Bimodal Radiotherapy with Active Raster-Scanning Carbon Ion Radiotherapy and Intensity-Modulated Radiotherapy in High-Risk Nasopharyngeal Carcinoma Results in Excellent Local Control

 , , ,
, , ,
Abstract
:1. Background
2. Methods
2.1. Evaluation
2.2. Patient Characteristics
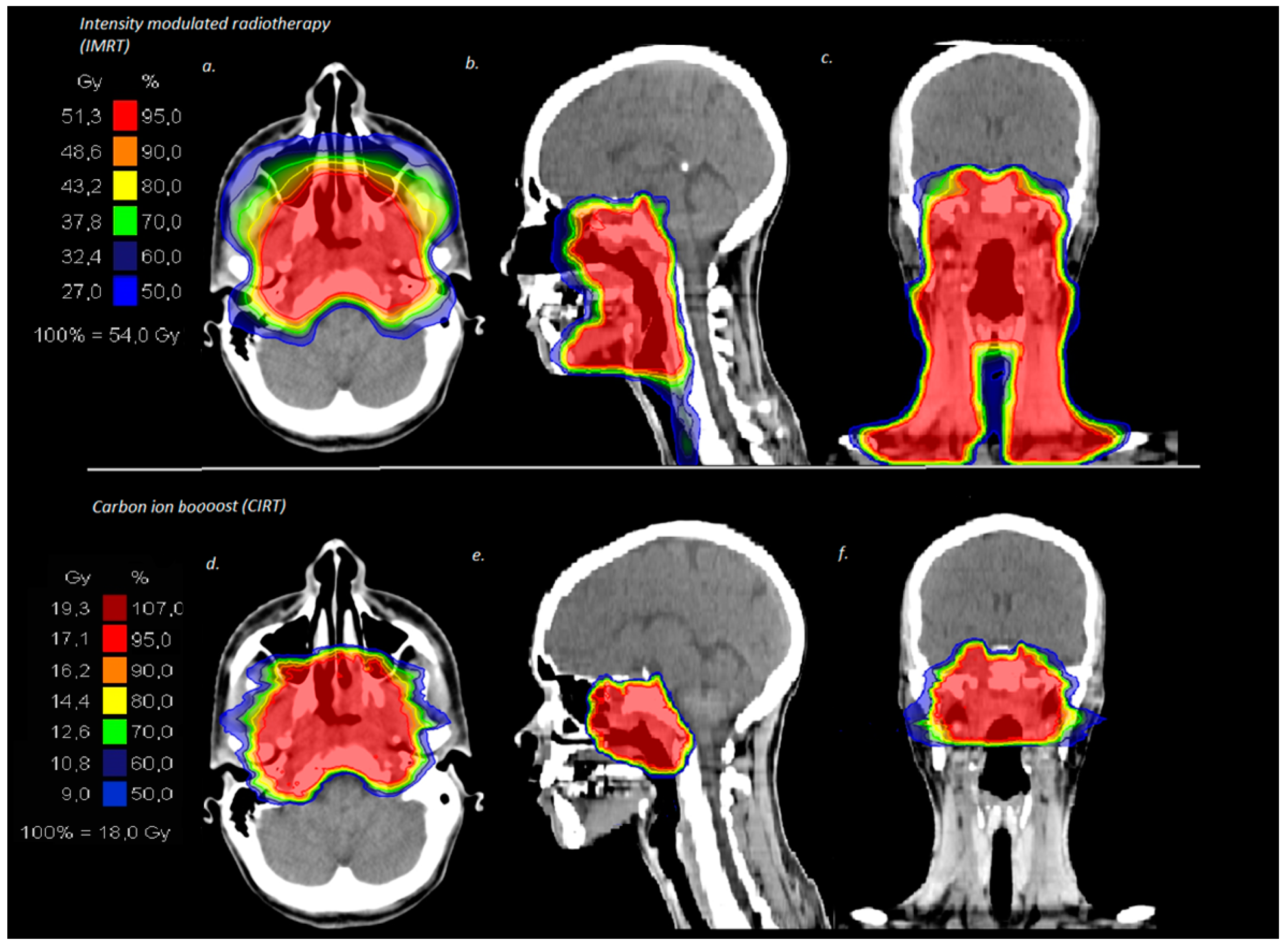
2.3. Treatment Features
3. Results
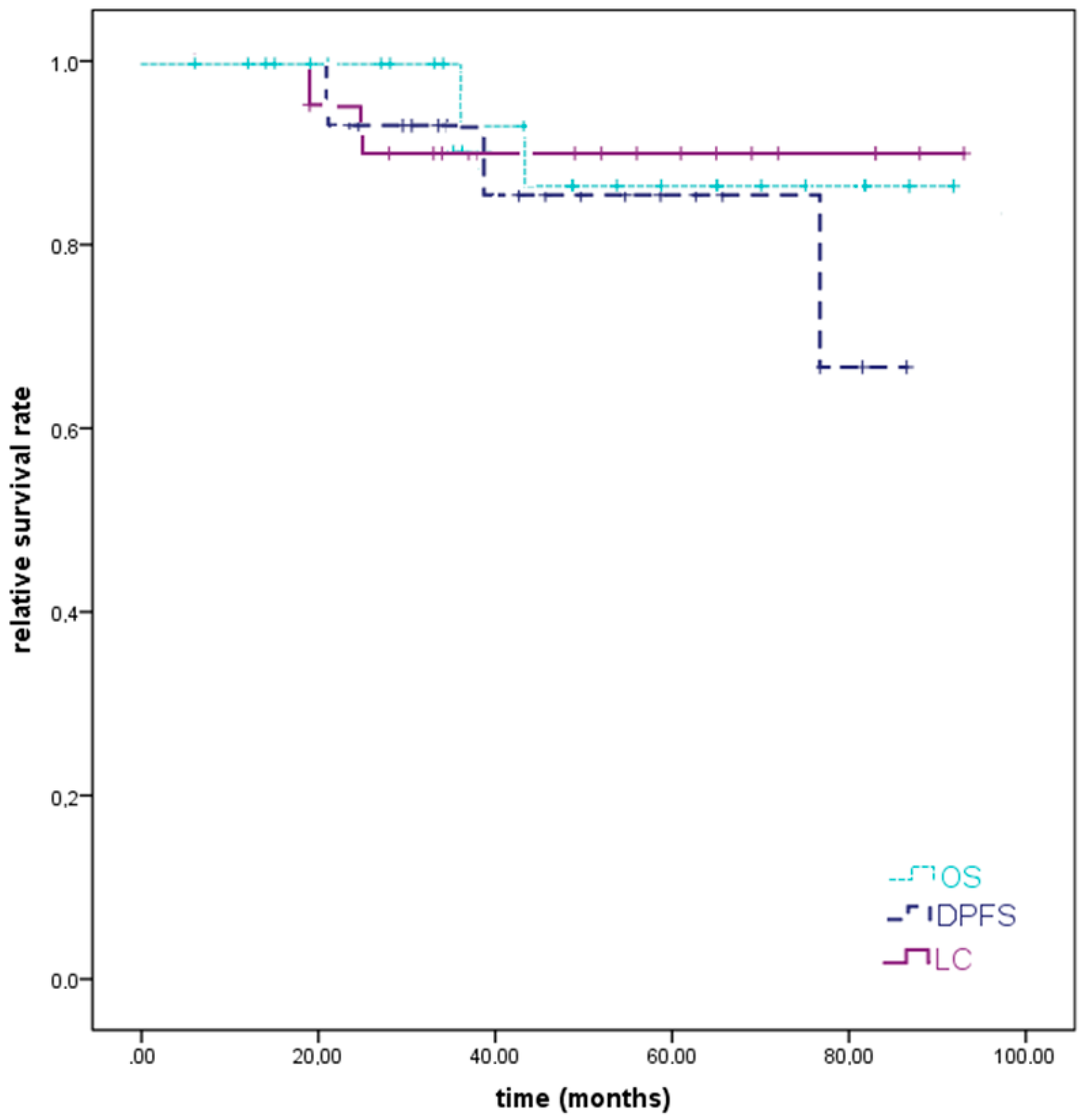
3.1. Survival Analysis
3.2. Toxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of Data and Material
Ethics Approval and Consent to Participate
Abbreviations
| ACC | adenoid cystic carcinoma |
| AJCC | American Joint Committee on Cancer |
| CIRT | carbon ion radiotherapy |
| CR | complete remission |
| CRT | chemoradiotherapy |
| CT | computed tomography |
| CTCAE | Common Terminology Criteria for Adverse Events |
| C12 | carbon ions |
| DPFS | distant progression-free survival |
| EQD2 | equivalent dose in 2 Gy fractions |
| HIT | Heidelberg Ion-Beam Therapy Center |
| LPFS | local progression-free survival |
| LC | local control |
| IMRT | intensity-modulated radiotherapy |
| MRI | magnetic resonance imaging |
| NPC | nasopharyngeal carcinoma |
| OS | overall survival |
| PR | partial remission |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| RT | radiotherapy |
| SD | stable disease |
| TNM | tumor, node, metastasis |
| UICC | International Union Against Cancer |
| WHO | World Health Organization |
References
- Ferlay, J.; Shin, H.R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- Barnes, L.; Eveson, J.W.; Reichert, P.; Sidransky, D. Pathology and genetics of head and neck tumors. In World Health Organization Classification of Tumors; IARC Press: Lyon, France, 2005. [Google Scholar]
- Pan, J.J.; Ng, W.T.; Zong, J.F.; Chan, L.L.; O’Sullivan, B.; Lin, S.J.; Sze, H.C.; Chen, Y.B.; Choi, H.C.; Guo, Q.J.; et al. Proposal for the 8th edition of the AJCC/UICC staging system for nasopharyngeal cancer in the era of intensity-modulated radiotherapy. Cancer 2016, 122, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Chua, M.L.K.; Wee, J.T.S.; Hui, E.P.; Chan, A.T.C. Nasopharyngeal carcinoma. Lancet 2016, 387, 1012–1024. [Google Scholar] [CrossRef]
- Chua, D.T.; Sham, J.S.; Kwong, D.L.; Au, G.K. Treatment outcome after radiotherapy alone for patients with Stage I-II nasopharyngeal carcinoma. Cancer 2003, 98, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Sze, W.M.; Au, J.S.; Leung, S.F.; Leung, T.W.; Chua, D.T.; Zee, B.C.; Law, S.C.; Teo, P.M.; Tung, S.Y.; et al. Treatment results for nasopharyngeal carcinoma in the modern era: The Hong Kong experience. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, P.; Lee, A.; Marguet, S.; Leclercq, J.; Ng, W.T.; Ma, J.; Chan, A.T.; Huang, P.Y.; Benhamou, E.; Zhu, G.; et al. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: An update of the MAC-NPC meta-analysis. Lancet Oncol. 2015, 16, 645–655. [Google Scholar] [CrossRef]
