansour, S.; Baratloo, A.; Bagheri-Hariri, S. Point-of-care ultrasound modalities in terms of diagnosing acute decompensated heart failure in emergency department; a diagnostic accuracy study. Intern. Emerg. Med. 2019. [Google Scholar] [CrossRef]
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; Platz, E.; DeSanto, K. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults With Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e190703. [Google Scholar] [CrossRef]
- Dehbozorgi, A.; Eslami Nejad, S.; Mousavi-Roknabadi, R.S.; Sharifi, M.; Tafakori, A.; Jalli, R. Lung and cardiac ultrasound (LuCUS) protocol in diagnosing acute heart failure in patients with acute dyspnea. Am. J. Emerg. Med. 2019, 37, 2055–2060. [Google Scholar] [CrossRef]
- Pivetta, E.; Goffi, A.; Nazerian, P.; Castagno, D.; Tozzetti, C.; Tizzani, P.; Tizzani, M.; Porrino, G.; Ferreri, E.; Buddo, V.; et al. Lung ultrasound integrated with clinical assessment for the diagnosis of acute decompensated heart failure in the emergency department: A randomized controlled trial. Eur. J. Heart Fail. 2019, 21, 754–766. [Google Scholar] [CrossRef] [Green Version]
- Lian, R.; Zhang, G.C.; Yan, S.T.; Sun, L.C.; Zhang, S.Q.; Zhang, G.Q. Role of Ultrasound Lung Comets in the Diagnosis of Acute Heart Failure in Emergency Department: A Systematic Review and Meta-analysis. Biomed. Environ. Sci. 2018, 31, 596–607. [Google Scholar] [CrossRef] [PubMed]
- Scharonow, M.; Weilbach, C. Prehospital point-of-care emergency ultrasound: A cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 596–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guttikonda, S.N.R.; Vadapalli, K. Approach to undifferentiated dyspnea in emergency department: Aids in rapid clinical decision-making. Int. J. Emerg. Med. 2018, 11, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrone, T.; Maggi, A.; Sgarlata, C.; Palumbo, I.; Mossolani, E.; Ferrari, S.; Melloul, A.; Mussinelli, R.; Boldrini, M.; Raimondi, A. Lung ultrasound in internal medicine: A bedside help to increase accuracy in the diagnosis of dyspnea. Eur. J. Intern. Med. 2017, 46, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Vizioli, L.; Forti, P.; Bartoli, E.; Giovagnoli, M.; Recinella, G.; Bernucci, D.; Masetti, M.; Martino, E.; Pirazzolli, G.L.; Zoli, M.; et al. Accuracy of Lung Ultrasound in Patients with Acute Dyspnea: The Influence of Age, Multimorbidity and Cognitive and Motor Impairment. Ultrasound Med. Biol. 2017, 43, 1846–1852. [Google Scholar] [CrossRef]
- Martindale, J.L.; Wakai, A.; Collins, S.P.; Levy, P.D.; Diercks, D.; Hiestand, B.C.; Fermann, G.J.; deSouza, I.; Sinert, R. Diagnosing Acute Heart Failure in the Emergency Department: A Systematic Review and Meta-analysis. Acad. Emerg. Med. 2016, 23, 223–242. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.P.; Zhang, Y.; Bian, H.; He, X.R.; Zhou, Y.J.; Wang, L.J.; Ding, N. Clinical application of rapid B-line score with lung ultrasonography in differentiating between pulmonary infection and pulmonary infection with acute left ventricular heart failure. Am. J. Emerg. Med. 2016, 34, 278–281. [Google Scholar] [CrossRef]
- Pivetta, E.; Goffi, A.; Lupia, E.; Tizzani, M.; Porrino, G.; Ferreri, E.; Volpicelli, G.; Balzaretti, P.; Banderali, A.; Iacobucci, A.; et al. Lung Ultrasound-Implemented Diagnosis of Acute Decompensated Heart Failure in the ED: A SIMEU Multicenter Study. Chest 2015, 148, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Al Deeb, M.; Barbic, S.; Featherstone, R.; Dankoff, J.; Barbic, D. Point-of-care ultrasonography for the diagnosis of acute cardiogenic pulmonary edema in patients presenting with acute dyspnea: A systematic review and meta-analysis. Acad. Emerg. Med. 2014, 21, 843–852. [Google Scholar] [CrossRef]
