The Impact of Immunomodulatory Treatment on Kappa Free Light Chains as Biomarker in Neuroinflammation

 , , and
, , and 
Abstract
:1. Introduction
2. Methods
2.1. Retrospectively Collected Data
2.2. Prospectively Collected Data
2.2.1. Intravenous Methylprednisolone Treatment
2.2.2. Plasma Exchange Therapy
2.2.3. Immunoadsorption Therapy
2.2.4. Intravenous Immunoglobulin Treatment
2.2.5. Pre-Analytic Conditions
2.3. Analytical Procedures
2.4. Statistical Analysis
3. Results
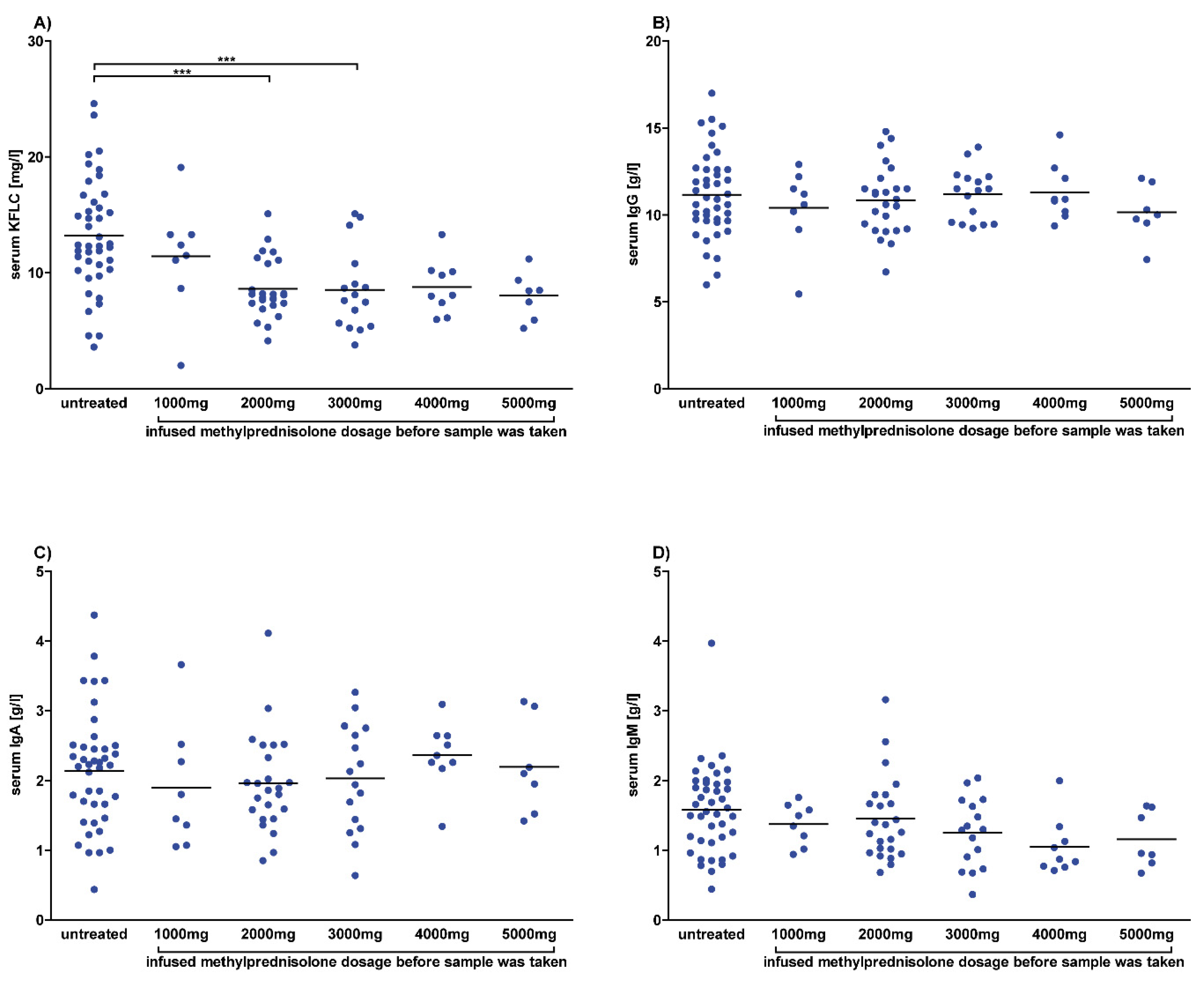
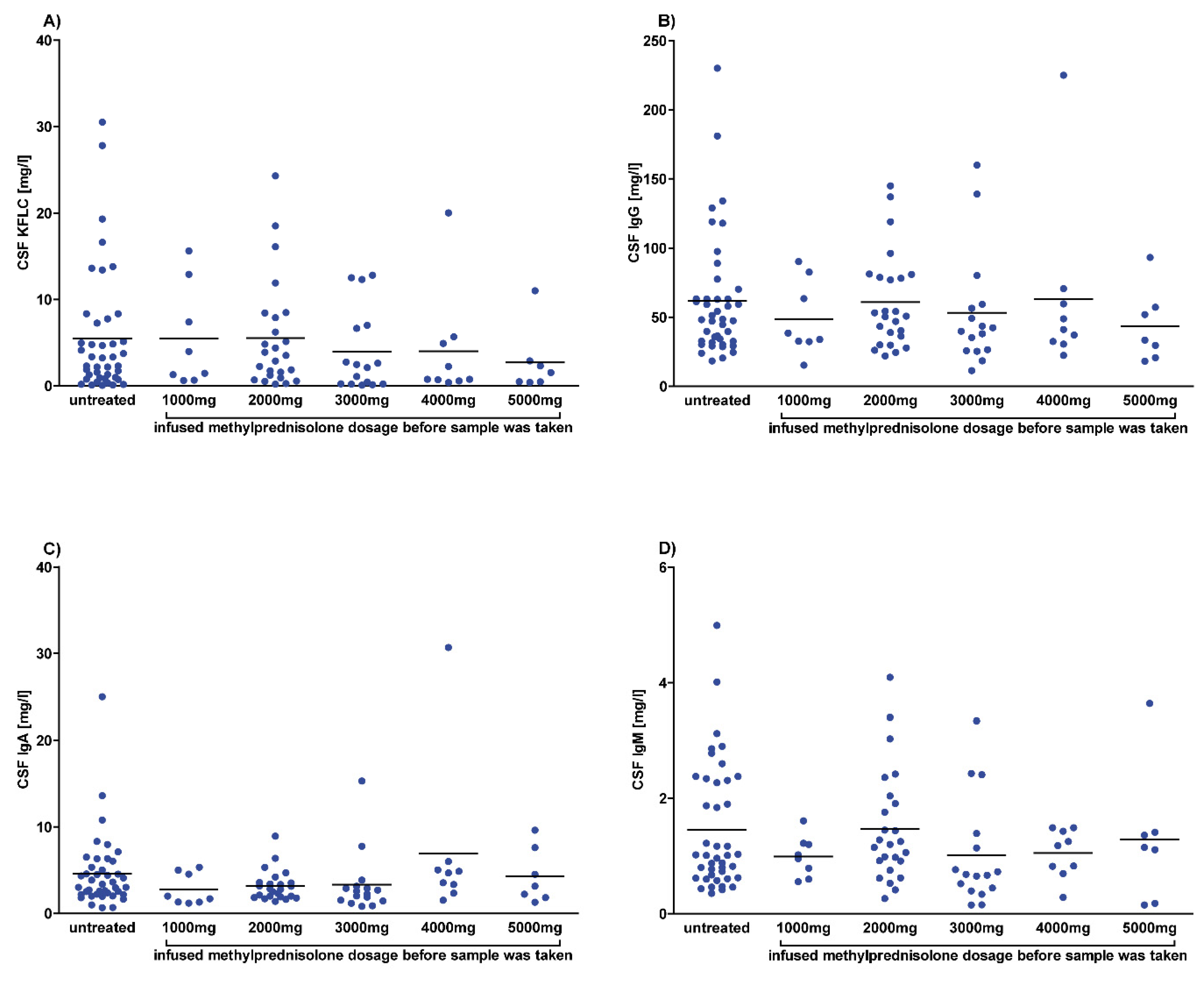
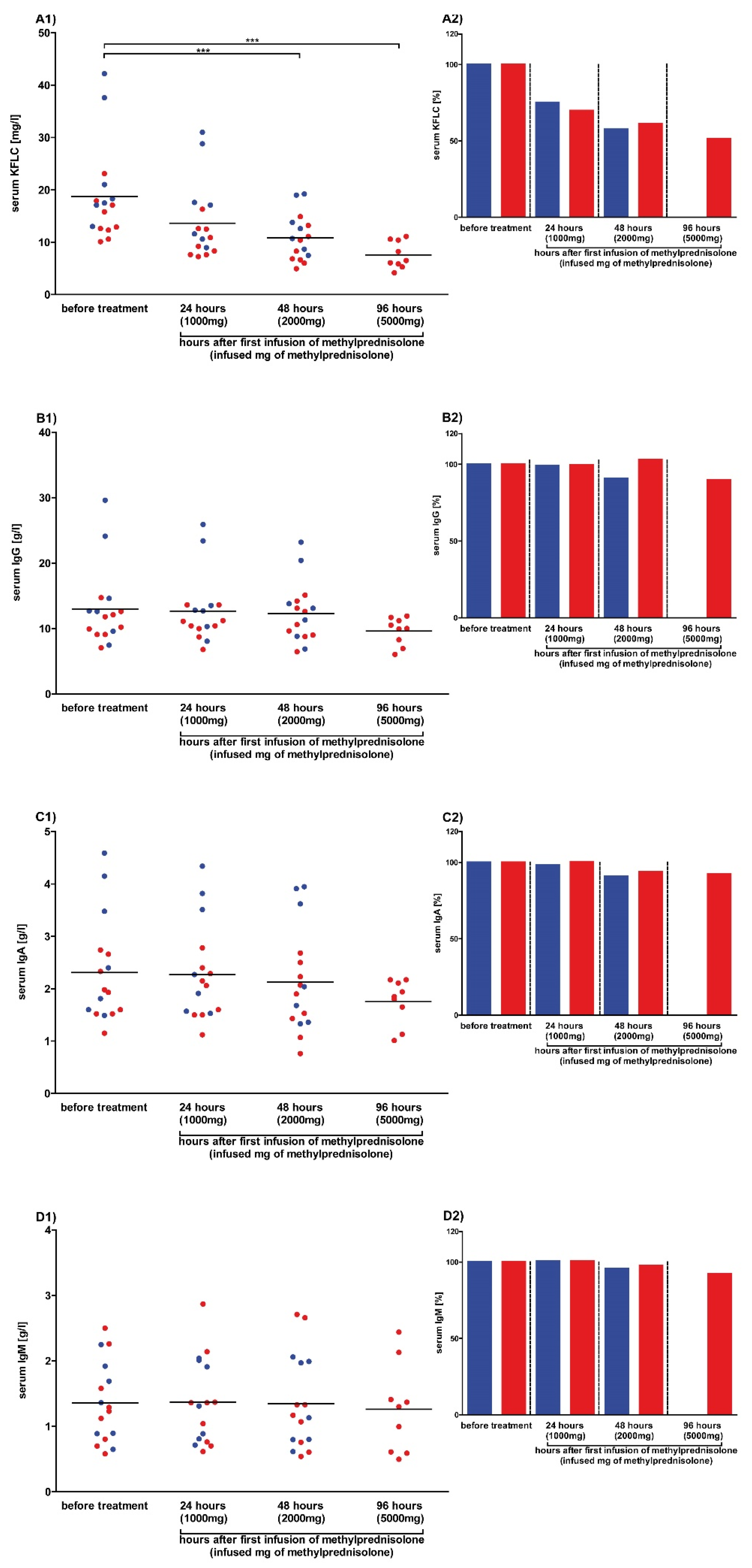
3.1. Mean Serum KFLC Concentrations are Lower in Patients Treated with Methylprednisolone
3.2. Serum KFLC Concentrations Continuously Decrease with Increasing Steroid Dosage
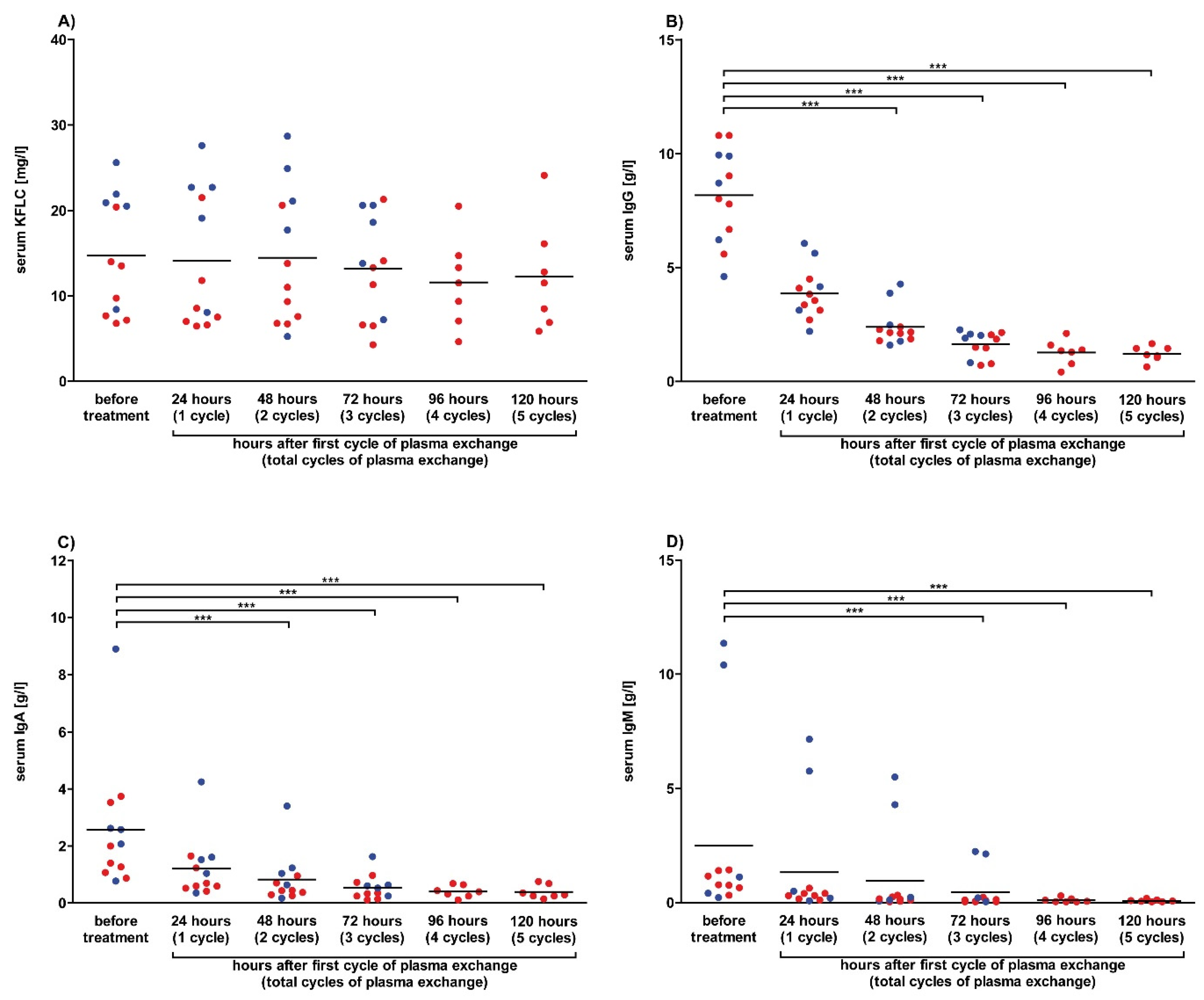
3.3. Plasmapheresis Has No Impact on Serum KFLC Concentrations
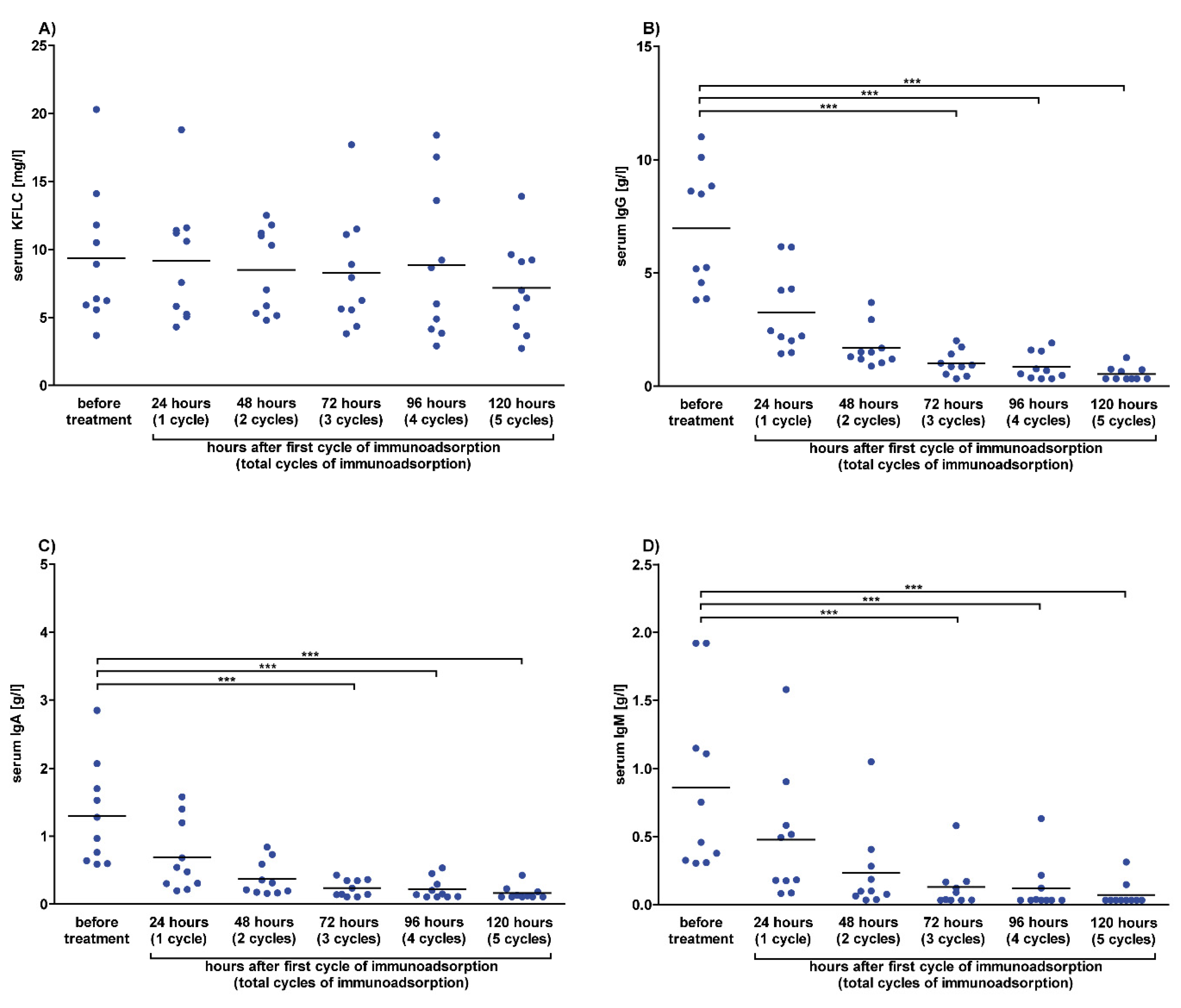
3.4. Immunoadsorption Has No Impact on Serum KFLC Concentrations
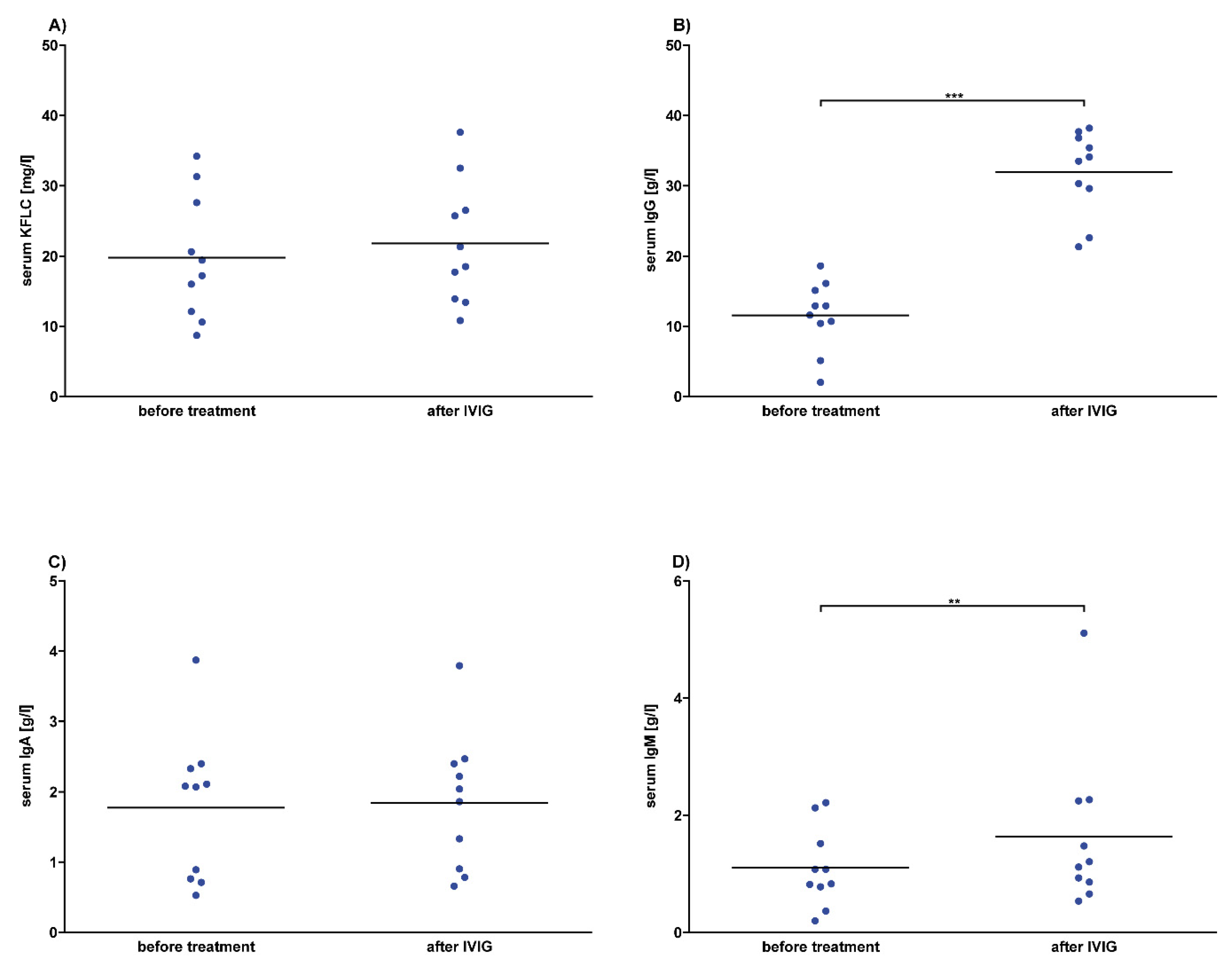
3.5. No Effects of Intravenous Immunoglobulins on Serum KFLC Values
3.6. KFLC Are Stable Despite Various Pre-Analytical Effects
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| KFLC | Kappa free light chains |
| CSF | cerebrospinal fluid |
| MS | multiple sclerosis |
| CIS | clinically isolated syndrome |
| Ig | immunoglobulin |
| IVIG | intravenous immunoglobulin |
| NMDA | N-methyl-D-aspartate |
References
- Stangel, M.; Fredrikson, S.; Meinl, E.; Petzold, A.; Stuve, O.; Tumani, H. The utility of cerebrospinal fluid analysis in patients with multiple sclerosis. Nat. Rev. Neurol. 2013, 9, 267–276. [Google Scholar] [CrossRef]
- Reiber, H. Cerebrospinal fluid data compilation and knowledge-based interpretation of bacterial, viral, parasitic, oncological, chronic inflammatory and demyelinating diseases. Diagnostic patterns not to be missed in neurology and psychiatry. Arq. Neuropsiquiatr. 2016, 74, 337–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2017, 17, 162–173. [Google Scholar] [CrossRef]
