Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
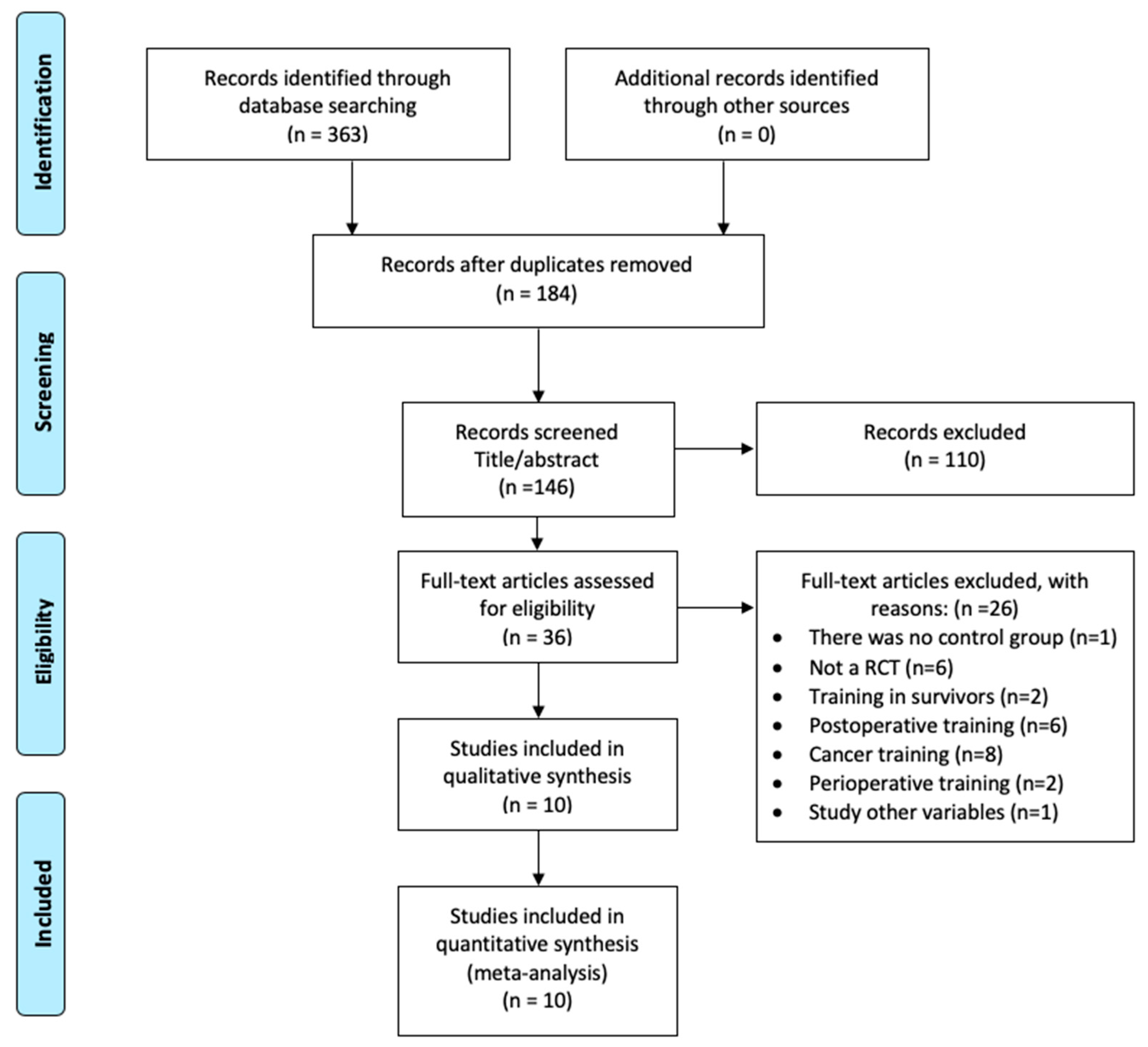
2.1. Information Sources and Searches
2.2. Study Selection
2.3. Outcome Assessment
2.4. Data Extraction and Quality Assessment
2.5. Data Syntheses and Statistical Analyses
2.6. Role of the Funding Source
2.7. Ethics
3. Results
3.1. Characteristics of Included Trials and Participants
3.2. Intervention Description
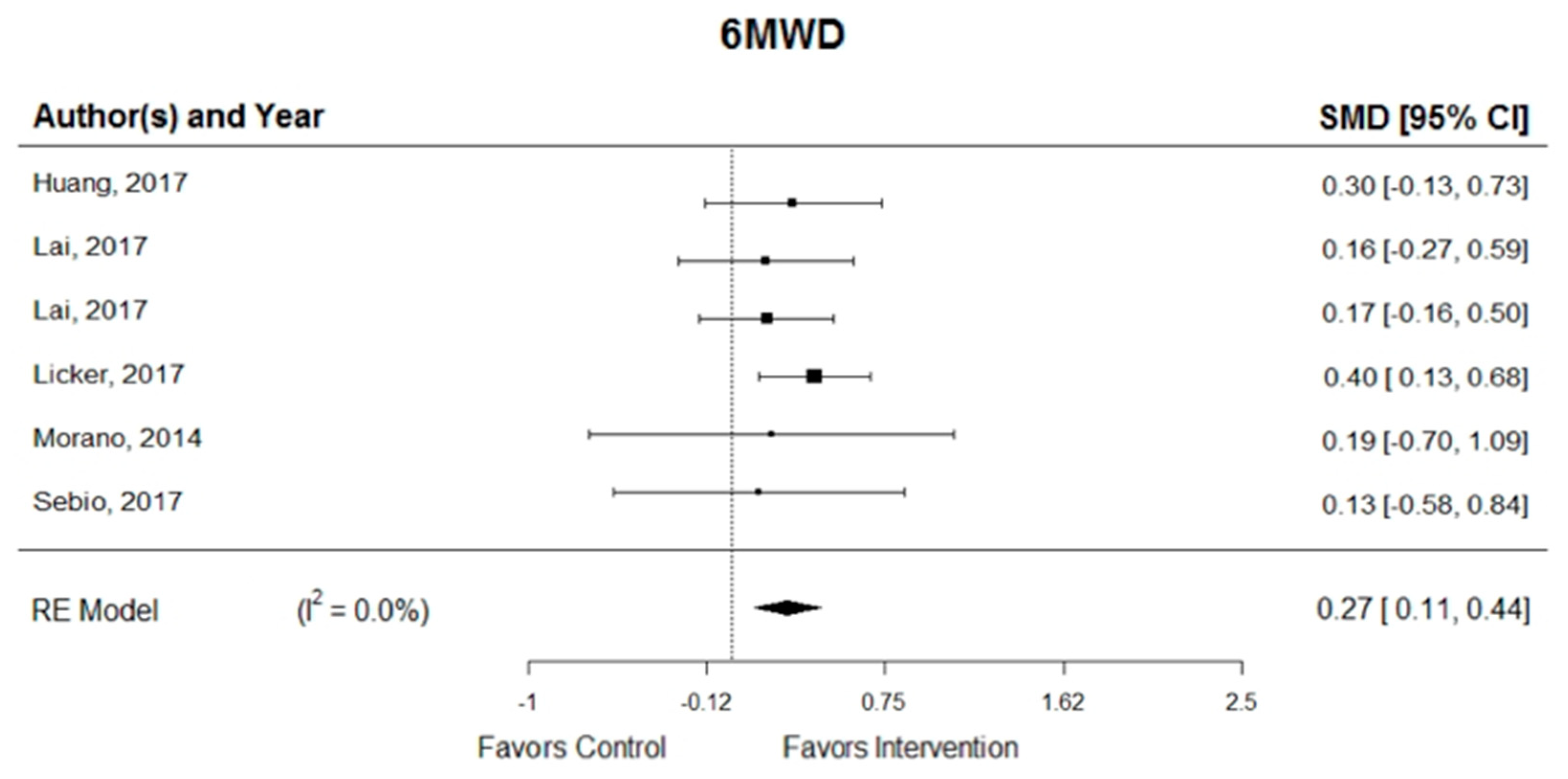
3.3. Primary Outcome: Functional Capacity
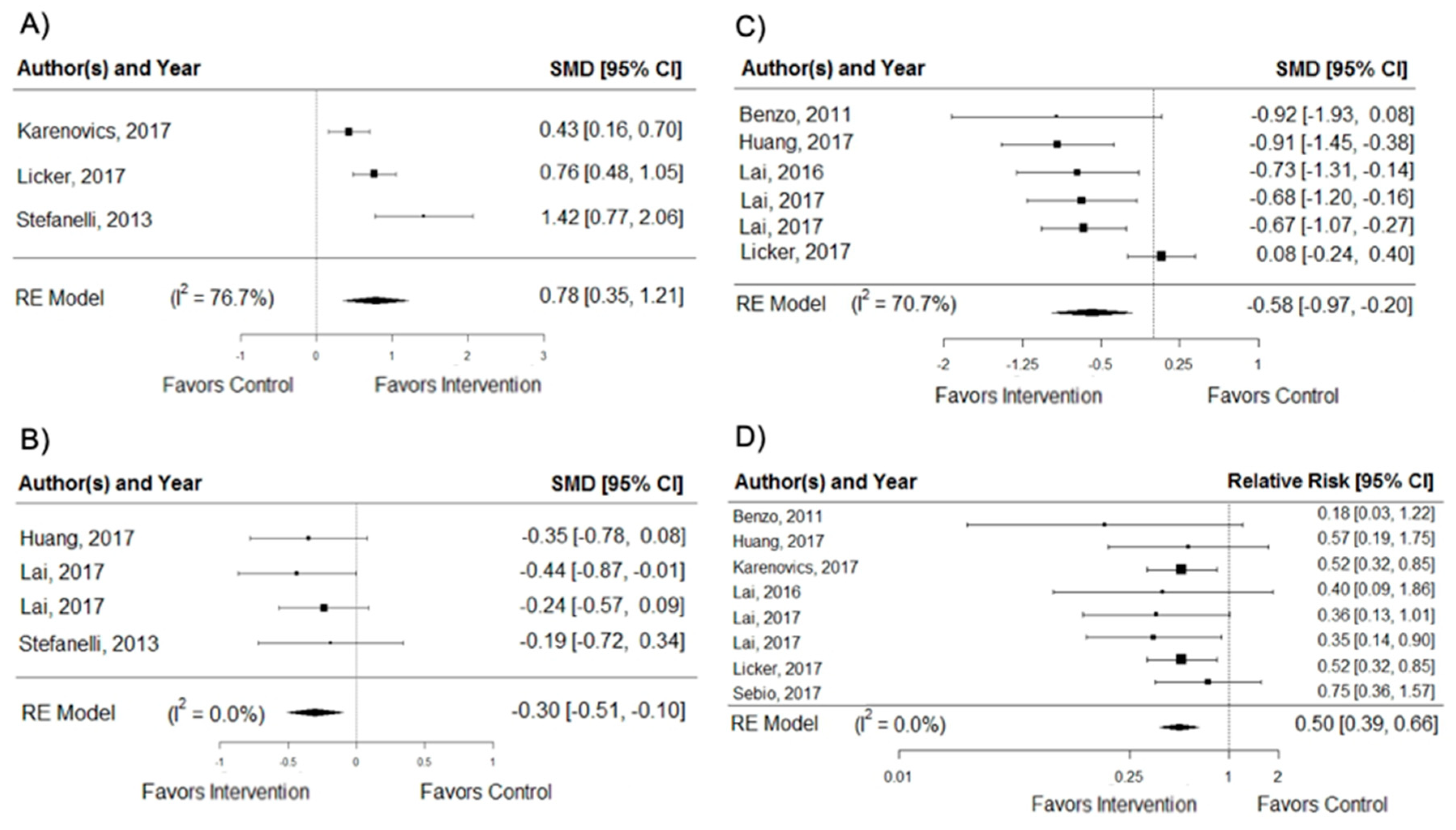
3.4. Secondary Outcomes
3.5. Quality Assessment
3.6. Effect According to the Type of Intervention
3.6.1. Combined Aerobic Exercise Training and IMT versus Usual Care
3.6.2. Combined Aerobic Exercise Training, Strength Training, and IMT versus Usual Care
3.6.3. Combined Aerobic Exercise Training and Strength Training versus Usual Care
3.6.4. Aerobic Exercise Training versus Usual Care
3.7. Effect According to the Duration and Frequency of the Intervention
3.7.1. MWD
3.7.2. VO2peak
3.7.3. Dyspnoea
3.7.4. Postoperative Hospitalization
3.7.5. PPCs
4. Discussion
5. Limitations of the Review
6. Conclusions and Future Recommendations
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ridge, C.A.; McErlean, A.M.; Ginsberg, M.S. Epidemiology of lung cancer. Semin. Interv. Radiol. 2013, 30, 93–98. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommer, M.; Trier, K.; Vibe-Petersen, J.; Missel, M.; Christensen, M.; Larsen, K.; Langer, S.; Hendriksen, C.; Clementsen, P.; Pedersen, J.; et al. Perioperative rehabilitation in operation for lung cancer (PROLUCA) rationale and design. BMC Cancer 2014, 14, 404. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Lung Cancer: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/cg121 (accessed on 14 March 2019).
- Nurgali, K.; Jagoe, R.T.; Abalo, R. Editorial: Adverse effects of cancer chemotherapy: Anything new to improve tolerance and reduce sequelae? Front. Pharm. 2018, 9, 245. [Google Scholar] [CrossRef] [PubMed]
- Jack, S.; West, M.A.; Raw, D.; Marwood, S.; Ambler, G.; Cope, T.M.; Shrotri, M.; Sturgess, R.P.; Calverley, P.M.; Ottensmeier, C.H.; et al. The effect of neoadjuvant chemotherapy on physical fitness and survival in patients undergoing oesophagogastric cancer surgery. Eur. J. Surg. Oncol. 2014, 40, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Messaggi-Sartor, M.; Marco, E.; Martinez-Tellez, E.; Rodriguez-Fuster, A.; Palomares, C.; Chiarella, S.; Muniesa, J.M.; Orozco-Levi, M.; Barreiro, E.; Guell, M.R. Combined aerobic exercise and high-intensity respiratory muscle training in patients surgically treated for non-small cell lung cancer: A pilot randomized clinical trial. Eur. J. Phys. Rehabil. Med. 2019, 55, 113–122. [Google Scholar] [CrossRef]
- Hanna, N.; Johnson, D.; Temin, S.; Baker, S., Jr.; Brahmer, J.; Ellis, P.M.; Giaccone, G.; Hesketh, P.J.; Jaiyesimi, I.; Leighl, N.B.; et al. Systemic therapy for stage IV non-small-cell lung cancer: American society of clinical oncology clinical practice guideline update. J. Clin. Oncol. 2017, 35, 3484–3515. [Google Scholar] [CrossRef]
- Kuehr, L.; Wiskemann, J.; Abel, U.; Ulrich, C.M.; Hummler, S.; Thomas, M. Exercise in patients with non-small cell lung cancer. Med. Sci. Sports. Exerc. 2014, 46, 656–663. [Google Scholar] [CrossRef]
- Crandall, K.; Maguire, R.; Campbell, A.; Kearney, N. Exercise intervention for patients surgically treated for Non-Small Cell Lung Cancer (NSCLC): A systematic review. Surg. Oncol. 2014, 23, 17–30. [Google Scholar] [CrossRef]