- Kajimoto, K.; Madeen, K.; Nakayama, T.; Tsudo, H.; Kuroda, T.; Abe, T. Rapid evaluation by lung-cardiac-inferior vena cava (LCI) integrated ultrasound for differentiating heart failure from pulmonary disease as the cause of acute dyspnea in the emergency setting. Cardiovasc. Ultrasound 2012, 10, 49. [Google Scholar] [CrossRef] [Green Version]
- Miger, K.C.; Fabricius-Bjerre, A.; Maschmann, C.P.; Wamberg, J.; Winkler Wille, M.M.; Abild-Nielsen, A.G.; Pedersen, L.; Henrik, H.; Schulz, L.; Nybing, J.D.; et al. Clinical Applicability of Lung Ultrasound Methods in the Emergency Department to Detect Pulmonary Congestion on Computed Tomography. Ultraschall Med. 2019. [Google Scholar] [CrossRef]
- Rinaldi, L.; Milione, S.; Fascione, M.C.; Pafundi, P.C.; Altruda, C.; Di Caterino, M.; Monaco, L.; Reginelli, A.; Perrotta, F.; Porta, G.; et al. Relevance of lung ultrasound in the diagnostic algorithm of respiratory diseases in a real-life setting: A multicentre prospective study. Respirology 2019. [Google Scholar] [CrossRef] [PubMed]
- Simonovic, D.; Coiro, S.; Carluccio, E.; Girerd, N.; Deljanin-Ilic, M.; Cattadori, G.; Ambrosio, G. Exercise elicits dynamic changes in extravascular lung water and haemodynamic congestion in heart failure patients with preserved ejection fraction. Eur. J. Heart Fail. 2018, 20, 1366–1369. [Google Scholar] [CrossRef] [PubMed]
- Öhman, J.; Harjola, V.P.; Karjalainen, P.; Lassus, J. Assessment of early treatment response by rapid cardiothoracic ultrasound in acute heart failure: Cardiac filling pressures, pulmonary congestion and mortality. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 311–320. [Google Scholar] [CrossRef]
- Russell, F.M.; Ehrman, R.R. A Modified Lung and Cardiac Ultrasound Protocol Saves Time and Rules in the Diagnosis of Acute Heart Failure. J. Emerg. Med. 2017, 52, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.P.; Shah, S.P.; Fils-Aime, R.; Desir, W.; Joasil, J.; Venesy, D.M.; Muruganandan, K.M. Focused cardiopulmonary ultrasound for assessment of dyspnea in a resource-limited setting. Crit. Ultrasound J. 2016, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Mantuani, D.; Frazee, B.W.; Fahimi, J.; Nagdev, A. Point-of-Care Multi-Organ Ultrasound Improves Diagnostic Accuracy in Adults Presenting to the Emergency Department with Acute Dyspnea. West. J. Emerg. Med. 2016, 17, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Platz, E.; Campbell, R.T.; Claggett, B.; Lewis, E.F.; Groarke, J.D.; Docherty, K.F.; Lee, M.M.Y.; Merz, A.A.; Silverman, M.; Swamy, V.; et al. Lung Ultrasound in Acute Heart Failure: Prevalence of Pulmonary Congestion and Short- and Long-Term Outcomes. JACC Heart Fail. 2019, 7, 849–858. [Google Scholar] [CrossRef]
- Platz, E.; Merz, A.A.; Jhund, P.S.; Vazir, A.; Campbell, R.; McMurray, J.J. Dynamic changes and prognostic value of pulmonary congestion by lung ultrasound in acute and chronic heart failure: A systematic review. Eur. J. Heart Fail. 2017, 19, 1154–1163. [Google Scholar] [CrossRef]
- Cogliati, C.; Casazza, G.; Ceriani, E.; Torzillo, D.; Furlotti, S.; Bossi, I.; Vago, T.; Costantino, G.; Montano, N. Lung ultrasound and short-term prognosis in heart failure patients. Int. J. Cardiol. 2016, 218, 104–108. [Google Scholar] [CrossRef]
