
Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review
by
 , , , and
, , , and
Walid Shalata
1,*,† ,
,
Amjad Abu-salman
2,†, 
Rachel Steckbeck
3,
Binil Mathew Jacob
3,
Ismaell Massalha
1 and
Alexander Yakobson
1 1
The Legacy Heritage Center & Dr. Larry Norton Institute, Soroka Medical Center, Beer Sheva 84105, Israel
2
Cardiology Division, Soroka Medical Center, Beer Sheva 84105, Israel
3
Medical School for International Health, Ben Gurion University of the Negev, Beer Sheva 84105, Israel
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this paper.
Cancers 2021, 13(20), 5218; https://doi.org/10.3390/cancers13205218
Submission received: 4 September 2021
/
Revised: 2 October 2021
/
Accepted: 8 October 2021
/
Published: 18 October 2021
(This article belongs to the Special Issue Cancer Immunotherapy and Immune-Related Adverse Events)
Abstract
:Simple Summary
This review article addresses the toxic effects on the heart associated with the use of certain cancer-treating drugs known as immune checkpoint inhibitors. These drugs target specific proteins in the cell cycle that are abundantly expressed in cancerous cells; however, they inadvertently damage non-cancerous tissue. In the heart, this occurs in the form of dysfunction or death of smooth muscle cells, leading to consequences such as infection, heart rhythm changes, and hormonally dependent and independent ischemia. This review examines the average and median onset of these drug toxicities as well as antidotes. One key observation is that these side effects are positively skewed, meaning they occur early in cancer treatment.
Abstract
Immune checkpoint inhibitors are immune stimulatory drugs used to treat many types of cancer. These drugs are antibodies against inhibitory proteins, such as CTLA-4 and PD-1/PD-L1, that are expressed on immune cells. When bound, they allow for increased stimulation of T cells to fight tumor cells. However, immune checkpoint inhibitors have several immune-related adverse effects. Many cases have come to light recently of cardiotoxicity as a result of treatment with these drugs. Cardiotoxicity from immune checkpoint inhibitors is unique due to its rarity and high mortality rate. Patients with this toxicity may present with myocarditis, pericarditis, Takotsubo cardiomyopathy, conduction disorders, and others within just a few weeks of starting immune checkpoint inhibitors. We present here a review of the current research on immune checkpoint inhibitors, their associated cardiotoxicities, the timing of presentation of these conditions, lab tests and histology for each condition, and finally the treatment of patients with cardiotoxicity. We observe a positive skew in the onset of presentation, which is significant for the treating physician.
1. Introduction
In the last several years, immune checkpoint inhibitors (ICIs) have become the backbone of the treatment plan in many types of cancer. Tumor cells express neoantigens, mutated proteins that immune cells can recognize as foreign and destroy; however, many tumors also express factors that inhibit the immune system, thus allowing them to grow undetected in the body [1]. Immune checkpoint inhibitors work by blocking the inhibitory signals from tumor cells to T cells that recognize them, thus allowing the tumor cells to be destroyed by the patient’s own immune system. The first ICI was approved by the FDA in 2011 [2], and since then several different ICIs against a variety of targets have been approved. These include monoclonal antibodies against programmed death-1 (PD-1), such as nivolumab or pembrolizumab; ligands of PD-1 (PD-L1), such as atezolizumab; and cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4), such as ipilimumab. These antibodies have complementary mechanisms of action to one another, and so they are often used in combination.
CTLA-4 is a marker expressed on activated T cells and regulatory T cells [3]. Competing with the stimulatory molecule B7, it binds to CD80 and CD86 on antigen presenting cells with high affinity, leading to inhibition of T cell proliferation and activity [3]. Blocking CTLA-4 with ipilimumab allows T cells to fight a tumor more effectively by removing inhibitory signals. The PD-1/PD-L1 system works very similarly; PD-1 on T cells binds to PD-L1, which is widely expressed on antigen-presenting cells as well as the tissues of the heart, muscle, lung, pancreas, and many more [4]. PD-L1 is considered essential to prevent autoimmunity in these tissues; lack of PD-1 leads to increased survival, proliferation, and killing capacity of T cells, which can cause autoimmunity [5]. PD-1/PD-L1 signaling also promotes the proliferation of regulatory T cells, further protecting against autoimmunity [4]. Importantly, some tumors can express PD-L1, thus inhibiting host immune responses against them [4]. Thus, blocking the PD-1/PD-L1 interaction through antibodies promotes immune reactions against tumor cells.
Though ICIs are effective in treating cancer; they have adverse effects distinct from cytotoxic chemotherapy because they directly affect the immune system. Immune-related adverse events (IRAEs) happen in 70–90% of patients treated with ICIs, with severe IRAEs happening in 10–15% of patients [6]; these reactions are fatal in up to 1.3% of patients [7]. Often, IRAEs occur within 1 year after treatment [8], but the risk of developing any IRAE increases with time [9]. These toxicities could be due to several causes: pre-existing self-reactive T cells that were inhibited becoming uninhibited, cross-reactivity between the tumor antigen and self-antigen, or T cells targeting a different but homologous antigen in the body as compared to the one on the tumor [6]. Signs and symptoms of ICI toxicity manifest as colitis, hepatitis, thyroiditis, hypophysitis, myo- or pericarditis, arthritis, uveitis, pneumonitis, or skin rash [8,10].
Cardiotoxicity due to ICIs is rare, with an incidence of up to 1% [11], but it is often severe and can be life threatening. Patients can present with cardiac fibrosis, cardiac arrest, autoimmune myocarditis, cardiomyopathy, heart failure, pericardial involvement, and vasculitis [10,11].
Here, we review immune checkpoint inhibitors, the cardiotoxicities they can cause, and the treatment of each cardiotoxicity. Though there have been multiple reviews on this subject already, there has been no research on the variations of time from beginning of treatment to the presentation of cardiotoxicity depending on the type of cardiotoxicity, the treatment, or the cancer being treated. In this review, we take special note of these differences and qualitatively evaluate them.
2. Materials and Methods
Multiple searches were performed on PubMed to obtain the studies used in this review, performed from 20 June 2021 to 31 July 2021. Search terms included “pericarditis with immune checkpoint inhibitors”, “cardiac toxicity immune checkpoint inhibitors”, and “myocarditis immune checkpoint inhibitors”, with results displayed from the last 10 years. The search terms were chosen to best find the broadest range of published papers on the topic of cardiac toxicity; in addition, myocarditis and pericarditis were searched for by name because they are the two most common cardiotoxicities that patients present with. From the search results, we reviewed all the papers displayed and found 134 relevant case studies and literature reviews.
All case reports were synthesized into a table. Of the case reports, all were published between the years 2015 and 2021, with the majority published between the years of 2018–2021. Case studies were segregated based on the specific antibody, the type of cardiotoxicity, and the type of cancer being treated. Trends were enumerated qualitatively through a table and a graph.
3. Cardiotoxicity
3.1. General
Cardiotoxicity is a very rare complication of immune checkpoint inhibitors, affecting up to 1% of patients; this percentage is higher in patients taking a combination of ICIs [11]. Others have argued that the total risk of cardiac events in patients with ICI therapy is much higher, from 3.1% [12] to 9.7% [13]. This discrepancy may be due to misclassification and difficult diagnosis of cardiac events caused by ICIs, especially during the current COVID-19 pandemic [14]. The most common presentation of cardiotoxicity due to ICIs is myocarditis (Table 1).
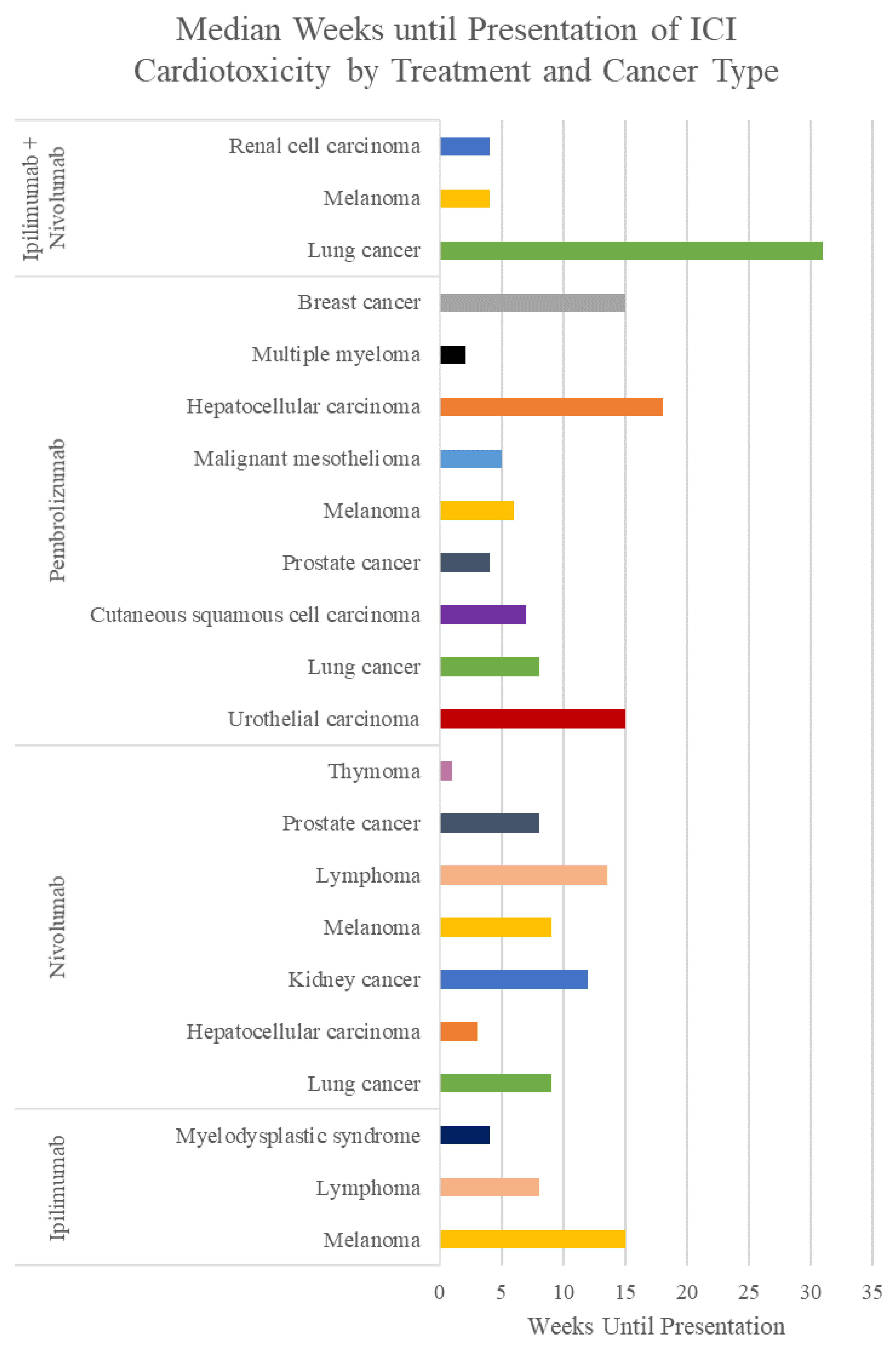
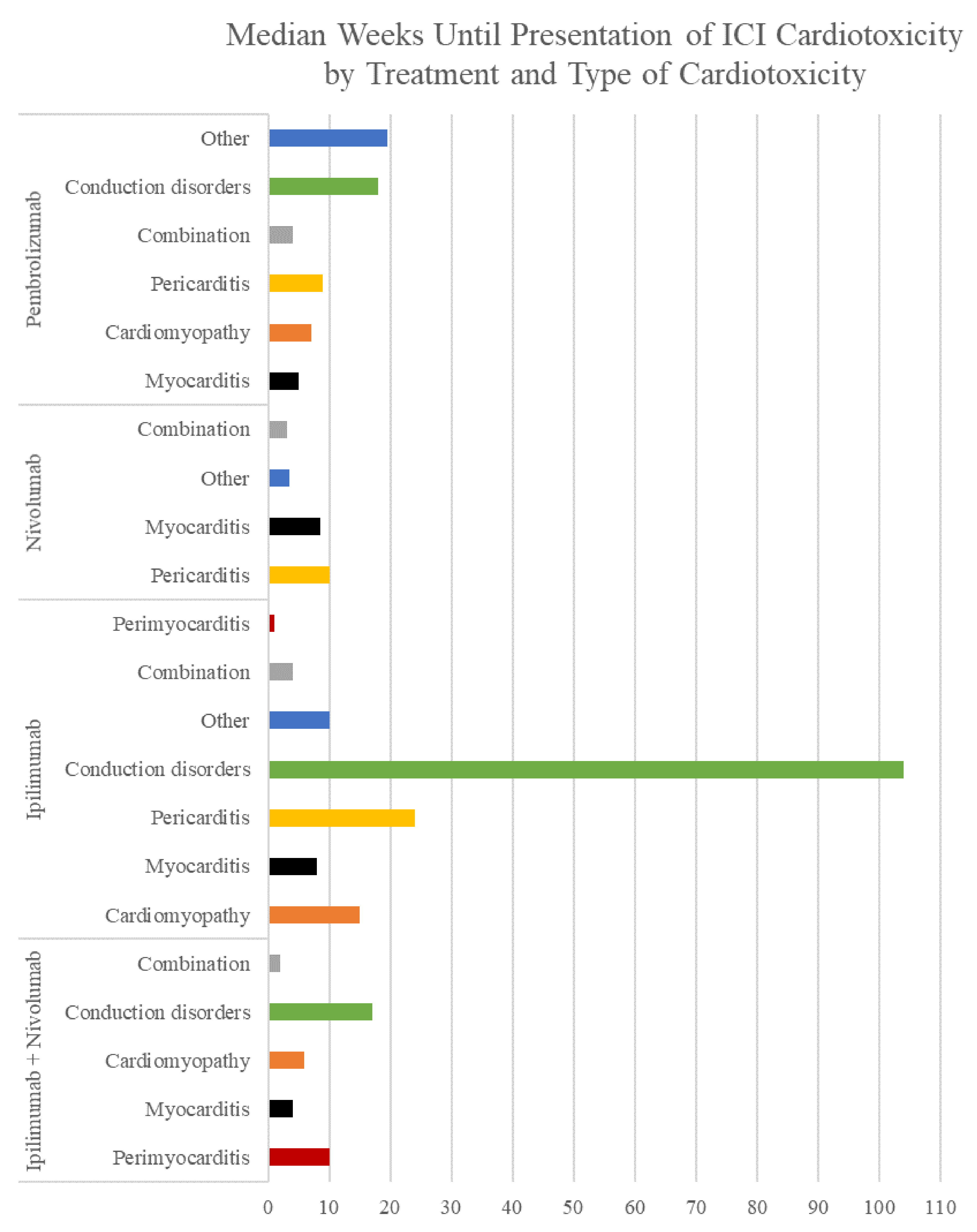
Patients can have a wide range of signs and symptoms, from asymptomatic to severe chest pain, dyspnea, multiorgan failure, and sudden death [27] (Appendix A). These symptoms usually begin within the first 3 months of starting immunotherapy, but they can also start up to a year after therapy finishes [27]; the average time until symptoms start varies between the treatment (Table 2), the patient’s cancer (Table 3, Figure 1), and the type of cardiotoxicity (Table 4, Figure 2).