- Granger, C.L.; McDonald, C.F.; Berney, S.; Chao, C.; Denehy, L. Exercise intervention to improve exercise capacity and health related quality of life for patients with Non-Small Cell Lung Cancer: A systematic review. Lung Cancer 2011, 72, 139–153. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Pennick, V.; Bombardier, C.; van Tulder, M. 2009 updated method guidelines for systematic reviews in the cochrane back review group. Spine 2009, 34, 1929–1941. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American college of sports medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Herbert, R.D.; Maher, C.G.; Moseley, A.M. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man.Therap. 2000, 5, 223–226. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine. Guidelines for Exercise Testing and Prescription, 7th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; p. 455. [Google Scholar]
- Edge, S.B.; Compton, C.C. The american joint committee on cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Lai, Y.; Zhou, X.; Li, S.; Su, J.; Yang, M.; Che, G. Short-term high-intensity rehabilitation in radically treated lung cancer: A three-armed randomized controlled trial. J. Thorac. Dis. 2017, 9, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Su, J.; Yang, M.; Zhou, K.; Che, G. Impact and effect of preoperative short-term pulmonary rehabilitation training on lung cancer patients with mild to moderate chronic obstructive pulmonary disease: A randomized trial. Zhongguo Fei Ai Za Zhi 2016, 19, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Huang, J.; Yang, M.; Su, J.; Liu, J.; Che, G. Seven-day intensive preoperative rehabilitation for elderly patients with lung cancer: A randomized controlled trial. J. Surg. Res. 2017, 209, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Su, J.; Qiu, P.; Wang, M.; Zhou, K.; Tang, Y.; Che, G. Systematic short-term pulmonary rehabilitation before lung cancer lobectomy: A randomized trial. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 476–483. [Google Scholar] [CrossRef]
- Benzo, R.; Wigle, D.; Novotny, P.; Wetzstein, M.; Nichols, F.; Shen, R.K.; Cassivi, S.; Deschamps, C. Preoperative pulmonary rehabilitation before lung cancer resection: Results from two randomized studies. Lung Cancer 2011, 74, 441–445. [Google Scholar] [CrossRef] [Green Version]
- Karenovics, W.; Licker, M.; Ellenberger, C.; Christodoulou, M.; Diaper, J.; Bhatia, C.; Robert, J.; Bridevaux, P.O.; Triponez, F. Short-term preoperative exercise therapy does not improve long-term outcome after lung cancer surgery: A randomized controlled study. Eur. J. Cardiovasc. Thorac. Surg. 2017, 52, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Licker, M.; Karenovics, W.; Diaper, J.; Frésard, I.; Triponez, F.; Ellenberger, C.; Schorer, R.; Kayser, B.; Bridevaux, P.O. Short-term preoperative high-intensity interval training in patients awaiting lung cancer surgery: A randomized controlled trial. J. Thorac. Oncol. 2017, 12, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Morano, M.; Mesquita, R.; Silva, G.; Araujo, A.; Pinto, J.; Neto, A.; Viana, C.; Moraes, F.M.; Pereira, E. Comparison of the effects of pulmonary rehabilitation with chest physical therapy on the levels of fibrinogen and albumin in patients with lung cancer awaiting lung resection: A randomized clinical trial. BMC Pulm. Med. 2014, 14, 121. [Google Scholar] [CrossRef] [PubMed]