- Al-Sarraf, M.; LeBlanc, M.; Giri, P.G.; Fu, K.K.; Cooper, J.; Vuong, T.; Forastiere, A.A.; Adams, G.; Sakr, W.A.; Schuller, D.E.; et al. Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: Phase III randomized Intergroup study 0099. J. Clin. Oncol. 1998, 16, 1310–1317. [Google Scholar] [CrossRef]
- Chan, A.T.; Gregoire, V.; Lefebvre, J.L.; Licitra, L.; Hui, E.P.; Leung, S.F.; Felip, E.; Group, E.-E.-E.G.W. Nasopharyngeal cancer: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23 (Suppl. 7), vii83–vii85. [Google Scholar] [CrossRef]
- Chen, Q.Y.; Wen, Y.F.; Guo, L.; Liu, H.; Huang, P.Y.; Mo, H.Y.; Li, N.W.; Xiang, Y.Q.; Luo, D.H.; Qiu, F.; et al. Concurrent chemoradiotherapy vs radiotherapy alone in stage II nasopharyngeal carcinoma: Phase III randomized trial. J. Natl. Cancer Inst. 2011, 103, 1761–1770. [Google Scholar] [CrossRef]
- Ribassin-Majed, L.; Marguet, S.; Lee, A.W.M.; Ng, W.T.; Ma, J.; Chan, A.T.C.; Huang, P.Y.; Zhu, G.; Chua, D.T.T.; Chen, Y.; et al. What Is the Best Treatment of Locally Advanced Nasopharyngeal Carcinoma? An Individual Patient Data Network Meta-Analysis. J. Clin. Oncol. 2017, 35, 498–505. [Google Scholar] [CrossRef]
- Chen, L.; Hu, C.S.; Chen, X.Z.; Hu, G.Q.; Cheng, Z.B.; Sun, Y.; Li, W.X.; Chen, Y.Y.; Xie, F.Y.; Liang, S.B.; et al. Concurrent chemoradiotherapy plus adjuvant chemotherapy versus concurrent chemoradiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma: A phase 3 multicentre randomised controlled trial. Lancet Oncol. 2012, 13, 163–171. [Google Scholar] [CrossRef]
- Chen, L.; Hu, C.S.; Chen, X.Z.; Hu, G.Q.; Cheng, Z.B.; Sun, Y.; Li, W.X.; Chen, Y.Y.; Xie, F.Y.; Liang, S.B.; et al. Adjuvant chemotherapy in patients with locoregionally advanced nasopharyngeal carcinoma: Long-term results of a phase 3 multicentre randomised controlled trial. Eur. J. Cancer 2017, 75, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Li, W.F.; Chen, N.Y.; Zhang, N.; Hu, G.Q.; Xie, F.Y.; Sun, Y.; Chen, X.Z.; Li, J.G.; Zhu, X.D.; et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: A phase 3, multicentre, randomised controlled trial. Lancet Oncol. 2016, 17, 1509–1520. [Google Scholar] [CrossRef]
- Cao, S.M.; Yang, Q.; Guo, L.; Mai, H.Q.; Mo, H.Y.; Cao, K.J.; Qian, C.N.; Zhao, C.; Xiang, Y.Q.; Zhang, X.P.; et al. Neoadjuvant chemotherapy followed by concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: A phase III multicentre randomised controlled trial. Eur. J. Cancer 2017, 75, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Poon, Y.F.; Foo, W.; Law, S.C.; Cheung, F.K.; Chan, D.K.; Tung, S.Y.; Thaw, M.; Ho, J.H. Retrospective analysis of 5037 patients with nasopharyngeal carcinoma treated during 1976–1985: Overall survival and patterns of failure. Int. J. Radiat. Oncol. Biol. Phys. 1992, 23, 261–270. [Google Scholar] [CrossRef]
- Hsu, M.M.; Tu, S.M. Nasopharyngeal carcinoma in Taiwan. Clinical manifestations and results of therapy. Cancer 1983, 52, 362–368. [Google Scholar] [CrossRef]
