Characterisation of Prostate Lesions Using Transrectal Shear Wave Elastography (SWE) Ultrasound Imaging: A Systematic Review

 , ,
, ,  , and
, and 
Abstract
:Simple Summary
Abstract
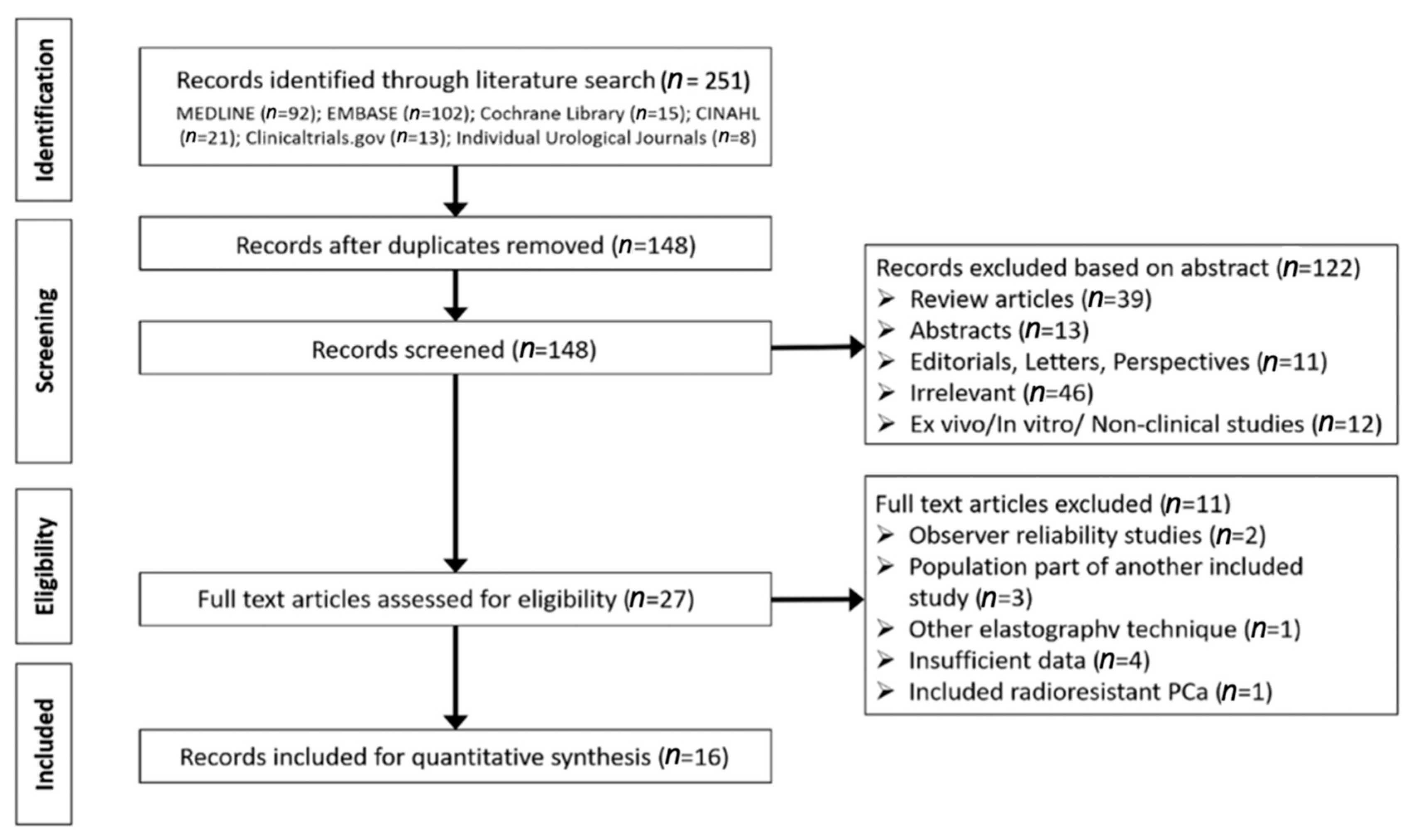
1. Introduction
- Evaluate detection rates of PCa with SWE, with respect to the reference standard used (i.e., SB level and whole-mount histopathology of the radical prostatectomy (RP) specimen);
- Compare diagnostic estimates between studies reporting detection of all PCa with studies reporting detection of csPCa (defined as having at least a Gleason score >6 with a tumour burden ≥3 mm).