- Tojo Villanueva Mdel, C.; Fernández López, M.; Canora Lebrato, J.; Satué Bartolomé, J.Á.; San Martín Prado, A.; Zapatero Gaviria, A. Utilidad pronóstica de la ecografía pulmonar en el seguimiento ambulatorio de pacientes con insuficiencia cardiaca [Use of lung ultrasound as a prognostic tool in outpatients with heart failure]. Med. Clin. 2016, 147, 13–15. [Google Scholar] [CrossRef]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; Carluccio, E.; Alunni, G.; Murrone, A.; Tritto, I.; Zannad, F.; Girerd, N. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur. J. Heart Fail. 2015, 17, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Pang, P.S.; Frassi, F.; Miglioranza, M.H.; Dini, F.L.; Landi, P.; Picano, E. Persistent pulmonary congestion before discharge predicts rehospitalization in heart failure: A lung ultrasound study. Cardiovasc. Ultrasound 2015, 13, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenstein, D. FALLS-protocol: Lung ultrasound in hemodynamic assessment of shock. Heart Lung Vessel. 2013, 5, 142–147. [Google Scholar] [PubMed]
- Torino, C.; Gargani, L.; Sicari, R.; Letachowicz, K.; Ekart, R.; Fliser, D.; Covic, A.; Siamopoulos, K.; Stravroulopoulos, A.; Massy, Z.A.; et al. The agreement between auscultation and lung ultrasound in hemodialysis patients: The LUST Study. Clin. J. Am. Soc. Nephrol. 2016, 11, 2005–2011. [Google Scholar] [CrossRef]
- Jambrik, Z.; Monti, S.; Coppola, V.; Agricola, E.; Mottola, G.; Miniati, M.; Picano, E. Usefulness of Ultrasound Lung Comets as a Nonradiologic Sign of Extravascular Lung Water. Am. J. Cardiol. 2004, 93, 1265–1270. [Google Scholar] [CrossRef]
- Frassi, F.; Gargani, L.; Tesorio, P.; Raciti, M.; Mottola, G.; Picano, E. Prognostic Value of Extravascular Lung Water Assessed With Ultrasound Lung Comets by Chest Sonography in Patient With Dyspnea and/or Chest Pain. J. Cardiac. Fail. 2007, 13, 830–835. [Google Scholar] [CrossRef]
- Mallamaci, F.; Benedetto, F.A.; Tripepi, R.; Rastelli, S.; Castellino, P.; Tripepi, G.; Picano, E.; Zoccali, C. Detection of pulmonary congestion by chest ultrasound in dialysis patients. JACC Cardiovasc. Imaging 2010, 3, 586–594. [Google Scholar] [CrossRef] [Green Version]
- Beaubien-Souligny, W.; Rhéaume, M.; Blondin, M.C.; El-Barnachawy, S.; Fortier, A.; Éthier, J.; Legault, L.; Denault, A.Y. A Simplified Approach to Extravascular Lung Water Assessment Using Point-of-Care Ultrasound in Patients with End-Stage Chronic Renal Failure Undergoing Hemodialysis. Blood Purif. 2018, 45, 79–87. [Google Scholar] [CrossRef]
- Noble, V.E.; Murray, A.F.; Capp, R.; Sylvia-Reardon, M.H.; Steele, D.J.R.; Liteplo, A. Ultrasound assessment for extravascular lung water in patients undergoing hemodialysis. Time course for resolution. Chest 2009, 135, 1433–1439. [Google Scholar] [CrossRef] [Green Version]
- Arun Thomas, E.T.; Mohandas, M.K.; George, J. Comparison between clinical judgment and integrated lung and inferior vena cava ultrasonography for dry weight estimation in hemodialysis patients. Hemodial. Int. 2019, 23, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Mottola, C.; Girerd, N.; Coiro, S.; Lamiral, Z.; Rossignol, P.; Frimat, L.; Girerd, S. Evaluation of Subclinical Fluid Overload Using Lung Ultrasound and Estimated Plasma Volume in the Postoperative Period Following Kidney Transplantation. Transplant. Proc. 2018, 50, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Donadio, C.; Bozzoli, L.; Colombini, E.; Pisanu, G.; Ricchiuti, G.; Picano, E.; Gargani, L. Effective and timely evaluation of pulmonary congestion: Qualitative comparison between lung ultrasound and thoracic bioelectrical impedance in maintenance hemodialysis patients. Medicine 2015, 94, e473. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.K.; Li, L.J.; Wang, X.H.; Wang, X.X.; Wang, Y.D.; Xu, Z.F. Role of Lung Ultrasound in Adjusting Ultrafiltration Volume in Hemodialysis Patients. Ultrasound Med. Biol. 2019, 45, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Loutradis, C.; Sarafidis, P.A.; Ekart, R.; Papadopoulos, C.; Sachpekidis, V.; Alexandrou, M.E.; Papadopoulou, D.; Efstratiadis, G.; Papagianni, A.; London, G.; et al. The effect of dry-weight reduction guided by lung ultrasound on ambulatory blood pressure in hemodialysis patients: A randomized controlled trial. Kidney Int. 2019, 95, 1505–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.L.; Liu, J.Y.; Zhou, C.J.; Wang, M.B.; Wang, H.Y.; Xu, Y. Risk factors and impacts on prognosis of ultrasound lung comets in patients undergoing hemodialysis. Zhonghua Yi Xue Za Zhi 2017, 97, 3796–3801. [Google Scholar] [CrossRef]
- Siriopol, D.; Voroneanu, L.; Hogas, S.; Apetrii, M.; Gramaticu, A.; Dumea, R.; Burlacu, A.; Sascau, R.; Kanbay, M.; Covic, A. Bioimpedance analysis versus lung ultrasonography for optimal risk prediction in hemodialysis patients. Int. J. Cardiovasc. Imaging 2016, 32, 263–270. [Google Scholar] [CrossRef]
- Panuccio, V.; Enia, G.; Tripepi, R.; Torino, C.; Garozzo, M.; Battaglia, G.G.; Marcantoni, C.; Infantone, L.; Giordano, G.; De Giorgi, M.L.; et al. Chest ultrasound and hidden lung congestion in peritoneal dialysis patients. Nephrol. Dial. Transplant. 2012, 27, 3601–3605. [Google Scholar] [CrossRef] [Green Version]
- Enia, G.; Torino, C.; Panuccio, V.; Tripepi, R.; Postorino, M.; Aliotta, R.; Bellantoni, M.; Tripepi, G.; Mallamaci, F.; Zoccali, C. Asymptomatic pulmonary congestion and physical functioning in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 1343–1348. [Google Scholar] [CrossRef] [Green Version]
- Buda, N.; Piskunowicz, M.; Porzezińska, M.; Kosiak, W.; Zdrojewski, Z. Lung Ultrasonography in the Evaluation of Interstitial Lung Disease in Systemic Connective Tissue Diseases: Criteria and Severity of Pulmonary Fibrosis—Analysis of 52 Patients. Ultraschall Med. 2016, 37, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Buda, N.; Masiak, A.; Zdrojewski, Z. Utility of lung ultrasound in ANCA-associated vasculitis with lung involvement. PLoS ONE 2019, 14, e0222189. [Google Scholar] [CrossRef] [PubMed]
- Papa, G.F.S.; Mondoni, M.; Volpicelli, G.; Carlucci, P.; Marco, F.D.; Parazzini, E.M.; Reali, F.; Pellegrino, G.M.; Fracasso, P.; Papa, S.S.; et al. Point-of-Care Lung Sonography: An Audit of 1150 Examinations. J. Ultrasound Med. 2017, 36, 1687–1692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathis, G. (Ed.) Lung consolidation. In Chest Sonography; Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 51–97. [Google Scholar]
- Nazerian, P.; Volpicelli, G.; Vanni, S.; Gigli, C.; Betti, L.; Bartolucci, M.; Zanobetti, M.; Ermini, F.R.; Iannello, C.; Grifoni, S. Accuracy of lung ultrasound for the diagnosis of consolidations when compared to chest computed tomography. Am. J. Emerg. Med. 2015, 33, 620–625. [Google Scholar] [CrossRef] [Green Version]