- Kuhle, J.; Disanto, G.; Dobson, R.; Adiutori, R.; Bianchi, L.; Topping, J.; Bestwick, J.P.; Meier, U.C.; Marta, M.; Costa, G.D.; et al. Conversion from clinically isolated syndrome to multiple sclerosis: A large multicentre study. Mult. Scler. 2015, 21, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Tintore, M.; Rovira, À.; Río, J.; Otero-Romero, S.; Arrambide, G.; Tur, C.; Comabella, M.; Nos, C.; Arévalo, M.J.; Negrotto, L.; et al. Defining high, medium and low impact prognostic factors for developing multiple sclerosis. Brain 2015, 138, 1863–1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franciotta, D.; Lolli, F. Interlaboratory reproducibility of isoelectric focusing in oligoclonal band detection. Clin. Chem. 2007, 53, 1557–1558. [Google Scholar] [CrossRef] [PubMed]
- Luxton, R.W.; McLean, B.N.; Thompson, E.J. Isoelectric focusing versus quantitative measurements in the detection of intrathecal local synthesis of IgG. Clin. Chim. Acta. 1990, 187, 297–308. [Google Scholar] [CrossRef]
- Presslauer, S.; Milosavljevic, D.; Brucke, T.; Bayer, P.; Hubl, W. Elevated levels of kappa free light chains in CSF support the diagnosis of multiple sclerosis. J. Neurol. 2008, 255, 1508–1514. [Google Scholar] [CrossRef]
- Senel, M.; Tumani, H.; Lauda, F.; Presslauer, S.; Mojib-Yezdani, R.; Otto, M.; Brettschneider, J. Cerebrospinal fluid immunoglobulin kappa light chain in clinically isolated syndrome and multiple sclerosis. PLoS ONE 2014, 9, e88680. [Google Scholar] [CrossRef]
- Hopper, J.E.; Papagiannes, E. Evidence by radioimmunoassay that mitogen-activated human blood mononuclear cells secrete significant amounts of light chain Ig unassociated with heavy chain. Cell Immunol. 1986, 101, 122–131. [Google Scholar] [CrossRef]