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abraham, N.E.; Mendhiratta, N.; Taneja, S.S. Patterns of repeat prostate biopsy in contemporary clinical practice. J. Urol. 2015, 193, 1178–1184. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25444971 (accessed on 5 August 2020). [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Serefoglu, E.C.; Altinova, S.; Ugras, N.S.; Akincioglu, E.; Asil, E.; Balbay, M.D. How reliable is 12-core prostate biopsy procedure in the detection of prostate cancer? J. Can. Urol. Assoc. 2013, 7, E293–E298. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22398204 (accessed on 5 August 2020). [CrossRef] [Green Version]
- EAU Guidelines: Prostate Cancer|Uroweb. Available online: https://uroweb.org/guideline/prostate-cancer/#note_193 (accessed on 5 August 2020).
- Richenberg, J.; Løgager, V.; Panebianco, V.; Rouviere, O.; Villeirs, G.; Schoots, I.G. The primacy of multiparametric MRI in men with suspected prostate cancer. Eur. Radiol. 2019, 29, 6940–6952. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31172275 (accessed on 5 August 2020). [CrossRef] [Green Version]
- Sonn, G.A.; Fan, R.E.; Ghanouni, P.; Wang, N.N.; Brooks, J.D.; Loening, A.M.; Daniel, B.L.; To’o, K.J.; Thong, A.E.; Leppert, J.T. Prostate Magnetic Resonance Imaging Interpretation Varies Substantially Across Radiologists. Eur. Urol. Focus 2019, 5, 592–599. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29226826 (accessed on 5 August 2020). [CrossRef] [PubMed] [Green Version]
- Beerlage, H.P.; Aarnink, R.G.; Ruijter, E.; Witjes, J.A.; Wijkstra, H.; Van De Kaa, C.A.; Debruyne, F.J.; De La Rosette, J.J.M.C.H. Correlation of transrectal ultrasound, computer analysis of transrectal ultrasound and histopathology of radical prostatectomy specimen. Prostate Cancer Prostatic Dis. 2001, 4, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bercoff, J.; Tanter, M.; Fink, M. Supersonic shear imaging: A new technique for soft tissue elasticity mapping. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2004, 51, 396–409. [Google Scholar] [CrossRef] [PubMed]
- Xiang, L.H.; Fang, Y.; Wan, J.; Xu, G.; Yao, M.H.; Ding, S.S.; Liu, H.; Wu, R. Shear-wave elastography: Role in clinically significant prostate cancer with false-negative magnetic resonance imaging. Eur. Radiol. 2019, 29, 6682–6689. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Tang, J.; Luo, Y.; Wang, Y.; Wu, M.; Memmott, B.; Gao, J. Diagnostic performance of multiparametric transrectal ultrasound in localized prostate cancer: A comparative study with magnetic resonance imaging. J. Ultrasound Med. 2019, 38, 1823–1830. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30561768 (accessed on 5 August 2020). [CrossRef]
- Sang, L.; Wang, X.M.; Xu, D.Y.; Cai, Y.F. Accuracy of shear wave elastography for the diagnosis of prostate cancer: A meta-analysis. Sci. Rep. 2017, 7, 1949. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28512326 (accessed on 5 August 2020). [CrossRef] [Green Version]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Shear-wave elastography for detection of prostate cancer: A systematic review and diagnostic meta-analysis. Am. J. Roentgenol. 2017, 209, 806–814. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28796546 (accessed on 5 August 2020). [CrossRef] [PubMed]
- Yang, Y.; Zhao, X.; Shi, J.; Huang, Y. Value of shear wave elastography for diagnosis of primary prostate cancer: A systematic review and meta-analysis. Med Ultrason. Soc. Romana Ultrason. Med. Biol. 2019, 21, 382–388. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31765445 (accessed on 5 August 2020). [CrossRef] [PubMed]