- Peng, G.; Wang, T.; Yang, K.Y.; Zhang, S.; Zhang, T.; Li, Q.; Han, J.; Wu, G. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother. Oncol. 2012, 104, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Ng, W.T.; Chan, L.L.; Hung, W.M.; Chan, C.C.; Sze, H.C.; Chan, O.S.; Chang, A.T.; Yeung, R.M. Evolution of treatment for nasopharyngeal cancer--success and setback in the intensity-modulated radiotherapy era. Radiother. Oncol. 2014, 110, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Pow, E.H.; Kwong, D.L.; McMillan, A.S.; Wong, M.C.; Sham, J.S.; Leung, L.H.; Leung, W.K. Xerostomia and quality of life after intensity-modulated radiotherapy vs. conventional radiotherapy for early-stage nasopharyngeal carcinoma: Initial report on a randomized controlled clinical trial. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 981–991. [Google Scholar] [CrossRef]
- Kam, M.K.; Leung, S.F.; Zee, B.; Chau, R.M.; Suen, J.J.; Mo, F.; Lai, M.; Ho, R.; Cheung, K.Y.; Yu, B.K.; et al. Prospective randomized study of intensity-modulated radiotherapy on salivary gland function in early-stage nasopharyngeal carcinoma patients. J. Clin. Oncol. 2007, 25, 4873–4879. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Liu, M.Z.; Liang, S.B.; Zong, J.F.; Mao, Y.P.; Tang, L.L.; Guo, Y.; Lin, A.H.; Zeng, X.F.; Ma, J. Preliminary results of a prospective randomized trial comparing concurrent chemoradiotherapy plus adjuvant chemotherapy with radiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma in endemic regions of china. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Hui, E.P.; Ma, B.B.; Leung, S.F.; King, A.D.; Mo, F.; Kam, M.K.; Yu, B.K.; Chiu, S.K.; Kwan, W.H.; Ho, R.; et al. Randomized phase II trial of concurrent cisplatin-radiotherapy with or without neoadjuvant docetaxel and cisplatin in advanced nasopharyngeal carcinoma. J. Clin. Oncol. 2009, 27, 242–249. [Google Scholar] [CrossRef]
- Chew, N.K.; Sim, B.F.; Tan, C.T.; Goh, K.J.; Ramli, N.; Umapathi, P. Delayed post-irradiation bulbar palsy in nasopharyngeal carcinoma. Neurology 2001, 57, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Kwong, D.L.; Leung, S.F.; Tung, S.Y.; Sze, W.M.; Sham, J.S.; Teo, P.M.; Leung, T.W.; Wu, P.M.; Chappell, R.; et al. Factors affecting risk of symptomatic temporal lobe necrosis: Significance of fractional dose and treatment time. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 75–85. [Google Scholar] [CrossRef]
- Lam, H.C.; Abdullah, V.J.; Wormald, P.J.; Van Hasselt, C.A. Internal carotid artery hemorrhage after irradiation and osteoradionecrosis of the skull base. Otolaryngol. Head Neck Surg. 2001, 125, 522–527. [Google Scholar] [CrossRef]
- Lam, T.C.; Wong, F.C.; Leung, T.W.; Ng, S.H.; Tung, S.Y. Clinical outcomes of 174 nasopharyngeal carcinoma patients with radiation-induced temporal lobe necrosis. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e57–e65. [Google Scholar] [CrossRef]
- Siala, W.; Mnejja, W.; Abid, M.; Ghorbel, A.; Frikha, M.; Daoud, J. Thyroid toxicity after radiotherapy of nasopharyngeal carcinoma. Ann. Endocrinol. (Paris) 2011, 72, 19–23. [Google Scholar] [CrossRef]