- Stefanelli, F.; Meoli, I.; Cobuccio, R.; Curcio, C.; Amore, D.; Casazza, D.; Tracey, M.; Rocco, G. High-intensity training and cardiopulmonary exercise testing in patients with chronic obstructive pulmonary disease and non-small-cell lung cancer undergoing lobectomy. Eur. J. Cardiovasc. Thorac Surg. 2013, 44, e260–e265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sebio García, R.; Yáñez-Brage, M.I.; Giménez Moolhuyzen, E.; Salorio Riobo, M.; Lista Paz, A.; Borro Mate, J.M. Preoperative exercise training prevents functional decline after lung resection surgery: A randomized, single-blind controlled trial. Clin. Rehabil. 2017, 31, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Yamana, I.; Takeno, S.; Hashimoto, T.; Maki, K.; Shibata, R.; Shiwaku, H.; Shimaoka, H.; Shiota, E.; Yamashita, Y. Randomized controlled study to evaluate the efficacy of a preoperative respiratory rehabilitation program to prevent postoperative pulmonary complications after esophagectomy. Dig. Surg. 2015, 32, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Sebio Garcia, R.; Yanez Brage, M.I.; Gimenez Moolhuyzen, E.; Granger, C.L.; Denehy, L. Functional and postoperative outcomes after preoperative exercise training in patients with lung cancer: A systematic review and meta-analysis. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 486–497. [Google Scholar] [CrossRef]
- Treanor, C.; Kyaw, T.; Donnelly, M. An international review and meta-analysis of prehabilitation compared to usual care for cancer patients. J. Cancer Surviv. 2018, 12, 64–73. [Google Scholar] [CrossRef]
- Weiner, P.; Weiner, M. Inspiratory muscle training may increase peak inspiratory flow in chronic obstructive pulmonary disease. Respiration 2006, 73, 151–156. [Google Scholar] [CrossRef]
- Rivas-Perez, H.; Nana-Sinkam, P. Integrating pulmonary rehabilitation into the multidisciplinary management of lung cancer: A review. Respir. Med. 2015, 109, 437–442. [Google Scholar] [CrossRef] [Green Version]
- Gosselink, R.; De Vos, J.; van den Heuvel, S.P.; Segers, J.; Decramer, M.; Kwakkel, G. Impact of inspiratory muscle training in patients with COPD: What is the evidence? Eur. Respir. J. 2011, 37, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W. Physical activity and lung cancer survivorship. Recent Results Cancer Res. 2011, 186, 255–274. [Google Scholar] [CrossRef] [PubMed]
- Gimenez, M.; Servera, E.; Vergara, P.; Bach, J.R.; Polu, J.M. Endurance training in patients with chronic obstructive pulmonary disease: A comparison of high versus moderate intensity. Arch. Phys. Med. Rehabil. 2000, 81, 102–109. [Google Scholar] [CrossRef]
- Corhay, J.L.; Nguyen, D.; Duysinx, B.; Graas, C.; Pirnay, F.; Bury, T.; Louis, R. Should we exclude elderly patients with chronic obstructive pulmonary disease from a long-time ambulatory pulmonary rehabilitation programme? J. Rehabil. Med. 2012, 44, 466–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, C.C.; Chu, W.H.; Yang, M.C.; Lee, C.H.; Wu, Y.K.; Wu, C.P. Benefits of pulmonary rehabilitation in patients with COPD and normal exercise capacity. Respir. Care 2013, 58, 1482–1488. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.L.; Holland, A.E.; Gordon, I.R.; Denehy, L. Minimal important difference of the 6-min walk distance in lung cancer. Chron. Respir. Dis. 2015, 12, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.W.; Watson, D.; Herndon, J.E., 2nd; Eves, N.D.; Haithcock, B.E.; Loewen, G.; Kohman, L. Peak oxygen consumption and long-term all-cause mortality in nonsmall cell lung cancer. Cancer 2010, 116, 4825–4832. [Google Scholar] [CrossRef] [PubMed]
