Treatment Outcome of 227 Patients with Sinonasal Adenoid Cystic Carcinoma (ACC) after Intensity Modulated Radiotherapy and Active Raster-Scanning Carbon Ion Boost: A 10-Year Single-Center Experience

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods and Materials
2.1. Evaluation
2.2. Patient Characteristics
2.3. Treatment Planning and Treatment Characteristics
2.4. Declarations
3. Results
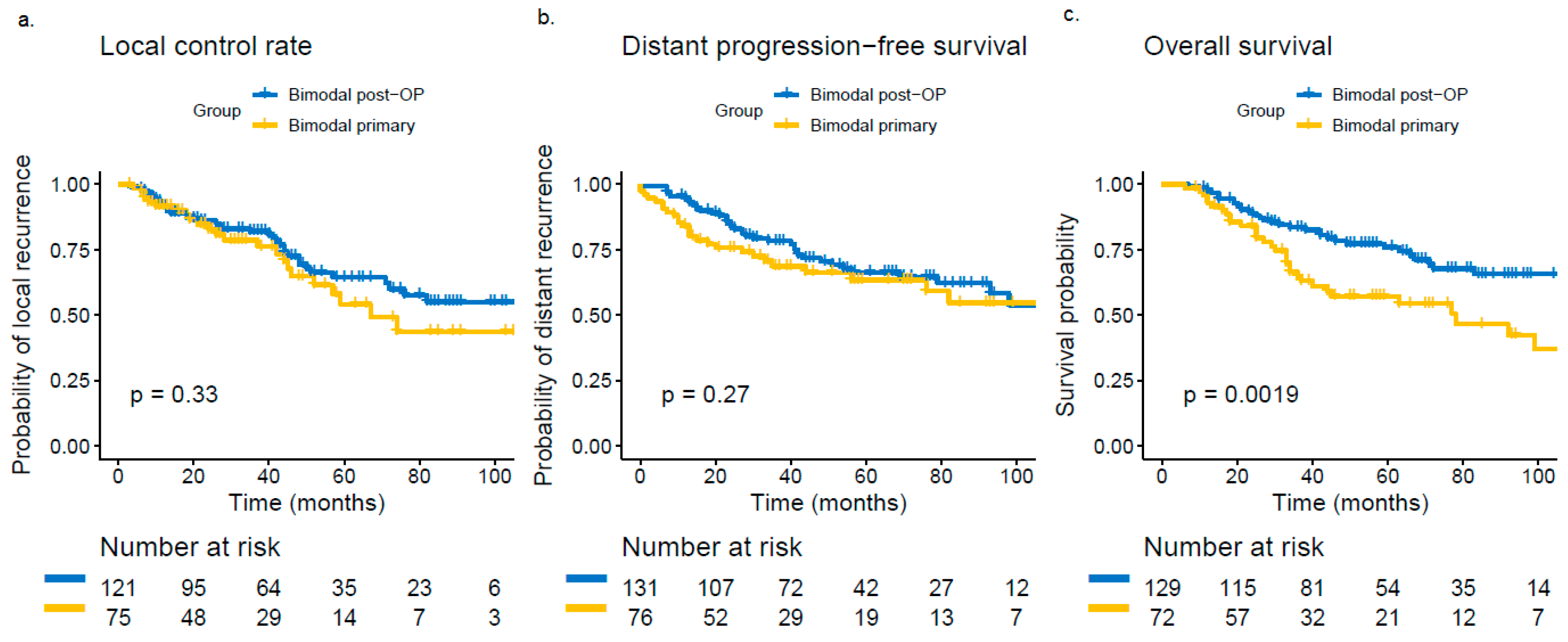
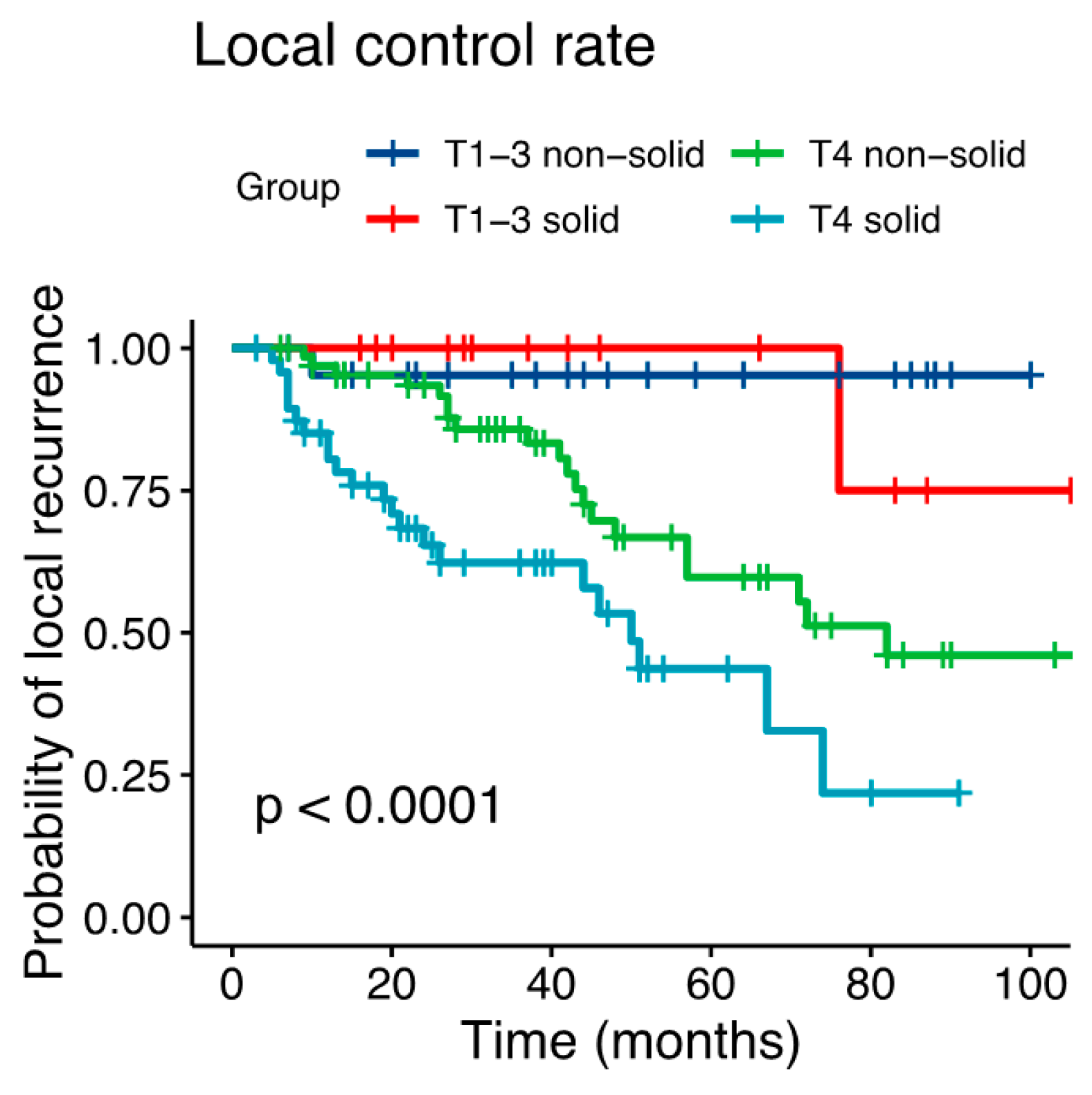
3.1. Failure Patterns
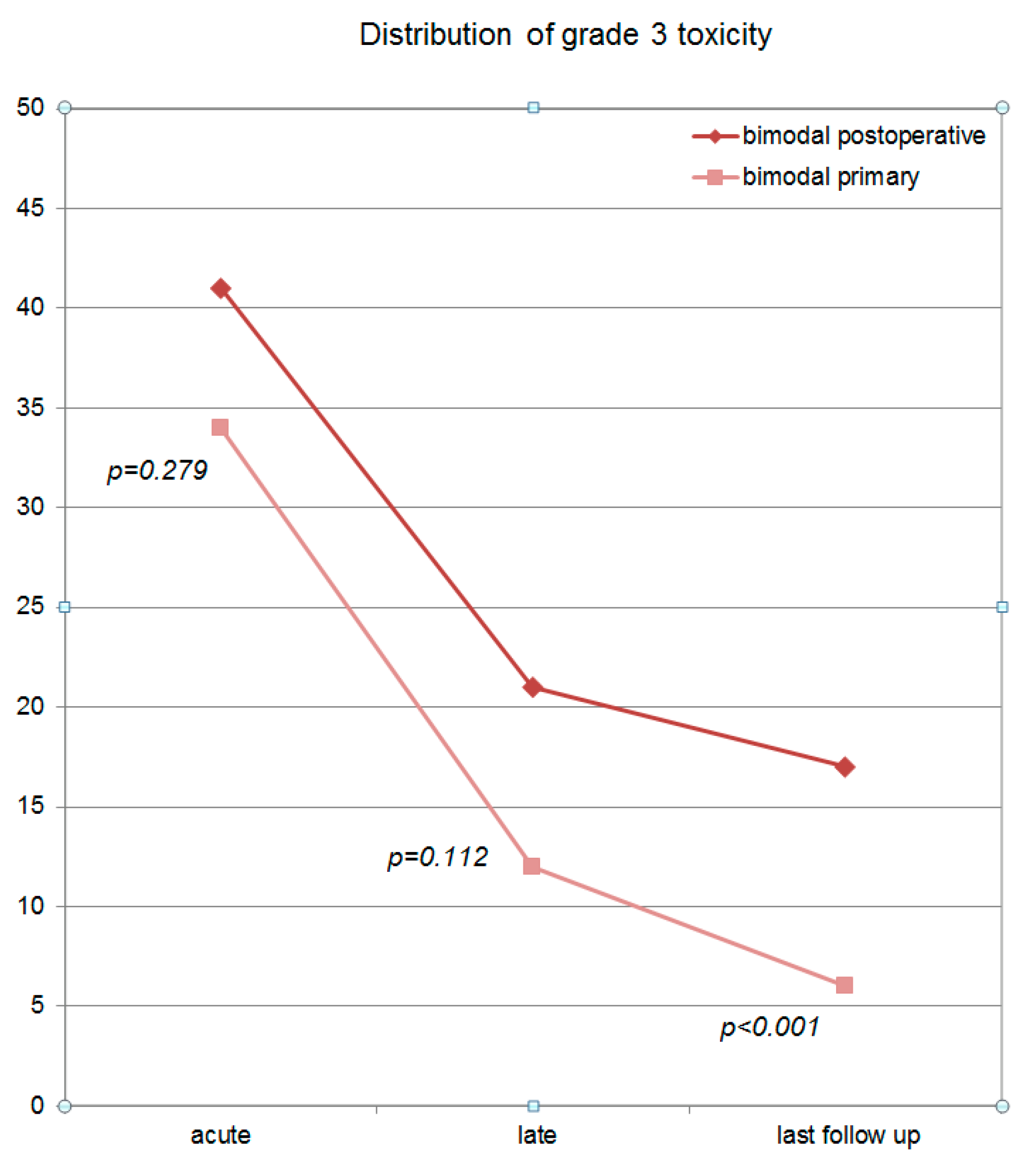
3.2. Toxicity Analysis
4. Discussion
4.1. Findings
4.2. Primary vs. Postoperative Radiotherapy
4.3. Prognostic Factors
4.4. Toxicity
4.5. Limitations and Outlook
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Spiro, R.H.; Huvos, A.G.; Strong, E.W. Adenoid cystic carcinoma of salivary origin. A clinicopathologic study of 242 cases. Am. J. Surg. 1974, 128, 512–520. [Google Scholar] [CrossRef]
- Michel, G.; Joubert, M.; Delemazure, A.S.; Espitalier, F.; Durand, N.; Malard, O. Adenoid cystic carcinoma of the paranasal sinuses: Retrospective series and review of the literature. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2013, 130, 257–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.E.; Park, H.C.; Keum, K.C.; Lee, C.G.; Suh, C.O.; Hur, W.J.; Kim, K.M.; Hong, W.P. Adenoid cystic carcinoma of the maxillary antrum. Am. J. Otolaryngol. 1999, 20, 77–84. [Google Scholar] [CrossRef]
- Spiro, R.H. Salivary neoplasms: Overview of a 35-year experience with 2807 patients. Head Neck Surg. 1986, 8, 177–184. [Google Scholar] [CrossRef]
- Chen, A.M.; Bucci, M.K.; Weinberg, V.; Garcia, J.; Quivey, J.M.; Schechter, N.R.; Phillips, T.L.; Fu, K.K.; Eisele, D.W. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: Prognostic features of recurrence. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 152–159. [Google Scholar] [CrossRef]
- Geara, F.B.; Sanguineti, G.; Tucker, S.L.; Garden, A.S.; Ang, K.K.; Morrison, W.H.; Peters, L.J. Carcinoma of the nasopharynx treated by radiotherapy alone: Determinants of distant metastasis and survival. Radiother. Oncol. 1997, 43, 53–61. [Google Scholar] [CrossRef]
- Chen, A.M.; Granchi, P.J.; Garcia, J.; Bucci, M.K.; Fu, K.K.; Eisele, D.W. Local-regional recurrence after surgery without postoperative irradiation for carcinomas of the major salivary glands: Implications for adjuvant therapy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 982–987. [Google Scholar] [CrossRef]
- Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Werning, J.W.; Hinerman, R.W.; Villaret, D.B. Radiotherapy alone or combined with surgery for adenoid cystic carcinoma of the head and neck. Head Neck 2004, 26, 154–162. [Google Scholar] [CrossRef]
- Terhaard, C.H.; Lubsen, H.; Van der Tweel, I.; Hilgers, F.J.; Eijkenboom, W.M.; Marres, H.A.; Tjho-Heslinga, R.E.; de Jong, J.M.; Roodenburg, J.L.; Dutch, H.; et al. Salivary gland carcinoma: Independent prognostic factors for locoregional control, distant metastases, and overall survival: Results of the Dutch head and neck oncology cooperative group. Head Neck 2004, 26, 681–692. [Google Scholar] [CrossRef]
- Katz, T.S.; Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Hinerman, R.W.; Villaret, D.B. Malignant tumors of the nasal cavity and paranasal sinuses. Head Neck 2002, 24, 821–829. [Google Scholar] [CrossRef]
- Ganly, I.; Patel, S.G.; Singh, B.; Kraus, D.H.; Bridger, P.G.; Cantu, G.; Cheesman, A.; De Sa, G.; Donald, P.; Fliss, D.; et al. Complications of craniofacial resection for malignant tumors of the skull base: Report of an International Collaborative Study. Head Neck 2005, 27, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Myers, L.L.; Nussenbaum, B.; Bradford, C.R.; Teknos, T.N.; Esclamado, R.M.; Wolf, G.T. Paranasal sinus malignancies: An 18-year single institution experience. Laryngoscope 2002, 112, 1964–1969. [Google Scholar] [CrossRef] [PubMed]
- Terhaard, C.H.; Lubsen, H.; Rasch, C.R.; Levendag, P.C.; Kaanders, H.H.; Tjho-Heslinga, R.E.; van Den Ende, P.L.; Burlage, F.; Dutch, H. Neck Oncology Cooperative G: The role of radiotherapy in the treatment of malignant salivary gland tumors. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Garden, A.S.; Weber, R.S.; Ang, K.K.; Morrison, W.H.; Matre, J.; Peters, L.J. Postoperative radiation therapy for malignant tumors of minor salivary glands. Outcome and patterns of failure. Cancer 1994, 73, 2563–2569. [Google Scholar] [CrossRef]
- Miglianico, L.; Eschwege, F.; Marandas, P.; Wibault, P. Cervico-facial adenoid cystic carcinoma: Study of 102 cases. Influence of radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 1987, 13, 673–678. [Google Scholar] [CrossRef]
- Laramore, G.E.; Krall, J.M.; Griffin, T.W.; Duncan, W.; Richter, M.P.; Saroja, K.R.; Maor, M.H.; Davis, L.W. Neutron versus photon irradiation for unresectable salivary gland tumors: Final report of an RTOG-MRC randomized clinical trial. Radiation Therapy Oncology Group. Medical Research Council. Int. J. Radiat. Oncol. Biol. Phys. 1993, 27, 235–240. [Google Scholar] [CrossRef]
- Douglas, J.G.; Koh, W.J.; Austin-Seymour, M.; Laramore, G.E. Treatment of salivary gland neoplasms with fast neutron radiotherapy. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 944–948. [Google Scholar] [CrossRef]