- Taheri-Kadkhoda, Z.; Bjork-Eriksson, T.; Nill, S.; Wilkens, J.J.; Oelfke, U.; Johansson, K.A.; Huber, P.E.; Munter, M.W. Intensity-modulated radiotherapy of nasopharyngeal carcinoma: A comparative treatment planning study of photons and protons. Radiat. Oncol. 2008, 3, 4. [Google Scholar] [CrossRef]
- Widesott, L.; Pierelli, A.; Fiorino, C.; Dell’oca, I.; Broggi, S.; Cattaneo, G.M.; Di Muzio, N.; Fazio, F.; Calandrino, R.; Schwarz, M. Intensity-modulated proton therapy versus helical tomotherapy in nasopharynx cancer: Planning comparison and NTCP evaluation. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 589–596. [Google Scholar] [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef]
- Bentzen, S.M.; Constine, L.S.; Deasy, J.O.; Eisbruch, A.; Jackson, A.; Marks, L.B.; Ten Haken, R.K.; Yorke, E.D. Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC): An introduction to the scientific issues. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S3–S9. [Google Scholar] [CrossRef]
- Wei, W.I.; Sham, J.S. Nasopharyngeal carcinoma. Lancet 2005, 365, 2041–2054. [Google Scholar] [CrossRef]
- Altun, M.; Fandi, A.; Dupuis, O.; Cvitkovic, E.; Krajina, Z.; Eschwege, F. Undifferentiated nasopharyngeal cancer (UCNT): Current diagnostic and therapeutic aspects. Int. J. Radiat. Oncol. Biol. Phys. 1995, 32, 859–877. [Google Scholar] [CrossRef]
- Hu, J.; Bao, C.; Gao, J.; Guan, X.; Hu, W.; Yang, J.; Hu, C.; Kong, L.; Lu, J.J. Salvage treatment using carbon ion radiation in patients with locoregionally recurrent nasopharyngeal carcinoma: Initial results. Cancer 2018, 124, 2427–2437. [Google Scholar] [CrossRef]
- Kong, L.; Gao, J.; Hu, J.; Hu, W.; Guan, X.; Lu, R.; Lu, J.J. Phase I/II trial evaluating concurrent carbon-ion radiotherapy plus chemotherapy for salvage treatment of locally recurrent nasopharyngeal carcinoma. Chin. J. Cancer 2016, 35, 101. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Su, S.; Chen, C.; Han, F.; Zhao, C.; Xiao, W.; Deng, X.; Huang, S.; Lin, C.; Lu, T. Long-term outcomes of intensity-modulated radiotherapy for 868 patients with nasopharyngeal carcinoma: An analysis of survival and treatment toxicities. Radiother. Oncol. 2014, 110, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Geara, F.B.; Sanguineti, G.; Tucker, S.L.; Garden, A.S.; Ang, K.K.; Morrison, W.H.; Peters, L.J. Carcinoma of the nasopharynx treated by radiotherapy alone: Determinants of distant metastasis and survival. Radiother. Oncol. 1997, 43, 53–61. [Google Scholar] [CrossRef]
- Le, Q.T.; Jones, C.D.; Yau, T.K.; Shirazi, H.A.; Wong, P.H.; Thomas, E.N.; Patterson, B.K.; Lee, A.W.; Zehnder, J.L. A comparison study of different PCR assays in measuring circulating plasma epstein-barr virus DNA levels in patients with nasopharyngeal carcinoma. Clin. Cancer Res. 2005, 11, 5700–5707. [Google Scholar] [CrossRef]