- Kaplan, B.; Aizenbud, B.M.; Golderman, S.; Yaskariev, R.; Sela, B.A. Free light chain monomers in the diagnosis of multiple sclerosis. J. Neuroimmunol. 2010, 229, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B.; Livneh, A.; Sela, B.A. Immunoglobulin free light chain dimers in human diseases. Sci. World J. 2011, 11, 726–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Süße, M.; Hannich, M.; Petersmann, A.; Zylla, S.; Pietzner, M.; Nauck, M.; Dressel, A. Kappa free light chains in cerebrospinal fluid to identify patients with oligoclonal bands. Eur. J. Neurol. 2018, 25, 1134–1139. [Google Scholar] [CrossRef]
- Schwenkenbecher, P.; Wurster, U.; Suhs, K.W.; Stangel, M.; Skripuletz, T. Applying the 2017 McDonald diagnostic criteria for multiple sclerosis. Lancet Neurol. 2018, 17, 498. [Google Scholar] [CrossRef]
- Schwenkenbecher, P.; Konen, F.F.; Wurster, U.; Jendretzky, K.F.; Gingele, S.; Sühs, K.W.; Pul, R.; Witte, T.; Stangel, M.; Skripuletz, T. The Persisting Significance of Oligoclonal Bands in the Dawning Era of Kappa Free Light Chains for the Diagnosis of Multiple Sclerosis. Int. J. Mol. Sci. 2018, 19, E3796. [Google Scholar] [CrossRef] [Green Version]
- Schwenkenbecher, P.; Sarikidi, A.; Bönig, L.; Wurster, U.; Bronzlik, P.; Sühs, K.W.; Pul, R.; Stangel, M.; Skripuletz, T. Clinically Isolated Syndrome According to McDonald 2010: Intrathecal IgG Synthesis Still Predictive for Conversion to Multiple Sclerosis. Int. J. Mol. Sci. 2017, 18, E2061. [Google Scholar] [CrossRef] [Green Version]
- Schwenkenbecher, P.; Sarikidi, A.; Wurster, U.; Bronzlik, P.; Sühs, K.W.; Raab, P.; Stangel, M.; Pul, R.; Skripuletz, T. McDonald Criteria 2010 and 2005 Compared: Persistence of High Oligoclonal Band Prevalence Despite Almost Doubled Diagnostic Sensitivity. Int. J. Mol. Sci. 2016, 17, E1592. [Google Scholar] [CrossRef] [Green Version]