- Laursen, C.B.; Sloth, E.; Lambrechtsen, J.; Lassen, A.T.; Madsen, P.H.; Henriksen, D.P.; Davidsen, J.R.; Rasmussen, F. Focused sonography of the heart, lungs, and deep veins identifies missed life-threatening conditions in admitted patients with acute respiratory symptoms. Chest 2013, 144, 1868–1875. [Google Scholar] [CrossRef]
- Amatya, Y.; Rupp, J.; Russell, F.M.; Saunders, J.; Bales, B.; House, D.R. Diagnostic use of lung ultrasound compared to chest radiograph for suspected pneumonia in a resource-limited setting. Int. J. Emerg. Med. 2018, 11, 8. [Google Scholar] [CrossRef] [Green Version]
- Chavez, M.A.; Shams, N.; Ellington, L.E.; Naithani, N.; Gilman, R.H.; Steinhoff, M.C.; Santosham, M.; Black, R.E.; Price, C.; Gross, M.; et al. Lung ultrasound for the diagnosis of pneumonia in adults: A systematic review and meta-analysis. Respir. Res. 2014, 15, 50. [Google Scholar] [CrossRef] [Green Version]
- Cortellaro, F.; Colombo, S.; Coen, D.; Duca, P.G. Lung ultrasound is an accurate diagnostic tool for the diagnosis of pneumonia in the emergency department. Emerg. Med. J. 2012, 29, 19–23. [Google Scholar] [CrossRef] [Green Version]
- D’Amato, M.; Rea, G.; Carnevale, V.; Grimaldi, M.A.; Saponara, A.R.; Rosenthal, E.; Maggi, M.M.; Dimitri, L.; Sperandeo, M. Assessment of thoracic ultrasound in complementary diagnosis and in follow up of community-acquired pneumonia (cap). BMC Med. Imaging 2017, 17, 52. [Google Scholar] [CrossRef] [Green Version]
- Long, L.; Zhao, H.T.; Zhang, Z.Y.; Wang, G.Y.; Zhao, H.L. Lung ultrasound for the diagnosis of pneumonia in adults: A meta-analysis. Medicine 2017, 96, e5713. [Google Scholar] [CrossRef]
- Ticinesi, A.; Lauretani, F.; Nouvenne, A.; Mori, G.; Chiwussi, G.; Maggio, M.; Meschi, T. Lung ultrasound and chest x-ray for detecting pneumonia in an acute geriatric ward. Medicine 2016, 95, e4153. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Xiao, H.; Chen, B.; Zhang, S. Accuracy of Lung Ultrasonography versus Chest Radiography for the Diagnosis of Adult Community-Acquired Pneumonia: Review of the Literature and Meta-Analysis. PLoS ONE 2015, 10, e0130066. [Google Scholar] [CrossRef] [PubMed]
- Llamas-Álvarez, A.M.; Tenza-Lozano, E.M.; Latour-Pérez, J. Accuracy of Lung Ultrasonography in the Diagnosis of Pneumonia in Adults: Systematic Review and Meta-Analysis. Chest 2017, 151, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Karimi, E. Comparing Sensitivity of Ultrasonography and Plain Chest Radiography in Detection of Pneumonia; a Diagnostic Value Study. Arch. Acad. Emerg. Med. 2019, 7, e8. [Google Scholar]
- Lichtenstein, D.; Mezière, G. A lung ultrasound sign allowing bedside distinction between pulmonary edema and COPD: The comet-tail artifact. Intensive Care Med. 1998, 24, 1331–1334. [Google Scholar] [CrossRef]
- Zanobetti, M.; Scorpiniti, M.; Gigli, C.; Nazerian, P.; Vanni, S.; Innocenti, F.; Stefanone, V.T.; Savinelli, C.; Coppa, A.; Bigiarini, S.; et al. Point-of-Care Ultrasonography for Evaluation of Acute Dyspnea in the ED. Chest 2017, 151, 1295–1301. [Google Scholar] [CrossRef]
- Zanobetti, M.; Poggioni, C.; Pini, R. Can chest ultrasonography replace standard chest radiography for evaluation of acute dyspnea in the ED? Chest 2011, 139, 1140–1147. [Google Scholar] [CrossRef] [Green Version]