- Leung, S.F.; Zee, B.; Ma, B.B.; Hui, E.P.; Mo, F.; Lai, M.; Chan, K.C.; Chan, L.Y.; Kwan, W.H.; Lo, Y.M.; et al. Plasma Epstein-Barr viral deoxyribonucleic acid quantitation complements tumor-node-metastasis staging prognostication in nasopharyngeal carcinoma. J. Clin. Oncol. 2006, 24, 5414–5418. [Google Scholar] [CrossRef]
- Rossi, A.; Molinari, R.; Boracchi, P.; Del Vecchio, M.; Marubini, E.; Nava, M.; Morandi, L.; Zucali, R.; Pilotti, S.; Grandi, C.; et al. Adjuvant chemotherapy with vincristine, cyclophosphamide, and doxorubicin after radiotherapy in local-regional nasopharyngeal cancer: Results of a 4-year multicenter randomized study. J. Clin. Oncol. 1988, 6, 1401–1410. [Google Scholar] [CrossRef] [PubMed]
- Lorch, J.H.; Goloubeva, O.; Haddad, R.I.; Cullen, K.; Sarlis, N.; Tishler, R.; Tan, M.; Fasciano, J.; Sammartino, D.E.; Posner, M.R.; et al. Induction chemotherapy with cisplatin and fluorouracil alone or in combination with docetaxel in locally advanced squamous-cell cancer of the head and neck: Long-term results of the TAX 324 randomised phase 3 trial. Lancet Oncol. 2011, 12, 153–159. [Google Scholar] [CrossRef]
- Vermorken, J.B.; Remenar, E.; van Herpen, C.; Gorlia, T.; Mesia, R.; Degardin, M.; Stewart, J.S.; Jelic, S.; Betka, J.; Preiss, J.H.; et al. Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. N. Engl. J. Med. 2007, 357, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, K.; Demizu, Y.; Hashimoto, N.; Mima, M.; Terashima, K.; Fujii, O.; Otsuki, N.; Murakami, M.; Fuwa, N.; Nibu, K. Particle radiotherapy using protons or carbon ions for unresectable locally advanced head and neck cancers with skull base invasion. Jpn. J. Clin. Oncol. 2014, 44, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Madani, I.; Bonte, K.; Vakaet, L.; Boterberg, T.; De Neve, W. Intensity-modulated radiotherapy for sinonasal tumors: Ghent University Hospital update. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.T.; Kamat, U.R.; Liebsch, N.J.; Curry, W.T.; Lin, D.T.; Barker, F.G., 2nd; Loeffler, J.S.; Chan, A.W. Proton radiation therapy for primary sphenoid sinus malignancies: Treatment outcome and prognostic factors. Head Neck 2009, 31, 1297–1308. [Google Scholar] [CrossRef]
- Pommier, P.; Liebsch, N.J.; Deschler, D.G.; Lin, D.T.; McIntyre, J.F.; Barker, F.G., 2nd; Adams, J.A.; Lopes, V.V.; Varvares, M.; Loeffler, J.S.; et al. Proton beam radiation therapy for skull base adenoid cystic carcinoma. Arch. Otolaryngol. Head Neck Surg. 2006, 132, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.D.; Zhou, G.Q.; Lv, J.W.; Zhou, H.Q.; Zhong, C.W.; Wu, C.F.; Zheng, Z.Q.; He, X.J.; Peng, L.; Ma, J.; et al. Competing risk nomograms for nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: A big-data, intelligence platform-based analysis. Radiother. Oncol. 2018, 129, 389–395. [Google Scholar] [CrossRef]
- Jensen, A.D.; Nikoghosyan, A.V.; Windemuth-Kieselbach, C.; Debus, J.; Munter, M.W. Treatment of malignant sinonasal tumours with intensity-modulated radiotherapy (IMRT) and carbon ion boost (C12). BMC Cancer 2011, 11, 190. [Google Scholar] [CrossRef]