- Zheng, X.; Ji, P.; Mao, H.; Hu, J. A comparison of virtual touch tissue quantification and digital rectal examination for discrimination between prostate cancer and benign prostatic hyperplasia. Radiol. Oncol. 2012, 46, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, R.G.; Memo, R.; Schaub, C.R. Shear wave ultrasound elastography of the prostate: Initial results. Ultrasound Q. 2012, 28, 13–20. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22357224 (accessed on 5 August 2020). [CrossRef] [PubMed]
- Woo, S.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Shear wave elastography for detection of prostate cancer: A preliminary study. Korean J. Radiol. 2014, 15, 346–355. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24843239 (accessed on 5 August 2020). [CrossRef] [Green Version]
- Boehm, K.; Salomon, G.; Beyer, B.; Schiffmann, J.; Simonis, K.; Graefen, M.; Budaeus, L. Shear wave elastography for localization of prostate cancer lesions and assessment of elasticity thresholds: Implications for targeted biopsies and active surveillance protocols. J. Urol. 2015, 193, 794–800. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25264337 (accessed on 5 August 2020). [CrossRef]
- Boehm, K.; Budäus, L.; Tennstedt, P.; Beyer, B.; Schiffmann, J.; Larcher, A.; Simonis, K.; Graefen, M.; Beyersdorff, D.; Salomon, G. Prediction of Significant Prostate Cancer at Prostate Biopsy and Per Core Detection Rate of Targeted and Systematic Biopsies Using Real-Time Shear Wave Elastography. Urol. Int. 2015, 95, 189–196. Available online: https://www.karger.com/Article/FullText/431233 (accessed on 5 August 2020). [CrossRef]
- Correas, J.M.; Tissier, A.M.; Khairoune, A.; Vassiliu, V.; Méjean, A.; Hélénon, O.; Memo, R.; Barr, R.G. Prostate cancer: Diagnostic performance of real-time shear-wave elastography. Radiology 2015, 275, 280–289. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25599156 (accessed on 5 August 2020). [CrossRef] [Green Version]
- Rouvière, O.; Melodelima, C.; Dinh, A.H.; Bratan, F.; Pagnoux, G.; Sanzalone, T.; Crouzet, S.; Colombel, M.; Mège-Lechevallier, F.; Souchon, R. Stiffness of benign and malignant prostate tissue measured by shear-wave elastography: A preliminary study. Eur. Radiol. 2017, 27, 1858–1866. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27553936 (accessed on 5 August 2020).
- Ahmad, S.; Cao, R.; Varghese, T.; Bidaut, L.; Nabi, G. Transrectal quantitative shear wave elastography in the detection and characterisation of prostate cancer. Surg. Endosc. 2013, 27, 3280–3287. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, P.; Yin, B.; Fei, X.; Xu, X.; Song, Y. Transrectal shear wave elastography combined with transition zone biopsy for detecting prostate cancer. Zhonghua Nan Ke Xue 2015, 21, 610–614. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26333222 (accessed on 5 August 2020). [PubMed]
- Porsch, M.; Görner, C.; Wendler, J.J.; Liehr, U.B.; Lux, A.; Siedentopf, S.; Schostak, M.; Pech, M. Inability of shear-wave elastography to distinguish malignant from benign prostate tissue—A comparison of biopsy, whole-mount sectioning and shear-wave elastography. J. Ultrason. 2016, 16, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Li, C.; Szewczyk-Bieda, M.; Upreti, D.; Lang, S.; Huang, Z.; Nabi, G. Performance Characteristics of Transrectal Shear Wave Elastography Imaging in the Evaluation of Clinically Localized Prostate Cancer: A Prospective Study. J. Urol. 2018, 200, 549–558. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29605444 (accessed on 5 August 2020). [CrossRef] [PubMed] [Green Version]
- Mannaerts, C.K.; Wildeboer, R.R.; Remmers, S.; van Kollenburg, R.A.; Kajtazovic, A.; Hagemann, J.; Postema, A.W.; van Sloun, R.J.; JRoobol, M.; Tilki, D.; et al. Multiparametric Ultrasound for Prostate Cancer Detection and Localization: Correlation of B-mode, Shear Wave Elastography and Contrast Enhanced Ultrasound with Radical Prostatectomy Specimens. J. Urol. 2019, 202, 1166–1173. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31246546 (accessed on 5 August 2020). [CrossRef]