- Papanagnou, D.; Secko, M.; Gullett, J.; Stone, M.; Zehtabchi, S. Clinician-Performed Bedside Ultrasound in Improving Diagnostic Accuracy in Patients Presenting to the ED with Acute Dyspnea. West. J. Emerg. Med. 2017, 18, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Gallard, E.; Redonnet, J.P.; Bourcier, J.E.; Deshaies, D.; Largeteau, N.; Amalric, J.; Chedaddi, F.; Bourgeois, J.; Garnier, D.; Geeraerts, T. Diagnostic performance of cardiopulmonary ultrasound performed by the emergency physician in the management of acute dyspnea. Am. J. Emerg. Med. 2015, 33, 352–358. [Google Scholar] [CrossRef]
- Gaber, H.R.; Mahmoud, M.I.; Carnell, J.; Rohra, A.; Wuhantu, J.; Williams, S.; Rafique, Z.; Peacock, W.F. Diagnostic accuracy and temporal impact of ultrasound in patients with dyspnea admitted to the emergency department. Clin. Exp. Emerg. Med. 2019, 6, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Bekgoz, B.; Kilicaslan, I.; Bildik, F.; Keles, A.; Demircan, A.; Hakolgu, O.; Coskun, G.; Demir, H.A. BLUE protocol ultrasonography in Emergency Department patients presenting with acute dyspnea. Am. J. Emerg. Med. 2019, 37, 2020–2027. [Google Scholar] [CrossRef]
- Karabinis, A.; Saranteas, T.; Karakitsos, D.; Lichtenstein, D.; Poularas, J.; Yang, C.; Stefanadis, C. The ‘cardiac-lung mass’ artifact: An echocardiographic sign of lung atelectasis and/or pleural effusion. Crit. Care 2008, 12, R122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Via, G.; Lichtenstein, D.; Mojoli, F.; Rodi, G.; Neri, L.; Storti, E.; Klersy, C.; Lotti, G.; Braschi, A. Whole lung lavage: A unique model for ultrasound assessment of lung aeration changes. Intensive Care Med. 2010, 36, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Nazerian, P.; Vanni, S.; Volpicelli, G.; Gigli, C.; Zanobetti, M.; Bartolucci, M.; Ciavattone, A.; Lamorte, A.; Veltri, A.; Fabbri, A.; et al. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest 2014, 145, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazerian, P.; Volpicelli, G.; Gigli, C.; Becattini, C.; Papa, G.F.S.; Grifoni, S.; Vanni, S.; the Ultrasound Wells Study Group. Diagnostic Performance of Wells Score Combined with Point-of-care Lung and Venous Ultrasound in Suspected Pulmonary Embolism. Acad. Emerg. Med. 2017, 24, 270–280. [Google Scholar] [CrossRef] [Green Version]
- Mathis, G.; Blank, W.; Reissig, A.; Lechleitner, P.; Reub, J.; Schuler, A.; Beckh, S. Thoracic ultrasound for diagnosing pulmonary embolism: A prospective multicenter study of 352 patients. Chest 2005, 128, 1531–1538. [Google Scholar] [CrossRef]
- Jiang, L.; Ma, Y.; Zhao, C.; Shen, W.; Feng, X.; Xu, Y.; Zhang, M. Role of Transthoracic Lung Ultrasonography in the Diagnosis of Pulmonary Embolism: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0129909. [Google Scholar] [CrossRef]
- Squizzato, A.; Rancan, E.; Dentali, F.; Bonzini, M.; Guasti, L.; Steidl, L.; Mathis, G.; Ageno, W. Diagnostic accuracy of lung ultrasound for pulmonary embolism: A systematic review and meta-analysis. J. Thromb. Haemost. 2013, 11, 1269–1278. [Google Scholar] [CrossRef]
- Comert, S.S.; Caglayan, B.; Akturk, U.; Fidan, A.; Kıral, N.; Parmaksız, E.; Salepci, B.; Kurtulus, B.A.O. The role of thoracic ultrasonography in the diagnosis of pulmonary embolism. Ann. Thorac. Med. 2013, 8, 99–104. [Google Scholar] [CrossRef]
- Mathis, G.; Bitschnau, R.; Gehmacher, O.; Scheier, M.; Kopf, A.; Schwärzler, B.; Amann, T.; Doringer, W.; Hergan, K. Chest ultrasound in diagnosis of pulmonary embolism in comparison to helical CT. Ultraschall Med. 1999, 20, 54–59. [Google Scholar] [CrossRef]