- Singh, F.; Newton, R.U.; Galvao, D.A.; Spry, N.; Baker, M.K. A systematic review of pre-surgical exercise intervention studies with cancer patients. Surg. Oncol. 2013, 22, 92–104. [Google Scholar] [CrossRef] [PubMed]
- Loewen, G.M.; Watson, D.; Kohman, L.; Herndon, J.E., 2nd; Shennib, H.; Kernstine, K.; Olak, J.; Mador, M.J.; Harpole, D.; Sugarbaker, D.; et al. Preoperative exercise Vo2 measurement for lung resection candidates: Results of cancer and leukemia group B protocol 9238. J. Thorac. Oncol. 2007, 2, 619–625. [Google Scholar] [CrossRef]
- Benzo, R.; Kelley, G.A.; Recchi, L.; Hofman, A.; Sciurba, F. Complications of lung resection and exercise capacity: A meta-analysis. Respir. Med. 2007, 101, 1790–1797. [Google Scholar] [CrossRef] [Green Version]
- Bobbio, A.; Chetta, A.; Ampollini, L.; Primomo, G.L.; Internullo, E.; Carbognani, P.; Rusca, M.; Olivieri, D. Preoperative pulmonary rehabilitation in patients undergoing lung resection for non-small cell lung cancer. Eur. J. Cardiovasc. Thorac Surg. 2008, 33, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, A.; Pompili, C.; Salati, M.; Refai, M.; Berardi, R.; Mazzanti, P.; Tiberi, M. Preoperative maximum oxygen consumption is associated with prognosis after pulmonary resection in stage I non-small cell lung cancer. Ann. Thorac. Surg. 2014, 98, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Bolliger, C.T.; Jordan, P.; Soler, M.; Stulz, P.; Tamm, M.; Wyser, C.; Gonon, M.; Perruchoud, A.P. Pulmonary function and exercise capacity after lung resection. Eur. Respir. J. 1996, 9, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.; Beckenkamp, P.R.; Hancock, M.; Solomon, M.; Young, J. Preoperative exercise halves the postoperative complication rate in patients with lung cancer: A systematic review of the effect of exercise on complications, length of stay and quality of life in patients with cancer. Br. J. Sports Med. 2018, 52, 344. [Google Scholar] [CrossRef] [PubMed]
- Ni, H.J.; Pudasaini, B.; Yuan, X.T.; Li, H.F.; Shi, L.; Yuan, P. Exercise training for patients pre- and postsurgically treated for non-small cell lung cancer: A systematic review and meta-analysis. Integr. Cancer 2017, 16, 63–73. [Google Scholar] [CrossRef]
- Rueth, N.M.; Parsons, H.M.; Habermann, E.B.; Groth, S.S.; Virnig, B.A.; Tuttle, T.M.; Andrade, R.S.; Maddaus, M.A.; D’Cunha, J. The long-term impact of surgical complications after resection of stage I nonsmall cell lung cancer: A population-based survival analysis. Ann. Surg. 2011, 254, 368–374. [Google Scholar] [CrossRef]
- Celli, B.R. Pulmonary rehabilitation. Isr. Med. Assoc. J. 2003, 5, 443–448. [Google Scholar]
- Rochester, C.L. Pulmonary rehabilitation for patients who undergo lung-volume-reduction surgery or lung transplantation. Respir. Care 2008, 53, 1196–1202. [Google Scholar]
- Holland, A.E.; Wadell, K.; Spruit, M.A. How to adapt the pulmonary rehabilitation programme to patients with chronic respiratory disease other than COPD. Eur Respir Rev. 2013, 22, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.; et al. An official American Thoracic Society/European Respiratory Society statement: Key concepts and advances in pulmonary rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Correa-Bautista, J.E.; Schmidt-Río, J.; Ramírez-Vélez, R. Effectiveness of physical exercise on fatigue in cancer patients during active treatment: a systematic review and meta-analysis. Cad. Saúde. Pública 2015, 31, 667–681. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference, Year | Intervention | Duration/Frequency | N | Setting | Follow-Up Time (Days) | Participants | Outcomes of Interest | Feasibility/AE | Additional Notes | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Aerobic exercise training and inspiratory muscle training | ||||||||||
