
Pre-Existing Humoral Immunological Memory Is Retained in Patients with Multiple Sclerosis Receiving Cladribine Therapy

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethics
2.3. Blood Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
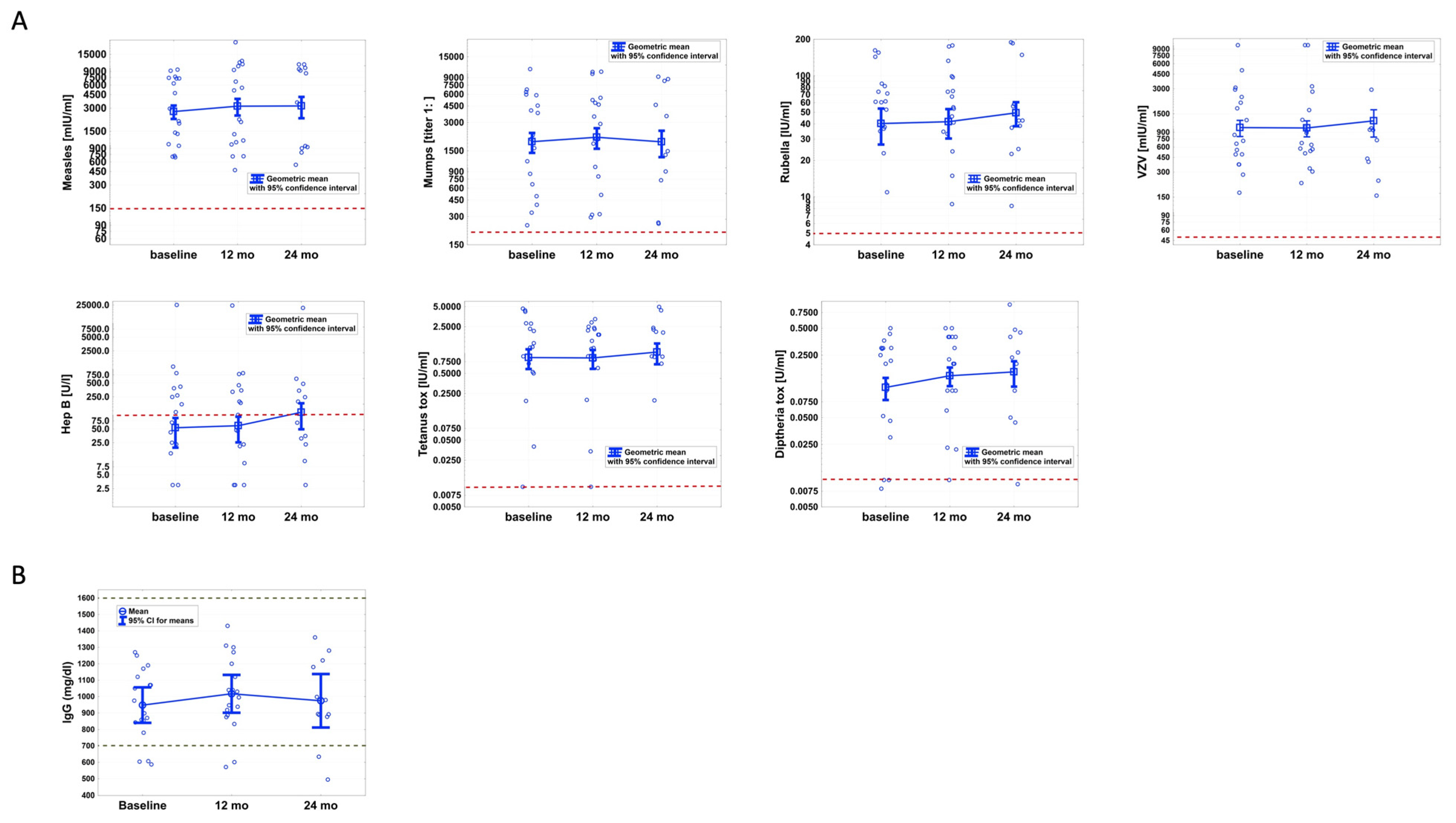
3.2. CLAD Has No Effect on Pathogen-Specific Blood Antibody Levels
3.3. Blood IgG Synthesis Is Not Altered during CLAD Therapy
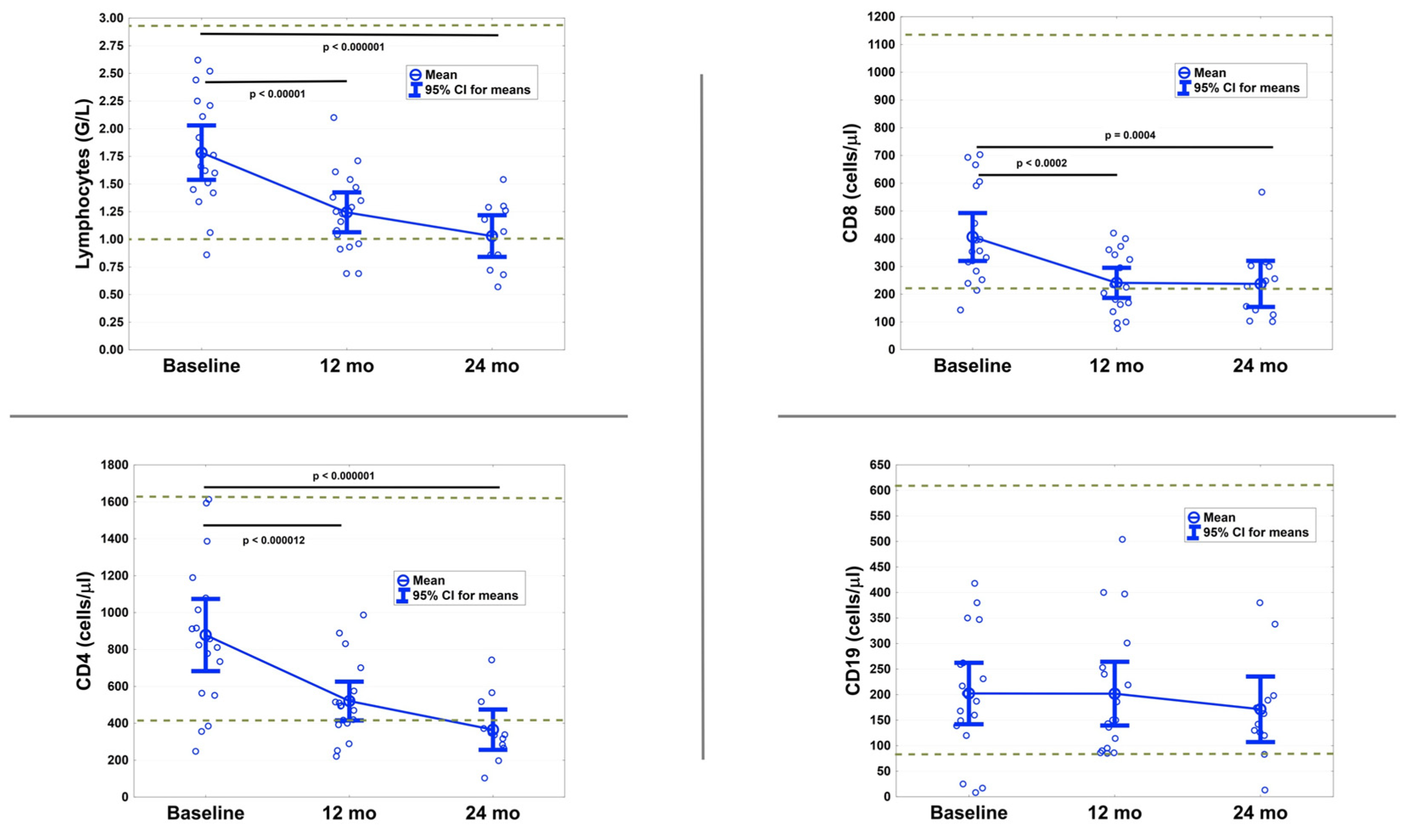
3.4. T Cells Are Significantly Reduced after 12 and 24 Months
3.5. No Serious Infections Occurred
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Pathogen | Cute Off | Kit | Manufacturer | Instrument | Method |
|---|---|---|---|---|---|
| Measles | >150 mIU/mL | Anti-Masern ELISA (IgG) | Euroimmun * | Euroimmun Analyzer I (EUROIMMUN) | ELISA |
| Mumps | >1:231 | Anti-Mumps ELISA (IgG) | Euroimmun * | Euroimmun Analyzer I | ELISA |
| VZV | >50 mIU/mL | Anti-VZV ELISA (IgG) | Euroimmun * | Euroimmun Analyzer I | ELISA |
| Rubella | >5 IU/mL | Alinity Rubella IgG assay | Abbott Diagnostics (Illinois, USA) | Architect i2000SR (Abbott Diagnostics) | CMIA |
| Hepatitis B | >100 U/L | Alinity Anti-HBs assay | Abbott Diagnostics (Illinois, USA) | Architect i2000SR (Abbott Diagnostics) | CMIA |
| Diphtheria | >0.01 U/mL | Anti-Diphteria Toxin ELISA (IgG) | Euroimmun * | Euroimmun Analyzer I | ELISA |
| Tetanus | >0.01 IU/mL | Anti-TetanusToxin ELISA (IgG) | Euroimmun * | Euroimmun Analyzer I | ELISA |
References
- Giovannoni, G. Cladribine to Treat Relapsing Forms of Multiple Sclerosis. Neurotherapeutics 2017, 14, 874–887. [Google Scholar] [CrossRef] [Green Version]
- Moser, T.; Akgun, K.; Proschmann, U.; Sellner, J.; Ziemssen, T. The role of TH17 cells in multiple sclerosis: Therapeutic implications. Autoimmun. Rev. 2020, 19, 102647. [Google Scholar] [CrossRef]
- Baker, D.; Marta, M.; Pryce, G.; Giovannoni, G.; Schmierer, K. Memory B Cells are Major Targets for Effective Immunotherapy in Relapsing Multiple Sclerosis. EBioMedicine 2017, 16, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moser, T.; Schwenker, K.; Seiberl, M.; Feige, J.; Akgun, K.; Haschke-Becher, E.; Ziemssen, T.; Sellner, J. Long-term peripheral immune cell profiling reveals further targets of oral cladribine in MS. Ann. Clin. Transl. Neurol. 2020, 7, 2199–2212. [Google Scholar] [CrossRef]
