Expression of GP88 (Progranulin) Protein Is an Independent Prognostic Factor in Prostate Cancer Patients


 ,
,  and
and
Abstract
:1. Introduction
2. Results
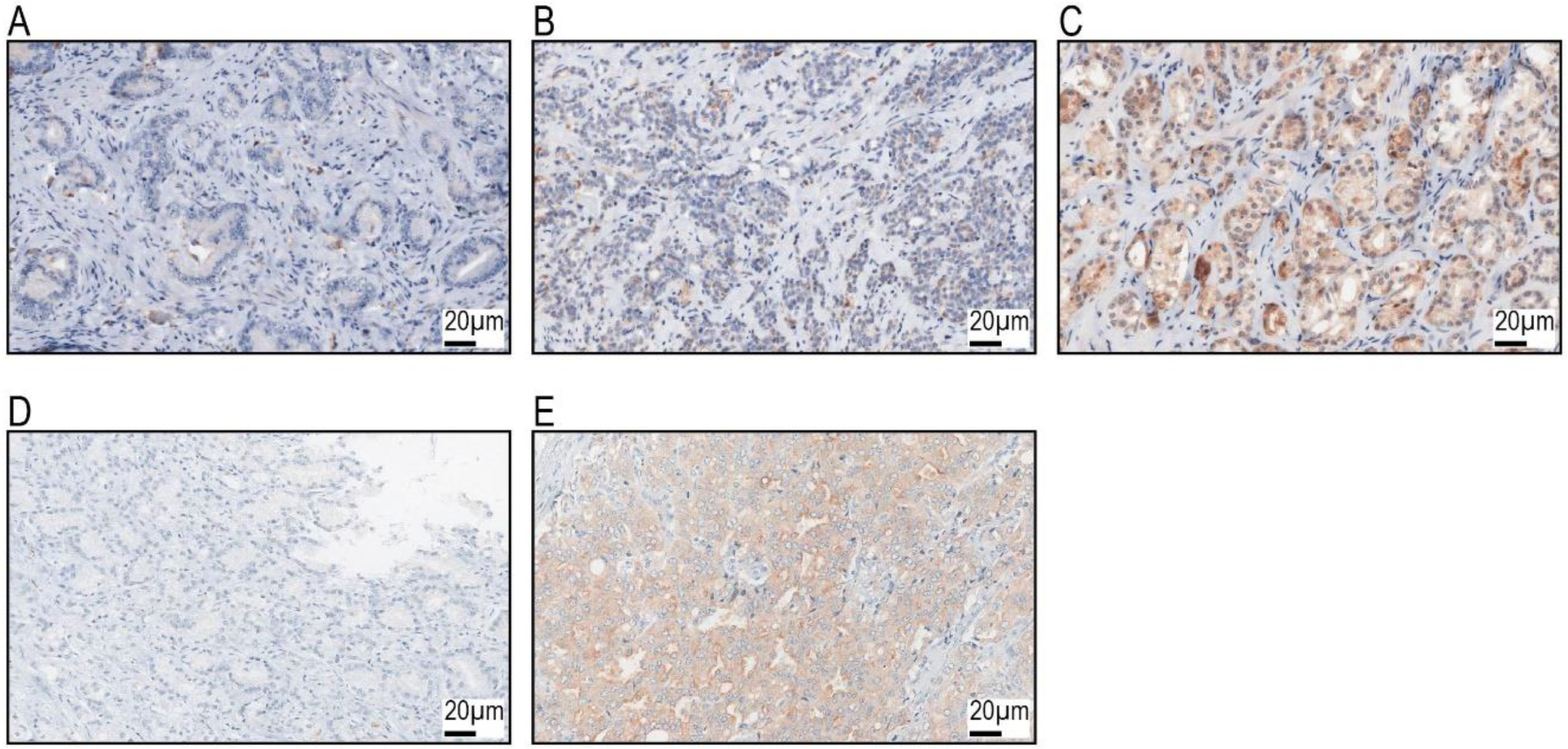
2.1. GP88 Expression and Correlation with Clinico-Pathological Parameters and the Expression of Selected Proteins
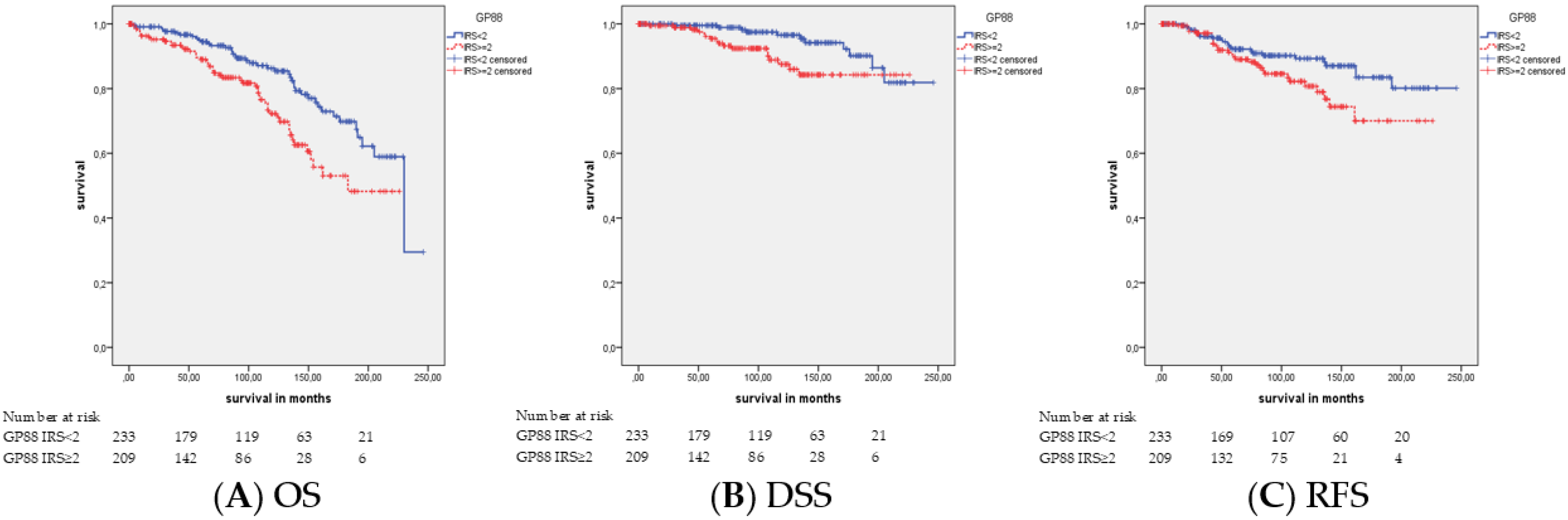
2.2. Association of GP88 Protein Expression and Survival
2.3. Association of GP88 Protein Expression and Survival Stratified by Tumor Stage
2.4. Association of GP88 Protein Expression and Survival Stratified by Gleason Score
2.5. Association of GP88 Protein Expression and Survival Stratified by Patient’s Age
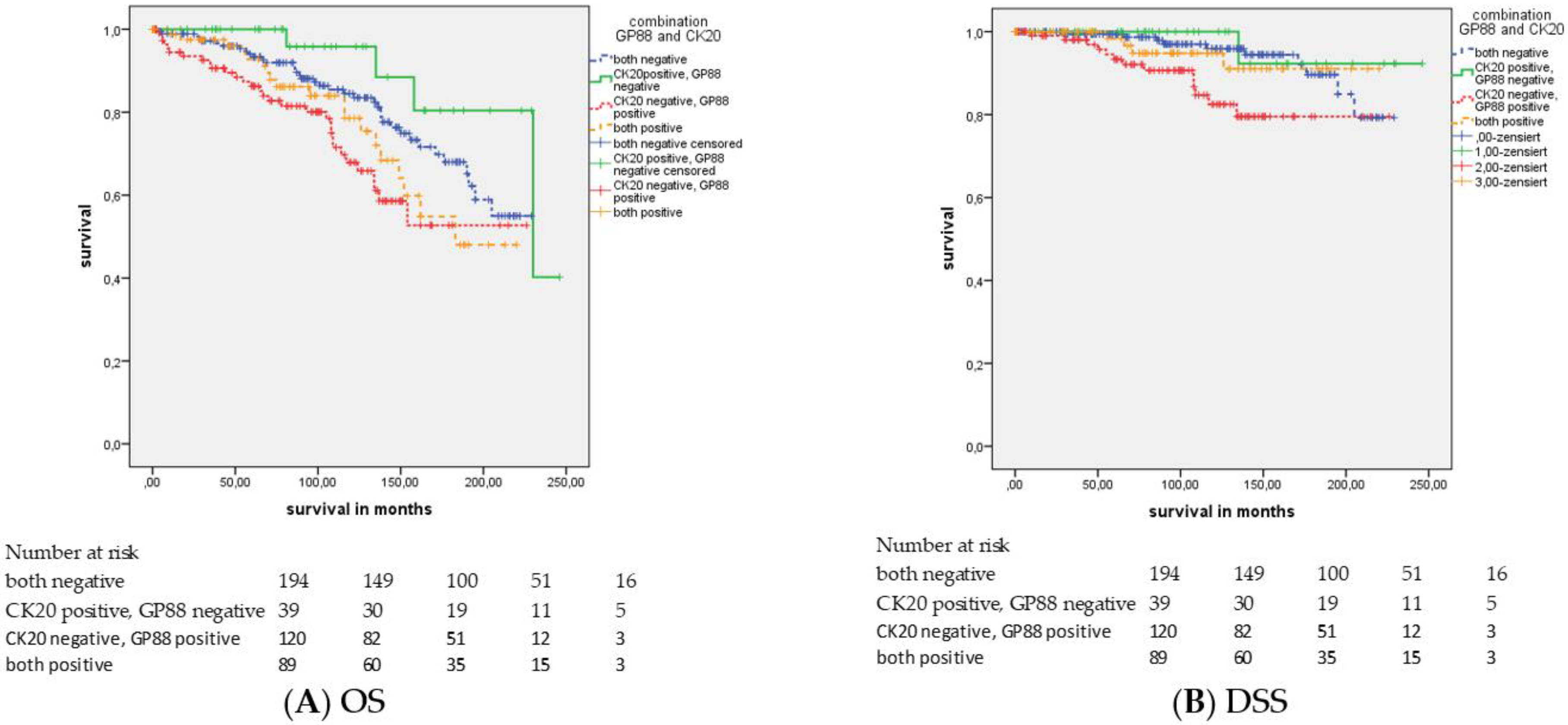
2.6. Association of GP88 Protein Expression and Survival Stratified by CK20 Staining
3. Discussion
4. Material and Methods
4.1. Patients and Tumor Material
4.2. Immunohistochemistry
4.3. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| PCa | prostate cancer |
| TMA | tissue microarray |
| OS | overall survival |
| DSS | disease-free survival |
| RFS | relapse-free survival |
| IHC | immunohistochemistry |
| pT | pathological tumor stage |
| pN | pathological lymph node stage |
| GS | Gleason score |
| IRS | immunoreactive score |
| n.s. | nonsignificant |
| n.d. | not determined |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.K.; Check, D.P.; Lortet-Tieulent, J.; Laversanne, M.; Jemal, A.; Ferlay, J.; Bray, F.; Cook, M.B.; Devesa, S.S. Prostate cancer incidence in 43 populations worldwide: An analysis of time trends overall and by age group. Int. J. Cancer 2016, 138, 1388–1400. [Google Scholar] [CrossRef] [PubMed]
- Inamura, K. Prostatic cancers: Understanding their molecular pathology and the 2016 WHO classification. Oncotarget 2018, 9, 14723–14737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, S.G.; Chang, S.L.; Erho, N.; Yu, M.; Lehrer, J.; Alshalalfa, M.; Speers, C.; Cooperberg, M.R.; Kim, W.; Ryan, C.J.; et al. Associations of luminal and basal subtyping of prostate cancer with prognosis and response to androgen deprivation therapy. JAMA Oncol. 