- Stannard, C.; Vernimmen, F.; Carrara, H.; Jones, D.; Fredericks, S.; Hille, J.; de Kock, E. Malignant salivary gland tumours: Can fast neutron therapy results point the way to carbon ion therapy? Radiother. Oncol. 2013, 109, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Huber, P.E.; Debus, J.; Latz, D.; Zierhut, D.; Bischof, M.; Wannenmacher, M.; Engenhart-Cabillic, R. Radiotherapy for advanced adenoid cystic carcinoma: Neutrons, photons or mixed beam? Radiother. Oncol. 2001, 59, 161–167. [Google Scholar] [CrossRef]
- Pommier, P.; Liebsch, N.J.; Deschler, D.G.; Lin, D.T.; McIntyre, J.F.; Barker, F.G.; Adams, J.A.; Lopes, V.V.; Varvares, M.; Loeffler, J.S.; et al. Proton beam radiation therapy for skull base adenoid cystic carcinoma. Arch. Otolaryngol. Head Neck Surg. 2006, 132, 1242–1249. [Google Scholar] [CrossRef]
- Mizoe, J.E.; Tsujii, H.; Kamada, T.; Matsuoka, Y.; Tsuji, H.; Osaka, Y.; Hasegawa, A.; Yamamoto, N.; Ebihara, S.; Konno, A.; et al. Dose escalation study of carbon ion radiotherapy for locally advanced head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Ertner, D.; Nikoghosyan, A.; Didinger, B.; Munter, M.; Jakel, O.; Karger, C.P.; Debus, J. Therapy strategies for locally advanced adenoid cystic carcinomas using modern radiation therapy techniques. Cancer 2005, 104, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Ertner, D.; Nikoghosyan, A.; Jakel, O.; Haberer, T.; Kraft, G.; Scholz, M.; Wannenmacher, M.; Debus, J. Feasibility and toxicity of combined photon and carbon ion radiotherapy for locally advanced adenoid cystic carcinomas. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 391–398. [Google Scholar] [CrossRef]
- Jensen, A.D.; Nikoghosyan, A.V.; Lossner, K.; Haberer, T.; Jakel, O.; Munter, M.W.; Debus, J. COSMIC: A Regimen of Intensity Modulated Radiation Therapy Plus Dose-Escalated, Raster-Scanned Carbon Ion Boost for Malignant Salivary Gland Tumors: Results of the Prospective Phase 2 Trial. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Mizoe, J.E.; Hasegawa, A.; Jingu, K.; Takagi, R.; Bessyo, H.; Morikawa, T.; Tonoki, M.; Tsuji, H.; Kamada, T.; Tsujii, H.; et al. Results of carbon ion radiotherapy for head and neck cancer. Radiother. Oncol. 2012, 103, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, K.; Demizu, Y.; Hashimoto, N.; Mima, M.; Terashima, K.; Fujii, O.; Otsuki, N.; Murakami, M.; Fuwa, N.; Nibu, K. Particle radiotherapy using protons or carbon ions for unresectable locally advanced head and neck cancers with skull base invasion. Jpn. J. Clin. Oncol. 2014, 44, 428–434. [Google Scholar] [CrossRef]