- Schwenkenbecher, P.; Konen, F.F.; Wurster, U.; Witte, T.; Gingele, S.; Sühs, K.W.; Stangel, M.; Skripuletz, T. Reiber’s Diagram for Kappa Free Light Chains: The New Standard for Assessing Intrathecal Synthesis? Diagnostics 2019, 9, E194. [Google Scholar] [CrossRef] [Green Version]
- Reiber, H. Cerebrospinal fluid--physiology, analysis and interpretation of protein patterns for diagnosis of neurological diseases. Mult. Scler. 1998, 4, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Reiber, H. Proteins in cerebrospinal fluid and blood: Barriers, CSF flow rate and source-related dynamics. Restor. Neurol. Neurosci. 2003, 21, 79–96. [Google Scholar] [PubMed]
- Andersson, M.; Alvarez-Cermeno, J.; Bernardi, G.; Cogato, I.; Fredman, P.; Frederiksen, J.; Fredrikson, S.; Gallo, P.; Grimaldi, L.M.; Grønning, M.; et al. Cerebrospinal fluid in the diagnosis of multiple sclerosis: A consensus report. J. Neurol. Neurosurg. Psychiatry 1994, 57, 897–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiber, H. External quality assessment in clinical neurochemistry: Survey of analysis for cerebrospinal fluid (CSF) proteins based on CSF/serum quotients. Clin. Chem. 1995, 41, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.; Cook, S.D.; Dowling, P.C. Steroid therapy in multiple sclerosis. Point of view. Arch. Neurol. 1987, 44, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Compston, A. Methylprednisolone and multiple sclerosis. Arch. Neurol. 1988, 45, 669–670. [Google Scholar] [CrossRef] [PubMed]
- Laterre, E.C.; Callewaert, A.; Heremans, J.F.; Sfaello, Z. Electrophoretic morphology of gamma globulins in cerebrospinal fluid of multiple sclerosis and other diseases of the nervous system. Neurology 1970, 20, 982–990. [Google Scholar] [CrossRef] [Green Version]