2017, 3, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.G.; Chen, W.S.; Das, R.; Chang, S.L.; Tomlins, S.A.; Chou, J.; Quigley, D.A.; Dang, H.X.; Barnard, T.J.; Mahal, B.A.; et al. Clinical and genomic implications of luminal and basal subtypes across carcinomas. Clin. Cancer Res. 2019, 25, 2450–2457. [Google Scholar] [CrossRef]
- McGrath, S.; Christidis, D.; Perera, M.; Hong, S.K.; Manning, T.; Vela, I.; Lawrentschuk, N. Prostate cancer biomarkers: Are we hitting the mark? Prostate Int. 2016, 4, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Zapała, P.; Dybowski, B.; Poletajew, S.; Radziszewski, P. What can be expected from prostate cancer biomarkers a clinical perspective. Urol. Int. 2018, 100, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Anceschi, U.; Tuderti, G.; Lugnani, F.; Biava, P.M.; Malossini, G.; Luciani, L.; Cai, T.; Marsiliani, D.; Filianoti, A.; Mattevi, D.; et al. Novel diagnostic biomarkers of prostate cancer: An update. Curr. Med. Chem. 2019, 26, 1045–1058. [Google Scholar] [CrossRef]
- Kohaar, I.; Petrovics, G.; Srivastava, S. A rich array of prostate cancer molecular biomarkers: Opportunities and challenges. Int. J. Mol. Sci. 2019, 20, 1813. [Google Scholar] [CrossRef] [Green Version]
- Bhandari, V.; Bateman, A. Structure and chromosomal location of the human granulin gene. Biochem. Biophys. Res. Commun. 1992, 188, 57–63. [Google Scholar] [CrossRef]
- Serrero, G. Potential of theranostic target mining in the development of novel diagnostic and therapeutic products in oncology: Progranulin/GP88 as a therapeutic and diagnostic target for breast and lung cancers. Rinsho Byori 2016, 64, 1296–1309. [Google Scholar] [PubMed]
- Lovat, F.; Bitto, A.; Xu, S.Q.; Fassan, M.; Goldoni, S.; Metalli, D.; Wubah, V.; McCue, P.; Serrero, G.; Gomella, L.G.; et al. Proepithelin is an autocrine growth factor for bladder cancer. Carcinogenesis 2009, 30, 861–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrero, G.; Ioffe, O.B. Expression of PC-cell-derived growth factor in benign and malignant human breast epithelium. Hum. Pathol. 2003, 34, 1148–1154. [Google Scholar] [CrossRef]