The mechanism of cardiotoxicity is still under research, but it may primarily involve CD4+ mediated T cell inflammation [28]. A study by Tay et al. confirmed that nivolumab does not induce cardiomyocyte apoptosis like a cytotoxic drug such as doxorubicin does—rather, it increases pro-inflammatory cytokine production in CD4+ T cells only [29]. The most common cytokines produced include TNF-α, granzyme B, and IFN-γ [27]. Expression of the inflammatory transcription factors NLRP3, MyD88, and p65/NF-κB are also increased in cardiomyocytes after ICI treatment [30]. Further proving this point, anti-PD-1-treated mice had more CD4+ and CD8+ T cell infiltration in the heart as compared to a control group [29]. However, it is unclear exactly what the T cells are targeting.
Reinforcing the idea that T cells are the primary mediators of cardiotoxicity with ICIs, a remarkable study by Wang et al. shows that fatal myocarditis was developed in mice genetically predisposed to systemic autoimmunity due to PD-1 deficiency [31]. However, in mice, the myocarditis was caused by CD4+ and CD8+ T cells as well as autoantibodies against cardiomyocytes. Mice with a genetic predisposition to autoimmunity but without a PD-1 deficiency did not develop myocarditis, demonstrating that prevention of myocarditis is likely mediated by PD-1 [31]. Love et al. found in a similar study that CTLA-4 removal on T cells also caused severe myocarditis in mice, but lack of IL-12 prevented CD8+ T cells from proliferating, thus ameliorating the myocarditis [32]. PD-L1 expressed in the human myocardium is involved in protecting immune-mediated cardiac injury and inflammation [29].
Autoantibodies have been postulated to lead to cardiotoxicity in patients treated with ICIs. A case described by Martinez-Calle et al. showed that the patient did have IgG autoantibodies against cardiac troponin T, but it is unknown if the antibodies were present before initiation of ICI therapy [33]. Two other patients have shown autoantibody deposition in cardiac muscle, suggesting a direct relationship between the antibodies and myocarditis [34]. However, many more cases have stated that no autoantibodies were found on histology or blood tests [11,15,35], leading to the conclusion that autoantibodies are generally not involved in the pathogenesis of cardiotoxicity with ICIs.
3.2. Myocarditis
Myocarditis, or inflammation of the myocardial muscle, is the most common form of cardiotoxicity caused by ICIs. It is also the most fatal form of cardiotoxicity, with a mortality rate of up to 50% [16,36,37]. It was first recognized as an IRAE during clinical trials, and as use of ICIs has increased, awareness has also increased.
Myocarditis can develop as early as 2 weeks after starting ICI therapy [17]; however, the median amount of time after beginning ICI treatment that patients experience symptoms is 65 days [18]. Eighty-one percent of patients present within 3 months of initiation of therapy [17]. Patients with ICI-associated myocarditis can present with a wide range of symptoms. Most commonly, patients will have a primary complaint of shortness of breath [15,19]. Palpitations and signs of congestive heart failure, such as edema, fatigue, weakness, or wheezing, are also common symptoms [18].
On lab tests, patients will often experience elevation of BNP or NT-proBNP, signs of active inflammation such as elevated CRP and hepcidin, and elevated troponin and CK-MB [17,20]. Troponin is an important predictor of the patient’s risk of a major adverse cardiac event (MACE), which is defined as cardiovascular death, cardiac arrest, complete heart block, or cardio-genic shock [11,37]. Troponin I is the most useful troponin for this purpose; troponin T may be elevated with concurrent myositis, reducing its usefulness [37]. Patients who do not have an elevated troponin I almost never have myocarditis, making it a very sensitive tool, though it is not specific [38]. NT-proBNP is less specific for myocarditis and can be elevated due to cancer-related inflammation rather than ICI-associated cardiotoxicity [16,39]. An abnormal ECG is also common but is not always present [17].
The gold standard to diagnose myocarditis is endomyocardial biopsy [40,41]. The biopsy needs to be taken from about six regions because the area of inflammation is localized to specific regions in the heart [21,40]. Patients have been reported to have a wide range of histological findings suggestive of myocarditis. As stated earlier, autoantibodies are almost never found in these patients [15]. Histopathological evaluation of endomyocardial biopsies has revealed a lymphocytic infiltrate of CD4+ and CD8+ cells in the myocardium and conducting system of patients with myocarditis [11,19]. There may also be fibrosis without granulomas or histiocytes [17,26]. These T cell populations are clonally similar to those found in tumors as well, suggesting that cardiotoxicity is caused by antigen similarity; however, it may also be caused by reduced inhibition of self-reactive T cells [27]. PD-L1 is also highly expressed in the myocardium of these patients [19]. One of the youngest cases of pembrolizumab-induced myocarditis, described by Läubli et al. [42], similarly demonstrated predominant infiltration of CD8+ cells on myocardial biopsy. These findings seem to indicate that the cardiotoxicity is T-cell-mediated rather than antibody-mediated.
However helpful endomyocardial biopsy may be, this procedure is invasive and not routinely performed. A cardiac magnetic resonance scan (CMR) is also very effective and is the gold standard of imaging for myocarditis [21]. On CMR, patients will have active inflammation with increased capillary permeability, possible myocardial ischemia, and late gadolinium enhancement [17,21]. If CMR is unavailable, PET/CT is a good alternative [22].
Several studies have found that patients who receive combination ICI therapy, most commonly ipilimumab and nivolumab, have an increased risk of developing myocarditis as compared to patients only taking one ICI [6,16,39,43,44]. Zhang et al. also report that there is an increased risk of myocarditis with the female sex and older age [6]; other studies disagree, saying that there is no age association and higher risk with the male sex [16,43]. This discrepancy may be due to the fact that cardiac-adverse events have been more commonly reported in male patients than female patients in the past, since females have often been less represented in clinical trials [43]. There is no association of myocarditis with a specific type of cancer [36]. In addition, there is an increased risk of ICI-associated myocarditis with hypertension; tobacco use; and the use of prescription statins, ACE inhibitors, and angiotensin inhibitors [23]. Up to half of all patients with ICI-associated myocarditis will present with other, concurrent IRAEs [23,44]; in particular, up to 25% of patients with myocarditis may have concomitant myositis, and 10% may have concomitant myasthenia gravis [36].
Interestingly, a study by Awadalla et al. shows that patients receiving ICI therapy may have a lower likelihood of developing myocarditis when they have been vaccinated for influenza [45]. The study’s results show that patients with myocarditis were less likely to have received the flu vaccine; in addition, vaccinated patients who did develop myocarditis had lower serum troponin levels and were less likely to have a MACE [45].
PD-1 expression is constitutive in the myocardium and is important for normal immune function, so inhibition of this pathway can lead to severe issues [46]. In one study, Wang et al. showed that PD-1 deficiency in mice causes them to develop fatal autoimmune myocarditis, almost always within 10 weeks after birth [31]. Myocarditis did not develop in mice with a deficiency in immune-regulating molecules not in the PD-1/PD-L1 pathway [31]. However, Love et al. showed that myocarditis can also develop in mice deficient in CTLA-4 [32]. In humans, patients with myocarditis often have high expression of PD-L1 in cardiac tissue, suggesting that PD-L1 is used by the heart to prevent inflammation [37].
3.3. Pericarditis
Pericardial disease, or inflammation of the pericardial sac surrounding the heart, is another common form of cardiotoxicity, with an incidence of 0.3% [24,47]. This includes pericarditis, pericardial effusion, and even clinical tamponade [17]. Though it is not as fatal as myocarditis, it has a mortality rate of 13–21% [6,16,19,48]. On average, patients who develop pericarditis do so within 30 days of starting ICI treatment [16], but several cases have been described where pericarditis was diagnosed several months after starting treatment [35,49,50,51]. Often, patients will present with chest pain, shortness of breath, and hemodynamic instability after ICI therapy [16,24]. Shortness of breath is the most common symptom on presentation [23].
Patients will frequently show ECG changes during pericardial disease [16]. In addition, pericardial effusion or thickening may be seen on CT scan, and CMR will show pericardial inflammation and/or fibrosis [25]. Analysis of pericardial effusion fluid shows lymphocytes and plasma cells without evidence of malignant cells or microorganisms causing the symptoms [17,25,50]. There may also be a hemorrhage or fibrinous exudate present [25]. Pericarditis has rarely been reported to occur in conjunction with myocarditis [44,52]; a normal troponin level can rule out this possibility.
Several studies have shown that there is a higher risk of pericardial disease when ICIs are given for non-small-cell lung cancer (NSCLC) [17,39,47,48,53]. It is hypothesized that this could be due to the use of radiotherapy in lung cancer in addition to ICIs, which exposes more shared antigens [39,50]; however, other studies argue that pericardial diseases are also common complications of certain cancers, thus inflating the significance of this result [48]. In addition, pericarditis is more common in males, but there is no increased risk with age [16,22,53]. Inno et al. found that treatment with anti-PD-1 or anti-PD-L1 therapy is more associated with pericardial disease than anti-CTLA-4 therapy [53]. Patients with pericarditis will frequently display other IRAEs in addition to pericarditis, such as hyper- or hypothyroidism, arthritis, or hepatitis [35,50].
Interestingly, Altan et al. demonstrated that T cells infiltrating the pericardium had lower granzyme B expression present, indicating that perhaps cytotoxic granules are not causing pericardial inflammation and damage [25]; instead, this damage may be due to cytokine production. Antibodies are not involved in pathogenesis of this condition [35].
3.4. Takotsubo Cardiomyopathy
Takotsubo cardiomyopathy is a form of stress-induced cardiomyopathy that is an uncommon presentation of ICI-associated cardiotoxicity. Patients often begin having symptoms between 15 weeks and 8 months into treatment [17]. It presents as transient cardiac regional wall motion abnormalities, new ECG changes, and elevated troponin and NT-proBNP [17,26]. Clinicians may also see an apical ballooning pattern on echocardiogram [23].
Takotsubo cardiomyopathy may be caused by a direct effect of ICIs; however, it may also be caused by a sudden release of large amounts of catecholamines [44]. In addition, it may be a result of delayed cardiotoxicity from previous rounds of chemotherapy in patients who have not received ICIs as first line therapy [44]. As this is a relatively uncommon cardiotoxicity, there has not been much research on this presentation to date, and the cause is undetermined in the majority of cases.
3.5. Conduction Diseases
Conduction diseases caused by ICIs can include atrial fibrillation, ventricular tachycardia or fibrillation, and atrioventricular conduction disorders [17]. These diseases may come in conjunction with myocarditis or may appear separately. All conduction diseases are associated with increased mortality [17,18]; they can frequently cause sudden death as well [39]. The most common conduction disorder is atrial fibrillation [22].
It is unknown what causes conduction disease, but local inflammation or fibrosis may play a role. Other hypotheses include an electrolyte imbalance or non-inflammatory left ventricular dysfunction [22]. Lyon et al. argues that systemic inflammation caused by cancer and ICI treatment may also worsen cardiovascular conditions, leading to arrhythmias [44].
3.6. Myocardial Infarction
This extremely rare cardiac complication has been seen in atezolizumab and pembrolizumab treatment. The exact cause of this cardiotoxicity manifestation is unknown, but Chen et al. hypothesize that it may be due to rupture of atherosclerotic plaques seen in chronic inflammatory conditions, coronary spasm, or direct activation of T cells, leading to coronary vasculitis [17]. In addition, a myocardial infarction may be a result of previous cardiac arrhythmias caused by the ICI treatment combined with the hypercoagulability that is seen in patients with advanced cancer.