- Sulaiman, N.S.; Demizu, Y.; Koto, M.; Saitoh, J.I.; Suefuji, H.; Tsuji, H.; Ohno, T.; Shioyama, Y.; Okimoto, T.; Daimon, T.; et al. Multicenter Study of Carbon-Ion Radiation Therapy for Adenoid Cystic Carcinoma of the Head and Neck: Subanalysis of the Japan Carbon-Ion Radiation Oncology Study Group (J-CROS) Study (1402 HN). Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 639–646. [Google Scholar] [CrossRef]
- Koto, M.; Demizu, Y.; Saitoh, J.I.; Suefuji, H.; Tsuji, H.; Okimoto, T.; Ohno, T.; Shioyama, Y.; Ikawa, H.; Nemoto, K.; et al. Definitive Carbon-Ion Radiation Therapy for Locally Advanced Sinonasal Malignant Tumors: Subgroup Analysis of a Multicenter Study by the Japan Carbon-Ion Radiation Oncology Study Group (J-CROS). Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 353–361. [Google Scholar] [CrossRef]
- Gomez, D.R.; Hoppe, B.S.; Wolden, S.L.; Zhung, J.E.; Patel, S.G.; Kraus, D.H.; Shah, J.P.; Ghossein, R.A.; Lee, N.Y. Outcomes and prognostic variables in adenoid cystic carcinoma of the head and neck: A recent experience. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1365–1372. [Google Scholar] [CrossRef]
- Jeraj, R.; Mackie, T.R.; Balog, J.; Olivera, G.; Pearson, D.; Kapatoes, J.; Ruchala, K.; Reckwerdt, P. Radiation characteristics of helical tomotherapy. Med. Phys. 2004, 31, 396–404. [Google Scholar] [CrossRef] [Green Version]
- Bentzen, S.M.; Constine, L.S.; Deasy, J.O.; Eisbruch, A.; Jackson, A.; Marks, L.B.; Ten Haken, R.K.; Yorke, E.D. Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC): An introduction to the scientific issues. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. 3), 3–9. [Google Scholar] [CrossRef] [PubMed]
- Brodin, N.P.; Kabarriti, R.; Garg, M.K.; Guha, C.; Tome, W.A. Systematic Review of Normal Tissue Complication Models Relevant to Standard Fractionation Radiation Therapy of the Head and Neck Region Published After the QUANTEC Reports. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Ciccolallo, L.; Licitra, L.; Cantu, G.; Gatta, G.; Group, E.W. Survival from salivary glands adenoid cystic carcinoma in European populations. Oral Oncol. 2009, 45, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.D.; Poulakis, M.; Nikoghosyan, A.V.; Welzel, T.; Uhl, M.; Federspil, P.A.; Freier, K.; Krauss, J.; Hoss, A.; Haberer, T.; et al. High-LET radiotherapy for adenoid cystic carcinoma of the head and neck: 15 years’ experience with raster-scanned carbon ion therapy. Radiother. Oncol. 2016, 118, 272–280. [Google Scholar] [CrossRef]