| Huang et al., 2017 [18] | Three conditions: 1. (a) IMT-ABT: two to three times daily for 15–20 min/s; -TBT (Voldyne 5000): 20 min at least four times daily; (b) CRT (NuStep): twice daily for 20 min/s; (c) psychological educational guidance (EG) 2. Single IMT (SG) 3. Routine preoperative preparation (CG) | 1 week 2 times a day | 60 | In hospital | No follow-up | 90 patients were randomized: age, mean (SD); Control group: n = 30, 63.6 (6.5); Exercise group: n = 30, 63.0 (8.7); Single group: n = 30, 64.1 (5.3) | Hospitalization postoperative days a PPCs c 6MWD (meters) ab PEF (L/min) ab FEV1 (L) cd FVC (L) cd Fatigue cd Dyspnoea cd DLCO (mL/min/mmHg) cd HRQoL ab Physical function cd Emotional function cd | The completion rates suggest that compliance with the programs is likely to be high and also supports the feasibility of the EG program | Proportion of subjects who completed the pogram (97%). Adherence to the prescribed training sessions NR. SG did not show significant differences in outcomes compared with CG | This hospital-based short-term pattern of PPR combining high-intensity IMT with CRT could be a feasible strategy for treating NSCLC patients, especially those with risk factors of PPCs awaiting surgery |
| Lai et al., 2016 [19] | Two conditions: 1. I. Pharmacotherapy (Bricanyl, Pulmicort, Mucosolvan): 2 times/day; II. Physical rehabilitation: (a) IMT-ABT: (20–30 rep in 15–30 min), -TBT (Voldyne 5000): 2–3 s, 12–20 rep/2 h; (b) -EET-LE (NuStep): 15–20 min/day, -Climbing ladder training (EG): 15–30 min/day 2. Underwent standard preoperative (CG) | 1 week Daily | 48 | In hospital | No follow-up | 48 patients were randomized: age, mean (SD); Exercise group: n = 24, 63.13 (6.26); Control group: n = 24, 64.04 (8.94) | Hospitalization postoperative days a PEF (L/min) b 6MWD (meters) b HRQoL d Physical function d Emotional function d Dyspnoea d Fatigue d PPCs c | No AE related to the intervention | Proportion of subjects who completed the pogram (100%). Adherence to the prescribed training sessions NR | Pre-operative short-term comprehensive pulmonary rehabilitation training can improve pulmonary resistance of patients with mild to moderate COPD, accelerate rapid recovery of patients after surgery, can be used as an important part of the PPR fast |
| Lai, Huang, et al., 2017 [20] | Two conditions: 1. (a) IMT-ABT: twice per day 15–20 min/s; -TBT (Voldyne 5000): 3 s/day 20 min/s. (b) EET (NuStep): 30 min/day 2. Usual care (CG) | 1 week Daily | 127 | In hospital | No follow-up | 60 patients were randomized: age, mean (SD); Exercise group: n = 30, 72.5 ± (3.4); Control group: n = 30, 71.6 ± (1.9) | Hospitalization postoperative days a PEF (L/min) ab FVC (L) c FEV1 (L) c DLCO (ml/min/mmHg) c 6MWD (meters) ab HRQoL c Physical function c Emotional function c Dyspnoea c PPCs a | 4 patients in the EG suspended the training because they could not endure the highly intensive regimen, 1 perceived a lack of benefit, and 1 suffered from knee pain | Proportion of subjects who completed the pogram (47%). Adherence to the prescribed training sessions NR | PPR played a positive physical role in improving the PEF and 6MWD in elderly surgical patients with LC while significantly reducing the postoperative length of stay. We, thus, consider the 7-day intensive pattern of PPR to be a feasible rehabilitation strategy for elderly NSCLC patients in China |