- Xiao, W.W.; Huang, S.M.; Han, F.; Wu, S.X.; Lu, L.X.; Lin, C.G.; Deng, X.W.; Lu, T.X.; Cui, N.J.; Zhao, C. Local control, survival, and late toxicities of locally advanced nasopharyngeal carcinoma treated by simultaneous modulated accelerated radiotherapy combined with cisplatin concurrent chemotherapy: Long-term results of a phase 2 study. Cancer 2011, 117, 1874–1883. [Google Scholar] [CrossRef]
- Zheng, Y.; Han, F.; Xiao, W.; Xiang, Y.; Lu, L.; Deng, X.; Cui, N.; Zhao, C. Analysis of late toxicity in nasopharyngeal carcinoma patients treated with intensity modulated radiation therapy. Radiat. Oncol. 2015, 10, 17. [Google Scholar] [CrossRef]
- Wang, W.; Feng, M.; Fan, Z.; Li, J.; Lang, J. Clinical outcomes and prognostic factors of 695 nasopharyngeal carcinoma patients treated with intensity-modulated radiotherapy. Biomed. Res. Int. 2014, 2014, 814948. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.A.; Tang, Y.; Lui, C.C.; Huang, Y.J.; Huang, E.Y. Treatment outcomes and late complications of 849 patients with nasopharyngeal carcinoma treated with radiotherapy alone. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 672–679. [Google Scholar] [CrossRef]
- Sumitsawan, Y.; Chaiyasate, S.; Chitapanarux, I.; Anansuthiwara, M.; Roongrotwattanasiri, K.; Vaseenon, V.; Tooncam, H. Late complications of radiotherapy for nasopharyngeal carcinoma. Auris Nasus Larynx 2009, 36, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, K.Y.; Yeh, S.A.; Chang, C.C.; Tsai, P.C.; Wu, J.M.; Gau, J.S. Cognitive function before and after intensity-modulated radiation therapy in patients with nasopharyngeal carcinoma: A prospective study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Teo, P.M.; Leung, S.F.; Chan, A.T.; Leung, T.W.; Choi, P.H.; Kwan, W.H.; Lee, W.Y.; Chau, R.M.; Yu, P.K.; Johnson, P.J. Final report of a randomized trial on altered-fractionated radiotherapy in nasopharyngeal carcinoma prematurely terminated by significant increase in neurologic complications. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 1311–1322. [Google Scholar] [CrossRef]
- Yeh, S.A.; Ho, J.T.; Lui, C.C.; Huang, Y.J.; Hsiung, C.Y.; Huang, E.Y. Treatment outcomes and prognostic factors in patients with supratentorial low-grade gliomas. Br. J. Radiol 2005, 78, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Schlampp, I.; Karger, C.P.; Jakel, O.; Scholz, M.; Didinger, B.; Nikoghosyan, A.; Hoess, A.; Kramer, M.; Edler, L.; Debus, J.; et al. Temporal lobe reactions after radiotherapy with carbon ions: Incidence and estimation of the relative biological effectiveness by the local effect model. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 815–823. [Google Scholar] [CrossRef]
- Pehlivan, B.; Ares, C.; Lomax, A.J.; Stadelmann, O.; Goitein, G.; Timmermann, B.; Schneider, R.A.; Hug, E.B. Temporal lobe toxicity analysis after proton radiation therapy for skull base tumors. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 1432–1440. [Google Scholar] [CrossRef]