- Ceronie, B.; Jacobs, B.M.; Baker, D.; Dubuisson, N.; Mao, Z.; Ammoscato, F.; Lock, H.; Longhurst, H.J.; Giovannoni, G.; Schmierer, K. Cladribine treatment of multiple sclerosis is associated with depletion of memory B cells. J. Neurol. 2018, 265, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Stuve, O.; Soelberg Soerensen, P.; Leist, T.; Giovannoni, G.; Hyvert, Y.; Damian, D.; Dangond, F.; Boschert, U. Effects of cladribine tablets on lymphocyte subsets in patients with multiple sclerosis: An extended analysis of surface markers. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419854986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, S.; Vermersch, P.; Comi, G.; Giovannoni, G.; Rammohan, K.; Rieckmann, P.; Sorensen, P.S.; Hamlett, A.; Miret, M.; Weiner, J.; et al. Safety and tolerability of cladribine tablets in multiple sclerosis: The CLARITY (CLAdRIbine Tablets treating multiple sclerosis orallY) study. Mult. Scler. 2011, 17, 578–593. [Google Scholar] [CrossRef]
- Giovannoni, G.; Comi, G.; Cook, S.; Rammohan, K.; Rieckmann, P.; Soelberg Sorensen, P.; Vermersch, P.; Chang, P.; Hamlett, A.; Musch, B.; et al. A placebo-controlled trial of oral cladribine for relapsing multiple sclerosis. N. Engl. J. Med. 2010, 362, 416–426. [Google Scholar] [CrossRef] [Green Version]
- Comi, G.; Cook, S.; Rammohan, K.; Soelberg Sorensen, P.; Vermersch, P.; Adeniji, A.K.; Dangond, F.; Giovannoni, G. Long-term effects of cladribine tablets on MRI activity outcomes in patients with relapsing-remitting multiple sclerosis: The CLARITY Extension study. Ther. Adv. Neurol. Disord. 2018, 11, 1756285617753365. [Google Scholar] [CrossRef]
- Ali, M.G.; Zhang, Z.; Gao, Q.; Pan, M.; Rowan, E.G.; Zhang, J. Recent advances in therapeutic applications of neutralizing antibodies for virus infections: An overview. Immunol. Res. 2020, 68, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Pulendran, B.; Davis, M.M. The science and medicine of human immunology. Science 2020, 369. [Google Scholar] [CrossRef]