| Lai, Su, et al., 2017 [21] | Two conditions: 1. (a) IMT-TBT (HUDSON RCI 2500): 3 s/day, 20 rep/s; -ABT: twice per day 15–30 min/s. (b) EET (NuStep): 30 min/day 2. Usual care (CG) | 1 week Daily | 101 | In hospital | No follow-up | 101 patients were randomized: age, mean (SD); Exercise group: n = 51, 63.8 ± (8.2); Control group: n = 50, 64.6 ± (6.6) Range: (50–80 years) | Hospitalization postoperative days a PEF (L/min) ab 6MWD (meters) ab HRQoL cd Physical function cd Emotional function cd Dyspnoea cd Fatigue cd PPCs a | No AE related to the intervention | Proportion of subjects who completed the pogram (94%). Adherence to the prescribed training sessions NR | Fewer PPCs and better postoperative recovery in the EG, which led to shorter postoperative hospital stays, reduced use of medications and medical care, consequently, lower in-hospital expenses |
| Stefanelli et al., 2013 [26] | Two conditions: 1. (a) IMT: Respiratory exercises on the bench, mattress pad and wall bar. (b) EET: High intensity training of UE (rowing ergometer) and LE (treadmill and the ergometric bicycle), 70% PWC (c) Pharmacotherapy (bronchodilators, inhaled corticosteroids) 2. Usual care (CG) | 3 weeks 5 times a week | 40 | In hospital | 60 | 40 patients were randomized: age, mean (SD); Exercise group: 65.5 (± 7.4) Control group: 64.8 (± 7.3) | FEV1 (L) ab VO2peak (mL/kg/min) ab DLCO (ml/min/mmHg) cd Dyspnoea ab | NR | Proportion of subjects who completed the pogram NR. Adherence to the prescribed training sessions NR | It is possible to state that preoperative high-intensity PRP improves the degree of physical performance of patients with COPD and NSCLC undergoing surgical resection compared with similar surgical patients who did not undergo preoperative PRP |
| Aerobic exercise training, strength training, and IMT | ||||||||||
| Benzo et al., 2011 [22] | Two studies: I. NR II. Two conditions: 1. (a) EET (LE/UE) (NuStep): 20 min (b) Strength alternating UE/LE every other day (Thera-band): 2s × 10–12 rep (c) (IMT) (Threshold IMT or the P-Flex valve) (EG): 15–20 min of daily use. 2. Usual care (CG) | I. 4 weeks II. 1 week 2 times a day | I. 9; II. 19 | I. In hospital II. In hospital | No follow-up | I. 9 patients were randomized: EG n = 5; CG n = 4 II. 17 patients were randomized: age, mean (SD); Exercise group: n = 9, 70.2 (8.61); Control group: n = 8, 72.0 (6.69) | II. Hospitalization postoperative days c PPCs a | I. Non-feasibility of 4 weeks of PPR. No AE related to the intervention | II. Proportion of subjects who completed the pogram (89%). Adherence to the prescribed training sessions NR | I. PPR is appropriate and recommended by experts. II. The development of a short and feasible PPR protocol was the natural consequence of the failure of the longer one. The 10-session protocol showed a high likelihood of decreasing hospital length of stay, a very meaningful outcome that is a crude estimation of postoperative morbidity and costs |