- Link, H.; Tibbling, G. Principles of albumin and IgG analyses in neurological disorders. III. Evaluation of IgG synthesis within the central nervous system in multiple sclerosis. Scand J. Clin. Lab. Invest. 1977, 37, 397–401. [Google Scholar] [CrossRef]
- Reiber, H.; Zeman, D.; Kušnierová, P.; Mundwiler, E.; Bernasconi, L. Diagnostic relevance of free light chains in cerebrospinal fluid - The hyperbolic reference range for reliable data interpretation in quotient diagrams. Clin. Chim. Acta. 2019, 497, 153–162. [Google Scholar] [CrossRef]
- Trotter, J.L.; Garvey, W.F. Prolonged effects of large-dose methylprednisolone infusion in multiple sclerosis. Neurology 1980, 30, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Tourtellotte, W.W.; Potvin, A.R.; Ma, B.I.; Baumhefner, R.W.; Walsh, M.J.; Dickstein, P.; Ingram, T.; Cowan, T.; Shapshak, P.; Delmotte, P. Isotachophoresis quantitation of subfractions of multiple sclerosis intra-blood-brain barrier IgG synthesis modulated by ACTH and/or steroids. Neurology 1982, 32, 261–266. [Google Scholar] [CrossRef]
- Tourtellotte, W.W.; Potvin, A.R.; Baumhefner, R.W.; Potvin, J.H.; Ma, B.I.; Syndulko, K.; Petrovich, Z. Multiple sclerosis de novo CNS IgG synthesis. Effect of CNS irradiation. Arch. Neurol. 1980, 37, 620–624. [Google Scholar] [CrossRef]
- Durelli, L.; Cocito, D.; Riccio, A.; Barile, C.; Bergamasco, B.; Baggio, G.F.; Perla, F.; Delsedime, M.; Gusmaroli, G.; Bergamini, L. High-dose intravenous methylprednisolone in the treatment of multiple sclerosis: Clinical-immunologic correlations. Neurology 1986, 36, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Frequin, S.T.; Barkhof, F.; Lamers, K.J.; Hommes, O.R.; Borm, G.F. CSF myelin basic protein, IgG and IgM levels in 101 MS patients before and after treatment with high-dose intravenous methylprednisolone. Acta. Neurol. Scand. 1992, 86, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Fauci, A.S. Mechanisms of corticosteroid action on lymphocyte subpopulations. I. Redistribution of circulating T and b lymphocytes to the bone marrow. Immunology 1975, 28, 669–680. [Google Scholar] [PubMed]
