FDG-PET Imaging for Hodgkin and Diffuse Large B-Cell Lymphoma—An Updated Overview

 ,
,  ,
,
Abstract
:1. Introduction
2. Initial Staging
2.1. Hodgkin Lymphoma
2.2. DLBCL
3. Early Response Assessment
3.1. Hodgkin Lymphoma
3.2. DLBCL
4. Late Response Evaluation
4.1. Hodgkin Lymphoma
4.2. DLBCL
5. Recent Advances and Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2019; Available online: https://seer.cancer.gov/csr/1975_2016/ (accessed on 19 November 2019).
- Eichenauer, D.A.; Aleman, B.M.P.; André, M.P.E.; Federico, M.; Hutchings, M.; Illidge, T.; Engert, A.; Ladetto, M. Hodgkin lymphoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv19–iv29. [Google Scholar] [CrossRef] [PubMed]
- Engert, A.; Plütschow, A.; Eich, H.T.; Lohri, A.; Dörken, B.; Borchmann, P.; Berger, B.; Greil, R.; Willborn, K.C.; Wilhelm, M.; et al. Reduced treatment intensity in patients with early-stage Hodgkin’s lymphoma. N. Engl. J. Med. 2010, 363, 640–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- André, M.P.E.; Girinsky, T.; Federico, M.; Reman, O.; Fortpied, C.; Gotti, M.; Casasnovas, O.; Brice, P.; van der Maazen, R.; Re, A.; et al. Early positron emission tomography response-adapted treatment in stage I and II Hodgkin lymphoma: Final results of the randomized EORTC/LYSA/FIL H10 trial. J. Clin. Oncol. 2017, 35, 1786–1794. [Google Scholar] [CrossRef]
- Gordon, L.I.; Hong, F.; Fisher, R.I.; Bartlett, N.L.; Connors, J.M.; Gascoyne, R.D.; Wagner, H.; Stiff, P.J.; Cheson, B.D.; Gospodarowicz, M.; et al. Randomized phase III trial of ABVD versus Stanford V with or without radiation therapy in locally extensive and advanced-stage Hodgkin lymphoma: An intergroup study coordinated by the Eastern Cooperative Oncology Group (E2496). J. Clin. Oncol. 2013, 31, 684–691. [Google Scholar] [CrossRef] [Green Version]
- Johnson, P.; Federico, M.; Kirkwood, A.; Fosså, A.; Berkahn, L.; Carella, A.; d’Amore, F.; Enblad, G.; Franceschetto, A.; Fulham, M.; et al. Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin’s Lymphoma. N. Engl. J. Med. 2016, 374, 2419–2429. [Google Scholar] [CrossRef] [PubMed]
- Borchmann, P.; Goergen, H.; Kobe, C.; Lohri, A.; Greil, R.; Eichenauer, D.A.; Zijlstra, J.M.; Markova, J.; Meissner, J.; Feuring-Buske, M.; et al. PET-guided treatment in patients with advanced-stage Hodgkin’s lymphoma (HD18): Final results of an open-label, international, randomised phase 3 trial by the German Hodgkin Study Group. Lancet 2018, 390, 2790–2802. [Google Scholar] [CrossRef]
- Kreissl, S.; Goergen, H.; Müller, H.; Meissner, J.; Mehnert, A.; Bürkle, C.; Fuchs, M.; Engert, A.; Behringer, K.; Borchmann, P. Survivors’ perspectives on risks and benefits of Hodgkin lymphoma treatment: Results of a survey by the German Hodgkin Study Group. Leuk. Lymphoma 2019, 60, 1389–1398. [Google Scholar] [CrossRef]
- Skoetz, N.; Trelle, S.; Rancea, M.; Haverkamp, H.; Diehl, V.; Engert, A.; Borchmann, P. Effect of initial treatment strategy on survival of patients with advanced-stage Hodgkin’s lymphoma: A systematic review and network meta-analysis. Lancet Oncol. 2013, 14, 943–952. [Google Scholar] [CrossRef]
- Steidl, C.; Connors, J.M.; Gascoyne, R.D. Molecular pathogenesis of Hodgkin’s lymphoma: Increasing evidence of the importance of the microenvironment. J. Clin. Oncol. 2011, 29, 1812–1826. [Google Scholar] [CrossRef]
- Liu, W.R.; Shipp, M.A. Signaling pathways and immune evasion mechanisms in classical Hodgkin lymphoma. Hematol. Am. Soc. Hematol. Educ. Program 2017, 2017, 310–316. [Google Scholar] [CrossRef] [Green Version]
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J.; Arber, D.A.; Hasserjian, R.P.; Le Beau, M.M.; et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, Review, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2017. [Google Scholar]