- Ji, Y.; Ruan, L.; Ren, W.; Dun, G.; Liu, J.; Zhang, Y.; Wan, Q. Stiffness of prostate gland measured by transrectal real-time shear wave elastography for detection of prostate cancer: A feasibility study. Br. J. Radiol. 2019, 92, 20180970. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30875242 (accessed on 5 August 2020). [CrossRef]
- Fu, S.; Tang, Y.; Tan, S.; Zhao, Y.; Cui, L. Diagnostic Value of Transrectal Shear Wave Elastography for Prostate Cancer Detection in Peripheral Zone: Comparison with MRI. J. Endourol. 2020. [Google Scholar] [CrossRef]
- Harvey, H.; Morgan, V.; Fromageau, J.; O’Shea, T.; Bamber, J.; de Souza, N.M. Ultrasound Shear Wave Elastography of the Normal Prostate: Interobserver Reproducibility and Comparison with Functional Magnetic Resonance Tissue Characteristics. Ultrason. Imaging 2018, 40, 158–170. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29353529 (accessed on 5 August 2020). [CrossRef]
- Woo, S.; Kim, S.Y.; Lee, M.S.; Cho, J.Y.; Kim, S.H. Shear wave elastography assessment in the prostate: An intraobserver reproducibility study. Clin. Imaging 2015, 39, 484–487. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25481218 (accessed on 5 August 2020). [CrossRef]
- Wildeboer, R.R.; Mannaerts, C.K.; van Sloun, R.J.; Budäus, L.; Tilki, D.; Wijkstra, H.; Salomon, G.; Mischi, M. Automated multiparametric localization of prostate cancer based on B-mode, shear-wave elastography, and contrast-enhanced ultrasound radiomics. Eur. Radiol. 2020, 30, 806–815. [Google Scholar] [CrossRef] [Green Version]
- Wei, C.; Zhang, Y.; Malik, H.; Zhang, X.; Alqahtani, S.; Upreti, D.; Szewczyk-Bieda, M.; Lang, S.; Nabi, G. Prediction of Postprostatectomy Biochemical Recurrence Using Quantitative Ultrasound Shear Wave Elastography Imaging. Front. Oncol. 2019, 9, 572. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31338325 (accessed on 5 August 2020). [CrossRef] [Green Version]
- Zheng, X.Z.; Ji, P.; Mao, H.W.; Zhang, X.Y.; Xia, E.H.; Chen, X.F. A novel approach to assessing changes in prostate stiffness with age using Virtual touch tissue quantification. J. Ultrasound Med. 2011, 30, 387–390. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21357561 (accessed on 5 August 2020). [CrossRef] [PubMed]
- Shoji, S.; Hashimoto, A.; Nakamura, T.; Hiraiwa, S.; Sato, H.; Sato, Y.; Tajiri, T.; Miyajima, A. Novel application of three-dimensional shear wave elastography in the detection of clinically significant prostate cancer. Biomed. Rep. 2018, 8, 373–377. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29541458 (accessed on 5 August 2020). [CrossRef] [PubMed]
- Wei, C.; Szewczyk-Bieda, M.; Nibblok, P.; Brown, E.; Lang, S.; Nabi, G. Quantitative transrectal shear wave elastography undergoing salvage extraperitoneal laparoscopic radical prostatectomy following failed radiotherapy. Surg. Endosc. 2018, 32, 4552–4561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glybochko, P.V.; Alyaev, Y.G.; Amosov, A.V.; Krupinov, G.E.; Ganzha, T.M.; Vorobev, A.V.; Lumpov, I.S.; Semendyaev, R.I. Prostate cancer detection by assessing stiffness of different tissues using shear wave ultrasound elastog-raphy. Urologiia 2016, 3, 56–61. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28247631 (accessed on 5 August 2020).
- Su, R.; Xu, G.; Xiang, L.; Ding, S.; Wu, R. A Novel Scoring System for Prediction of Prostate Cancer Based on Shear Wave Elastography and Clinical Parameters. Urology 2018, 121, 112–117. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30171925 (accessed on 5 August 2020). [CrossRef]
- Wu, F.; Zhang, M.B.; Wang, Y.R.; Yang, Y.Y.; Li, Y.Y. Application Value of Transrectal Shear Wave Elastography Mode Combined with Elastic Modulus in the Diagnosis of Prostate Cancer. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2020, 42, 73–79. Available online: http://www.ncbi.nlm.nih.gov/pubmed/32131943 (accessed on 5 August 2020).