- Burbelo, P.D.; Ching, K.H.; Bush, E.R.; Han, B.L.; Iadarola, M.J. Antibody-profiling technologies for studying humoral responses to infectious agents. Expert Rev. Vaccines 2010, 9, 567–578. [Google Scholar] [CrossRef]
- Rejdak, K.; Stelmasiak, Z.; Grieb, P. Cladribine induces long lasting oligoclonal bands disappearance in relapsing multiple sclerosis patients: 10-year observational study. Mult. Scler. Relat. Disord. 2019, 27, 117–120. [Google Scholar] [CrossRef]
- Ward, E.S.; Ober, R.J. Targeting FcRn to Generate Antibody-Based Therapeutics. Trends Pharm. Sci. 2018, 39, 892–904. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Leist, T.; Comi, G.; Montalban, X.; Giovannoni, G.; Nolting, A.; Hicking, C.; Galazka, A.; Sylvester, E. Safety of cladribine tablets in the treatment of patients with multiple sclerosis: An integrated analysis. Mult. Scler. Relat. Disord. 2019, 29, 157–167. [Google Scholar] [CrossRef] [Green Version]
- Leist, T.P.; Comi, G.; Cree, B.A.C.; Coyle, P.K.; Freedman, M.S.; Hartung, H.-P.; Vermersch, P.; Casset-Semanaz, F.; Scaramozza, M. Effect of oral cladribine on time to conversion to clinically definite multiple sclerosis in patients with a first demyelinating event (ORACLE MS): A phase 3 randomised trial. Lancet Neurol. 2014, 13, 257–267. [Google Scholar] [CrossRef]
- Giovannoni, G.; Soelberg Sorensen, P.; Cook, S.; Rammohan, K.; Rieckmann, P.; Comi, G.; Dangond, F.; Adeniji, A.K.; Vermersch, P. Safety and efficacy of cladribine tablets in patients with relapsing-remitting multiple sclerosis: Results from the randomized extension trial of the CLARITY study. Mult. Scler. 2018, 24, 1594–1604. [Google Scholar] [CrossRef] [Green Version]
- Wray, S.; Havrdova, E.; Snydman, D.R.; Arnold, D.L.; Cohen, J.A.; Coles, A.J.; Hartung, H.P.; Selmaj, K.W.; Weiner, H.L.; Daizadeh, N.; et al. Infection risk with alemtuzumab decreases over time: Pooled analysis of 6-year data from the CAMMS223, CARE-MS I, and CARE-MS II studies and the CAMMS03409 extension study. Mult. Scler. 2019, 25, 1605–1617. [Google Scholar] [CrossRef] [PubMed]