- Gómez León, N.; Delgado-Bolton, R.C.; Del Campo Del Val, L.; Cabezas, B.; Arranz, R.; García, M.; Cannata, J.; González Ortega, S.; Pérez Sáez, M.Á.; López-Botet, B.; et al. Multicenter comparison of contrast-enhanced FDG PET/CT and 64-slice multi-detector-row CT for initial staging and response evaluation at the end of treatment in patients with lymphoma. Clin. Nucl. Med. 2017, 42, 595–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamot, C.; Klingbiel, D.; Hitz, F.; Renner, C.; Pabst, T.; Driessen, C.; Mey, U.; Pless, M.; Bargetzi, M.; Krasniqi, F.; et al. Final results of a prospective evaluation of the predictive value of interim positron emission tomography in patients with diffuse large B-cell lymphoma treated with R-CHOP-14 (SAKK 38/07). J. Clin. Oncol. 2015, 33, 2523–2529. [Google Scholar] [CrossRef] [PubMed]
- Freeman, C.L.; Savage, K.J.; Villa, D.; Scott, D.W.; Srour, L.; Gerrie, A.S.; Brown, M.J.; Slack, G.W.; Farinha, P.; Skinnider, B.; et al. Long-term results of PET-guided radiation therapy in patients with advanced-stage diffuse large B-cell lymphoma treated with R-CHOP in British Columbia. Blood 2017, 130, 823. [Google Scholar]
- Pfreundschuh, M.; Christofyllakis, K.; Altmann, B.; Ziepert, M.; Haenel, M.; Viardot, A.; Neubauer, A.; Held, A.; Truemper, L.; Schmidt, C.; et al. Radiotherapy to bulky disease PET-negative after immunochemotherapy in elderly DLBCL patients: Results of a planned interim analysis of the first 187 patients with bulky disease treated in the OPTIMAL > 60 study of the DSHNHL. J. Clin. Oncol. 2017, 35, 7506. [Google Scholar] [CrossRef]
- Dührsen, U.; Müller, S.; Hertenstein, B.; Thomssen, H.; Kotzerke, J.; Mesters, R.; Berdel, W.E.; Franzius, C.; Kroschinsky, F.; Weckesser, M.; et al. PETAL trial investigators. Positron emission tomography-guided therapy of aggressive non-Hodgkin lymphomas (PETAL): A multicenter, randomized phase III trial. J. Clin. Oncol. 2018, 36, 2024–2034. [Google Scholar] [CrossRef]
- Hüttmann, A.; Rekowski, J.; Müller, S.P.; Hertenstein, B.; Franzius, C.; Mesters, R.; Weckesser, M.; Kroschinsky, F.; Kotzerke, J.; Ganser, A.; et al. Six versus eight doses of rituximab in patients with aggressive B cell lymphoma receiving six cycles of CHOP: Results from the “Positron Emission Tomography-Guided Therapy of Aggressive Non-Hodgkin Lymphomas” (PETAL) trial. Ann. Hematol. 2019, 98, 897–907. [Google Scholar] [CrossRef]
- Poeschel, V.; Held, G.; Ziepert, M.; Witzens-Harig, M.; Holte, H.; Thurner, L.; Borchmann, P.; Viardot, A.; Soekler, M.; Keller, U.; et al. Four versus six cycles of CHOP chemotherapy in combination with six applications of rituximab in patients with aggressive B-cell lymphoma with favourable prognosis (FLYER): A randomised, phase 3, non-inferiority trial. Lancet 2020, 394, 2271–2281. [Google Scholar] [CrossRef] [Green Version]
- The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma. N. Engl. J. Med. 1993, 329, 987–994. [Google Scholar] [CrossRef]
- Tilly, H.; Gomes da Silva, M.; Vitolo, U.; Jack, A.; Meignan, M.; Lopez-Guillermo, A.; Walewski, J.; André, M.P.E.; Johnson, P.W.; Pfreundschuh, M.; et al. ESMO Guidelines Committee. Diffuse large B-cell lymphoma (DLBCL): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v116–v125. [Google Scholar] [CrossRef]
- Pfreundschuh, M.; Schubert, J.; Ziepert, M.; Schmits, R.; Mohren, M.; Lengfelder, E.; Reiser, M.; Nickenig, C.; Clemens, M.; Peter, N.; et al. German High-Grade Non-Hodgkin Lymphoma Study Group (DSHNHL). Six versus eight cycles of bi-weekly CHOP-14 with or without rituximab in elderly patients with aggressive CD20 + B-cell lymphomas: A randomised controlled trial (RICOVER-60). Lancet Oncol. 2008, 9, 105–116. [Google Scholar] [CrossRef]