- Shear, Q.B. Real time two-dimensional Prostate, wave elastography in diagnosis of prostate cancer. Pract Oncol. 2017, 23, 454–457. [Google Scholar]
- Barr, R.G.; Cosgrove, D.; Brock, M.; Cantisani, V.; Correas, J.M.; Postema, A.W.; Salomon, G.; Tsutsumi, M.; Xu, H.X.; Dietrich, C.F. Wfumb Guidelines and Recommendations On The Clinical Use Of Ultrasound Elastography: Part 5. Prostate. Ultrasound Med. Biol. 2017. [Google Scholar] [CrossRef] [Green Version]
- Correas, J.M.; Halpern, E.J.; Barr, R.G.; Ghai, S.; Walz, J.; Bodard, S.; Dariane, C.; de la Rosette, J. Advanced ultrasound in the diagnosis of prostate cancer. World J. Urol. 2020, 1–16. [Google Scholar] [CrossRef]
- Zhen, L.; Liu, X.; Yegang, C.; Yongjiao, Y.; Yawei, X.; Jiaqi, K.; Xianhao, W.; Yuxuan, S.; Rui, H.; Wei, Z.; et al. Accuracy of multiparametric magnetic resonance imaging for diagnosing prostate Cancer: A systematic review and meta-analysis. BMC Cancer. 2019, 19. [Google Scholar] [CrossRef] [Green Version]
- Le, J.D.; Tan, N.; Shkolyar, E.; Lu, D.Y.; Kwan, L.; Marks, L.S.; Huang, J.; Margolis, D.J.; Raman, S.S.; Reiter, R.E. Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: Correlation with whole-mount histopathology. Eur. Urol. 2015, 67, 569–576. [Google Scholar] [CrossRef]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.-M.; D’Onofrio, M.; Drakonaki, E.E.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastographypart 1: Basic principles and technology. Ultraschall Med. 2013, 34, 169–184. Available online: https://pubmed.ncbi.nlm.nih.gov/23558397/ (accessed on 5 August 2020).
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22007046 (accessed on 5 August 2020). [CrossRef]
- Doebler, P.; Holling, H. Meta-Analysis of Diagnostic Accuracy with mada. Available online: http://r-forge.r-project.org/projects/mada/ (accessed on 5 August 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Country | Year | Design | n | n with PCa | Inclusion Criteria | Mean | Pathology Reference | Definition of PCa | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | PSA (ng/mL) | Prostate Volume (mL) | |||||||||
| Zheng [14] | China | 2012 | Retrosp | 107 | NS | Planned SB (biopsy indication: BPH and PSA > 4 ng/mL, as well as abnormal DRE and abnormal findings on TRUS) | 66.7 | NS | NS | SB | Not specified |
| Barr [15] | United States | 2012 | Prosp | 53 | 11 | Planned SB (biopsy indication: PSA > 4 ng/mL and/or abnormal DRE). | 64.2 | 5.05 | NS | SB | Not specified |
| Ahmad a [21] | United Kingdom | 2013 | Prosp | 39 | 22 | Planned prostate biopsy (PSA > 4 ng/mL, abnormal DRE, on active surveillance, and/or previous abnormal prostate biopsy). | 69 | >20 | NS | -SWE-targeted biopsy -SB | Gleason score of 6 or greater. |
| Ahmad b [21] | 11 | 11 | 4–20 | ||||||||
| Woo [16] | Korea | 2014 | Retrosp | 87 | 26 | Planned SB (biopsy indication: PSA > 4 ng/mL and/or abnormal DRE). | 66.0 | 12.8 | 58.6 | SB | Not specified |
| Boehm a [17] | Germany | 2015 | Prosp | 28 | 28 | Planned open or robotic assisted RP following biopsy proven PCa. | NS | 8.6 (median) | NS | Whole-mount RP histopathology | Gleason score of 6 or greater. |
| Boehm b [18] | Germany | 2015 | Prosp | 95 | 38 | Planned prostate biopsy (PSA > 4 ng/mL and/or abnormal DRE and no history of prostate cancer or TURP). | 67 (median) | 6.7 (median) | 50.0 (median) | -SWE-targeted biopsy -SB | Gleason pattern 4 or greater with more than two affected cores. |