- Coca-Pelaz, A.; Rodrigo, J.P.; Bradley, P.J.; Vander Poorten, V.; Triantafyllou, A.; Hunt, J.L.; Strojan, P.; Rinaldo, A.; Haigentz, M.; Jr Takes, R.P.; et al. Adenoid cystic carcinoma of the head and neck—An update. Oral Oncol. 2015, 51, 652–661. [Google Scholar] [CrossRef]
- Rackwitz, T.; Debus, J. Clinical applications of proton and carbon ion therapy. Semin. Oncol. 2019. [Google Scholar] [CrossRef]
- Tanvetyanon, T.; Qin, D.; Padhya, T.; McCaffrey, J.; Zhu, W.; Boulware, D.; DeConti, R.; Trotti, A. Outcomes of postoperative concurrent chemoradiotherapy for locally advanced major salivary gland carcinoma. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 687–692. [Google Scholar] [CrossRef]
- Airoldi, M.; Gabriele, A.M.; Gabriele, P.; Pedani, F.; Marchionatti, S.; Succo, G.; Beatrice, F.; Bumma, C. Concomitant chemoradiotherapy followed by adjuvant chemotherapy in parotid gland undifferentiated carcinoma. Tumori 2001, 87, 14–17. [Google Scholar] [CrossRef]
- Dreyfuss, A.I.; Clark, J.R.; Fallon, B.G.; Posner, M.R.; Norris, C.M., Jr.; Miller, D. Cyclophosphamide, doxorubicin, and cisplatin combination chemotherapy for advanced carcinomas of salivary gland origin. Cancer 1987, 60, 2869–2872. [Google Scholar] [CrossRef]
- Garden, A.S.; Weber, R.S.; Morrison, W.H.; Ang, K.K.; Peters, L.J. The influence of positive margins and nerve invasion in adenoid cystic carcinoma of the head and neck treated with surgery and radiation. Int. J. Radiat. Oncol. Biol. Phys. 1995, 32, 619–626. [Google Scholar] [CrossRef]
- Armstrong, J.G.; Harrison, L.B.; Thaler, H.T.; Friedlander-Klar, H.; Fass, D.E.; Zelefsky, M.J.; Shah, J.P.; Strong, E.W.; Spiro, R.H. The indications for elective treatment of the neck in cancer of the major salivary glands. Cancer 1992, 69, 615–619. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, B.H.; Choi, E.C. Nineteen-year oncologic outcomes and the benefit of elective neck dissection in salivary gland adenoid cystic carcinoma. Head Neck 2014, 36, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Mendenhall, W.M.; Parsons, J.T.; Stringer, S.P.; Cassisi, N.J.; Million, R.R. Squamous Cell Carcinoma of the Head and Neck Treated With Irradiation: Management of the Neck. Semin. Radiat. Oncol. 1992, 2, 163–170. [Google Scholar] [CrossRef]
- Mendenhall, W.M.; Million, R.R.; Bova, F.J. Analysis of time-dose factors in clinically positive neck nodes treated with irradiation alone in squamous cell carcinoma of the head and neck. Int. J. Radiat. Oncol. Biol. Phys. 1984, 10, 639–643. [Google Scholar] [CrossRef]