- Serrero, G.; Hawkins, D.M.; Yue, B.; Ioffe, O.; Bejarano, P.; Phillips, J.T.; Head, J.F.; Elliott, R.L.; Tkaczuk, K.R.; Godwin, A.K.; et al. Progranulin (GP88) tumor tissue expression is associated with increased risk of recurrence in breast cancer patients diagnosed with estrogen receptor positive invasive ductal carcinoma. Breast. Cancer Res. 2012, 14, R26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edelman, M.J.; Feliciano, J.; Yue, B.; Bejarano, P.; Ioffe, O.; Reisman, D.; Hawkins, D.; Gai, Q.; Hicks, D.; Serrero, G. GP88 (progranulin): A novel tissue and circulating biomarker for non-small cell lung carcinoma. Hum. Pathol. 2014, 45, 1893–1899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, Y.; Goto, N.; Takemura, M.; Yamasuge, W.; Yabe, K.; Takami, T.; Miyazaki, T.; Takeuchi, T.; Shiraki, M.; Shimizu, M.; et al. Association between increased serum GP88 (progranulin) concentrations and prognosis in patients with malignant lymphomas. Clin. Chim. Acta 2017, 473, 139–146. [Google Scholar] [CrossRef]
- Pan, C.X.; Kinch, M.S.; Kiener, P.A.; Langermann, S.; Serrero, G.; Sun, L.; Corvera, J.; Sweeney, C.J.; Li, L.; Zhang, S.; et al. PC cell-derived growth factor expression in prostatic intraepithelial neoplasia and prostatic adenocarcinoma. Clin. Cancer Res. 2004, 10, 1333–1337. [Google Scholar] [CrossRef] [Green Version]
- Monami, G.; Emiliozzi, V.; Bitto, A.; Lovat, F.; Xu, S.Q.; Goldoni, S.; Fassan, M.; Serrero, G.; Gomella, L.G.; Baffa, R.; et al. Proepithelin regulates prostate cancer cell biology by promoting cell growth, migration, and anchorageindependent growth. Am. J. Pathol. 2009, 174, 1037–1047. [Google Scholar] [CrossRef] [Green Version]
- Greither, T.; Fischer, K.; Theil, G.; Marcou, M.; Holzhausen, H.J.; Weigelt, K.; Serrero, G.; Hicks, D.; Yue, B.; Fornara, P.; et al. Expression of GP88 (progranulin) in serum of prostate cancer patients is associated with Gleason scores and overall survival. Cancer Manag. Res. 2018, 10, 4173–4180. [Google Scholar] [CrossRef] [Green Version]