- Farez, M.F.; Correale, J.; Armstrong, M.J.; Rae-Grant, A.; Gloss, D.; Donley, D.; Holler-Managan, Y.; Kachuck, N.J.; Jeffery, D.; Beilman, M.; et al. Practice guideline update summary: Vaccine-preventable infections and immunization in multiple sclerosis: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2019, 93, 584–594. [Google Scholar] [CrossRef] [Green Version]
- Achiron, A.; Mandel, M.; Dreyer-Alster, S.; Harari, G.; Magalashvili, D.; Sonis, P.; Dolev, M.; Menascu, S.; Flechter, S.; Falb, R.; et al. Humoral immune response to COVID-19 mRNA vaccine in patients with multiple sclerosis treated with high-efficacy disease-modifying therapies. Ther. Adv. Neurol. Disord. 2021, 14, 17562864211012835. [Google Scholar] [CrossRef] [PubMed]
- Sormani, M.P.; Inglese, M.; Schiavetti, I.; Carmisciano, L.; Laroni, A.; Lapucci, C.; Da Rin, G.; Serrati, C.; Gandoglia, I.; Tassinari, T.; et al. Effect of SARS-CoV-2 mRNA vaccination in MS patients treated with disease modifying therapies. EBioMedicine 2021, 103581. [Google Scholar] [CrossRef] [PubMed]
- Drulovic, J.; Ivanovic, J.; Martinovic, V.; Tamas, O.; Veselinovic, N.; Cujic, D.; Gnjatovic, M.; Mesaros, S.; Pekmezovic, T. Humoral response to SARS-CoV-2 COVID-19 vaccines in patients with multiple sclerosis treated with immune reconstitution therapies. Mult. Scler. Relat. Disord. 2021, 54, 103150. [Google Scholar] [CrossRef]
- Mohn, N.; Pfeuffer, S.; Ruck, T.; Gross, C.C.; Skripuletz, T.; Klotz, L.; Wiendl, H.; Stangel, M.; Meuth, S.G. Alemtuzumab therapy changes immunoglobulin levels in peripheral blood and CSF. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7. [Google Scholar] [CrossRef] [Green Version]
- Derfuss, T.; Weber, M.; Hughes, R.; Wang, Q.; Sauter, A.; Koendgen, H.; Hauser, S.L.; Bar-Or, A.; Hartung, H.-P. Serum immunoglobulin levels and risk of serious infections in the pivotal Phase III trials of ocrelizumab in multiple sclerosis and their open-label extensions. Mult. Scler. 2019, 25, 20. [Google Scholar] [CrossRef]