- Parsons, J.T.; Mendenhall, W.M.; Mancuso, A.A.; Cassisi, N.J.; Million, R.R. Malignant tumors of the nasal cavity and ethmoid and sphenoid sinuses. Int. J. Radiat. Oncol. Biol. Phys. 1988, 14, 11–22. [Google Scholar] [CrossRef]
- Cowie, V.J.; Pointon, R.C. Adenoid cystic carcinoma of the salivary glands. Clin. Radiol. 1984, 35, 331–333. [Google Scholar] [CrossRef]
- Ganly, I.; Gross, N.D.; Patel, S.G.; Bilsky, M.H.; Shah, J.P.; Kraus, D.H. Outcome of craniofacial resection in patients 70 years of age and older. Head Neck 2007, 29, 89–94. [Google Scholar] [CrossRef]
- Harbo, G.; Grau, C.; Bundgaard, T.; Overgaard, M.; Elbrond, O.; Sogaard, H.; Overgaard, J. Cancer of the nasal cavity and paranasal sinuses. A clinico-pathological study of 277 patients. Acta Oncol. 1997, 36, 45–50. [Google Scholar] [CrossRef]
- Schulz-Ertner, D.; Jakel, O.; Schlegel, W. Radiation therapy with charged particles. Semin. Radiat. Oncol. 2006, 16, 249–259. [Google Scholar] [CrossRef]
- Munter, M.W.; Schulz-Ertner, D.; Hof, H.; Nikoghosyan, A.; Jensen, A.; Nill, S.; Huber, P.; Debus, J. Inverse planned stereotactic intensity modulated radiotherapy (IMRT) in the treatment of incompletely and completely resected adenoid cystic carcinomas of the head and neck: Initial clinical results and toxicity of treatment. Radiat. Oncol. 2006, 1, 17. [Google Scholar] [CrossRef]
- Chen, Y.J.; Wang, C.P.; Wang, C.C.; Jiang, R.S.; Lin, J.C.; Liu, S.A. Carotid blowout in patients with head and neck cancer: Associated factors and treatment outcomes. Head Neck 2015, 37, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.K.; Sim, B.F.; Tan, C.T.; Goh, K.J.; Ramli, N.; Umapathi, P. Delayed post-irradiation bulbar palsy in nasopharyngeal carcinoma. Neurology 2001, 57, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.C.; Wong, F.C.; Leung, T.W.; Ng, S.H.; Tung, S.Y. Clinical outcomes of 174 nasopharyngeal carcinoma patients with radiation-induced temporal lobe necrosis. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e57–e65. [Google Scholar] [CrossRef] [PubMed]
- Demizu, Y.; Murakami, M.; Miyawaki, D.; Niwa, Y.; Akagi, T.; Sasaki, R.; Terashima, K.; Suga, D.; Kamae, I.; Hishikawa, Y. Analysis of Vision loss caused by radiation-induced optic neuropathy after particle therapy for head-and-neck and skull-base tumors adjacent to optic nerves. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Schlampp, I.; Karger, C.P.; Jakel, O.; Scholz, M.; Didinger, B.; Nikoghosyan, A.; Hoess, A.; Kramer, M.; Edler, L.; Debus, J.; et al. Temporal lobe reactions after radiotherapy with carbon ions: Incidence and estimation of the relative biological effectiveness by the local effect model. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 815–823. [Google Scholar] [CrossRef]