| Correas [19] | France, United STates | 2015 | Prosp | 184 | 68 | Planned SB (PSA > 4.0 ng/mL or increasing PSA and/or abnormal DRE). | 65.1 | 7.46 | 52.0 | SB | Gleason score of 6 or greater and at least 3 mm. |
| Zhang a [22] | China | 2015 | Retrosp | 489 | 221 | Suspected PCa undergoing prostate biopsy | 70.21 | 14.52 | NS | -SB -SWE combined with transition zone biopsy | Not specified |
| Rouviere a [20] | France | 2016 | Prosp | 30 | 30 | Planned RP | 63 (median) | 6.5 (median) | 42 (median) | Whole mount RP histopathology | Gleason score of 5 or greater. |
| Rouviere b [20] | |||||||||||
| Prosch a [23] | Germany | 2016 | Prosp | 10 | 10 | Patients who received SWE investigation and treated with RP based on TRUS guided biopsy results. | 61.5 | 7.2 | 32.6 | SB | Gleason score of 6 or greater. |
| Prosch b [23] | Whole-mount RP histopathology | ||||||||||
| Wei [24] | United Kingdom | 2018 | Prosp | 212 | 212 | Confirmed PCa on SB and imaging (≤cT2) and scheduled for LRP. | 67.6 | 11.8 | 66.9 | Whole-mount RP histopathology | Gleason score greater than 6 and cancer burden greater than 5 mm. |
| Mannaerts [25] | Netherlands, Germany | 2019 | Prosp | 48 | 48 | PCa proven on biopsy with PSA ≤ 20 ng/mL and no extracapsular disease on DRE. Men who underwent PCa therapy or have contraindication to CEUS were excluded. | 65 (median) | 7.7 (median) | 40.0 (median) | Whole-mount RP histopathology | Gleason score of 7 or greater and at least 0.5 ml tumour volume. |
| Xiang [9] | China | 2019 | Retrosp | 367 | 135 | Patients who underwent transperineal prostate biopsy (PSA > 10 ng/mL, increasing PSA levels by 0.75 ng/mL/year, or abnormal DRE). Excluded if they did not undergo MRI or SWE, or if PSA > 100 ng/mL | 66.9 | 16.1 | 44.6 | SB | Gleason score of 7 or greater. |
| Zhang b [10] | China | 2019 | Prosp | 78 | 38 | Planned SB (PSA > 4 ng/mL or increasing PSA levels by 0.50 ng/mL/year, and interval between prostate biopsy and TRUS and MRI examination < 1 week). Malignant PCa group included only stage 2a or lower based on histopathology. | 66.3 | 18.2 | 52.4 | -SB | Gleason score of 6 or greater. |
| Ji [26] | China | 2019 | Prosp | 215 | 113 | Patients with abnormal PSA, a nodule palpated on DRE, or one or more nodules on TRUS and MRI. Excluded if have a history of prostate biopsy/surgery or received endocrine therapy. | 71.3 | NS | NS | SB | Not specified |
| Fu [27] | China | 2020 | Prosp | 221 | 85 | Patients with elevated serum PSA level (>4 ng/mL), palpable nodular lesion in DRE, abnormal TRUS, or MRI finding. | 68.8 | 5.0 | 52.4 | -SWE-targeted biopsy -SB | Gleason score of 7 or greater and/or % cancer greater than 50% |
| First Author | Year | SWE Ultrasound System | Plane of Scan | QAB Size (mm) | SWE Focus Region | No. of SWE Readings/Patient | Total SWE Readings | Blinded | SWE Cut-Off Value (kPa) | Analyses Performed |
|---|---|---|---|---|---|---|---|---|---|---|
| Zheng [14] | 2012 | Acuson S2000 | NS | 10 × 5 | Whole prostate | NS | 209 | Y | 2.5 m/s | Sample level |
| Barr [15] | 2012 | Aixplorer | Axial and transverse | 6 | PZ | 6 | 318 | Y | 37.0 | Sample level |
| Ahmad a [21] | 2013 | Aixplorer | Axial and Sagittal | NS | Whole prostate | 12 | 485 | Y | NS | Sample level |
| Ahmad b [21] | 141 | |||||||||
| Woo [16] | 2014 | Aixplorer | Axial and Sagittal | 5 | Whole prostate | 12 | 1058 | Y | 43.9 | Sample level |
| Correas [19] | 2015 | Aixplorer | Transverse | 3–7 | PZ | 12 | 1040 | Y | 35.0 | Sample and participant level |