- Lechleitner, P.; Raneburger, W.; Gamper, G.; Riedl, B.; Benedikt, E.; Theurl, A. Lung sonographic findings in patients with suspected pulmonary embolism. Ultraschall Med. 1998, 19, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Pfeil, A.; Reissig, A.; Heyne, J.P.; Wolf, G.; Kaiser, W.A.; Kroegel, C.; Hansch, A. Transthoracic sonography in comparison to multislice computed tomography in detection of peripheral pulmonary embolism. Lung 2010, 188, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Reissig, A.; Kroegel, C. Transthoracic ultrasound of lung and pleura in the diagnosis of pulmonary embolism: A novel non-invasive bedside approach. Respiration 2003, 70, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Reissig, A.; Heyne, J.P.; Kroegel, C. Diagnostik der Lungenembolie mittels transthorakaler Sonographie. Sonomorphologische Charakterisierung pulmonaler Läsionen und Vergleich mit der Spiral-Computertomographie [Diagnosis of pulmonary embolism by transthoracic sonography. Sono-morphologic characterization of pulmonary lesions and comparison with spiral computed tomography]. Dtsch. Med. Wochenschr. 2000, 125, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- Bugalho, A.; Ferreira, D.; Dias, S.S.; Schuhmann, M.; Branco, J.C.; Marques Gomes, M.J.; Eberhardt, R. The diagnostic value of transthoracic ultrasonographic features in predicting malignancy in undiagnosed pleural effusions: A prospective observational study. Respiration 2014, 87, 270–278. [Google Scholar] [CrossRef]
- Chen, M.H.; Yan, K.; Zhang, J.S. Ultrasonography in differential diagnosis of peripheral pulmonary diseases. Zhonghua Yi Xue Za Zhi 1994, 74, 19–22. [Google Scholar]
- Kang, H.W.; Kim, T.O.; Lee, B.R.; Yu, J.Y.; Chi, S.Y.; Ban, H.J.; Oh, I.J.; Kim, K.S.; Kwon, Y.S.; Kim, Y.I.; et al. Influence of diaphragmatic mobility on hypercapnia in patients with chronic obstructive pulmonary disease. J. Korean Med. Sci. 2011, 26, 1209–1213. [Google Scholar] [CrossRef]
- Okura, K.; Kawagoshi, A.; Iwakura, M.; Sugawara, K.; Takahashi, H.; Kashiwagura, T.; Homma, M.; Satake, M.; Shioya, T. Contractile capability of the diaphragm assessed by ultrasonography predicts nocturnal oxygen saturation in COPD. Respirology 2017, 22, 301–306. [Google Scholar] [CrossRef]
- Marchioni, A.; Castaniere, I.; Tonelli, R.; Fantini, R.; Fontana, M.; Tabbì, L.; Viani, A.; Giaroni, F.; Ruggieri, V.; Cerri, S.; et al. Ultrasound-assessed diaphragmatic impairment is a predictor of outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease undergoing noninvasive ventilation. Crit. Care 2018, 22, 109. [Google Scholar] [CrossRef] [Green Version]
- Antenora, F.; Fantini, R.; Iattoni, A.; Castaniere, I.; Sdanganelli, A.; Livrieri, F.; Tonelli, R.; Zona, S.; Monelli, M.; Clini, E.M. Prevalence and outcomes of diaphragmatic dysfunction assessed by ultrasound technology during acute exacerbation of COPD: A pilot study. Respirology 2017, 22, 338–344. [Google Scholar] [CrossRef]
- Matamis, D.; Soilemezi, E.; Tsagourias, M.; Akoumianaki, E.; Dimassi, S.; Boroli, F.; Richard, J.C.M.; Brochard, M. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013, 39, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Schepens, T.; Verbrugghe, W.; Dams, K.; Corthouts, B.; Parizel, P.M.; Jorens, P.G. The course of diaphragm atrophy in ventilated patients assessed with ultrasound: A longitudinal cohort study. Crit. Care 2015, 19, 422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reissig, A.; Copetti, R.; Mathis, G.; Mempel, C.; Schuler, A.; Zechner, P.; Aliberti, S.; Neumann, R.; Kroegel, C.; Hoyer, H. Lung ultrasound in the diagnosis and follow-up of community-acquired pneumonia: A prospective, multicenter, diagnostic accuracy study. Chest 2012, 142, 965–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acar, H.; Yılmaz, S.; Yaka, E.; Doğan, N.