- Huang, J.; Kong, F.F.; Oei, R.W.; Zhai, R.P.; Hu, C.S.; Ying, H.M. Dosimetric predictors of temporal lobe injury after intensity-modulated radiotherapy for T4 nasopharyngeal carcinoma: A competing risk study. Radiat. Oncol. 2019, 14, 31. [Google Scholar] [CrossRef]
- Sanguineti, G.; Geara, F.B.; Garden, A.S.; Tucker, S.L.; Ang, K.K.; Morrison, W.H.; Peters, L.J. Carcinoma of the nasopharynx treated by radiotherapy alone: Determinants of local and regional control. Int. J. Radiat. Oncol. Biol. Phys. 1997, 37, 985–996. [Google Scholar] [CrossRef]
- Kong, L.; Lu, J.J.; Liss, A.L.; Hu, C.; Guo, X.; Wu, Y.; Zhang, Y. Radiation-induced cranial nerve palsy: A cross-sectional study of nasopharyngeal cancer patients after definitive radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1421–1427. [Google Scholar] [CrossRef] [PubMed]
- Urie, M.M.; Fullerton, B.; Tatsuzaki, H.; Birnbaum, S.; Suit, H.D.; Convery, K.; Skates, S.; Goitein, M. A dose response analysis of injury to cranial nerves and/or nuclei following proton beam radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 1992, 23, 27–39. [Google Scholar] [CrossRef]
- Demizu, Y.; Murakami, M.; Miyawaki, D.; Niwa, Y.; Akagi, T.; Sasaki, R.; Terashima, K.; Suga, D.; Kamae, I.; Hishikawa, Y. Analysis of Vision loss caused by radiation-induced optic neuropathy after particle therapy for head-and-neck and skull-base tumors adjacent to optic nerves. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1487–1492. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. (%) |
|---|---|
| median age | 49 (28–73) years |
| gender | |
| male | 11 (42) |
| female | 15 (58) |
| Karnofsky performance score in % | |
| 100 | 6 (23) |
| 90 | 9 (35) |
| 80 | 5 (19) |
| 70 | 4 (15) |
| 60 | 2 (8) |
| nicotine abuse | |
| yes | 9 (35) |
| no | 17 (65) |
| alcohol abuse | |
| yes | 5 (19) |
| no | 21 (81) |
| histology | |
| WHO I | 3 (12) |
| WHO II | 7 (27) |
| WHO III | 16 (62) |
| UICC stage | |
| I | 1 (4) |
| II | 1 (4) |
| III | 6 (23) |
| IVA | 15 (58) |
| IVB | 3 (12) |
| IVC | none |
| TNM stage | |
| T1 | 2 (8) |
| T2 | 1 (4) |
| T3 | 7 (27) |
| T4 | 16 (62) |
| T4 with skull base infiltration | 11 (42) |
| N0 | 8 (31) |
| N+ | 14 (54) |
| Nx | 4 (15) |
| M0 | 26 (100) |
| definitive RT | 17 (65) |
| postoperative RT | 9 (35) |
| Rx | 2 (8) |
| R1 | 3 (12) |
| R2 | 4 (15) |
| therapy regimes | |
| 50 Gy/2 Gy IMRT + 24 Gy/3 Gy (RBE) C12 | 5 (19) |
| 56 Gy/2 Gy IMRT + 18 Gy/3 Gy (RBE) C12 | 21 (81) |
| median total dose | 74 Gy (RBE) (72–74 Gy (RBE)) |
| median CTV1 | 118 cc (24–324 cc) |
| median CTV2 | 481 cc (131–1070 cc) |
| concomitant chemotherapy | 0 |
| cisplatin 40 mg/m2 weekly | 19 (73) |
| cisplatin and fluorouracil | 1 (4) |
| carboplatin and fluorouracil | 1 (4) |
| Characteristic | Acute Toxicity, No. (%) | Chronic Toxicity, No. (%) | |||
|---|---|---|---|---|---|
| Under RT and Until 6 Weeks Post RT | 3–6 Months Post RT | 12 Months Post RT | 24 Months Post RT | At Last Follow-Up | |