4. Treatments
4.1. Ipilimumab
Ipilimumab is a fully human recombinant antibody against CTLA-4 [54]. It was initially approved by the FDA in 2011 and is now used for treatment of multiple cancers, including melanoma, renal cell carcinoma, colorectal cancer, hepatocellular carcinoma, and non-small-cell lung cancer [55] (Table 5). There are no contraindications [55].
Because ipilimumab works by stimulating the immune system, patients do not experience common cytotoxic chemotherapy side effects such as bone marrow suppression; instead, immune-related adverse events develop in up to 90% of patients [8]. The most common adverse effects patients experience while taking ipilimumab include fatigue, diarrhea, pruritis, rash, and colitis; severe immune-related reactions include enterocolitis, hepatitis, dermatitis, neuropathy, and endocrinopathy; it is seen in less than 1% of patients [55]. Ipilimumab very rarely causes cardiotoxicity. These IRAEs are dose-dependent and often happen within the first 3 months of the start of treatment [8]. If a patient experiences a severe IRAE, most physicians recommend permanent discontinuation of the drug. For more minor side effects, the drug may be withheld until the patient improves, but afterward, the patient can continue treatment [55,56].
4.2. Pembrolizumab
Pembrolizumab is a humanized IgG4 antibody against PD-1 [57]. This antibody does not trigger antibody-dependent cellular cytotoxicity, unlike normal IgG antibodies [10]. It was initially approved by the FDA in 2014 and is currently approved for treatment of many cancers, including melanoma, lung cancer, several types of squamous cell cancer, several types of lymphomas, urothelial carcinoma, any cancer that is high in microsatellite instability or is mismatch-repair-deficient, gastric and esophageal cancer, cervical cancer, hepatocellular carcinoma, Merkel cell carcinoma, renal cell carcinoma, endometrial carcinoma, tumor mutational burden high cancer, and triple-negative breast cancer (Table 5) [58].
Similar to ipilimumab, pembrolizumab commonly causes immune-related adverse events rather than cytotoxic effects, seen in up to 70% of patients [8]. These events can be severe or even fatal and happen in any body system or organ [58]. The most common adverse events experienced by patients are fatigue, musculoskeletal pain, decreased appetite, diarrhea, rash, fever, cough, constipation, nausea, abdominal pain, and pruritis [58]. Rarely, pembrolizumab can cause cardiotoxicity such as myocarditis and pericarditis, but this occurs in less than 1% of patients [58].
4.3. Nivolumab
Nivolumab is a fully human IgG4 antibody against PD-1 [59]. Similar to pembrolizumab, it does not work in the pathway of antibody-dependent cellular cytotoxicity [10]. It was initially approved by the FDA in 2014 and is now approved for treatment of many cancers, including melanoma, non-small-cell lung cancer, malignant pleural mesothelioma, renal cell carcinoma, classical Hodgkin lymphoma, squamous cell carcinoma of the head and neck, urothelial carcinoma, colorectal cancer, hepatocellular carcinoma, and esophageal squamous cell carcinoma (Table 5) [60].
In patients, nivolumab can cause a number of side effects related to immune cell overactivation, which can be severe. The most common adverse effects seen are fatigue, rash, pruritis, and diarrhea [1]; other common symptoms include musculoskeletal pain, nausea, vomiting, abdominal pain, constipation, cough, dyspnea, asthenia, upper respiratory tract infections, fever, and headache [60]. These IRAEs can develop very late after finishing ICI treatment because a single administration of nivolumab can cause inactivation of PD-1 molecules for almost 3 months [61]. Cardiac adverse effects have been seen in less than 1% of patients [60].
Ipilimumab is often administered with nivolumab for treatment of advanced renal cell carcinoma, microsatellite instability-high or mismatch repair deficient metastatic colon cancer, hepatocellular carcinoma, and metastatic non-small-cell lung cancer (even if PD-L1 expression is less than 1%) [55,62]. However, side effects of this combination can be severe, leading to discontinuation of therapy in up to 40% of patients [46]. Though cardiotoxicity is still rare, combination ipilimumab and nivolumab therapy has a higher incidence of cardiac-adverse effects than either treatment alone [11].
4.4. Atezolizumab
Atezolizumab is a humanized IgG mouse antibody against PD-L1 [63]. It was initially approved by the FDA in 2016 and has since been approved for urothelial carcinoma, non-small-cell lung cancer, triple-negative breast cancer, small-cell lung cancer, hepatocellular carcinoma, and melanoma (Table 5) [64]. The most common reported adverse effects include fatigue, nausea and vomiting, cough, dyspnea, decreased appetite, alopecia, constipation or diarrhea, headache, and rash; the specific side effects vary based on the cancer being treated [64]. Myocarditis or pericarditis are less common side effects occurring in less than 1% of patients; for any grade severity of cardiotoxicity, the drug is recommended to be permanently discontinued [63,64]. To the best of our knowledge, only one case has been reported in the literature about cardiotoxicity using atezolizumab specifically [65]. More case reports may be seen in the future as this drug continues to be used more frequently as a first-line biologic agent.
4.5. Durvalumab
Durvalumab is a fully human IgG antibody against PD-L1 that was initially approved by the FDA in 2017 [66,67]. It is indicated for the treatment of urothelial carcinoma after platinum-containing therapy and non-small-cell lung cancer (Table 5) [66]. The most common side effects reported include fatigue, constipation, urinary tract infections, edema, pneumonitis, dyspnea, rash, cough, and nausea, depending on the patient’s cancer type [66]. More severe side effects include hyperthyroidism or hypothyroidism, colitis, diarrhea, and hepatitis, which can be fatal [67]. With high-grade side effects, the drug may need to be permanently discontinued, but usually the drug only needs to be halted or the dose lowered [67]. Cardiotoxicity for this drug is very rare and has only been reported in three cases by name [19,20,38]. Expanded use of this drug may reveal more significant cardiotoxicity in the future.
5. Antidotes for ICI-Associated Cardiotoxicity
The most frequently recommended treatment for ICI-associated cardiotoxicity is high-dose corticosteroids [68,69]. Especially for myocarditis, higher doses of corticosteroids have been associated with better outcomes for patients [20]. Patel et al. recommend that patients receive 1000 mg/day of corticosteroids initiated within 24 h of presentation; after resolution of symptoms, steroids should be tapered over at least 4–6 weeks [23].
However, there have also been cases of cardiotoxicity that are refractory to steroids. In these cases, Brahmer et al. recommend cardiac transplant rejection medications, including mycophenolate mofetil, infliximab, or anti-thymocyte globulin [68]. However, infliximab cannot be given to patients with heart failure [6]. In addition, other symptom-based treatments are often used, such as anti-coagulants, beta blockers or ACE inhibitors in heart failure, amiodarone with arrhythmias, and pericardiocentesis or pericardial window placement in cardiac tamponade [22]. For pericarditis specifically, Waliany et al. recommend that NSAIDs and colchicine are also effective in treating signs and symptoms [7].
Several studies have recommended that even after minor grade cardiotoxicity, ICIs need to be discontinued temporarily; in high-grade toxicities, they must be permanently discontinued [56]. However, ICIs have a long half-life in the body; therefore, stopping treatment will not immediately reverse the biological effect of the drug [44]. Due to this pharmacological property, steroid treatment often has to be tapered over several weeks to ensure that the patient’s condition does not worsen after halting treatment.
To prevent severe cardiotoxicity in the future, several studies recommend routine cardiac surveillance before starting ICI treatment and within the first 1–4 cycles or up to 12 weeks into treatment [39,44,70]. Lyon et al. recommends testing NT-proBNP, cardiac troponin, and an ECG for this purpose [44]. This surveillance is particularly important in patients with pre-existing cardiac problems [71,72]. In order to carry out this surveillance, baseline cardiac function testing needs to be performed, because patients with preexisting cardiac problems may have high troponin levels due to that disease process rather than ICI cardiotoxicity [73]. Sarocchi et al. report that, during a trial of monitoring troponin levels to predict myocarditis, a few patients developed a small elevation of troponin levels without any symptoms related to this increase; because of this, they postulate that many patients may have subclinical myocarditis [73].
6. Discussion
Cardiotoxicity, though a rare side effect of immune checkpoint inhibitors, is a concerning one due to its high mortality rate and presentation soon after treatment initiation. The most common cardiotoxicity, myocarditis, has by far the highest mortality rate of all cardiotoxicities. However, if they do not progress to become fatal, these cardiotoxicities often resolve quickly with steroid treatment.
There is much variability in the weeks until cardiotoxicity presentation between the type of cardiotoxicity, the specific antibody, and the type of cancer being treated. As shown by the averages and medians in Table 2, Table 3 and Table 4, the bell curve of weeks until presentation of cardiotoxicity is positively skewed. This indicates that though the majority of cases present soon after initiation of ICI treatment, there are several cases that have presented as far as 2 years after initiation of treatment. Based on this information, clinicians must be fully vigilant regarding cardiac toxicity in patients soon after treatment initiation. However, the risk of cardiotoxicity never completely disappears; patients may need to be monitored for suspicious symptoms even years after starting ICI treatment.
Between treatments, ipilimumab appears to be the treatment that presents with cardiotoxicity the latest, and ipilimumab + nivolumab patients present in the shortest time (excluding atezolizumab due to lack of corroborating data). It is unclear why this is the case. However, several studies have stated that the PD-1/PD-L1 pathway specifically is important in preventing cardiac autoimmunity [4,5,46,74], so the CTLA-4 pathway may be less important and thus take longer to cause cardiotoxicity. In addition, a combination of ICIs may cause a faster presentation of immune-related adverse events in general due to more widespread blockage of inhibitory signals.
Within cancer types, there is much variability as well, but there does not appear to be a clear pattern in terms of which cancer presents with cardiotoxicity in a shorter or longer timeframe. Within types of cardiotoxicity, however, clearer trends are seen. Patients who present with a combination of cardiotoxicities frequently present very early into treatment as compared to single cardiotoxicities. In addition, myocarditis tends to present in a shorter time frame than many other cardiotoxicity types. It is unclear why this trend appears. Additional research needs to be done to confirm these trends and investigate why this occurs.
Further research also needs to be done on myocardial infarctions and Takotsubo cardiomyopathy in patients taking immune checkpoint inhibitors. These presentations are uncommon but can be fatal, and the timing, histopathological findings, and symptoms of patients with these conditions due to ICI treatment is poorly understood. In addition, very few case reports were found for patients with cardiotoxicity taking durvalumab or atezolizumab; as these drugs become more widely used, investigations into the likelihood of cardiotoxicity with these antibodies need to be carried out.
7. Conclusions
Immune checkpoint inhibitors may cause several immune-related side effects; one rare side effect is cardiac toxicity, including myocarditis, pericarditis, Takotsubo cardiomyopathy, arrhythmias, and/or myocardial infarction. Though these side effects are rare, they have a high mortality rate; it is important to be aware of the common symptoms and lab results associated with them while treating patients. The best way to treat any cardiac toxicity is usually high doses of steroids; other symptomatic treatments may also be warranted.
Author Contributions
Conceptualization, R.S., A.A.-s. and W.S.; methodology, R.S., A.A.-s., I.M. and W.S.; software, R.S. and B.M.J.; validation, R.S., B.M.J., I.M., A.A.-s. and W.S.; formal analysis, R.S. and W.S.; investigation, R.S., A.A.-s. and W.S.; resources, R.S., B.M.J. and W.S.; data curation, R.S. and W.S.; writing—original draft preparation, R.S., A.Y. and W.S.; writing—review and editing, B.M.J. and W.S.; visualization, R.S., B.M.J., A.A.-s., I.M., A.Y. and W.S.; supervision, W.S.; project administration, W.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ICI | Immune checkpoint inhibitor |
| IRAE | Immune-related adverse event |
| MACE | Major adverse cardiac event |
| CMR | Cardiovascular magnetic resonance imaging |
| NSCLC | Non-small-cell lung cancer |
Appendix A

{kind=link}
{kind=link}
Table A1.
Patients with a wide range of signs and symptoms, from asymptomatic to severe chest pain, dyspnea, multiorgan failure, and sudden death.
Table A1.