- Fauci, A.S.; Dale, D.C. The effect of in vivo hydrocortisone on sub-populations of human lymphocytes. J. Clin. Invest. 1974, 53, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Cohn, L.A. The influence of corticosteroids on host defense mechanisms. J. Vet. Intern. Med. 1991, 5, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Berger, B.; Hottenrott, T.; Leubner, J.; Dersch, R.; Rauer, S.; Stich, O.; Prüss, H. Transient spurious intrathecal immunoglobulin synthesis in neurological patients after therapeutic apheresis. BMC Neurol. 2015, 15, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, W.F.; Stewart, A.K.; Rock, G.A.; Sternbach, M.; Sutton, D.M.; Barrett, B.J.; Heidenheim, A.P.; Garg, A.X.; Churchill, D.N. Canadian Apheresis Group. Plasma exchange when myeloma presents as acute renal failure: A randomized, controlled trial. Ann. Intern. Med. 2005, 143, 777–784. [Google Scholar] [CrossRef] [PubMed]
- McLeod, B.C.; Viernes, A.L.; Sassetti, R.J. Serum-free light chain analysis by crossed immunoelectrophoresis: Correlation with plasmapheresis in light chain disease nephropathy. Am. J. Hematol. 1983, 15, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Cserti, C.; Haspel, R.; Stowell, C.; Dzik, W. Light-chain removal by plasmapheresis in myeloma-associated renal failure. Transfusion 2007, 47, 511–514. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A. Light chains of human immunoglobulins. Methods Enzymol. 