| toxicity | |||||
| <grade 3 | 21 (84) | 14 (56) | 11 (44) | 8 (32) | 9 (36) |
| =grade 3 | 5 (20) | 3 (12) | 4 (16) | 4 (16) | 4 (16) |
| >grade 3 | 0 | 0 | 0 | 0 | 0 |
| mucositis | |||||
| grade 1 | 6 (24) | 4 (16) | 0 | 0 | 0 |
| grade 2 | 12 (48) | 0 | 0 | 0 | 0 |
| grade 3 | 5 (20) | 0 | 0 | 0 | 0 |
| dermatitis | |||||
| grade 1 | 8 (32) | 3 (12) | 0 | 0 | 0 |
| grade 2 | 5 (20) | 0 | 0 | 0 | 0 |
| grade 3 | 1 (4) | 0 | 0 | 0 | 0 |
| dysphagia | |||||
| grade 1 | 5 (20) | 4 (16) | 3 (12) | 3 (12) | 3 (12) |
| grade 2 | 7 (28) | 1 (4) | 0 | 0 | 0 |
| grade 3 | 4 (16) | 0 | 0 | 0 | 0 |
| odynophagia | |||||
| grade 1 | 5 (20) | 4 (16) | 0 | 0 | 0 |
| grade 2 | 8 (32) | 0 | 0 | 0 | 0 |
| grade 3 | 4 (16) | 0 | 0 | 0 | 0 |
| hyposmia | |||||
| grade 1 | 3 (12) | 3 (12) | 3 (12) | 0 | 0 |
| grade 2 | 3 (12) | 1 (4) | 0 | 0 | 0 |
| grade 3 | 1 (4) | 0 | 0 | 0 | 0 |
| xerostomia | |||||
| grade 1 | 8 (32) | 9 (36) | 8 (32) | 7 (28) | 7 (28) |
| grade 2 | 7 (28) | 4 (16) | 1 (4) | 1 (4) | 1 (4) |
| gastric tube dependence | 6 (24) | 1 (4) | 0 | 0 | 0 |
| keratoconjunctivitis sicca | |||||
| grade 1 | 1 (4) | 1 (4) | 1 (4) | 1 (4) | 1 (4) |
| grade 2 | 3 (12) | 1 (4) | 0 | 0 | 0 |
| grade 3 | 1 (4) | 1 (4) | 1 (4) | 1 (4) | 1 (4) |
| tympanic effusion | |||||
| grade 1 | 9 (36) | 7 (28) | 7 (28) | 5 (20) | 5 (20) |
| grade 2 | 8 (32) | 3 (12) | 3 (12) | 2 (8)) | 2 (8) |
| cranial nerves affected | |||||
| auditory nerve | |||||
| grade 2 | 2 (8) | 0 | 0 | 0 | 0 |
| abducent nerve | |||||
| grade 1 | 0 | 1 (4) | 0 | 0 | 1 (4) |
| hypoglossal nerve | |||||
| grade 2 | 0 | 0 | 0 | 1 (4) | 0 |
| facial nerve | |||||
| grade 2 | 0 | 0 | 0 | 0 | 1 (4) |
| temporal lobe necrosis | |||||
| grade 1 | 0 | 0 | 1 (4) | 0 | 0 |
| grade 2 | 0 | 0 | 0 | 0 | 1 (4) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akbaba, S.; Held, T.; Lang, K.; Forster, T.; Federspil, P.; Herfarth, K.; Häfner, M.; Plinkert, P.; Rieken, S.; Debus, J.; et al. Bimodal Radiotherapy with Active Raster-Scanning Carbon Ion Radiotherapy and Intensity-Modulated Radiotherapy in High-Risk Nasopharyngeal Carcinoma Results in Excellent Local Control. Cancers 2019, 11, 379. https://doi.org/10.3390/cancers11030379
Akbaba S, Held T, Lang K, Forster T, Federspil P, Herfarth K, Häfner M, Plinkert P, Rieken S, Debus J, et al. Bimodal Radiotherapy with Active Raster-Scanning Carbon Ion Radiotherapy and Intensity-Modulated Radiotherapy in High-Risk Nasopharyngeal Carcinoma Results in Excellent Local Control. Cancers. 2019; 11(3):379. https://doi.org/10.3390/cancers11030379
Chicago/Turabian StyleAkbaba, Sati, Thomas Held, Kristin Lang, Tobias Forster, Philippe Federspil, Klaus Herfarth, Matthias Häfner, Peter Plinkert, Stefan Rieken, Jürgen Debus, and et al. 2019. "Bimodal Radiotherapy with Active Raster-Scanning Carbon Ion Radiotherapy and Intensity-Modulated Radiotherapy in High-Risk Nasopharyngeal Carcinoma Results in Excellent Local Control" Cancers 11, no. 3: 379. https://doi.org/10.3390/cancers11030379