Patients with a wide range of signs and symptoms, from asymptomatic to severe chest pain, dyspnea, multiorgan failure, and sudden death.
| Study | Sex | Age | Type of Cancer | Cancer Treatment | Type of Cardiotoxicity | Weeks until Presentation | Complaint at Presentation | Antidote |
|---|---|---|---|---|---|---|---|---|
| [38] | M | 76 | Lung cancer | Durvalumab | Myocarditis | 8 weeks | NR | Prednisone |
| [38] | F | 67 | Renal cell carcinoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Dyspnea | Dexamethasone |
| [38] | M | 82 | Urothelial carcinoma | Pembrolizumab | Myocarditis | 15 weeks | Chest pain and dyspnea | Methylprednisone and prednisone |
| [19] | M | 70 | Lung cancer | Nivolumab | Acute pericarditis and pericardial effusion | 13 weeks | Pleuritic chest pain | Prednisone |
| [19] | F | 60 | Lung cancer | Nivolumab and THU-decitabine | Acute pericarditis and pericardial effusion | 9 weeks | Pleuritic chest pain, shortness of breath, productive cough | Colchicine and ibuprofen |
| [19] | M | 58 | Non-small cell lung cancer | Nivolumab | Pericardial effusion | 10 weeks | Shortness of breath | Prednisone |
| [19] | M | 60 | Melanoma | Ipilimumab + nivolumab, then nivolumab | Cardiomyopathy | 22 weeks | Chest tightness, decreased exercise tolerance | Prednisone |
| [19] | F | 84 | Lung cancer | Pembrolizumab | Cardiomyopathy | 7 weeks | Shortness of breath | Heart failure treatment |
| [19] | F | 71 | Lung cancer | Durvalumab | Cardiomyopathy and pericardial effusion | 22 weeks | Abdominal pain, shortness of breath on exertion | Prednisone |
| [19] | M | 67 | Melanoma | Ipilimumab | Cardiomyopathy | 17 weeks | Intermittent chest discomfort, shortness of breath on exertion | Carvedilol |
| [19] | F | 80 | Cutaneous squamous cell carcinoma | Pembrolizumab | Myocarditis | 7 weeks | Bilateral eye ptosis, generalized weakness and fatigue | Prednisone |
| [19] | M | 80 | Prostate cancer | Pembrolizumab | Myocarditis | 4 weeks | Right eye ptosis, generalized weakness and fatigue | Prednisone |
| [75] | M | 75 | Myelodysplastic syndrome | Ipilimumab + nivolumab + azacitidine | Pericardial effusion and pleural effusion | 7 weeks | Fever, cough, dyspnea, rash | IVIG, rosuvastatin |
| [75] | M | 78 | Myelodysplastic syndrome | Ipilimumab and azacitidine | Perimyocarditis | 1 week | Fever and pneumonia | IVIG, colchicine, atorvastatin |
| [75] | F | 74 | Melanoma | Ipilimumab and evofosfamide | Paroxysmal atrial fibrillation, sinus tachycardia, myocarditis | 4 weeks | Dyspnea, fever, hypotension, rash | IVIG, colchicine, rosuvastatin, hydroxychloroquine |
| [52] | M | 62 | Hepatocellular carcinoma | Nivolumab | Perimyocarditis, takotsubo syndrome, myocardial infarction | 3 weeks | Chest pain, nausea, and vomiting | Methylprednisolone, prednisone, broad spectrum antibiotics |
| [49] | M | 58 | Non-small cell lung cancer | Nivolumab | Pericarditis | 78 weeks | limb edema | Methylprednisolone, prednisolone, infliximab |
| [76] | F | 58 | Lung cancer | Nivolumab | Pericarditis | 12 weeks | dyspnea and cough | Pericardiocentesis and corticosteroids |
| [76] | M | 65 | Lung cancer | Nivolumab | Pericarditis | 106 weeks | Acute respiratory failure | Corticosteroids and pericardiocentesis |
| [74] | F | 78 | Melanoma | Pembrolizumab | Myocarditis | 6 weeks | Chest pain | Prednisone |
| [74] | F | 55 | Melanoma | Nivolumab, then ipilimumab + nivolumab | Myocarditis | 4 weeks after ipilimumab + nivolumab | Chest pain, fever, and dyspnea | |
| [77] | F | 52 | Non-small cell lung cancer | Ipilimumab + nivolumab | Myocarditis and acute heart failure | 52 weeks | Dyspnea on exertion, chest pain, and lower extremity edema | Methylprednisolone |
| [78] | M | 62 | Lung cancer | Pembrolizumab | Pericarditis | 15 weeks | Shortness of breath | Pericardial window and prednisone |
| [79] | M | 62 | Lung cancer | Nivolumab | Cardiac tamponade | 1 week | Dyspnea | Pericardiocentesis |
| [80] | F | 66 | Lung cancer | Pembrolizumab | Pericardial effusion | 1 week | NR | Pericardiocentesis and prednisone |
| [81] | M | 68 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 6 weeks | Dyspnea, irregular heartbeats, tachycardia | Prednisone and solumedrol |
| [82] | F | 66 | Lung cancer | Nivolumab | Myocarditis | 9 weeks | Chest pain | Methylprednisolone, plasmapheresis, abatacept |
| [83] | F | 71 | Melanoma | Pembrolizumab | Myocarditis and cardiac arrhythmia | 6 weeks | Dyspnea | Methylprednisolone, mycophenolate mofetil, plasmapheresis, rituximab, alemtuzumab |
| [84] | F | 79 | Lung cancer | Pembrolizumab | Pericarditis | 9 weeks | Chest pain | Pyridostigmine and methylprednisolone |
| [25] | M | 72 | Lung cancer | anti-PD-L1 | Pericarditis | 11 weeks | Dyspnea, hypotension, hypoxia | NR |
| [25] | F | 65 | Lung cancer | anti-CTLA-4 and anti-PD-1 | Arrhythmias | 19 weeks | Loss of consciousness and hypotension | Pacemaker |
| [25] | M | 57 | Lung cancer | anti-PD-L1 | Cardiac tamponade | 14 weeks | Dyspnea, orthopnea, bilateral lower extremity edema | NR |
| [85] | M | 80 | Kidney cancer | Nivolumab | Myocarditis and atrial fibrillation | 12 weeks | Severe asthenia | Methylprednisolone |
| [86] | F | 78 | Melanoma | Nivolumab | Myocarditis | 4 weeks | Muscle weakness and dyspnea | Methylprednisolone to pulse steroid |
| [65] | F | 61 | Lung cancer | Atezolizumab | Myocarditis | Less than 1 week | Dyspnea, fatigue | Methylprednisolone and mycophenolate mofetil |
| [87] | F | 55 | Melanoma | Nivolumab | Myocarditis | 6 weeks | Dysphagia, dyspnea, limb weakness | IGI, steroid pulse, plasma exchange |
| [88] | M | 74 | Lung cancer | Nivolumab | Myocardial necrosis | 6 weeks | General malaise, appetite decrease, dyspnea | Catecholamines |
| [89] | F | 76 | T cell lymphoma | Brentuximab and nivolumab | Acute heart failure | 3 weeks | Fatigue, dyspnea, orthopnea | Solumedrol, Impella implant |
| [90] | M | 33 | Hodgkin lymphoma | Nivolumab | Complete heart block, myocarditis | 24 weeks | NR | Mycophenolate mofetil and steroids |
| [91] | M | 73 | Malignant mesothelioma | Pembrolizumab | Myocarditis | 5 weeks | Progressive dyspnea and fatigue | Prednisolone, pacemaker, IGI, and plasmapheresis |
| [91] | M | 89 | Melanoma | Pembrolizumab | Myocarditis | 3 weeks | Weakness, myalgias, and dyspnea | Methylprednisolone, oral prednisone, anti-thymocyte globulin |
| [91] | F | 65 | Lung cancer | Nivolumab | Acute coronary syndrome, acute decompensated heart failure | 1 week | Dyspnea, edema, bradycardia | Methylprednisolone, prednisone, furosemide, anti-thymocyte globulin |
| [91] | M | 67 | Melanoma | Nivolumab | Myocarditis | 9 weeks | Chest pain and palpitations | prednisone, infliximab, oral corticosteroids |
| [92] | M | 42 | Hepatocellular carcinoma | Pembrolizumab | Bradycardia | 18 weeks | Fatigue, dizziness, and anorexia | Cortisone |
| [93] | F | 47 | Melanoma | Ipilimumab + nivolumab, then nivolumab | Heart failure, asymptomatic supraventricular tachycardia | 17 weeks | Dyspnea, tachycardia, and pulmonary edema | Methylprednisolone and infliximab |
| [76] | F | 58 | Lung cancer | Nivolumab | Pericardial effusion | 12 weeks | Dyspnea and cough | Pericardiocentesis and steroids |
| [76] | M | 65 | Lung cancer | Nivolumab | Pericardial effusion | 106 weeks | Acute respiratory failure and fever | Surgical drainage and steroids |
| [94] | M | 70 | Lung cancer | Pembrolizumab | Cardiac tamponade | 9 weeks | Dyspnea and general fatigue | Pericardiocentesis |
| [95] | M | 65 | Lung cancer | Nivolumab | Cardiac tamponade | 8 weeks | Dyspnea | Pericardiocentesis |
| [95] | M | 71 | Lung cancer | Nivolumab | Cardiac tamponade | 6 weeks | Chest pain and dyspnea | Pericardiocentesis |
| [76] | F | 55 | Lung cancer | Nivolumab | Pericardial effusion | 9 weeks | None | None |
| [96] | M | 71 | Lung cancer | Nivolumab | Pericardial effusion | 5 weeks | NR | Pericardiocentesis and pericardial window |
| [97] | M | 79 | Prostate cancer | Nivolumab | Myocarditis | 8 weeks | Blurred vision, pain and stiffness in the upper back | Methylprednisolone, oral prednisone taper |
| [98] | F | 70 | Lung cancer | Nivolumab | Pericardial effusion | Less than 1 week | Chest pain and shortness of breath | Colchicine and prednisone |
| [99] | M | 74 | Lung cancer | Pembrolizumab | Myocarditis and arrhythmia | 8 weeks | Dyspnea on exertion | Prednisone, aspirin, clopidogrel, IV heparin, metoprolol succinate |
| [69] | M | 77 | Melanoma | Ipilimumab | Myocarditis | NR | Malaise, nausea, cough, bradycardia | Methylprednisolone |
| [33] | F | 67 | Multiple myeloma | Pembrolizumab | Myocarditis | 2 weeks | Dyspnea and malaise | Methylprednisolone |
| [100] | M | 52 | Renal cell carcinoma | Ipilimumab + nivolumab | Myocarditis | 6 weeks | None | Beta blocker therapy |
| [101] | M | 67 | Melanoma | Ipilimumab + nivolumab | Acute decompensated heart failure, arrhythmia, chronic heart failure | 2 weeks | Dyspnea and cough | Methylprednisolone, anti-thymocyte globulin, and permanent pacemaker implantation |
| [50] | M | 69 | Lung cancer | Nivolumab | Pericarditis, pericardial tamponade | 73 weeks | Dyspnea, tachycardia, and fever | Prednisone |
| [102] | F | 45 | Melanoma | Ipilimumab + nivolumab | Acute heart failure, Takotsubo-like syndrome | Less than 1 week | NR | Methylprednisolone |
| [102] | M | 77 | Melanoma | Ipilimumab, nivolumab | Takotsubo-like syndrome | 6 weeks | NR | Methylprednisolone |
| [21] | F | 41 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 9 weeks | Dyspnea | Methylprednisolone |
| [103] | M | 60 | Melanoma | Nivolumab | Myocarditis | 39 weeks | Fatigue and fever | Prednisolone, IGI |
| [20] | F | 75 | Extraskeletal myxoid carcinoma | Durvalumab and tremelimumab | Myocarditis, heart failure, complete heart block | 3 weeks | Difficulty ambulating and dyspnea | Methylprednisolone, mycophenolate mofetil |
| [104] | F | 55 | Breast cancer | Pembrolizumab | Pericardial tamponade | 15 weeks | Pericardial chest pain | Anterior pericardectomy, corticosteroids |
| [105] | F | 76 | Lung cancer | Nivolumab | Myocarditis, complete atrioventricular block | 3 weeks | Dyspnea | Methylprednisolone and infliximab |
| [106] | M | 72 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 20 weeks | Dyspnea, leg edema | Prednisolone |
| [107] | M | 73 | Lung cancer | Pembrolizumab | Complete atrioventricular block and myocarditis | 2 weeks | Faintness | Methylprednisolone and temporary pacemaker implantation |
| [108] | M | 43 | Thymoma | Nivolumab | Myocarditis | 1 week | Chest discomfort, fatigue, lower limb myalgias | IGI, methylprednisolone |
| [109] | M | 55 | Lung cancer | Nivolumab | Acute decompensated right-sided heart failure and cardiogenic shock | 1 week | Lethargy and dyspnea | NR |
| [110] | F | 49 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Atypical chest discomfort at the cardiac apex | Methylprednisolone and IGI |
| [111] | F | 35 | Melanoma | Ipilimumab | Myocarditis | 2 weeks | Progressive dyspnea | Methylprednisolone, IGI, plasma exchanges |
| [112] | M | 61 | Lung cancer | Nivolumab | Acute coronary syndrome | 33 weeks | NR | Corticosteroids |
| [113] | M | 60 | Lung cancer | Nivolumab | Pericarditis | 17 weeks | NR | Pericardiocentesis and methylprednisolone |
| [114] | M | 68 | Histiocytosis and left buttock sarcoma | Anti-PD-L1 and anti-CTLA-4 (unspecified) | Myocarditis and arrhythmia | 2 weeks | Fatigue, general malaise, weakness | Steroids, mycophenolate mofetil, temporary transvenous pacing wire followed by a permanent pacemaker |
| [115] | M | 54 | Lung cancer | Nivolumab | Heart failure | 4 weeks | Dizziness, nausea, loss of consciousness, general paralysis | High dose steroids and a pacemaker |