- Held, G.; Murawski, N.; Ziepert, M.; Fleckenstein, J.; Pöschel, V.; Zwick, C.; Bittenbring, J.; Hänel, M.; Wilhelm, S.; Schubert, J.; et al. Role of radiotherapy to bulky disease in elderly patients with aggressive B-cell lymphoma. J. Clin. Oncol. 2014, 32, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Carbone, P.P.; Kaplan, H.S.; Musshoff, K.; Smithers, D.W.; Tubiana, M. Report of the committee on Hodgkin’s disease staging classification. Cancer Res. 1971, 31, 1860–1861. [Google Scholar] [PubMed]
- Barrington, S.F.; Kirkwood, A.A.; Franceschetto, A.; Fulham, M.J.; Roberts, T.H.; Almquist, H.; Brun, E.; Hjorthaug, K.; Viney, Z.N.; Pike, L.C.; et al. PET-CT for staging and early response: Results from the response-adapted therapy in advanced Hodgkin lymphoma study. Blood 2016, 127, 1531–1538. [Google Scholar] [CrossRef] [Green Version]
- Moulin-Romsee, G.; Hindié, E.; Cuenca, X.; Brice, P.; Decaudin, D.; Bénamor, M.; Brière, J.; Anitei, M.; Filmont, J.E.; Sibon, D.; et al. 18F-FDG PET/CT bone/bone marrow findings in Hodgkin’s lymphoma may circumvent the use of bone marrow trephine biopsy at diagnosis staging. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1095–1105. [Google Scholar] [CrossRef]
- El-Galaly, T.C.; d’Amore, F.; Mylam, K.J.; de Nully Brown, P.; Bøgsted, M.; Bukh, A.; Specht, L.; Loft, A.; Iyer, V.; Hjorthaug, K.; et al. Routine bone marrow biopsy has little or no therapeutic consequence for positron emission tomography/computed tomography-staged treatment-naïve patients with Hodgkin lymphoma. J. Clin. Oncol. 2012, 30, 4508–4514. [Google Scholar] [CrossRef]
- Weiler-Sagie, M.; Kagna, O.; Dann, E.J.; Ben-Barak, A.; Israel, O. Characterizing bone marrow involvement in Hodgkin’s lymphoma by FDG-PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1133–1140. [Google Scholar] [CrossRef]
- Chen-Liang, T.H.; Martin-Santos, T.; Jerez, A.; Senent, L.; Orero, M.T.; Remigia, M.J.; Muiña, B.; Romera, M.; Fernandez-Muñoz, H.; Raya, J.M.; et al. The role of bone marrow biopsy and FDG-PET/CT in identifying bone marrow infiltration in the initial diagnosis of high grade non-Hodgkin B-cell lymphoma and Hodgkin lymphoma. Accuracy in a multicenter series of 372 patients. Am. J. Hematol. 2015, 90, 686–690. [Google Scholar] [CrossRef]
- Purz, S.; Mauz-Körholz, C.; Körholz, D.; Hasenclever, D.; Krausse, A.; Sorge, I.; Ruschke, K.; Stiefel, M.; Amthauer, H.; Schober, O.; et al. [18F] fluorodeoxyglucose positron emission tomography for detection of bone marrow involvement in children and adolescents with Hodgkin’s lymphoma. J. Clin. Oncol. 2011, 29, 3523–3528. [Google Scholar] [CrossRef]
- Voltin, C.A.; Goergen, H.; Baues, C.; Fuchs, M.; Mettler, J.; Kreissl, S.; Oertl, J.; Klaeser, B.; Moccia, A.; Drzezga, A.; et al. Value of bone marrow biopsy in Hodgkin lymphoma patients staged by FDG PET: Results from the German Hodgkin Study Group trials HD16, HD17, and HD18. Ann. Oncol. 2018, 29, 1926–1931. [Google Scholar] [CrossRef]
- Pedersen, M.A.; Gormsen, L.C.; Kamper, P.; Wassberg, C.; Andersen, M.D.; d’Amore, A.L.; Barrington, S.F.; Johnson, P.; Hamilton-Dutoit, S.; Amini, R.M.; et al. Focal skeletal FDG uptake indicates poor prognosis in cHL regardless of extent and first-line chemotherapy. Br. J. Haematol. 2019, 186, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.; de Klerk, J.M.; Fijnheer, R.; Heggelman, B.G.; Dubois, S.V.; Nievelstein, R.A.; Kwee, T.C. Variety in bone marrow 18F-FDG uptake in Hodgkin lymphoma patients without lymphomatous bone marrow involvement: Does it have an explanation? Nucl. Med. Commun. 