- Tangkeangsirisin, W.; Serrero, G. PC cell-derived growth factor (PCDGF/GP88, progranulin) stimulates migration, invasiveness and VEGF expression in breast cancer cells. Carcinogenesis 2004, 25, 1587–1592. [Google Scholar] [CrossRef]
- He, Z.; Ismail, A.; Kriazhev, L.; Sadvakassova, G.; Bateman, A. Progranulin (PC-cell-derived growth factor/acrogranin) regulates invasion and cell survival. Cancer Res. 2002, 62, 5590–5596. [Google Scholar] [PubMed]
- Grant, G.M.; Giambernardi, T.A.; Grant, A.M.; Klebe, R.J. Overview of expression of matrix metalloproteinases (MMP-17, MMP-18, and MMP-20) in cultured human cells. Matrix Biol. 1999, 18, 145–148. [Google Scholar] [CrossRef]
- Escaff, S.; Fernández, J.M.; González, L.O.; Suárez, A.; González-Reyes, S.; González, J.M.; Vizoso, F.J. Study of matrix metalloproteinases and their inhibitors in prostate cancer. Br. J. Cancer 2010, 102, 922–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.E.; Yue, B.; Serrero, G. Signaling pathway of GP88 (Progranulin) in breast cancer cells: Upregulation and phosphorylation of c-myc by GP88/Progranulin in Her2-overexpressing breast cancer cells. Breast Cancer (Auckl) 2016, 9, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Ouyang, X.; Banach-Petrosky, W.A.; Shen, M.M.; Abate-Shen, C. Emergence of androgen independence at early stages of prostate cancer progression in Nkx3.1; Pten mice. Cancer Res. 2006, 66, 7929–7933. [Google Scholar] [CrossRef] [Green Version]
- Carver, B.S.; Chapinski, C.; Wongvipat, J.; Hieronymus, H.; Chen, Y.; Chandarlapaty, S.; Arora, V.K.; Le, C.; Koutcher, J.; Scher, H.; et al. Reciprocal feedback regulation of PI3K and androgen receptor signaling in PTEN-deficient prostate cancer. Cancer Cell 2011, 19, 575–586. [Google Scholar] [CrossRef] [Green Version]
- Mulholland, D.J.; Tran, L.M.; Li, Y.; Cai, H.; Morim, A.; Wang, S.; Plaisier, S.; Garraway, I.P.; Huang, J.; Graeber, T.G.; et al. Cell autonomous role of PTEN in regulating castration-resistant prostate cancer growth. Cancer Cell 2011, 19, 792–804. [Google Scholar] [CrossRef] [Green Version]