| [116] | M | 63 | Melanoma | Nivolumab | Atrioventricular block, myocardial infarction | 3 weeks | Dyspnea, dysphagia, worsened muscle pain | Prednisone and antibiotic therapy (sultamicillin), aspirin, and unfractionated heparin |
| [117] | M | 59 | Lung cancer | Nivolumab | Cardiac tamponade | 9 weeks | NR | Pericardiocentesis, prednisone, and anti-tubercular treatment |
| [118] | M | 67 | Lung cancer | Nivolumab | Cardiac tamponade | 15 weeks | Acute respiratory failure | Pericardiocentesis and prednisone |
| [35] | F | 65 | Melanoma | Ipilimumab | Cardiac tamponade | 38 weeks | Shortness of breath and chest discomfort | Pericardiocentesis and methylprednisolone |
| [119] | M | 46 | Small cell lung cancer | Nivolumab | Cardiac tamponade | 9 weeks | NR | Pericardiocentesis |
| [119] | F | 54 | Lung cancer | Nivolumab | Cardiac tamponade | 7 weeks | NR | Pericardiocentesis and prednisone |
| [11] | F | 65 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Atypical chest pain, dyspnea, fatigue | Methylprednisolone |
| [11] | M | 63 | Melanoma | Ipilimumab + nivolumab | Myocarditis | 2 weeks | Fatigue and myalgias | Methylprednisolone and infliximab |
| [120] | M | 60 | Melanoma | Ipilimumab | Atrial fibrillation | 104 weeks | None | Lisinopril, metoprolol changed to carvedilol |
| [121] | F | 68 | Melanoma | Ipilimumab and nivolumab | Myocarditis | 2 weeks | Right eye ptosis, generalized weakness and fatigue | Steroids |
| [122] | M | 73 | Melanoma | Ipilimumab and nivolumab followed by pembrolizumab | Myocarditis with cardiomyopathy and ventricular arrhythmia | 2 weeks after starting pembrolizumab | NR | Prednisolone |
| [122] | M | 87 | Melanoma | Nivolumab | Asystole | 17 weeks | Cardiac arrest | Prednisolone |
| [122] | M | 77 | Melanoma | Ipilimumab followed by penbrolizumab | Stable angina pectoris | 10 weeks | Stable angina pectoris | None |
| [123] | F | 69 | Melanoma | Nivolumab | Myocarditis | 9 weeks | General malaise and palpitations | Prednisolone |
| [26] | M | 72 | Melanoma | Ipilimumab | Myocarditis | 9 weeks | Dyspnea and anasarca | Corticosteroids |
| [26] | M | 68 | Melanoma | Ipilimumab | Cardiomyopathy | 12 weeks | Dyspnea and lower extremity edema | Diuresis and coronary catheterization |
| [26] | M | 71 | Melanoma | Ipilimumab | Myocardial fibrosis | 6 weeks | No obvious cardiac symptoms | High dose steroids |
| [26] | M | 81 | Melanoma | Ipilimumab | Heart failure, myocarditis | 20 weeks | Progressive subacute dyspnea | Diuretics |
| [26] | M | 23 | Melanoma | Ipilimumab | Myocarditis and heart failure | 30 weeks | Chest pain and cough | Methylprednisolone converted to prednisone |
| [26] | M | 64 | Melanoma | Ipilimumab | Myocarditis | 6 weeks | Fatigue, seizures, and abdominal pain (Yun et al. 2015) | Dopamine and fentanyl |
| [26] | M | 88 | Melanoma | Pembrolizumab | Cardiac arrest | 24 weeks | Myalgia and pain in the shoulder | Corticosteroids |
| [26] | M | 80 | Non-Hodgkin lymphoma | Ipilimumab | Myocarditis | 8 weeks | Dyspnea, edema, and arrhythmia | Methylprednisolone and prednisone |
| [124] | M | 64 | Lung cancer | Nivolumab | Cardiac tamponade | 13 weeks | Pericardial chest pain | Pericardiocentesis and pericardial window |
| [125] | M | 75 | Lung cancer | Nivolumab | Myocarditis | 18 weeks | Acute dyspnea and chest pain | Prednisolone, ACE inhibitor, beta blocker, diuretic therapy |
| [126] | F | 68 | Lung cancer | Nivolumab | Myocarditis and arrhythmia | 3 weeks | Altered mental status, nausea, and vomiting | Methylprednisolone and amiodarone IV |
| [127] | F | 83 | Melanoma | Ipilimumab | Takotsubo cardiomyopathy | 15 weeks | Substernal chest pain and dyspnea | Beta blocker therapy |
| [42] | F | 73 | Melanoma | Pembrolizumab | Acute heart failure | 15 weeks | Progressive dyspnea | AT-2 receptor blocker, beta blocker, spironolactone, and diuretics |
| [128] | M | 59 | Melanoma | Ipilimumab | Acute fibrinous pericarditis | 24 weeks | Chest pain and dyspnea | Methylprednisolone, prednisone, budesonide |
References
- Varricchi, G.; Galdiero, M.R.; Marone, G.; Criscuolo, G.; Triassi, M.; Bonaduce, D.; Marone, G.; Tocchetti, C.G. Cardiotoxicity of immune checkpoint inhibitors. ESMO Open 2017, 2, e000247. Available online: https://pubmed.ncbi.nlm.nih.gov/29104763/ (accessed on 5 July 2021).
- Zhang, B.; Rocci, M.L.; Twomey, J.D. Theme: Identification and Implementation of Predictive Biomarkers for Checkpoint Targeted Immunotherapy Cancer Immunotherapy Update: FDA-Approved Checkpoint Inhibitors and Companion Diagnostics. AAPS J. 2021, 23, 39. [Google Scholar]
- Rowshanravan, B.; Halliday, N.; Sansom, D.M. CTLA-4: A moving target in immunotherapy. Blood Am. Soc. Hematol. 2018, 131, 58–67. Available online: http://ashpublications.org/blood/article-pdf/131/1/58/1367947/blood741033.pdf (accessed on 30 June 2021). [CrossRef]
- Qin, W.; Hu, L.; Zhang, X.; Jiang, S.; Li, J.; Zhang, Z.; Wang, X. The Diverse Function of PD-1/PD-L Pathway Beyond Cancer. Front. Immunol. 2019, 10, 2298. [Google Scholar] [CrossRef]
- Tarrio, M.L.; Grabie, N.; Bu, D.-X.; Sharpe, A.H.; Lichtman, A.H. PD-1 Protects against Inflammation and Myocyte Damage in T Cell-Mediated Myocarditis. J. Immunol. 2012, 188, 4876–4884. Available online: https://pubmed.ncbi.nlm.nih.gov/22491251/ (accessed on 27 June 2021).
- Zhang, L.; Reynolds, K.L.; Lyon, A.R.; Palaskas, N.; Neilan, T.G. The Evolving Immunotherapy Landscape and the Epidemiology, Diagnosis, and Management of Cardiotoxicity. JACC CardioOncol. 2021, 3, 35–47. [Google Scholar] [CrossRef]
- Waliany, S.; Lee, D.; Witteles, R.M.; Neal, J.W.; Nguyen, P.; Davis, M.M.; Salem, J.-E.; Wu, S.M.; Moslehi, J.J.; Zhu, H. Immune Checkpoint Inhibitor Cardiotoxicity: Understanding Basic Mechanisms and Clinical Characteristics and Finding a Cure. Annu. Rev. Pharmacol. Toxicol. 2021, 61, 113–134. [Google Scholar] [CrossRef]
- Michot, J.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel-Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur. J. Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef]
- Cathcart-Rake, E.J.; Sangaralingham, L.R.; Henk, H.J.; Shah, N.D.; bin Riaz, I.; Mansfield, A.S. A Population-based Study of Immunotherapy-related Toxicities in Lung Cancer. Clin. Lung Cancer 2020, 21, 421–427.e2. [Google Scholar] [CrossRef]
- Puzanov, I.; on behalf of the Society for Immunotherapy of Cancer Toxicity Management Working Group; Diab, A.; Abdallah, K.; Bingham, C.O.; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; et al. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5, 95. Available online: https://pubmed.ncbi.nlm.nih.gov/29162153/ (accessed on 20 June 2021).
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. Available online: https://pubmed.ncbi.nlm.nih.gov/27806233/ (accessed on 20 June 2021).
- Rubio-Infante, N.; Ramírez-Flores, Y.A.; Castillo, E.C.; Lozano, O.; García-Rivas, G.; Torre-Amione, G. Cardiotoxicity associated with immune checkpoint inhibitor therapy: A meta-analysis. Eur. J. Heart Fail. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34196077/ (accessed on 31 June 2021).
- D’Souza, M.; Nielsen, D.; Svane, I.M.; Iversen, K.; Rasmussen, P.V.; Madelaire, C.; Fosbøl, E.; Køber, L.; Gustafsson, F.; Andersson, C.; et al. The risk of cardiac events in patients receiving immune checkpoint inhibitors: A nationwide Danish study. Eur. Heart J. 2021, 42, 1621–1631. Available online: https://pubmed.ncbi.nlm.nih.gov/33291147/ (accessed on 31 June 2021).
- Totzeck, M.; Lutgens, E.; Neilan, T.G. Are we underestimating the potential for cardiotoxicity related to immune checkpoint inhibitors? Eur. Heart J. 2021, 42, 1632–1635. Available online: https://pubmed.ncbi.nlm.nih.gov/33291139/ (accessed on 31 June 2021).
- Michel, L.; Rassaf, T.; Totzeck, M. Cardiotoxicity from immune checkpoint inhibitors. IJC Heart Vasc. 2019, 25, 100420. [Google Scholar] [CrossRef]
- Hu, J.R.; Florido, R.; Lipson, E.J.; Naidoo, J.; Ardehali, R.; Tocchetti, C.G.; Lyon, A.R.; Padera, R.F.; Johnson, D.B.; Moslehi, J. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc. Res. 2019, 115, 854–868. Available online: https://pubmed.ncbi.nlm.nih.gov/30715219/ (accessed on 5 June 2021).
- Chen, D.-Y.; Huang, W.-K.; Wu, V.C.-C.; Chang, W.-C.; Chen, J.-S.; Chuang, C.-K.; Chu, P.-H. Cardiovascular toxicity of immune checkpoint inhibitors in cancer patients: A review when cardiology meets immuno-oncology. J. Formos. Med. Assoc. 2020, 119, 1461–1475. [Google Scholar] [CrossRef]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.J.; Scemama, U.; Jacquier, A.; et al. Clinical features, management, and outcomes of immune checkpoint inhibitor-related cardiotoxicity. Circulation 2017, 136, 2085–2087. Available online: https://pubmed.ncbi.nlm.nih.gov/29158217/ (accessed on 27 June 2021).
- Chahine, J.; Collier, P.; Maroo, A.; Tang, W.W.; Klein, A.L. Myocardial and Pericardial Toxicity Associated With Immune Checkpoint Inhibitors in Cancer Patients. JACC Case Rep. 2020, 2, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.v.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated With Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. Available online: https://pubmed.ncbi.nlm.nih.gov/29567210/ (accessed on 27 June 2021).
- Ganatra, S.; Neilan, T.G. Immune Checkpoint Inhibitor-Associated Myocarditis. Oncologist 2018, 23, 879–886. Available online: https://pubmed.ncbi.nlm.nih.gov/29802219/ (accessed on 5 June 2021).
- Sławiński, G.; Wrona, A.; Dabrowska-Kugacka, A.; Raczak, G.; Lewicka, E. Immune checkpoint inhibitors and cardiac toxicity in patients treated for non-small lung cancer: A review. Int. J. Mol. Sci. 2020, 21, 1–19. Available online: https://pubmed.ncbi.nlm.nih.gov/33003425/ (accessed on 5 June 2021).
- Patel, R.P.; Parikh, R.; Gunturu, K.S.; Tariq, R.Z.; Dani, S.S.; Ganatra, S.; Nohria, A. Cardiotoxicity of Immune Checkpoint Inhibitors. Curr. Oncol. Rep. 2021, 23. Available online: https://pubmed.ncbi.nlm.nih.gov/33937956/ (accessed on 5 June 2021).
- Lobenwein, D.; Kocher, F.; Dobner, S.; Gollmann-Tepeköylü, C.; Holfeld, J. Cardiotoxic mechanisms of cancer immunotherapy—A systematic review. Int. J. Cardiol. 2021, 323, 179–187. [Google Scholar] [CrossRef]
- Altan, M.; Toki, M.; Gettinger, S.N.; Carvajal-Hausdorf, D.E.; Zugazagoitia, J.; Sinard, J.H.; Herbst, R.S.; Rimm, D.L. Immune Checkpoint Inhibitor–Associated Pericarditis. J. Thorac. Oncol. 2019, 14, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Heinzerling, L.; Ott, P.A.; Hodi, F.S.; Husain, A.N.; Tajmir-Riahi, A.; Tawbi, H.; Pauschinger, M.; Gajewski, T.F.; Lipson, E.J.; Luke, J.J. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J. Immunother. Cancer 2016, 4, 50. Available online: https://pubmed.ncbi.nlm.nih.gov/27532025/ (accessed on 5 June 2021).
- Zhou, Y.-W.; Zhu, Y.-J.; Wang, M.-N.; Xie, Y.; Chen, C.-Y.; Zhang, T.; Xia, F.; Ding, Z.-Y.; Liu, J.-Y. Immune Checkpoint Inhibitor-Associated Cardiotoxicity: Current Understanding on Its Mechanism, Diagnosis and Management. Front. Pharmacol. 2019, 10, 1350. [Google Scholar] [CrossRef]
- Baik, A.H.; Oluwole, O.O.; Johnson, D.B.; Shah, N.; Salem, J.-E.; Tsai, K.K.; Moslehi, J.J. Mechanisms of Cardiovascular Toxicities Associated With Immunotherapies. Circ. Res. 2021, 128, 1780–1801. Available online: https://pubmed.ncbi.nlm.nih.gov/33934609/ (accessed on 31 June 2021).
- Tay, W.T.; Fang, Y.-H.; Beh, S.T.; Liu, Y.-W.; Hsu, L.-W.; Yen, C.-J.; Liu, P.-Y. Programmed Cell Death-1: Programmed Cell Death-Ligand 1 Interaction Protects Human Cardiomyocytes Against T-Cell Mediated Inflammation and Apoptosis Response In Vitro. Int. J. Mol. Sci. 2020, 21, 2399. Available online: https://pubmed.ncbi.nlm.nih.gov/32244307/ (accessed on 20 June 2021).