1985, 116, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Leung, N.; Gertz, M.A.; Zeldenrust, S.R.; Rajkumar, S.V.; Dispenzieri, A.; Fervenza, F.C.; Kumar, S.; Lacy, M.Q.; Lust, J.A.; Greipp, P.R.; et al. Improvement of cast nephropathy with plasma exchange depends on the diagnosis and on reduction of serum free light chains. Kidney Int. 2008, 73, 1282–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchison, C.A.; Cockwell, P.; Stringer, S.; Bradwell, A.; Cook, M.; Gertz, M.A.; Dispenzieri, A.; Winters, J.L.; Kumar, S.; Rajkumar, S.V.; et al. Early reduction of serum-free light chains associates with renal recovery in myeloma kidney. J. Am. Soc. Nephrol. 2011, 22, 1129–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snozek, C.L.H.; Kinard, T.N.; Adamski, J. Rapid reduction of extremely high kappa free light chains in a patient with myeloma cast nephropathy. J. Clin. Apher. 2018, 33, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Snyder, H.W., Jr.; Balint, J.P., Jr.; Jones, F.P. Modulation of immunity in patients with autoimmune disease and cancer treated by extracorporeal immunoadsorption with PROSORBA® columns. Semin. Hematol. 1989, 26, 31–41. [Google Scholar] [PubMed]
- Titulaer, M.J.; McCracken, L.; Gabilondo, I.; Armangué, T.; Glaser, C.; Iizuka, T.; Honig, L.S.; Benseler, S.M.; Kawachi, I.; Martinez-Hernandez, E.; et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: An observational cohort study. Lancet Neurol. 2013, 12, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaveri, S.V.; Maddur, M.S.; Hegde, P.; Lacroix-Desmazes, S.; Bayry, J. Intravenous immunoglobulins in immunodeficiencies: More than mere replacement therapy. Clin. Exp. Immunol. 2011, 164, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Mignogna, M.D.; Fortuna, G.; Ruoppo, E.; Adamo, D.; Leuci, S.; Fedele, S. Variations in serum hemoglobin, albumin, and electrolytes in patients receiving intravenous immunoglobulin therapy: A real clinical threat? Am. J. Clin. Dermatol. 2007, 8, 291–299. [Google Scholar] [CrossRef]