- Nickols, N.G.; Nazarian, R.; Zhao, S.G.; Tan, V.; Uzunangelov, V.; Xia, Z.; Baertsch, R.; Neeman, E.; Gao, A.C.; Thomas, G.V.; et al. MEK-ERK signaling is a therapeutic target in metastatic castration resistant prostate cancer. Prostate Cancer Prostatic Dis. 2019, 22, 531–538. [Google Scholar] [CrossRef]
- Hawksworth, D.; Ravindranath, L.; Chen, Y.; Furusato, B.; Sesterhenn, I.A.; McLeod, D.G.; Srivastava, S.; Petrovics, G. Overexpression of C-MYC oncogene in prostate cancer predicts biochemical recurrence. Prostate Cancer Prostatic Dis. 2010, 13, 311–315. [Google Scholar] [CrossRef] [Green Version]
- Tatarov, O.; Mitchell, T.J.; Seywright, M.; Leung, H.Y.; Brunton, V.G.; Edwards, J. SRC family kinase activity is up-regulated in hormone-refractory prostate cancer. Clin. Cancer Res. 2009, 15, 3540–3549. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Serrero, G. Inhibition of PC cell-derived growth factor (PCDGF, epithelin/granulin precursor) expression by antisense PCDGF cDNA transfection inhibits tumorigenicity of the human breast carcinoma cell line MDA-MB-468. Proc. Natl. Acad. Sci. USA 2000, 97, 3993–3998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buraschi, S.; Xu, S.Q.; Stefanello, M.; Moskalev, I.; Morcavallo, A.; Genua, M.; Tanimoto, R.; Birbe, R.; Peiper, S.C.; Gomella, L.G.; et al. Suppression of progranulin expression inhibits bladder cancer growth and sensitizes cancer cells to cisplatin. Oncotarget 2016, 7, 39980–39995. [Google Scholar] [CrossRef] [PubMed]
- Wong, N.C.; Cheung, P.F.; Yip, C.W.; Chan, K.F.; Ng, I.O.; Fan, S.T.; Cheung, S.T. Antibody against granulin-epithelin precursor sensitizes hepatocellular carcinoma to chemotherapeutic agents. Mol. Cancer Ther. 2014, 13, 3001–3012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckstein, M.; Jung, R.; Weigelt, K.; Sikic, D.; Stöhr, R.; Geppert, C.; Agaimy, A.; Lieb, V.; Hartmann, A.; Wullich, B.; et al. Piwi-like 1 and-2 protein expression levels are prognostic factors for muscle invasive urothelial bladder cancer patients. Sci. Rep. 2018, 8, 17693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taubert, H.; Wach, S.; Jung, R.; Pugia, M.; Keck, B.; Bertz, S.; Nolte, E.; Stoehr, R.; Lehmann, J.; Ohlmann, C.H.; et al. Piwil 2 expression is correlated with disease-specific and progression-free survival of chemotherapy-treated bladder cancer patients. Mol. Med. 2015, 21, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| N | |