- Quagliariello, V.; Passariello, M.; Rea, D.; Barbieri, A.; Iovine, M.; Bonelli, A.; Caronna, A.; Botti, G.; De Lorenzo, C.; Maurea, N. Evidences of CTLA-4 and PD-1 Blocking Agents-Induced Cardiotoxicity in Cellular and Preclinical Models. J. Pers. Med. 2020, 10, 1–19. Available online: https://pubmed.ncbi.nlm.nih.gov/33086484/ (accessed on 31 June 2021).
- Wang, J.; Okazaki, I.-M.; Yoshida, T.; Chikuma, S.; Kato, Y.; Nakaki, F.; Hiai, H.; Honjo, T.; Okazaki, T. PD-1 deficiency results in the development of fatal myocarditis in MRL mice. Int. Immunol. 2010, 22, 443–452. Available online: https://pubmed.ncbi.nlm.nih.gov/20410257/ (accessed on 20 June 2021).
- Love, V.A.; Grabie, N.; Duramad, P.; Stavrakis, G.; Sharpe, A.; Lichtman, A. CTLA-4 ablation and interleukin-12-driven differentiation synergistically augment cardiac pathogenicity of cytotoxic T lymphocytes. Circ. Res. 2007, 101, 248–257. Available online: https://pubmed.ncbi.nlm.nih.gov/17569889/ (accessed on 27 June 2021).
- Martinez-Calle, N.; Rodriguez-Otero, P.; Villar, S.; Mejías, L.; Melero, I.; Prosper, F.; Marinello, P.; Paiva, B.; Idoate-Gastearena, M.; Miguel, J.S. Anti-PD1 associated fulminant myocarditis after a single pembrolizumab dose: The role of occult pre-existing autoimmunity. Haematologica 2018, 103, e318–e321. Available online: https://europepmc.org/articles/PMC6029537 (accessed on 8 June 2021). [CrossRef]
- Xu, S.; Sharma, U.C.; Tuttle, C.; Pokharel, S. Immune Checkpoint Inhibitors: Cardiotoxicity in Pre-clinical Models and Clinical Studies. Front. Cardiovasc. Med. 2021, 8, 619650. [Google Scholar] [CrossRef]
- Dasanu, C.A.; Jen, T.; Skulski, R. Late-onset pericardial tamponade, bilateral pleural effusions and recurrent immune monoarthritis induced by ipilimumab use for metastatic melanoma. J. Oncol. Pharm. Pract. 2017, 23, 231–234. [Google Scholar] [CrossRef]
- Moslehi, J.J.; Salem, J.E.; Sosman, J.A.; Lebrun-Vignes, B.; Johnson, D.B. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet 2018, 391, 933. Available online: https://pubmed.ncbi.nlm.nih.gov/29536852/ (accessed on 27 June 2021).
- Palaskas, N.; Lopez-Mattei, J.; Durand, J.B.; Iliescu, C.; Deswal, A. Immune Checkpoint Inhibitor Myocarditis: Pathophysiological Characteristics, Diagnosis, and Treatment. J. Am. Hear. Assoc. 2020, 9, e013757. [Google Scholar] [CrossRef] [PubMed]
- Waliany, S.; Neal, J.W.; Reddy, S.; Wakelee, H.; Shah, S.A.; Srinivas, S.; Padda, S.K.; Fan, A.C.; Colevas, A.D.; Wu, S.M.; et al. Myocarditis Surveillance With High-Sensitivity Troponin I During Cancer Treatment With Immune Checkpoint Inhibitors. JACC CardioOncol. 2021, 3, 137–139. Available online: https://pubmed.ncbi.nlm.nih.gov/33796869/ (accessed on 31 June 2021).
- Pirozzi, F.; Poto, R.; Aran, L.; Cuomo, A.; Galdiero, M.R.; Spadaro, G.; Abete, P.; Bonaduce, D.; Marone, G.; Tocchetti, C.G.; et al. Cardiovascular Toxicity of Immune Checkpoint Inhibitors: Clinical Risk Factors. Curr. Oncol. Rep. 2021, 23, 13. Available online: https://pubmed.ncbi.nlm.nih.gov/33415405/ (accessed on 5 June 2021).
- Balanescu, D.V.; Donisan, T.; Palaskas, N.L.; Iliescu, C. Emerging Concerns in Cardio-Oncology: Immune Checkpoint Inhibitor Cardiotoxicity. Am. Coll. Cardiol. 2019. Available online: https://www.acc.org/latest-in-cardiology/articles/2019/06/21/08/45/emerging-concerns-in-cardio-oncology (accessed on 30 June 2021).
- Wang, D.Y.; Okoye, G.; Neilan, T.G.; Johnson, D.B.; Moslehi, J.J. Cardiovascular Toxicities Associated with Cancer Immunotherapies. Curr. Cardiol. Rep. 2017, 19, 21. [Google Scholar] [CrossRef]
- Läubli, H.; Balmelli, C.; Bossard, M.; Pfister, O.; Glatz, K.; Zippelius, A. Acute heart failure due to autoimmune myocarditis under pembrolizumab treatment for metastatic melanoma. J. Immunother. Cancer 2015, 3, 11. Available online: https://pubmed.ncbi.nlm.nih.gov/25901283/ (accessed on 20 June 2021).
- Lal, J.C.; Brown, S.-A.; Collier, P.; Cheng, F. A retrospective analysis of cardiovascular adverse events associated with immune checkpoint inhibitors. Cardio-Oncology 2021, 7, 1–10. Available online: https://pubmed.ncbi.nlm.nih.gov/34049595/ (accessed on 5 June 2021).
- Lyon, A.R.; Yousaf, N.; Battisti, N.M.L.; Moslehi, J.; Larkin, J. Immune checkpoint inhibitors and cardiovascular toxicity. Lancet Oncol. 2018, 19, e447–e458. [Google Scholar] [CrossRef]
- Awadalla, M.; Golden, D.L.A.; Mahmood, S.S.; Alvi, R.M.; Mercaldo, N.D.; Hassan, M.; Banerji, D.; Rokicki, A.; Mulligan, C.; Murphy, S.P.T.; et al. Influenza vaccination and myocarditis among patients receiving immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 53. Available online: https://jitc.bmj.com/lookup/doi/10.1186/s40425-019-0535-y (accessed on 27 June 2021). [CrossRef]
- Varricchi, G.; Galdiero, M.R.; Tocchetti, C.G. Cardiac toxicity of immune checkpoint inhibitors: Cardio-oncology meets immunology. Circulation 2017, 136, 1989–1992. Available online: http://ahajournals.org (accessed on 30 June 2021). [CrossRef] [PubMed]
- Gong, J.; Drobni, Z.D.; Zafar, A.; Quinaglia, T.; Hartmann, S.; Gilman, H.K.; Raghu, V.K.; Gongora, C.E.; Sise, M.; Alvi, R.M.; et al. Pericardial disease in patients treated with immune checkpoint inhibitors. J. Immunother. Cancer 2021, 9, e002771. Available online: https://pubmed.ncbi.nlm.nih.gov/34145031/ (accessed on 5 June 2021).
- Salem, J.E.; Manouchehri, A.; Moey, M.; Lebrun-Vignes, B.; Bastarche, L.; Pariente, A.; Gobert, A.; Spano, J.-P.; Balko, J.M.; Bonaca, M.P.; et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: An observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018, 19, 1579–1589. Available online: https://pubmed.ncbi.nlm.nih.gov/30442497/ (accessed on 8 June 2021). [CrossRef]
- Moriyama, S.; Fukata, M.; Tatsumoto, R.; Kono, M. Refractory constrictive pericarditis caused by an immune checkpoint inhibitor properly managed with infliximab: A case report. Eur. Heart J. Case Rep. 2021, 5, ytab002. Available online: https://pubmed.ncbi.nlm.nih.gov/33644656/ (accessed on 5 June 2021).
- De Almeida, D.V.; Gomes, J.R.; Haddad, F.J.; Buzaid, A.C. Immune-mediated Pericarditis With Pericardial Tamponade During Nivolumab Therapy. J. Immunother. 2018, 41, 329–331. [Google Scholar] [CrossRef]
- Yang, S.; Asnani, A. Cardiotoxicities associated with immune checkpoint inhibitors. Curr. Probl. Cancer 2018, 42, 422–432. [Google Scholar] [CrossRef]
- Tan, N.Y.L.; Anavekar, N.S.; Wiley, B.M. Concomitant myopericarditis and takotsubo syndrome following immune checkpoint inhibitor therapy. BMJ Case Rep. 2020, 13, e235265. [Google Scholar] [CrossRef]
- Inno, A.; Maurea, N.; Metro, G.; Carbone, A.; Russo, A.; Gori, S. Immune checkpoint inhibitors-associated pericardial disease: A systematic review of case reports. Cancer Immunol. Immunother. 2021, 70, 3041–3053. Available online: https://pubmed.ncbi.nlm.nih.gov/33877385/ (accessed on 5 June 2021).
- BC Cancer. Ipilimumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Ipilimumab_monograph.pdf (accessed on 3 June 2021).
- FDA. Highlights of Prescribing Information: Ipilimumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125377s110lbl.pdf (accessed on 3 June 2021).
- Dolladille, C.; Ederhy, S.; Sassier, M.; Cautela, J.; Thuny, F.; Cohen, A.A.; Fedrizzi, S.; Chrétien, B.; DA Silva, A.; Plane, A.-F.; et al. Immune Checkpoint Inhibitor Rechallenge After Immune-Related Adverse Events in Patients With Cancer. JAMA Oncol. 2020, 6, 865–871. [Google Scholar] [CrossRef]
- BC Cancer. Pembrolizumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/pembrolizumab_monograph.pdf (accessed on 3 June 2021).
- FDA. Highlights of Prescribing Information: Pembrolizumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125514s096lbl.pdf (accessed on 3 June 2021).
- BC Cancer. Nivolumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/nivolumab_monograph.pdf (accessed on 3 June 2021).
- FDA. Highlights of Prescribing Information: Nivolumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/125554s090lbl.pdf (accessed on 3 June 2021).
- Brahmer, J.R.; Drake, C.G.; Wollner, I.; Powderly, J.D.; Picus, J.; Sharfman, W.H.; Stankevich, E.; Stankevich, A.; Salay, T.M.; McMiller, T.L.; et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: Safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3167–3175. Available online: https://pubmed.ncbi.nlm.nih.gov/20516446/ (accessed on 7 June 2021).
- June 25 2020—EPOV Scott Gettinger—The ASCO Post. Available online: https://ascopost.com/issues/june-25-2020/epov-scott-gettinger/ (accessed on 20 June 2021).
- BC Cancer. Atezolizumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Atezolizumab_Monograph.pdf (accessed on 6 August 2021).
- FDA. Highlights of Prescribing Information: Atezolizumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/761034s033s034s035s036s037s038lbl.pdf (accessed on 6 August 2021).
- Liu, S.-Y.; Huang, W.-C.; Yeh, H.-I.; Ko, C.-C.; Shieh, H.-R.; Hung, C.-L.; Chen, T.-Y.; Chen, Y.-J. Sequential Blockade of PD-1 and PD-L1 Causes Fulminant Cardiotoxicity-From Case Report to Mouse Model Validation. Cancers 2019, 11, 580. Available online: https://pubmed.ncbi.nlm.nih.gov/31022941/ (accessed on 6 August 2021).
- FDA. Highlights of Prescribing Information: Durvalumab. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/761069s002lbl.pdf (accessed on 6 August 2021).
- BC Cancer. Durvalumab. Available online: http://www.bccancer.bc.ca/drug-database-site/Drug%20Index/Durvalumab_monograph.pdf (accessed on 6 August 2021).
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, L.; Ernstoff, M.S.; Gardner, G.M.; Ginex, P.; et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J. Clin. Oncol. 2018, 36, 1714–1768. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6481621/ (accessed on 30 June 2021). [CrossRef]
- Samara, Y.; Yu, C.L.; Dasanu, C.A. Acute autoimmune myocarditis and hepatitis due to ipilimumab monotherapy for malignant melanoma. J. Oncol. Pharm. Pract. 2019, 25, 966–968. [Google Scholar] [CrossRef]
- Poto, R.; Marone, G.; Pirozzi, F.; Galdiero, M.R.; Cuomo, A.; Formisano, L.; Bianco, R.; Maria Della Corte, C.; Morgillo, F.; Napolitano, S.; et al. How can we manage the cardiac toxicity of immune checkpoint inhibitors? Expert Opin. Drug Saf. 2021, 20. Available online: https://pubmed.ncbi.nlm.nih.gov/33749484/ (accessed on 30 July 2021).
- Konala, V.M.; Adapa, S.; Aronow, W.S. Immune Checkpoint Inhibitors–Related Cardiotoxicity. Am. J. Ther. 2020, 27, e591–e598. Available online: https://pubmed.ncbi.nlm.nih.gov/31008763/ (accessed on 30 July 2021).
- Spallarossa, P.; Sarocchi, M.; Tini, G.; Arboscello, E.; Toma, M.; Ameri, P.; Porto, I. How to Monitor Cardiac Complications of Immune Checkpoint Inhibitor Therapy. Front. Pharmacol. 2020, 11, 972. Available online: https://pubmed.ncbi.nlm.nih.gov/32676031/ (accessed on 31 July 2021).