2016, 37, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Picardi, M.; Soricelli, A.; Grimaldi, F.; Nicolai, E.; Gallamini, A.; Pane, F. Fused FDG-PET/contrast-enhanced CT detects occult subdiaphragmatic involvement of Hodgkin’s lymphoma thereby identifying patients requiring six cycles of anthracycline-containing chemotherapy and consolidation radiation of spleen. Ann. Oncol. 2011, 22, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Fuertes, S.; Setoain, X.; López-Guillermo, A.; Montserrat, E.; Fuster, D.; Paredes, P.; Lomeña, F.; Pons, F. The value of positron emission tomography/computed tomography (PET/CT) in the staging of diffuse large B-cell lymphoma. Med. Clin. 2007, 129, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Raanani, P.; Shasha, Y.; Perry, C.; Metser, U.; Naparstek, E.; Apter, S.; Nagler, A.; Polliack, A.; Ben-Bassat, I.; Even-Sapir, E. Is CT scan still necessary for staging in Hodgkin and non-Hodgkin lymphoma patients in the PET/CT era? Ann. Oncol. 2006, 17, 117–122. [Google Scholar] [CrossRef]
- Elstrom, R.L.; Leonard, J.P.; Coleman, M.; Brown, R.K. Combined PET and low-dose, noncontrast CT scanning obviates the need for additional diagnostic contrast-enhanced CT scans in patients undergoing staging or restaging for lymphoma. Ann. Oncol. 2008, 19, 1770–1773. [Google Scholar] [CrossRef]
- Cerci, J.J.; Györke, T.; Fanti, S.; Paez, D.; Meneghetti, J.C.; Redondo, F.; Celli, M.; Auewarakul, C.; Rangarajan, V.; Gujral, S.; et al. Combined PET and biopsy evidence of marrow involvement improves prognostic prediction in diffuse large B-cell lymphoma. J. Nucl. Med. 2014, 55, 1591–1597. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.B.; Barrington, S.F.; Mikhaeel, N.G.; Hunt, A.A.; Cameron, L.; Morris, T.; Carr, R. PET-CT staging of DLBCL accurately identifies and provides new insight into the clinical significance of bone marrow involvement. Blood 2013, 122, 61–67. [Google Scholar] [CrossRef]
- Alzahrani, M.; El-Galaly, T.C.; Hutchings, M.; Hansen, J.W.; Loft, A.; Johnsen, H.E.; Iyer, V.; Wilson, D.; Sehn, L.H.; Savage, K.J.; et al. The value of routine bone marrow biopsy in patients with diffuse large B-cell lymphoma staged with PET/CT: A Danish-Canadian study. Ann. Oncol. 2016, 27, 1095–1099. [Google Scholar] [CrossRef]
- Kaddu-Mulindwa, D.; Altmann, B.; Held, G.; Ziepert, M.; Menhart, K.; Grosse, J.; Angel, S.; Stilgenbauer, S.; Pfreundschuh, M.; Herrmann, K.; et al. Role of FDG PET/CT to detect bone marrow involvement in the initial staging of aggressive non-Hodgkin lymphoma. Blood 2019, 134, 2892. [Google Scholar] [CrossRef]
- Meignan, M.; Gallamini, A.; Haioun, C. Report on the First International Workshop on Interim-PET-Scan in Lymphoma. Leuk. Lymphoma 2009, 50, 1257–1260. [Google Scholar] [CrossRef] [PubMed]
- Radford, J.; Illidge, T.; Counsell, N.; Hancock, B.; Pettengell, R.; Johnson, P.; Wimperis, J.; Culligan, D.; Popova, B.; Smith, P.; et al. Results of a trial of PET-directed therapy for early-stage Hodgkin’s lymphoma. N. Engl. J. Med. 2015, 372, 1598–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, M.; Goergen, H.; Kobe, C.; Kuhnert, G.; Lohri, A.; Greil, R.; Sasse, S.; Topp, M.S.; Schäfer, E.; Hertenstein, B.; et al. Positron emission tomography-guided treatment in early-stage favorable hodgkin lymphoma: Final results of the international, randomized phase III HD16 trial by the German Hodgkin Study Group. J. Clin. Oncol. 2019, 37, 2835–2845. [Google Scholar] [CrossRef] [PubMed]