| Sebio García et al., 2017 [27] | Two conditions: 1. (a) EET moderate (cycle ergometer-Monark): -30 min interval training -5 min warm-up (30% PWC) -1 min (80% PWC) -4 min (active rest 50% PWC). -4 min cool down (30% PWC) (b) CRT: - elastic bands (Thera-Band®) body-weight exercises: six different exercises: 15 rep × 3 s, 45 s micropause (increased to 4 s if tolerated) (c) IMT (Coach 2 Incentive Spirometer®). -TBT: 2 s/day 30 sustained inspirations (80% MVC) end inspiratory hold (2–3 s). 6 cycles × 5 rep, 1 min pause/ cycle. 2. Usual care (CG) | Median of 16 sessions 3–5 times a week | 40 | In hospital | 55 | 22 patients were randomized: age, mean (SD); Exercise group: n = 10, 70.9 ± (6.1); Control group: n = 12, 69.4 ± (9.4) | Hospitalization postoperative days c PPCsc 6MWD (meters) cd Physical Component ad Physical functioning d Emotional function d | No AE related to the intervention. | Proportion of subjects who completed the pogram (55%). Adherence to the prescribed training sessions NR | Although no significant differences between groups were observed at three weeks in any of the variables analyzed, three months postoperatively, there were statistically significant differences in the mean change for the exercise capacity, the physical component summary, and the upper and lower muscle strength assessment leading to two opposite trends in patients’ recovery |
| Aerobic exercise training and strength training | ||||||||||
| Licker et al., 2017 [24] | Two conditions: 1. (a) Warm-up: 5 min (50% PWC); 2 s × 10 min [(interv 15 s (80–100% PWC), micropause 15 s, macropause 4 min/s; Cooled down: 5 min (30% PWC) (b) EET (cycle ergometer) (c) strengthening UE/LE: leg press, leg extension, back extension, seat row, biceps curls or chest and shoulder press 2. Usual care (CG) | 3–4 weeks 2–3 times a week | 164 | In hospital | No follow-up | 151 patients were randomized: age, mean (SD); Exercise group: n = 74, 64 (13); Control group: n = 77, 64 (10) | VO2peak (mL/kg/min) ab 6MWD (meters) ab PPCs a Hospitalization postoperative (days) c | No AE related to the intervention | Proportion of subjects who completed the pogram (92%). Adherence to the prescribed training sessions. EG: 87 ± 18% | Demonstrated the safety and effectiveness of a short-term exercise training program in improving aerobic performances in patients LC. However, this HIIT rehabilitation modality failed to produce significant difference in composite morbidity-mortality index, compared with usual care |
| Multicomponent training and IMT | ||||||||||
| Morano et al., 2014 [25] | Two conditions: 1. (a) Stretching LE/UE; (b) warm-up exercises; (c) strengthening UE (50% PWC), PNF (barbells); (d) EET (treadmill) 80% PWC; (e) IMT; (f) educational sessions 2. (a) CPT (routine protocol of the hospital comprising lung expansion techniques) -sustained maximum inspiration; -fractional inspiration; -breathing patterns; -pursed lip breathing; -use of a flow-based incentive spirometer (Respiron) (b) Educational sessions (CG) | 4 weeks 5 times a week | 31 | In hospital | 30 | 24 patients were randomized: age, mean (SD); Exercise group: n = 12, 65 ± (8); Control group: n = 12, 69 ± (7) | 6MWD (meters) cd HRQoL cd | No AE related to the intervention | Proportion of subjects who completed the pogram (100%). Adherence to the prescribed training sessions NR | The study showed improvements in PEF and 6MWD and reductions in the total / postoperative length of stay, hospital costs and occurrence of PPCs |
| Only aerobic exercise training | ||||||||||