- Sarocchi, M.; Grossi, F.; Arboscello, E.; Bellodi, A.; Genova, C.; Bello, M.G.D.; Rijavec, E.; Barletta, G.; Biello, F.; Ghigliotti, G.; et al. Serial Troponin for Early Detection of Nivolumab Cardiotoxicity in Advanced Non-Small Cell Lung Cancer Patients. Oncologist 2018, 23, 936–942. Available online: https://pubmed.ncbi.nlm.nih.gov/29567824/ (accessed on 30 July 2021).
- Shalata, W.; Peled, N.; Gabizon, I.; Abu Saleh, O.; Kian, W.; Yakobson, A. Associated Myocarditis: A Predictive Factor for Response? Case Rep. Oncol. 2020, 13, 550–557. [Google Scholar] [CrossRef]
- Balanescu, D.V.; Donisan, T.; Palaskas, N.; Lopez-Mattei, J.; Kim, P.Y.; Buja, L.M.; McNamara, D.M.; Kobashigawa, J.A.; Durand, J.B.; Iliescu, C.A. Immunomodulatory treatment of immune checkpoint inhibitor-induced myocarditis: Pathway toward precision-based therapy. Cardiovasc. Pathol. 2020, 47, 107211. Available online: https://pubmed.ncbi.nlm.nih.gov/32268262/ (accessed on 31 July 2021).
- Saade, A.; Mansuet-Lupo, A.; Arrondeau, J.; Thibault, C.; Mirabel, M.; Goldwasser, F.; Oudard, S.; Weiss, L. Pericardial effusion under nivolumab: Case-reports and review of the literature. J. Immunother. Cancer 2019, 7, 335. Available online: https://pubmed.ncbi.nlm.nih.gov/31627742/ (accessed on 31 July 2021).
- Al-Obaidi, A.; Parker, N.A.; Choucair, K.; Alderson, J.; Deutsch, J.M. A Case of Acute Heart Failure Following Immunotherapy for Metastatic Lung Cancer. Cureus 2020, 12, e8093. Available online: https://pubmed.ncbi.nlm.nih.gov/32542148/ (accessed on 31 July 2021).
- Khan, A.M.; Munir, A.; Thalody, V.; Munshi, M.K.; Mehdi, S. Cardiac tamponade in a patient with stage IV lung adenocarcinoma treated with pembrolizumab. Immunotherapy 2019, 11, 1533–1540. Available online: https://pubmed.ncbi.nlm.nih.gov/31815569/ (accessed on 31 July 2021).
- Asai, M.; Kato, Y.; Kawai, S.; Watanabe, K.; Yomota, M.; Okuma, Y.; Hosomi, Y.; Hishima, T.; Okamura, T. Management of cardiac tamponade during nivolumab of lung cancer with intrapericardial bleomycin: Case report. Immunotherapy 2019, 11, 467–472. Available online: https://pubmed.ncbi.nlm.nih.gov/30727791/ (accessed on 22 July 2021).
- Atallah-Yunes, S.A.; Kadado, A.J.; Soe, M.H. Pericardial effusion due to pembrolizumab-induced immunotoxicity: A case report and literature review. Curr. Probl. Cancer. 2019, 43, 504–510. Available online: https://pubmed.ncbi.nlm.nih.gov/30685067/ (accessed on 22 July 2021).
- Khoury, Z.H.; Hausner, P.F.; Idzik-Starr, C.L.; Frykenberg, M.R.A.; Brooks, J.K.; Dyalram, D.; Basile, J.R.; Younis, R.H. Combination nivolumab/ipilimumab immunotherapy for melanoma with subsequent unexpected cardiac arrest: A case report and review of literature. J. Immunother. 2019, 42, 313–317. [Google Scholar] [CrossRef]
- Salem, J.E.; Allenbach, Y.; Vozy, A.; Brechot, N.; Johnson, D.B.; Moslehi, J.J.; Kerneis, M. Abatacept for severe immune checkpoint inhibitor-associated myocarditis. N. Engl. J. Med. 2019, 380, 2377–2379. [Google Scholar] [CrossRef]
- Esfahani, K.; Buhlaiga, N.; Thébault, P.; Lapointe, R.; Johnson, N.A.; Miller, W.H. Alemtuzumab for immune-related myocarditis due to PD-1 therapy. N. Engl. J. Med. 2019, 380, 2375–2376. [Google Scholar] [CrossRef]
- Dhenin, A.; Samartzi, V.; Lejeune, S.; Seront, E. Cascade of immunologic adverse events related to pembrolizumab treatment. BMJ Case Rep. 2019, 12, 6. [Google Scholar] [CrossRef]
- Huertas, R.M.; Serrano, C.S.; Perna, C.; Gómez, A.F.; Gordoa, T.A. Cardiac toxicity of immune-checkpoint inhibitors: A clinical case of nivolumab-induced myocarditis and review of the evidence and new challenges. Cancer Manag. Res. 2019, 11, 4541. [Google Scholar] [CrossRef] [Green Version]
- Fazel, M.; Jedlowski, P.M. Severe myositis, myocarditis, and myasthenia gravis with elevated anti-striated muscle antibody following single dose of ipilimumab-nivolumab therapy in a patient with metastatic melanoma. Case Reports Immunol. 2019, 2019, 2539493. [Google Scholar] [CrossRef] [Green Version]
- So, H.; Ikeguchi, R.; Kobayashi, M.; Suzuki, M.; Shimizu, Y.; Kitagawa, K. PD-1 inhibitor-associated severe myasthenia gravis with necrotizing myopathy and myocarditis. J. Neurol. Sci. 2019, 399, 97–100. [Google Scholar] [CrossRef]
- Sakai, T.; Yahagi, K.; Hoshino, T.; Yokota, T.; Tanabe, K.; Mori, M.; Ikeda, S. Nivolumab-induced myocardial necrosis in a patient with lung cancer: A case report. Respir. Med. Case Rep. 2019, 27, 100839. [Google Scholar] [CrossRef]
- Sharma, M.; Suero-Abreu, G.A.; Kim, B. A Case of Acute Heart Failure due to Immune Checkpoint Blocker Nivolumab. Cardiol. Res. 2019, 10, 120–123. [Google Scholar] [CrossRef]
- Charles, J.; Giovannini, D.; Terzi, N.; Schwebel, C.; Sturm, N.; Masson, D.; Leccia, M.T.; Cahn, J.Y.; Manches, O.; Bulabois, C.E.; et al. Multi-organ failure induced by Nivolumab in the context of allo-stem cell transplantation. Exp. Hematol. Oncol. 2019, 8, 8. [Google Scholar] [CrossRef]
- Agrawal, N.; Khunger, A.; Vachhani, P.; Colvin, T.A.; Hattoum, A.; Spangenthal, E.; Curtis, A.B.; Dy, G.K.; Ernstoff, M.S.; Puzanov, I. Cardiac toxicity associated with immune checkpoint inhibitors: Case series and review of the literature. Case Rep. Oncol. 2019, 12, 260–276. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Su, Y.W.; Chen, S.C. Sick sinus syndrome associated with anti-programmed cell death-1. J. Immunother. Cancer 2018, 6, 72. [Google Scholar] [CrossRef] [Green Version]
- Gallegos, C.; Rottmann, D.; Nguyen, V.Q.; Baldassarre, L.A. Myocarditis with checkpoint inhibitor immunotherapy: Case report of late gadolinium enhancement on cardiac magnetic resonance with pathology correlate. Eur. Heart J. Case Rep. 2019, 3, yty149. [Google Scholar] [CrossRef]
- Tachihara, M.; Yamamoto, M.; Yumura, M.; Yoshizaki, A.; Kobayashi, K.; Nishimura, Y. Non-parallel anti-tumour effects of pembrolizumab: A case of cardial tamponade. Respirol. Case Rep. 2019, 7, e00404. [Google Scholar] [CrossRef]
- Yamasaki, M.; Daido, W.; Saito, N.; Funaishi, K.; Okada, T.; Kawamoto, K.; Matsumoto, Y.; Matsumoto, N.; Taniwaki, M.; Ohashi, N.; et al. Pericardial Effusion With Tamponade in Lung Cancer Patients During Treatment With Nivolumab: A Report of Two Cases. Front. Oncol. 2019, 9, 4. [Google Scholar] [CrossRef] [Green Version]
- Vittorio, A.; Sharma, R.; Siejka, D.; Bhattarai, K.; Hardikar, A. Recurrent Pericardial Effusion While Receiving Nivolumab for Metastatic Lung Adenocarcinoma: Case Report and Review of the Literature. Clin. Lung Cancer 2018, 19, e717–e720. [Google Scholar] [CrossRef] [PubMed]
- Monge, C.; Maeng, H.; Brofferio, A.; Apolo, A.B.; Sathya, B.; Arai, A.E.; Gulley, J.L.; Bilusic, M. Myocarditis in a patient treated with Nivolumab and PROSTVAC: A case report. J. Immunother. Cancer 2018, 6, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaheen, S.; Mirshahidi, H.; Nagaraj, G.; Hsueh, C.T. Conservative management of nivolumab-induced pericardial effusion: A case report and review of literature. Exp. Hematol. Oncol. 2018, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Inayat, F.; Masab, M.; Gupta, S.; Ullah, W. New drugs and new toxicities: Pembrolizumab-induced myocarditis. BMJ Case Rep. 2018, 2018, bcr2017223252. [Google Scholar] [CrossRef]
- Thibault, C.; Vano, Y.; Soulat, G.; Mirabel, M. Immune checkpoint inhibitors myocarditis: Not all cases are clinically patent. Eur. Heart J. 2018, 39, 3553. [Google Scholar] [CrossRef]
- Jain, V.; Mohebtash, M.; Rodrigo, M.E.; Ruiz, G.; Atkins, M.B.; Barac, A. Autoimmune myocarditis caused by immune checkpoint inhibitors treated with antithymocyte globulin. J. Immunother. 2018, 41, 332–335. [Google Scholar] [CrossRef]
- Ederhy, S.; Cautela, J.; Ancedy, Y.; Escudier, M.; Thuny, F.; Cohen, A. Takotsubo-Like Syndrome in Cancer Patients Treated With Immune Checkpoint Inhibitors. JACC Cardiovasc. Imaging. 2018, 11, 1187–1190. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Morimoto, R.; Okumura, T.; Yamashita, Y.; Haga, T.; Kuwayama, T.; Yokoi, T.; Hiraiwa, H.; Kondo, T.; Sugiura, Y.; et al. Late-onset fulminant myocarditis with immune checkpoint inhibitor nivolumab. Can. J. Cardiol. 2018, 34, 812.e1–812.e3. [Google Scholar] [CrossRef] [PubMed]
- Oristrell, G.; Baneras, J.; Ros, J.; Munoz, E. Cardiac tamponade and adrenal insufficiency due to pembrolizumab: A case report. Eur. Heart J. Case Rep. 2018, 2, yty038. [Google Scholar] [CrossRef] [PubMed]
- Frigeri, M.; Meyer, P.; Banfi, C.; Giraud, R.; Hachulla, A.L.; Spoerl, D.; Friedlaender, A.; Pugliesi-Rinaldi, A.; Dietrich, P.Y. Immune checkpoint inhibitor-associated myocarditis: A new challenge for cardiologists. Can. J. Cardiol. 2018, 34, 92.e1–92.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tajmir-Riahi, A.; Bergmann, T.; Schmid, M.; Agaimy, A.; Schuler, G.; Heinzerling, L. Life-threatening autoimmune cardiomyopathy reproducibly induced in a patient by checkpoint inhibitor therapy. J. Immunother. 2018, 41, 35–38. [Google Scholar] [CrossRef]
- Katsume, Y.; Isawa, T.; Toi, Y.; Fukuda, R.; Kondo, Y.; Sugawara, S.; Ootomo, T. Complete atrioventricular block associated with pembrolizumab-induced acute myocarditis: The need for close cardiac monitoring. Intern. Med. 2018, 57, 3157–3162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Huang, D.S.; Zhang, L.W.; Li, Y.Q.; Wang, H.W.; Liu, H.B. Fatal myocarditis and rhabdomyolysis induced by nivolumab during the treatment of type B3 thymoma. Clin. Toxicol. 2018, 56, 667–671. [Google Scholar] [CrossRef]
- Matson, D.R.; Accola, M.A.; Rehrauer, W.M.; Corliss, R.F. Fatal Myocarditis Following Treatment with the PD-1 Inhibitor Nivolumab. J. Forensic. Sci. 2018, 63, 954–957. [Google Scholar] [CrossRef]
- Norwood, T.G.; Westbrook, B.C.; Johnson, D.B.; Litovsky, S.H.; Terry, N.L.; McKee, S.B.; Gertler, A.S.; Moslehi, J.J.; Conry, R.M. Smoldering myocarditis following immune checkpoint blockade. J. Immunother. Cancer 2017, 5, 91. [Google Scholar] [CrossRef]
- Arangalage, D.; Delyon, J.; Lermuzeaux, M.; Ekpe, K.; Ederhy, S.; Pages, C.; Lebbé, C. Survival after fulminant myocarditis induced by immune-checkpoint inhibitors. Ann. Intern. Med. 2017, 167, 683–684. [Google Scholar] [CrossRef]
- Penel, N.; Cordoba, A.; Mathoulin-Pelissier, S. Lessons from three phase III trials assessing neoadjuvant treatment in sarcoma patients. Ann. Oncol. 2017, 28, 2891–2893. [Google Scholar] [CrossRef]
- Zarogoulidis, P.; Chinelis, P.; Athanasiadou, A.; Tsiouda, T.; Trakada, G.; Kallianos, A.; Veletza, L.; Hatzibougias, D.; Mihalopoulou, E.; Goupou, E.; et al. Possible adverse effects of immunotherapy in non-small cell lung cancer; Treatment and follow-up of three cases. Respir. Med. Case Rep. 2017, 22, 101–105. [Google Scholar] [CrossRef]