- Gallamini, A.; Tarella, C.; Viviani, S.; Rossi, A.; Patti, C.; Mulé, A.; Picardi, M.; Romano, A.; Cantonetti, M.; La Nasa, G.; et al. Early chemotherapy intensification with escalated beacopp in patients with advanced-stage Hodgkin lymphoma with a positive interim positron emission tomography/computed tomography scan after two ABVD cycles: Long-term results of the GITIL/FIL HD 0607 trial. J. Clin. Oncol. 2018, 36, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Casasnovas, R.O.; Bouabdallah, R.; Brice, P.; Lazarovici, J.; Ghesquieres, H.; Stamatoullas, A.; Dupuis, J.; Gac, A.C.; Gastinne, T.; Joly, B.; et al. PET-adapted treatment for newly diagnosed advanced Hodgkin lymphoma (AHL2011): A randomised, multicentre, non-inferiority, phase 3 study. Lancet Oncol. 2019, 20, 202–215. [Google Scholar] [CrossRef]
- Kobe, C.; Goergen, H.; Baues, C.; Kuhnert, G.; Voltin, C.A.; Zijlstra, J.; Hoekstra, O.; Mettler, J.; Drzezga, A.; Engert, A.; et al. Outcome-based interpretation of early interim PET in advanced-stage Hodgkin lymphoma. Blood 2018, 132, 2273–2279. [Google Scholar] [CrossRef] [Green Version]
- Sehn, L.H.; Savage, K.J.; Hoskins, P.; Klasa, R.; Shenkier, T.; Gascoyne, R.D.; Voss, N.; Wilson, D.; Connors, J. Limited-stage DLBCL patients with a negative PET scan following three cycles of R-CHOP have an excellent outcome following abbreviated immuno-chemotherapy alone. Ann. Oncol. 2008, 19, 99. [Google Scholar]
- Casasnovas, R.O.; Salles, G.A.; Oberic, L.; Bodet-Milin, C.; Briere, J.; Morschhauser, F.; Tilly, H.; Ribrag, V.; Lamy, T.; Thieblemont, C.; et al. Obinutuzumab versus rituximab in combination with ACVBP-14 or CHOP-14 following a PET-driven strategy in Aa-IPI 1-3 DLBCL patients (<60 years): Third planned interim and final analyses of the gained trial. Blood 2017, 626, 190. [Google Scholar]
- Casasnovas, R.O.; Ysebaert, L.; Thieblemont, C.; Bachy, E.; Feugier, P.; Delmer, A.; Tricot, S.; Gabarre, J.; André, M.P.E.; Fruchart, C.; et al. FDG-PET-driven consolidation strategy in diffuse large B-cell lymphoma: Final results of a randomized phase 2 study. Blood 2017, 130, 1315–1326. [Google Scholar] [CrossRef] [Green Version]
- Eertink, J.J.; Burggraaff, C.N.; Heymans, M.W.; Barrington, S.F.; Mikhaeel, G.; Dührsen, U.; Hüttmann, A.; Ceriani, L.; Zucca, E.; Carr, R.; et al. The optimal timing of interim 18F-FDG PET in diffuse large B-cell lymphoma: An individual patient data meta-analysis by the Petra consortium. Blood 2019, 134, 487. [Google Scholar] [CrossRef]
- Canellos, G.P. Residual mass in lymphoma may not be residual disease. J. Clin. Oncol. 1988, 6, 931–933. [Google Scholar] [CrossRef] [PubMed]
- Jerusalem, G.; Beguin, Y.; Fassotte, M.F.; Najjar, F.; Paulus, P.; Rigo, P.; Fillet, G. Whole-body positron emission tomography using 18F-fluorodeoxyglucose for posttreatment evaluation in Hodgkin’s disease and non-Hodgkin’s lymphoma has higher diagnostic and prognostic value than classical computed tomography scan imaging. Blood 1999, 94, 429–433. [Google Scholar] [CrossRef] [PubMed]
- De Wit, M.; Bohuslavizki, K.H.; Buchert, R.; Bumann, D.; Clausen, M.; Hossfeld, D.K. 18FDG-PET following treatment as valid predictor for disease-free survival in Hodgkin’s lymphoma. Ann. Oncol. 2001, 12, 29–37. [Google Scholar] [CrossRef]
- Spaepen, K.; Stroobants, S.; Dupont, P.; Thomas, J.; Vandenberghe, P.; Balzarini, J.; De Wolf-Peeters, C.; Mortelmans, L.; Verhoef, G. Can positron emission tomography with [18F]-fluorodeoxyglucose after first-line treatment distinguish Hodgkin’s disease patients who need additional therapy from others in whom additional therapy would mean avoidable toxicity? Br. J. Haematol. 2001, 115, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Weihrauch, M.R.; Re, D.; Scheidhauer, K.; Ansén, S.; Dietlein, M.; Bischoff, S.; Bohlen, H.; Wolf, J.; Schicha, H.; Diehl, V.; et al. Thoracic positron emission tomography using 18F-fluorodeoxyglucose for the evaluation of residual mediastinal Hodgkin disease. Blood 2001, 98, 2930–2934. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, N.G.; Taverna, C.; Strobel, K.; Wastl, C.; Kurrer, M.; Hany, T.F. Hodgkin disease: Diagnostic value of FDG PET/CT after first-line therapy—Is biopsy of FDG-avid lesions still needed? Radiology 2007, 244, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Kobe, C.; Dietlein, M.; Franklin, J.; Markova, J.; Lohri, A.; Amthauer, H.; Klutmann, S.; Knapp, W.H.; Zijlstra, J.M.; Bockisch, A.; et al. Positron emission tomography has a high negative predictive value for progression or early relapse for patients with residual disease after first-line chemotherapy in advanced-stage Hodgkin lymphoma. Blood 2008, 112, 3989–3994. [Google Scholar] [CrossRef]
- Markova, J.; Kahraman, D.; Kobe, C.; Skopalova, M.; Mocikova, H.; Klaskova, K.; Dedeckova, K.; Eich, H.T.; Böll, B.; Dietlein, M.; et al. Role of [18F]-fluoro-2-deoxy-D-glucose positron emission tomography in early and late therapy assessment of patients with advanced Hodgkin lymphoma treated with bleomycin, etoposide, adriamycin, cyclophosphamide, vincristine, procarbazine and prednisone. Leuk. Lymphoma 2012, 53, 64–70. [Google Scholar] [CrossRef]
- Jerusalem, G.; Beguin, Y.; Fassotte, M.F.; Belhocine, T.; Hustinx, R.; Rigo, P.; Fillet, G. Early detection of relapse by whole-body positron emission tomography in the follow-up of patients with Hodgkin’s disease. Ann. Oncol. 2003, 14, 123–130. [Google Scholar] [CrossRef]
- Mocikova, H.; Obrtlikova, P.; Vackova, B.; Trneny, M. Positron emission tomography at the end of first-line therapy and during follow-up in patients with Hodgkin lymphoma: A retrospective study. Ann. Oncol. 2010, 21, 1222–1227. [Google Scholar] [CrossRef]
- Zinzani, P.L.; Stefoni, V.; Tani, M.; Fanti, S.; Musuraca, G.; Castellucci, P.; Marchi, E.; Fina, M.; Ambrosini, V.; Pellegrini, C.; et al. Role of [18F] fluorodeoxyglucose positron emission tomography scan in the follow-up of lymphoma. J. Clin. Oncol. 2009, 27, 1781–1787. [Google Scholar] [CrossRef] [PubMed]
- Picardi, M.; Pugliese, N.; Cirillo, M.; Zeppa, P.; Cozzolino, I.; Ciancia, G.; Pettinato, G.; Salvatore, C.; Quintarelli, C.; Pane, F. Advanced-stage Hodgkin lymphoma: US/chest radiography for detection of relapse in patients in first complete remission—A randomized trial of routine surveillance imaging procedures. Radiology 2014, 272, 262–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobe, C.; Kuhnert, G.; Kahraman, D.; Haverkamp, H.; Eich, H.T.; Franke, M.; Persigehl, T.; Klutmann, S.; Amthauer, H.; Bockisch, A.; et al. Assessment of tumor size reduction improves outcome prediction of positron emission tomography/computed tomography after chemotherapy in advanced-stage Hodgkin lymphoma. J. Clin. Oncol. 2014, 32, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Gallamini, A.; Rossi, A.; Patti, C.; Picardi, M.; Romano, A.; Cantonetti, M.; Oppi, S.; Viviani, S.; Bolis, S.; Trentin, L.; et al. Consolidation radiotherapy could be omitted in advanced hodgkin lymphoma with large nodal mass in complete metabolic response after ABVD. Final analysis of the randomized HD0607 trial. Hematol. Oncol. 2019, 37, 99. [Google Scholar] [CrossRef] [Green Version]
- Barrington, S.F.; Phillips, E.H.; Counsell, N.; Hancock, B.; Pettengell, R.; Johnson, P.; Townsend, W.; Culligan, D.; Popova, B.; Clifton-Hadley, L.; et al. Positron emission tomography score has greater prognostic significance than pretreatment risk stratification in early-stage hodgkin lymphoma in the UK RAPID Study. J. Clin. Oncol. 2019, 37, 1732–1741. [Google Scholar] [CrossRef]
- Itti, E.; Meignan, M.; Berriolo-Riedinger, A.; Biggi, A.; Cashen, A.F.; Véra, P.; Tilly, H.; Siegel, B.A.; Gallamini, A.; Casasnovas, R.O.; et al. An international confirmatory study of the prognostic value of early PET/CT in diffuse large B-cell lymphoma: Comparison between Deauville criteria and ΔSUVmax. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1312–1320. [Google Scholar] [CrossRef]