- Pehlivan, B.; Ares, C.; Lomax, A.J.; Stadelmann, O.; Goitein, G.; Timmermann, B.; Schneider, R.A.; Hug, E.B. Temporal lobe toxicity analysis after proton radiation therapy for skull base tumors. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 1432–1440. [Google Scholar] [CrossRef]
- Douglas, J.G.; Laramore, G.E.; Austin-Seymour, M.; Koh, W.J.; Lindsley, K.L.; Cho, P.; Griffin, T.W. Neutron radiotherapy for adenoid cystic carcinoma of minor salivary glands. Int. J. Radiat. Oncol. Biol. Phys. 1996, 36, 87–93. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristic | No. (%) | p-Value | ||
|---|---|---|---|---|
| Overall (n = 227) | Primary Bimodal (n = 90) | Postop. Bimodal (n = 137) | Primary vs. Postoperative | |
| Sex | 0.102 | |||
| male | 118 (52.0) | 40 (44.4) | 78 (56.9) | |
| female | 109 (48.0) | 50 (55.5) | 59 (43.1) | |
| Median age at first diagnosis | 55 years | 56years | 53 years | 0.184 |
| range | (17–80 years) | (21–80 years) | (17–77 years) | |
| Karnofsky performance status | 0.920 | |||
| 100 | 39 (17.1) | 15 (16.7) | 24 (17.5) | |
| 90 | 116 (51.1) | 47 (52.2) | 69 (50.4) | |
| 80 | 52 (22.9) | 19 (21.1) | 33 (24.1) | |
| ≤70 | 20 (8.8) | 9 (10.0) | 11 (8.0) | |
| Tumor location | 0.157 | |||
| maxillary sinus | 122 (53.7) | 42 (46.7) | 80 (58.4) | |
| sphenoid sinus | 18 (7.9) | 11 (12.2) | 7 (5.1) | |
| ethmoid sinus | 6 (2.2) | 1 (1.1) | 4 (2.9) | |
| frontal sinus | 1 (0.4) | none | 1 (0.7) | |
| infiltration of ≥2 sinuses | 81 (35.7) | 36 (40.0) | 45 (32.8) | |
| Tumor side | 0.318 | |||
| unilateral | 148 (65.2) | 55 (61.1) | 93 (67.9) | |
| bilateral (midline involving) | 79 (34.8) | 35 (38.9) | 44 (32.1) | |
| Histological subtype (of n = 197) | 0.624 | |||
| solid | 73 (32.1) | 32 (35.6) | 40 (29.2) | |
| non-solid | 96 (42.3) | 36 (40.0) | 60 (43.8) | |
| mixed | 43 (18.9) | 16 (17.8) | 27 (19.7) | |
| kribriform | 48 (21.1) | 19 (21.1) | 29 (21.2) | |
| tubular | 3 (1.3) | none | 3 (2.2) | |
| trabecular | 2 (0.8) | none | 2 (1.5) | |
| serous | 1 (0.4) | 1 (1.1) | none | |
| unknown | 58 (25.6) | 22 (24.4) | 36 (26.3) | |
| TNM classification | ||||
| T stage | 0.012 * | |||
| 1 | 2 (0.8) | 2 (2.2) | none | |
| 2 | 9 (4.0) | none | 9 (6.6) | |
| 3 | 36 (15.9) | 9 (10.0) | 27 (19.7) | |
| 4 | 180 (79.3) | 79 (87.8) | 101 (73.7) | |
| N stage | 0.008 | |||
| 0 | 199 (87.7) | 77 (85.6) | 122 (89.1) | |
| 1 | 10 (4.4) | 4 (4.4) | 6 (4.4) | |
| 2 | 18 (7.9) | 9 (10.0) | 9 (6.6) | |