- Reddy, N.; Moudgil, R.; Lopez-Mattei, J.C.; Karimzad, K.; Mouhayar, E.N.; Somaiah, N.; Conley, A.P.; Patel, S.; Giza, D.E.; Iliescu, C. Progressive and Reversible Conduction Disease With Checkpoint Inhibitors. Can. J. Cardiol. 2017, 33, 1335.e13–1335.e15. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Tounai, Y.; Nagato, K.; Morimoto, J.I.; Tounai, Y. A case of heart failure after treatment with anti-PD-1 antibody followed by adoptive transfer of cytokine-activated killer cells in a recurrent lung cancer patient. J. Thorac. Oncol. 2017, 12, e128–e130. [Google Scholar] [CrossRef] [PubMed]
- Behling, J.; Kaes, J.; Munzel, T.; Grabbe, S.; Loquai, C. New-onset third-degree atrioventricular block because of autoimmune-induced myositis under treatment with anti-programmed cell death-1 (nivolumab) for metastatic melanoma. Melanoma Res. 2017, 27, 155–158. [Google Scholar] [CrossRef]
- Chu, Y.C.; Fang, K.C.; Chen, H.C.; Yeh, Y.C.; Tseng, C.E.; Chou, T.Y.; Lai, C.L. Pericardial tamponade caused by a hypersensitivity response to tuberculosis reactivation after anti-PD-1 treatment in a patient with advanced pulmonary adenocarcinoma. J. Thorac. Oncol. 2017, 12, e111–e114. [Google Scholar] [CrossRef]
- Kushnir, I.; Wolf, I. Nivolumab-induced pericardial tamponade: A case report and discussion. Cardiology 2017, 136, 49–51. [Google Scholar] [CrossRef]
- Kolla, B.C.; Patel, M.R. Recurrent pleural effusions and cardiac tamponade as possible manifestations of pseudoprogression associated with nivolumab therapy—a report of two cases. J. Immunother. Cancer 2016, 4, 80. [Google Scholar] [CrossRef] [Green Version]
- Roth, M.E.; Muluneh, B.; Jensen, B.C.; Madamanchi, C.; Lee, C.B. Left ventricular dysfunction after treatment with ipilimumab for metastatic Melanoma. Am. J. Ther. 2016, 23, e1925–e1928. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Gupta, A.; Hannallah, F.; Koshy, T.; Reimold, S. Myocarditis as an immune-relatedadverse event with ipilimumab/nivolumab combination therapy for meta-static melanoma. Melanoma Res. 2016, 26, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, L.; Goldinger, S.M.; Hofmann, L.; Loquai, C.; Ugurel, S.; Thomas, I.; Schmidgen, M.I.; Gutzmer, R.; Utikal, J.S.; Göppner, D.; et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur. J. Cancer 2016, 60, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Tadokoro, T.; Keshino, E.; Makiyama, A.; Sasaguri, T.; Ohshima, K.; Katano, H.; Mohri, M. Acute lymphocytic myocarditis with anti-PD-1 antibody nivolumab. Circ. Heart Fail. 2016, 9, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nesfeder, J.; Elsensohn, A.N.; Thind, M.; Lennon, J.; Domsky, S. Pericardial effusion with tamponade physiology induced by nivolumab. Int. J. Cardiol. 2016, 222, 613–614. [Google Scholar] [CrossRef] [PubMed]
- Semper, H.; Muehlberg, F.; Schulz-Menger, J.; Allewelt, M.; Grohé, C. Drug-induced myocarditis after nivolumab treatment in a patient with PDL1-negative squamous cell carcinoma of the lung. Lung Cancer. 2016, 99, 117–119. [Google Scholar] [CrossRef]
- Gibson, R.; Delaune, J.; Szady, A.; Markham, M. Suspected autoimmune myocarditis and cardiac conduction abnormalities with nivolumab therapy for non-small cell lung cancer. BMJ Case Rep. 2016, 2016, bcr2016216228. [Google Scholar] [CrossRef] [PubMed]
- Geisler, B.P.; Raad, R.A.; Esaian, D.; Sharon, E.; Schwartz, D.R. Apical ballooning and cardiomyopathy in a melanoma patient treated with ipilimumab: A case of takotsubo-like syndrome. J. Immunother. Cancer 2015, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Yun, S.; Vincelette, N.D.; Mansour, I.; Hariri, D.; Motamed, S. Late onset ipilimumab-induced pericarditis and pericardial effusion: A rare but life threatening complication. Case Rep. Oncol. Med. 2015, 2015, 794842. [Google Scholar] [CrossRef]
Figure 1.
Median weeks until presentation of ICI cardiotoxicity by treatment and cancer type. All cancer types and treatments present within a median of 1–31 weeks after starting treatment.
Figure 1.
Median weeks until presentation of ICI cardiotoxicity by treatment and cancer type. All cancer types and treatments present within a median of 1–31 weeks after starting treatment.

Figure 2.
Median weeks until presentation of ICI cardiotoxicity by treatment and type of cardiotoxicity. All types of cardiotoxicity and treatments present within a median of 1–104 weeks after starting treatment.
Figure 2.
Median weeks until presentation of ICI cardiotoxicity by treatment and type of cardiotoxicity. All types of cardiotoxicity and treatments present within a median of 1–104 weeks after starting treatment.

Table 1.
ICI-associated cardiotoxicities and their characteristics.
| Type of Cardiotoxicity | Median Onset | Most Common Symptoms | Diagnosis | Treatment | Sources |
|---|---|---|---|---|---|
| Myocarditis | 65 days | Shortness of breath, palpitations, edema, and fatigue | NT-proBNP, troponin I, endomyocardial biopsy, and CMR | High-dose corticosteroids | [15,16,17,18,19,20,21] |
| Pericarditis | 30 days | Shortness of breath, chest pain | ECG changes, CMR, pericardial effusion, and fluid analysis | Pericardiocentesis, NSAIDs, colchicine, and high-dose corticosteroids | [7,16,22,23,24,25] |
| Takotsubo cardiomyopathy | 15 weeks to 8 months | Unknown | ECG changes, troponin and NT-proBNP | High-dose corticosteroids | [17,23,26] |
| Arrhythmias and conduction disorders | Unknown | Unknown | ECG changes | High-dose corticosteroids, supportive | [17,18,22] |
| Myocardial infarction | Unknown | Chest pain and shortness of breath | ECG changes, troponin, and others | Cardiac catheterization, supportive | [17] |
Abbreviations: ICI, immune checkpoint inhibitor; NT–proBNP, N-terminal -prohormone brain natriuretic peptide; CMR, cardiovascular magnetic resonance imaging; ECG, electrocardiogram; NSAIDs, non-steroidal anti-inflammatory drugs.
Table 2.
Weeks until Presentation of ICI-associated cardiotoxicity, organized by treatment.
| Treatment | Ipilimumab | Nivolumab | Pembrolizumab | Ipilimumab + Nivolumab | Durvalumab | Atezolizumab | Unspecified |
|---|---|---|---|---|---|---|---|
| Number of Cases | 18 | 43 | 20 | 17 | 3 | 1 | 5 |
| Average Weeks until Presentation | 18 | 17 | 9 | 10 | 11 | 1 | -- |
| Median Weeks until Presentation | 10 | 9 | 7 | 6 | 8 | 1 | -- |
Table 3.
Weeks until ICI-associated cardiotoxicity, organized by treatment and type of cancer.
| Treatment | Type of Cancer Treated | Number of Cases | Average Weeks until Presentation | Median Weeks until Presentation |
|---|---|---|---|---|
| Ipilimumab | Melanoma | 13 | 21 | 15 |
| Lymphoma | 1 | 8 | 8 | |
| MDS | 2 | 4 | 4 | |
| Nivolumab | Lung Cancer | 30 | 20 | 9 |
| HCC | 1 | 3 | 3 | |
| Kidney Cancer | 1 | 12 | 12 | |
| Melanoma | 7 | 12 | 9 | |
| Lymphoma | 2 | 14 | 14 | |
| Prostate Cancer | 1 | 8 | 8 | |
| Thymoma | 1 | 1 | 1 | |
| Pembrolizumab | Urothelial Carcinoma | 1 | 15 | 15 |
| Lung Cancer | 7 | 7 | 8 | |
| Cutaneous SCC | 1 | 7 | 7 | |
| Prostate Cancer | 1 | 4 | 4 | |
| Melanoma | 6 | 9 | 6 | |
| Malignant Mesothelioma | 1 | 5 | 5 | |
| HCC | 1 | 18 | 18 | |
| Multiple Myeloma | 1 | 2 | 2 | |
| Breast Cancer | 1 | 15 | 15 | |
| Ipilimumab + Nivolumab | Lung Cancer | 2 | 31 | 31 |
| Melanoma | 13 | 8 | 4 | |
| RCC | 2 | 4 | 4 |
Abbreviations: MDS, myelodysplastic syndrome; HCC, hepatocellular carcinoma; SCC, squamous cell carcinoma; and RCC, renal cell carcinoma.
Table 4.
Weeks until ICI-associated cardiotoxicity, organized by treatment and type of cardiotoxicity.
Table 4.
Weeks until ICI-associated cardiotoxicity, organized by treatment and type of cardiotoxicity.
| Treatment | Type of Cardiotoxicity | Number of Cases | Average Weeks until Presentation | Median Weeks until Presentation |
|---|---|---|---|---|
| Ipilimumab + Nivolumab | Perimyocarditis | 1 | 10 | 10 |
| Myocarditis | 11 | 10 | 4 | |
| Cardiomyopathy | 3 | 13 | 6 | |
| Conduction Disorders | 1 | 17 | 17 | |
| Combination | 1 | 2 | 2 | |
| Ipilimumab | Perimyocarditis | 1 | 1 | 1 |
| Myocarditis | 7 | 12 | 8 | |
| Cardiomyopathy | 3 | 15 | 15 | |
| Conduction Disorders | 1 | 104 | 104 | |
| Pericarditis | 3 | 23 | 24 | |
| Combination | 1 | 4 | 4 | |
| Other | 1 | 10 | 10 | |
| Nivolumab | Myocarditis | 10 | 11 | 9 |
| Pericarditis | 21 | 22 | 10 | |
| Combination | 6 | 4 | 3 | |
| Other | 6 | 10 | 4 | |
| Pembrolizumab | Myocarditis | 7 | 6 | 5 |
| Cardiomyopathy | 1 | 7 | 7 | |
| Conduction Disorders | 1 | 18 | 18 | |
| Pericarditis | 5 | 10 | 9 | |
| Combination | 4 | 5 | 4 | |
| Other | 2 | 20 | 20 |
Table 5.
Immune checkpoint inhibitors, their indications, and side effects.
| Drug | First Approved | Cancers Approved for Treatment | Most Common Side Effects |
|---|---|---|---|
| Ipilimumab | 2011 | Melanoma, RCC, CRC, HCC, and NSCLC | Fatigue, diarrhea, pruritis, rash, and colitis |
| Pembrolizumab | 2014 | Melanoma, lung cancer, SCC, lymphomas, urothelial carcinoma, cancers high in MSI, MMR-deficient cancers, gastric cancers, esophageal cancers, cervical cancers, HCC, Merkel cell cancer, RCC, endometrial carcinoma, tumor mutational burden-high cancer, and triple-negative breast cancer | Fatigue, musculoskeletal pain, decreased appetite, diarrhea, rash, fever, cough, constipation, nausea, abdominal pain, and pruritis |
| Nivolumab | 2014 | Melanoma, NSCLC, malignant pleural mesothelioma, RCC, classic Hodgkin lymphoma, HNSCC, urothelial carcinoma, CRC, HCC, and esophageal squamous cell carcinoma | Fatigue, rash, pruritis, and diarrhea |
| Atezolizumab | 2016 | Urothelial carcinoma, NSCLC, triple-negative breast cancer, SCLC, HCC, and melanoma | Fatigue, nausea, vomiting, cough, dyspnea, decreased appetite, alopecia, constipation or diarrhea, headache, and rash |
| Durvalumab | 2017 | Urothelial carcinoma and NSCLC | Fatigue, constipation, UTIs, edema, pneumonitis, dyspnea, rash, cough, and nausea |
Abbreviations: RCC, renal cell carcinoma; CRC, colorectal cancer; HCC, hepatocellular carcinoma, NSCLC, non-small-cell lung cancer; SCC, squamous cell carcinoma; MSI, microsatellite instability; MMR, mismatch repair; HNSCC, head and neck squamous cell carcinoma; SCLC, small-cell lung cancer; and UTIs, urinary tract infections.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shalata, W.; Abu-salman, A.; Steckbeck, R.; Mathew Jacob, B.; Massalha, I.; Yakobson, A. Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review. Cancers 2021, 13, 5218. https://doi.org/10.3390/cancers13205218
AMA Style
Shalata W, Abu-salman A, Steckbeck R, Mathew Jacob B, Massalha I, Yakobson A. Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review. Cancers. 2021; 13(20):5218. https://doi.org/10.3390/cancers13205218
Chicago/Turabian StyleShalata, Walid, Amjad Abu-salman, Rachel Steckbeck, Binil Mathew Jacob, Ismaell Massalha, and Alexander Yakobson. 2021. "Cardiac Toxicity Associated with Immune Checkpoint Inhibitors: A Systematic Review" Cancers 13, no. 20: 5218. https://doi.org/10.3390/cancers13205218
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.