Ö.; Özbek, A.E.; Pekdemir, M. Evaluation of the Diagnostic Role of Bedside Lung Ultrasonography in Patients with Suspected Pulmonary Embolism in the Emergency Department. Balkan Med. J. 2017, 34, 356–361. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Voting Results | Conclusion | Designation or Reaction |
|---|---|---|
| ≥80% positive votes | Agreed for | 1 |
| ≤50% positive votes | Agreed against | 2 |
| 51–79% positive votes | Indeterminate | Statement re-debated and voted on in second and/or the third round voting |
| Grade | Interpretation |
|---|---|
| A | High—data from multiple meta-analyses, and/or it is unlikely that further research will change the credibility of the effectiveness or accuracy of the method |
| B | Moderate—data from individual large non-randomized trials (meta-analysis, prospective cohort study), and/or further testing may have a significant impact on the credibility of the effectiveness or accuracy of the method |
| C | Low or very low—agreed expert opinion and/or data from small studies, retrospective studies, registers, case series, or case reports, and/or it is very likely that further testing will have an important impact on the credibility of effectiveness or accuracy of the method. Any estimation of the effects or accuracy of the method is very uncertain (very low) |
| Strength of Recommendation | Interpretation and Practical Implication of Recommendation |
|---|---|
| 1A | strong recommendation; the given procedure should be widely used, as long as there are no strong contraindications |
| 1B | strong recommendation, but with a smaller degree of certainty; probably right in most individual cases |
| 1C | the average (mean) strength of recommendation; the recommendation may change after obtaining more reliable data; probably right |
| 2A | the average (mean) strength of recommendation; the decision on its adoption is a matter of choice and may depend on local and individual conditions; intervention does not have to be used |
| 2B | weak recommendation; alternative conduct can be just as good or better |
| 2C | weak recommendation; alternative treatment is probably equally acceptable |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buda, N.; Kosiak, W.; Wełnicki, M.; Skoczylas, A.; Olszewski, R.; Piotrkowski, J.; Skoczyński, S.; Radzikowska, E.; Jassem, E.; Grabczak, E.M.; et al. Recommendations for Lung Ultrasound in Internal Medicine. Diagnostics 2020, 10, 597. https://doi.org/10.3390/diagnostics10080597
Buda N, Kosiak W, Wełnicki M, Skoczylas A, Olszewski R, Piotrkowski J, Skoczyński S, Radzikowska E, Jassem E, Grabczak EM, et al. Recommendations for Lung Ultrasound in Internal Medicine. Diagnostics. 2020; 10(8):597. https://doi.org/10.3390/diagnostics10080597
Chicago/Turabian StyleBuda, Natalia, Wojciech Kosiak, Marcin Wełnicki, Agnieszka Skoczylas, Robert Olszewski, Jakub Piotrkowski, Szymon Skoczyński, Elżbieta Radzikowska, Ewa Jassem, Elżbieta Magdalena Grabczak, and et al. 2020. "Recommendations for Lung Ultrasound in Internal Medicine" Diagnostics 10, no. 8: 597. https://doi.org/10.3390/diagnostics10080597