- Rossi, C.; Kanoun, S.; Berriolo-Riedinger, A.; Dygai-Cochet, I.; Humbert, O.; Legouge, C.; Chrétien, M.L.; Bastie, J.N.; Brunotte, F.; Casasnovas, R.O. Interim 18F-FDG PET SUVmax reduction is superior to visual analysis in predicting outcome early in Hodgkin lymphoma patients. J. Nucl. Med. 2014, 55, 569–573. [Google Scholar] [CrossRef] [Green Version]
- Cottereau, A.S.; Versari, A.; Loft, A.; Casasnovas, O.; Bellei, M.; Ricci, R.; Bardet, S.; Castagnoli, A.; Brice, P.; Raemaekers, J.; et al. Prognostic value of baseline metabolic tumor volume in early-stage Hodgkin lymphoma in the standard arm of the H10 trial. Blood 2018, 131, 1456–1463. [Google Scholar] [CrossRef]
- Akhtari, M.; Milgrom, S.A.; Pinnix, C.C.; Reddy, J.P.; Dong, W.; Smith, G.L.; Mawlawi, O.; Abou Yehia, Z.; Gunther, J.; Osborne, E.M.; et al. Reclassifying patients with early-stage Hodgkin lymphoma based on functional radiographic markers at presentation. Blood 2018, 131, 84–94. [Google Scholar] [CrossRef] [Green Version]
- Mettler, J.; Müller, H.; Voltin, C.A.; Baues, C.; Klaeser, B.; Moccia, A.; Borchmann, P.; Engert, A.; Kuhnert, G.; Drzezga, A.; et al. Metabolic tumor volume for response prediction in advanced-stage hodgkin lymphoma. J. Nucl. Med. 2019, 60, 207–211. [Google Scholar] [CrossRef] [Green Version]
- Mikhaeel, N.G.; Smith, D.; Dunn, J.T.; Phillips, M.; Møller, H.; Fields, P.A.; Wrench, D.; Barrington, S.F. Combination of baseline metabolic tumour volume and early response on PET/CT improves progression-free survival prediction in DLBCL. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1209–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitz, C.; Hüttmann, A.; Müller, S.P.; Hanoun, M.; Boellaard, R.; Brinkmann, M.; Jöckel, K.H.; Dührsen, U.; Rekowski, J. Dynamic risk assessment based on positron emission tomography scanning in diffuse large B-cell lymphoma: Post-hoc analysis from the PETAL trial. Eur. J. Cancer 2019, 124, 25–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercellino, L.; Cottereau, A.S.; Casasnovas, R.O.; Tilly, H.; Feugier, P.; Chartier, L.; Fruchart, C.; Roulin, L.; Obéric, L.; Pica, G.M.; et al. High total metabolic tumor volume at baseline allows discrimination of survival even in patients aged 60 to 80 years responding to R-CHOP. Blood 2020. [Google Scholar] [CrossRef] [PubMed]
- Cottereau, A.S.; Nioche, C.; Dirand, A.S.; Clerc, J.; Morschhauser, F.; Casasnovas, O.; Meignan, M.A.; Buvat, I. 18F-FDG-PET dissemination features in diffuse large B cell lymphoma are prognostic of outcome. J. Nucl. Med. 2019, 61, 40–45. [Google Scholar] [CrossRef]
- Barrington, S.F.; Meignan, M. Time to prepare for risk adaptation in lymphoma by standardizing measurement of metabolic tumor burden. J. Nucl. Med. 2019, 60, 1096–1102. [Google Scholar] [CrossRef] [Green Version]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50, 122S–150S. [Google Scholar] [CrossRef] [Green Version]
- Boellaard, R.; Sera, T.; Kaalep, A.; Hoekstra, O.S.; Barrington, S.F.; Zijlstra, J.M. Updating PET/CT performance standards and PET/CT interpretation criteria should go hand in hand. EJNMMI Res. 2019, 9, 95. [Google Scholar] [CrossRef]
- Voltin, C.A.; Mettler, J.; Boellaard, R.; Kuhnert, G.; Dietlein, M.; Borchmann, P.; Drzezga, A.; Kobe, C. Quantitative assessment of 18F-FDG PET in patients with Hodgkin lymphoma: Is it significantly affected by contrast-enhanced computed tomography attenuation correction? Nucl. Med. Commun. 2019, 40, 249–257. [Google Scholar] [CrossRef]
- Bröckelmann, P.J.; Goergen, H.; Keller, U.; Meissner, J.; Ordemann, R.; Halbsguth, T.V.; Sasse, S.; Sökler, M.; Kerkhoff, A.; Mathas, S.; et al. Nivolumab and AVD for Early-Stage Unfavorable Hodgkin Lymphoma (NIVAHL). Blood 2019, 134, 236. [Google Scholar] [CrossRef]