|---|---|
| All PCa Patients | 442 |
| Age median in years (range) (IQR) | 65 (45–83) (61–69) |
| Pathological tumor stage (pT) | |
| pT2 | 260 |
| pT3 | 151 |
| pT4 | 31 |
| Gleason score (GS) | |
| GS 6 | 237 |
| GS 7a | 82 |
| GS 7b | 32 |
| GS 8 | 27 |
| GS 9–10 | 34 |
| GS unknown | 30 |
| PSA at prostatectomy (median) (IQR) | (3.54) (0.83–7.46) |
| <4 ng/mL | 194 |
| ≥4 ng/mL | 180 |
| unknown | 68 |
| GP88 staining (median) (IQR) | (1.5) (0–4) |
| IRS < 2 | 233 |
| IRS ≥ 2 | 209 |
| CK20 staining (median) (IQR) | (0) (0–2) |
| IRS < 2 | 314 |
| IRS ≥ 2 | 128 |
| Clinical endpoint | GP88 IRS < 2 | GP88 IRS ≥ 2 | CK20 IRS < 2 | CK20 IRS ≥ 2 | ||
|---|---|---|---|---|---|---|
| Overall survival (OS) | N | N | ||||
| alive | 350 | 191 | 159 | 350 | 245 | 105 |
| dead | 92 | 42 | 50 | 92 | 69 | 23 |
| Disease-specific survival (DSS) | ||||||
| Yes | 414 | 222 | 192 | 414 | 291 | 123 |
| No | 28 | 11 | 17 | 28 | 23 | 5 |
| Relapse-free survival (RFS) | ||||||
| Yes | 389 | 209 | 180 | 389 | 279 | 110 |
| No | 53 | 24 | 29 | 53 | 35 | 18 |
| Kaplan–Meier Analysis | |||||||
|---|---|---|---|---|---|---|---|
| GP88 | N | OS | DSS | RFS | |||
| IRS ≥ 2 vs. IRS < 2 | |||||||
| Months | p | Months | p | Months | p | ||
| All patients | 442 | 164.9 vs. 195.8 | 0.002 | 204.3 vs. 231.1 | 0.018 | 186.4 vs. 218.1 | 0.040 |
| Tumor stage pT2 | 260 | 159.9 vs. 193.4 | 0.020 | 196.1 vs. 220.7 | 0.021 | n.s. | |
| GS7b (GS8*) | 32 | n.d. | 0.004 | n.d. | 0.029 | 99.0 vs. 201.8 | 0.008 |
| Age ≤ 65 years | 230 | 169.5 vs. 227.3 | 0.001 | 186.1 vs. 237.1 | 0.003 | 153.1 vs. 222.8 | 0.004 |
| CK20 IRS < 2 | 314 | 162.9 vs. 186.8 | 0.009 | 197.5 vs. 216.1 | 0.005 | n.s. | |
| Univariate Cox’s Regression Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|
| GP88 | N | OS | DSS | N | RFS | |||