| Boehm a [17] | 2015 | Aixplorer | NS | NS | Whole prostate | 12 | 322 | Y | 50.0 | Sample level |
| Zhang a [22] | 2015 | Aixplorer | NS | NS | Whole prostate | NS | NS | Y | 28.5 | Sample level |
| Boehm b [18] | 2015 | Aixplorer | NS | NS | PZ | NS | NS | Y | 50.0 | Participant level |
| Rouviere a [20] | 2016 | Aixplorer | Axial | NS | PZ | NS | 251 | Y | 45.0 | Sample level |
| Rouviere b [20] | Sagittal | 52 | 52.0 | |||||||
| Prosch a [23] | 2016 | Aixplorer | Transverse | NS | Whole prostate | 12 | 120 | NS | 50.0 | Sample level |
| Prosch b [23] | ||||||||||
| Wei [24] | 2018 | Aixplorer | Axial and Sagittal | 4–6 | Whole prostate | 12 | 2544 | Y | 82.6 | Sample level |
| Mannaerts [25] | 2019 | Aixplorer | Transverse | NS | Whole prostate | 12 | 576 | Y | 50.0 | Sample level |
| Xiang [9] | 2019 | Aixplorer | Transverse | 3–5 | PZ | 6 | NS | Y | 40.8 | Sample level |
| Zhang b [10] | 2019 | Aixplorer | Transverse | NS | Whole prostate | NS | NS | Y | NS | Participant level |
| Ji [26] | 2019 | Aixplorer | Transverse | NS | Whole prostate | 6 | NS | Y | 62.3 | Participant level |
| Fu [27] | 2020 | Aixplorer | NS | 3–7 | Whole prostate | 6 | 2749 | Y | 42.0 | Sample and participant level |
| Variable | SB as Reference | Whole-Mount RP Histopathology as Reference | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Covariate | No. of Studies | Pooled Sensitivity (95% CI) | p-Value | Pooled Specificity (95% CI) | p-Value | Number of Studies | Pooled Sensitivity (95% CI) | p-Value | Pooled Specificity (95% CI) | p-Value |
| Study design | ||||||||||
| Prospective | 5 | 0.90 (0.82–0.95) | 0.038 | 0.87 (0.72–0.95) | 0.487 | 5 | 0.71 (0.55–0.83) | - | 0.74 (0.42–0.92) | - |
| Retrospective | 4 | 0.73 (0.51–0.88) | 0.81 (0.68–0.89) | 0 | - | - | ||||
| csPCa definition used | ||||||||||
| Yes | 2 | 0.82 (0.74–0.88) | 0.732 | 0.79 (0.43–0.94) | 0.557 | 3 | 0.77 (0.53–0.91) | 0.309 | 0.84 (0.42–0.97) | 0.292 |
| No/Unspecified | 7 | 0.86 (0.72–0.94) | 0.85 (0.75–0.92) | 2 | 0.62 (0.53–0.70) | 0.53 (0.21–0.83) | ||||
| SWE focus region | ||||||||||
| Whole gland | 6 | 0.81 (0.67–0.90) | 0.161 | 0.84 (0.73–0.91) | 0.879 | 4 | 0.74 (0.54–0.87) | 0.566 | 0.75 (0.34–0.94) | 0.915 |
| PZ only | 3 | 0.94 (0.74–0.99) | 0.86 (0.56–0.96) | 1 | 0.61 (0.50–0.72) | 0.70 (0.64–0.77) | ||||
| Year of publication | ||||||||||
| 2011–2015 | 6 | 0.88 (0.73–0.93) | 0.407 | 0.88 (0.83–0.92) | 0.027 | 1 | 0.81 (0.74–0.87) | 0.495 | 0.69 (0.62–0.75) | 0.877 |
| 2016–2020 | 3 | 0.79 (0.70–0.86) | 0.69 (0.30–0.96) | 4 | 0.68 (0.47–0.84) | 0.75 (0.35–0.94) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anbarasan, T.; Wei, C.; Bamber, J.C.; Barr, R.G.; Nabi, G. Characterisation of Prostate Lesions Using Transrectal Shear Wave Elastography (SWE) Ultrasound Imaging: A Systematic Review. Cancers 2021, 13, 122. https://doi.org/10.3390/cancers13010122
Anbarasan T, Wei C, Bamber JC, Barr RG, Nabi G. Characterisation of Prostate Lesions Using Transrectal Shear Wave Elastography (SWE) Ultrasound Imaging: A Systematic Review. Cancers. 2021; 13(1):122. https://doi.org/10.3390/cancers13010122
Chicago/Turabian StyleAnbarasan, Thineskrishna, Cheng Wei, Jeffrey C. Bamber, Richard G. Barr, and Ghulam Nabi. 2021. "Characterisation of Prostate Lesions Using Transrectal Shear Wave Elastography (SWE) Ultrasound Imaging: A Systematic Review" Cancers 13, no. 1: 122. https://doi.org/10.3390/cancers13010122