- Younes, A.; Hilden, P.; Coiffier, B.; Hagenbeek, A.; Salles, G.; Wilson, W.; Seymour, J.F.; Kelly, K.; Gribben, J.; Pfreunschuh, M.; et al. International Working Group consensus response evaluation criteria in lymphoma (RECIL 2017). Ann. Oncol. 2017, 28, 1436–1447. [Google Scholar] [CrossRef]
- Verhoeff, S.R.; van den Heuvel, M.M.; van Herpen, C.M.L.; Piet, B.; Aarntzen, E.H.J.G.; Heskamp, S. Programmed cell death-1/Ligand-1 PET imaging: A novel tool to optimize immunotherapy? PET Clin. 2020, 15, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heskamp, S.; Hobo, W.; Molkenboer-Kuenen, J.D.; Olive, D.; Oyen, W.J.; Dolstra, H.; Boerman, O.C. Noninvasive imaging of tumor PD-L1 expression using radiolabeled Anti-PD-L1 antibodies. Cancer Res. 2015, 75, 2928–2936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wester, H.J.; Keller, U.; Schottelius, M.; Beer, A.; Philipp-Abbrederis, K.; Hoffmann, F.; Šimeček, J.; Gerngross, C.; Lassmann, M.; Herrmann, K.; et al. Disclosing the CXCR4 expression in lymphoproliferative diseases by targeted molecular imaging. Theranostics 2015, 5, 618–630. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H.; et al. 68Ga-FAPI PET/CT: Tracer uptake in 28 different kinds of cancer. J. Nucl. Med. 2019, 60, 801–805. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Score | Criteria | Interpretation * |
|---|---|---|
| 1 | No FDG uptake | CR |
| 2 | FDG uptake lower than or equal to the mediastinal blood pool | |
| 3 | FDG uptake higher than the mediastinal blood pool but lower or equal to liver | |
| 4 | FDG uptake moderately increased compared to the liver | PR/SD/PD |
| 5 | FDG uptake markedly increased compared to the liver and/or new sites of disease |
| Threshold | Advantages | Disadvantages |
|---|---|---|
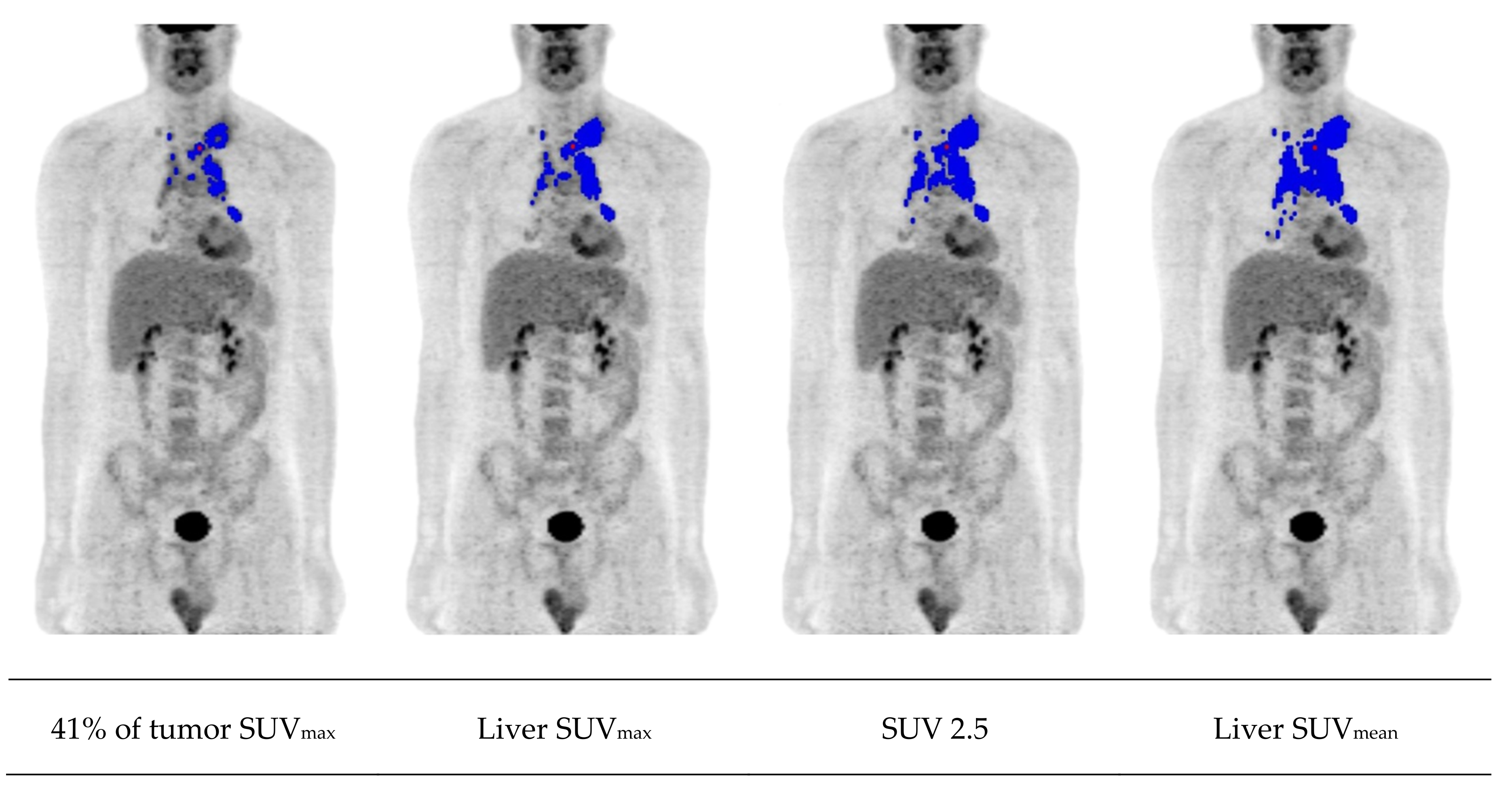
| Fixed absolute (e.g., SUV 2.5 or 4.0) | High reproducibility | Overestimation if tumor lies adjacent to areas of high physiologic uptake |
| Observer-independence | Underestimation in tumors that have many voxels with an uptake less than the threshold | |
| Reference regions (e.g., liver or mediastinum) * | Adjusted to patient and scan | More time-consuming |
| Low availability on commercial software | ||
| Fixed relative (e.g., 41% of tumor SUVmax) | Observer-independence | Overestimation in case of low lesion-to-background ratio |
| Underestimation of tumors with heterogeneous uptake and high SUVmax | ||
| Adaptive (e.g., signal-to-background ratio) | Adjusted to patient and scan | More time-consuming |
| Low availability on commercial software |
| Indication | Hodgkin Lymphoma | DLBCL |
|---|---|---|
| Staging | + + + | + + + |
| Early response assessment | + + | + + |
| End-of-treatment | + + | + + |
| Follow-up | +/- | +/- |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voltin, C.-A.; Mettler, J.; Grosse, J.; Dietlein, M.; Baues, C.; Schmitz, C.; Borchmann, P.; Kobe, C.; Hellwig, D. FDG-PET Imaging for Hodgkin and Diffuse Large B-Cell Lymphoma—An Updated Overview. Cancers 2020, 12, 601. https://doi.org/10.3390/cancers12030601
Voltin C-A, Mettler J, Grosse J, Dietlein M, Baues C, Schmitz C, Borchmann P, Kobe C, Hellwig D. FDG-PET Imaging for Hodgkin and Diffuse Large B-Cell Lymphoma—An Updated Overview. Cancers. 2020; 12(3):601. https://doi.org/10.3390/cancers12030601
Chicago/Turabian StyleVoltin, Conrad-Amadeus, Jasmin Mettler, Jirka Grosse, Markus Dietlein, Christian Baues, Christine Schmitz, Peter Borchmann, Carsten Kobe, and Dirk Hellwig. 2020. "FDG-PET Imaging for Hodgkin and Diffuse Large B-Cell Lymphoma—An Updated Overview" Cancers 12, no. 3: 601. https://doi.org/10.3390/cancers12030601