| IRS ≥ 2 vs. IRS < 2 | ||||||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |||
| All patients | 442 | 1.9 (1.2–2.9) | 0.003 | 2.5 (1.1–5.3) | 0.021 | 442 | 1.7 (1.0–3.0) | 0.043 |
| Tumor stage pT2 | 260 | 2.1 (1.1–3.9) | 0.022 | 4.6 (1.2–18.4) | 0.030 | 260 | n.s. | |
| GS7b (GS8*) | 32 | n.s. | n.s. | 27 | 10.2 (1.2–86.4) | 0.033 | ||
| Age ≤ 65 years | 230 | 3.6 (1.6–8.3) | 0.002 | 5.5 (1.6–18.9) | 0.006 | 230 | 2.9 (1.4–6.4) | 0.005 |
| CK20 IRS < 2 | 314 | 1.9 (1.2–3.1) | 0.010 | 3.2 (1.4–7.5) | 0.007 | 314 | n.s. | |
| Multivariate Cox’s Regression Analysis | ||||||||
| GP88 | N | OS | DSS | N | RFS | |||
| IRS ≥ 2 vs. IRS < 2 | ||||||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |||
| All patients | 412 | 1.8 (1.1–2.7) | 0.011 | 2.4 (1.0–5.5) | 0.039 | 412 | 1.7 (1.0–3.1) | 0.046 |
| Tumor stage pT2 | 242 | 1.9 (1.0–3.8) | 0.043 | n.s. | 242 | n.s. | ||
| GS7b (GS8*) | 32 | n.s. | n.s. | 27 | n.s. | |||
| Age ≤ 65 years | 215 | 3.8 (1.5–9.6) | 0.004 | 6.0 (1.6–22.7) | 0.008 | 215 | 3.7 (1.6–8.8) | 0.003 |
| CK20 IRS < 2 | 296 | 1.8 (1.1–3.0) | 0.018 | 2.8 (1.1–7.0) | 0.028 | 296 | n.s. | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdulrahman, A.; Eckstein, M.; Jung, R.; Guzman, J.; Weigelt, K.; Serrero, G.; Yue, B.; Geppert, C.; Stöhr, R.; Hartmann, A.; et al. Expression of GP88 (Progranulin) Protein Is an Independent Prognostic Factor in Prostate Cancer Patients. Cancers 2019, 11, 2029. https://doi.org/10.3390/cancers11122029
Abdulrahman A, Eckstein M, Jung R, Guzman J, Weigelt K, Serrero G, Yue B, Geppert C, Stöhr R, Hartmann A, et al. Expression of GP88 (Progranulin) Protein Is an Independent Prognostic Factor in Prostate Cancer Patients. Cancers. 2019; 11(12):2029. https://doi.org/10.3390/cancers11122029
Chicago/Turabian StyleAbdulrahman, Amer, Markus Eckstein, Rudolf Jung, Juan Guzman, Katrin Weigelt, Ginette Serrero, Binbin Yue, Carol Geppert, Robert Stöhr, Arndt Hartmann, and et al. 2019. "Expression of GP88 (Progranulin) Protein Is an Independent Prognostic Factor in Prostate Cancer Patients" Cancers 11, no. 12: 2029. https://doi.org/10.3390/cancers11122029