- Jenner, E. Serum free light chains in clinical laboratory diagnostics. Clin. Chim. Acta. 2014, 427, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwenkenbecher, P.; Janssen, T.; Wurster, U.; Neyazi, A.; Ahlbrecht, J.; Puppe, W.; Bönig, L.; Sühs, K.W.; Stangel, M.; Ganzenmüller, T.; et al. The Influence of Blood Contamination on Cerebrospinal Fluid Diagnostics. Front. Neurol. 2019, 10, 584. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment or Pre-Analytic Condition | Females, n (%) | Median Age, Years (Range) |
|---|---|---|
| Intravenous methylprednisolone | 10/16 (63%) | 41.5 (18–70) |
| Plasma exchange | 5/12 (42%) | 50.5 (24–80) |
| Immunoadsorption | 6/10 (60%) | 31 (19–52) |
| Intravenous immunoglobulin | 4/10 (40%) | 63 (45–76) |
| Sample method (EDTA or serum tube) | 17/33 (52%) | 45 (25–84) |
| Storage time and temperature | 8/16 (50%) | 44.5 (25–80) |
| Blood contamination | 11/17 (65%) | 44 (32–84) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konen, F.F.; Wurster, U.; Witte, T.; Jendretzky, K.F.; Gingele, S.; Tumani, H.; Sühs, K.-W.; Stangel, M.; Schwenkenbecher, P.; Skripuletz, T. The Impact of Immunomodulatory Treatment on Kappa Free Light Chains as Biomarker in Neuroinflammation. Cells 2020, 9, 842. https://doi.org/10.3390/cells9040842
Konen FF, Wurster U, Witte T, Jendretzky KF, Gingele S, Tumani H, Sühs K-W, Stangel M, Schwenkenbecher P, Skripuletz T. The Impact of Immunomodulatory Treatment on Kappa Free Light Chains as Biomarker in Neuroinflammation. Cells. 2020; 9(4):842. https://doi.org/10.3390/cells9040842
Chicago/Turabian StyleKonen, Franz Felix, Ulrich Wurster, Torsten Witte, Konstantin Fritz Jendretzky, Stefan Gingele, Hayrettin Tumani, Kurt-Wolfram Sühs, Martin Stangel, Philipp Schwenkenbecher, and Thomas Skripuletz. 2020. "The Impact of Immunomodulatory Treatment on Kappa Free Light Chains as Biomarker in Neuroinflammation" Cells 9, no. 4: 842. https://doi.org/10.3390/cells9040842