| Karenovics et al., 2017 [23] | Two conditions: 1. (a) Warm-up: 5 min (50% PWC); 2 s × 10 min (interv 15 s sprint and 15 s pause, macropause 4 min/s); Cooled down: 5 min (30% PWC) (b) EET (cycle ergometer) 2. Usual care (CG) | 2–4 weeks 3 times a week | 164 | In hospital | 30 | 151 patients were randomized: age, mean (SD); Exercise group: n = 74, 64 (13); Control group: n = 77, 64 (10) | VO2peak (mL/kg/min) a PPCs a | No AE related to the intervention | Proportion of subjects who completed the pogram (92%). Adherence to the prescribed training sessions was 87 ± 18% (median 8 sessions, IQ 25–75% [7,8,9,10]) in EG | A HIIT program limited to the preoperative period is not associated with better functional and clinical outcome 1 year after lung cancer surgery |
| Reference, Year | Type of Exercise | Duration | Frequency | Intensity | Total Score |
|---|---|---|---|---|---|
| Benzo et al., 2011 [22] | Yes | Yes | Yes | No | 3/4 |
| Huang et al., 2017 [18] | Yes | Yes | Yes | No | 3/4 |
| Karenovics et al., 2017 [23] | Yes | Yes | Yes | Yes | 4/4 |
| Lai et al., 2016 [19] | Yes | Yes | Yes | No | 3/4 |
| Lai, Huang, et al., 2017 [20] | Yes | Yes | Yes | No | 3/4 |
| Lai, Su, et al., 2017 [21] | Yes | Yes | Yes | No | 3/4 |
| Licker et al., 2017 [24] | Yes | Yes | Yes | Yes | 4/4 |
| Morano et al., 2014 [25] | Yes | No | Yes | Yes | 3/4 |
| Sebio García et al., 2017 [27] | Yes | Yes | Yes | Yes | 4/4 |
| Stefanelli et al., 2013 [26] | Yes | Yes | Yes | Yes | 4/4 |
| Study | Eligibility Criteria Specified * | Random Allocation | Concealed Allocation | Groups Similar at Baseline | Participant Blinding | Therapist Blinding | Assessor Blinding | Adequate Follow-Up | Intention-To-Treat Analysis | Between-Group Comparison | Point Estimates and Variability | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Benzo et al., 2011 [22] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | Yes | 6/10 |
| Huang et al., 2017 [18] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Karenovics et al., 2017 [23] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Lai et al., 2016 [19] | Yes | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4/10 |
| Lai, Huang, et al., 2017 [20] | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7/10 |
| Lai, Su, et al., 2017 [21] | No | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | 7/10 |
| Licker et al., 2017 [24] | No | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Morano et al., 2014 [25] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | 7/10 |
| Sebio García et al., 2017 [27] | Yes | Yes | Yes | Yes | No | No | Yes | No | No | Yes | Yes | 6/10 |
| Stefanelli et al., 2013 [26] | No | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4/10 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosero, I.D.; Ramírez-Vélez, R.; Lucia, A.; Martínez-Velilla, N.; Santos-Lozano, A.; Valenzuela, P.L.; Morilla, I.; Izquierdo, M. Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer. Cancers 2019, 11, 944. https://doi.org/10.3390/cancers11070944
Rosero ID, Ramírez-Vélez R, Lucia A, Martínez-Velilla N, Santos-Lozano A, Valenzuela PL, Morilla I, Izquierdo M. Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer. Cancers. 2019; 11(7):944. https://doi.org/10.3390/cancers11070944
Chicago/Turabian StyleRosero, Ilem D., Robinson Ramírez-Vélez, Alejando Lucia, Nicolas Martínez-Velilla, Alejandro Santos-Lozano, Pedro L. Valenzuela, Idoia Morilla, and Mikel Izquierdo. 2019. "Systematic Review and Meta-Analysis of Randomized, Controlled Trials on Preoperative Physical Exercise Interventions in Patients with Non-Small-Cell Lung Cancer" Cancers 11, no. 7: 944. https://doi.org/10.3390/cancers11070944