- Cyster, J.G.; Allen, C.D.C. B Cell Responses: Cell Interaction Dynamics and Decisions. Cell 2019, 177, 524–540. [Google Scholar] [CrossRef] [Green Version]
- Hermann, R.; Karlsson, M.O.; Novakovic, A.M.; Terranova, N.; Fluck, M.; Munafo, A. The Clinical Pharmacology of Cladribine Tablets for the Treatment of Relapsing Multiple Sclerosis. Clin. Pharm. 2019, 58, 283–297. [Google Scholar] [CrossRef] [Green Version]
- Probstel, A.K.; Hauser, S.L. Multiple Sclerosis: B Cells Take Center Stage. J. Neuroophthalmol. 2018, 38, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Richards, S.; Surks, H.K.; Jacobs, A.; Panzara, M.A. Clinical pharmacology of alemtuzumab, an anti-CD52 immunomodulator, in multiple sclerosis. Clin. Exp. Immunol. 2018, 194, 295–314. [Google Scholar] [CrossRef] [Green Version]


| No. | 18 |
| Female/Male (%) | 14/4 (78/22) |
| Mean Age, y (±SD) | 36.7 (8.8) |
| Mean Disease Duration, Mo (±SD) | 103.6 (97.6) |
| Median EDSS (IQR) | 1.75 (1–3.5) |
| Mean CD19+ B Cell Count/µL, (95% CI of the Mean); normal range: 80–616 | 202.2 (146.0–258.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moser, T.; O’Sullivan, C.; Puttinger, C.; Feige, J.; Pilz, G.; Haschke-Becher, E.; Cadamuro, J.; Oberkofler, H.; Hitzl, W.; Harrer, A.; et al. Pre-Existing Humoral Immunological Memory Is Retained in Patients with Multiple Sclerosis Receiving Cladribine Therapy. Biomedicines 2021, 9, 1584. https://doi.org/10.3390/biomedicines9111584
Moser T, O’Sullivan C, Puttinger C, Feige J, Pilz G, Haschke-Becher E, Cadamuro J, Oberkofler H, Hitzl W, Harrer A, et al. Pre-Existing Humoral Immunological Memory Is Retained in Patients with Multiple Sclerosis Receiving Cladribine Therapy. Biomedicines. 2021; 9(11):1584. https://doi.org/10.3390/biomedicines9111584
Chicago/Turabian StyleMoser, Tobias, Ciara O’Sullivan, Christian Puttinger, Julia Feige, Georg Pilz, Elisabeth Haschke-Becher, Janne Cadamuro, Hannes Oberkofler, Wolfgang Hitzl, Andrea Harrer, and et al. 2021. "Pre-Existing Humoral Immunological Memory Is Retained in Patients with Multiple Sclerosis Receiving Cladribine Therapy" Biomedicines 9, no. 11: 1584. https://doi.org/10.3390/biomedicines9111584