| M stage | 0.561 | |||
| 0 | 224 (98.7) | 88 (97.8) | 136 (99.3) | |
| 1 | 3 (1.3) | 2 (2.2) | 1 (0.7) | |
| G stage | 0.686 | |||
| 1 | 13 (5.7) | 5 (5.5) | 8 (5.8) | |
| 2 | 34 (15.0) | 9 (10.0) | 25 (18.2) | |
| 3 | 13 (5.7) | 5 (5.6) | 8 (5.8) | |
| X | 167 (73.6) | 71 (78.9) | 96 (70.1) | |
| LVPn | 0.497 | |||
| 0 | 11 (4.8) | 2 (2.2) | 9 (6.6) | |
| 1 | 97 (42.7) | 32 (35.6) | 65 (47.4) | |
| X | 119 (52.4) | 56 (62.2) | 63 (46.0) | |
| R stage | NA | |||
| R0 | 15 (6.6) | none | 15 (10.9) | |
| R1 | 35 (15.4) | none | 35 (25.5) | |
| R2 | 86 (37.9) | none | 86 (62.8) | |
| Concomitant systemic therapy with cetuximab | 8 (3.5) | 4 (4.4) | 4 (2.9) | NA |
| Treatment volume | ||||
| median CTV1 | 390 cc (100–1247 cc) | 392 cc (100–1247 cc) | 390 cc (100–1116 cc) | 0.728 |
| median CTV2 | 175 cc (28–647 cc) | 181 cc (28–647 cc) | 170 cc (44–396 cc) | 0.196 |
| Treatment doses | ||||
| EQD2 CTV1 | 50 Gy (48 Gy–56 Gy) | 50 Gy (48 Gy–56 Gy) | 50 Gy (48 Gy–56 Gy) | 0.016 |
| EQD2 CTV2 | 80 Gy (71 Gy– 80 Gy) | 80 Gy (71 Gy–80 Gy) | 80 Gy (73 Gy–80 Gy) | 0.781 |
| Variable | HR (95%-CI) | p-Value |
|---|---|---|
| primary vs. postop. | 1.057 (0.574–1.947) | 0.859 |
| solid vs. non-solid histology | 2.350 (1.287–4.290) | 0.005 |
| T4 vs. T3/T2/T1 | 10.021 (2.411–41.662) | 0.002 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akbaba, S.; Ahmed, D.; Mock, A.; Held, T.; Bahadir, S.; Lang, K.; Syed, M.; Hoerner-Rieber, J.; Forster, T.; Federspil, P.; et al. Treatment Outcome of 227 Patients with Sinonasal Adenoid Cystic Carcinoma (ACC) after Intensity Modulated Radiotherapy and Active Raster-Scanning Carbon Ion Boost: A 10-Year Single-Center Experience. Cancers 2019, 11, 1705. https://doi.org/10.3390/cancers11111705
Akbaba S, Ahmed D, Mock A, Held T, Bahadir S, Lang K, Syed M, Hoerner-Rieber J, Forster T, Federspil P, et al. Treatment Outcome of 227 Patients with Sinonasal Adenoid Cystic Carcinoma (ACC) after Intensity Modulated Radiotherapy and Active Raster-Scanning Carbon Ion Boost: A 10-Year Single-Center Experience. Cancers. 2019; 11(11):1705. https://doi.org/10.3390/cancers11111705
Chicago/Turabian StyleAkbaba, Sati, Dina Ahmed, Andreas Mock, Thomas Held, Suzan Bahadir, Kristin Lang, Mustafa Syed, Juliane Hoerner-Rieber, Tobias Forster, Philippe Federspil, and et al. 2019. "Treatment Outcome of 227 Patients with Sinonasal Adenoid Cystic Carcinoma (ACC) after Intensity Modulated Radiotherapy and Active Raster-Scanning Carbon Ion Boost: A 10-Year Single-Center Experience" Cancers 11, no. 11: 1705. https://doi.org/10.3390/cancers11111705