 Giulia M. Giordano1
Giulia M. Giordano1 Pasquale Pezzella1
Pasquale Pezzella1 Armida Mucci1*
Armida Mucci1* Stephen F. Austin2
Stephen F. Austin2 Andreas Erfurth3
Andreas Erfurth3 Birte Glenthøj4,5
Birte Glenthøj4,5 Alex Hofer6
Alex Hofer6 Jan Hubenak7
Jan Hubenak7 Jan Libiger7
Jan Libiger7 Ingrid Melle8
Ingrid Melle8 Mette Ø. Nielsen4,5
Mette Ø. Nielsen4,5 Janusz K. Rybakowski9
Janusz K. Rybakowski9 Pawel Wojciak9
Pawel Wojciak9 Silvana Galderisi1†
Silvana Galderisi1† Gabriele Sachs10†
Gabriele Sachs10†- 1Department of Psychiatry, University of Campania “Luigi Vanvitelli”, Naples, Italy
- 2Psychiatric Research Unit, Region Zealand Psychiatry, Slagelse, Denmark
- 36th Psychiatric Department, Otto-Wagner-Spital, Vienna, Austria
- 4Center for Neuropsychiatric Schizophrenia Research (CNSR) and Center for Clinical Intervention and Neuropsychiatric Schizophrenia Research (CINS), Mental Health Center Glostrup, Glostrup, Denmark
- 5Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
- 6Medical University Innsbruck, Department of Psychiatry, Psychotherapy, Psychosomatics and Medical Psychology, Division of Psychiatry I, Innsbruck, Austria
- 7Department of Psychiatry, Charles University, Faculty of Medicine and University Hospital Hradec Králové, Hradec Králové, Czechia
- 8NORMENT Centre, Institute of Clinical Psychiatry, University of Oslo and Oslo University Hospital, Oslo, Norway
- 9Department of Adult Psychiatry, Poznan University of Medical Sciences, Poznan, Poland
- 10Department of Psychiatry and Psychotherapy, Medical University of Vienna, Vienna, Austria
Introduction: In this study we assessed the contribution of psychopathology, including the two domains of negative symptoms (motivational deficit and expressive deficit), processing speed as an index of neurocognition, and emotion recognition, as an index of social cognition, to poor functional outcomes in people with schizophrenia.
Methods: The Positive and Negative Syndrome Scale was used to evaluate positive symptoms and disorganization and the Brief Negative Symptom Scale to assess negative symptoms. The Symbol Coding and the Trail Making Test A and B were used to rate processing speed and the Facial Emotion Identification Test to assess emotion recognition. Functional outcome was assessed with the Personal and Social Performance Scale (PSP). Regression analyses were performed to identify predictors of functional outcome. Mediation analyses was used to investigate whether social cognition and negative symptom domains fully or partially mediated the impact of processing speed on functional outcome.
Results: One hundred and fifty subjects from 8 different European centers were recruited. Our data showed that the expressive deficit predicted global functioning and together with motivational deficit fully mediated the effects of neurocognition on it. Motivational deficit was a predictor of personal and social functioning and fully mediated neurocognitive impairment effects on the same outcome. Both motivational deficit and neurocognitive impairment predicted socially useful activities, and the emotion recognition domain of social cognition partially mediated the impact of neurocognitive deficits on this outcome.
Conclusions: Our results indicate that pathways to functional outcomes are specific for different domains of real-life functioning and that negative symptoms and social cognition mediate the impact of neurocognitive deficits on different domains of functioning. Our results suggest that both negative symptoms and social cognition should be targeted by psychosocial interventions to enhance the functional impact of neurocognitive remediation.
1 Introduction
Schizophrenia is a severe and heterogenous mental disorder (1–3), that has profound effects on the functional outcomes of those living with the disorder (4–13). Major areas of functioning are impaired in subjects with schizophrenia, such as social, vocational, independent living, self-care, interpersonal relationships, everyday life skills and work abilities (4–6, 14–18). Functional outcome in schizophrenia does not depend only on clinical symptoms, but also on several other variables; some of these are related to patient’s personal resources, some others to the environment in which the patient lives and some to the disease (4–6, 15–17, 19, 20). Among personal resources, coping strategies, recovery style, physical status and resilience, were found to affect real-life functioning (21–24); additionally, environmental factors, including poor economic status, support services, and neighborhoods conditions, have been associated with poor functional outcome (17, 25).
In the present article we will focus on disease-related aspects, in particular on neurocognition, social cognition and negative symptoms, since they represent the major predictors of a poor functional outcome (17, 26, 27). However, to date, the recognition, assessment and management of these factors have often been inadequate, and there are limited treatment options for their management (26–35). Moreover, the complex relationships among these predictors and functioning are still poorly investigated. Understanding pathways to real-life functioning of patients with schizophrenia is essential to design new integrated and personalized treatment plans and to improve patient’s quality of life (29, 30).
Neurocognition has been found to be directly or indirectly (through the impact of other variables) associated to two important domains of functioning, i.e., work skills and everyday life skills (4, 5, 9). It is important to emphasize that neurocognition in schizophrenia is characterized by impairments in different cognitive domains such as attention, memory, verbal learning, visual learning, problem solving and processing speed (27, 36). Among these domains, processing speed has been found to be present in most patients. Indeed, in two meta-analyses its effect size was estimated to be between -1.3 and 1.5 (37, 38). Furthermore, impairment in processing speed was not only associated with poor functional outcome at baseline, but also predicted a poor prognosis longitudinally (27, 37, 39–43). Negative symptoms and social cognition seem to be the most important variables that may serve as mediators of the relationship between neurocognition and functional outcome (4–6, 9, 15, 17, 42, 44–49).
Social cognition is another important factor strongly related to the impairment of functioning in people with schizophrenia (4–6, 9, 27, 50–54). This factor represents a multidimensional and complex construct including four domains (55): emotion recognition, social perception, theory of mind (ToM), and attributional bias (4, 27). Impaired emotion recognition is found in all phases of the disease, even in subjects at risk to develop a psychosis and in those with a first-episode psychosis (56–58) and predicts poor real-life functioning, including both community and social functioning (59–61).
According to some studies, social cognition is even more strongly associated to functional outcome than neurocognition; it is associated to work skills and interpersonal relationships directly (4, 9) and with everyday life skills through functional capacity (5, 62). According to other studies, it acts as a mediator between the latter and functional outcome (4–6, 15, 45–47, 59, 63–67), and between specific neurocognitive domains, such as processing speed (65), sustained attention (65) and verbal memory (64) and functional outcome. Social perception has been reported as a mediator between early visual processing and functional outcome (66), ToM as mediator between neurocognition and social competence that, in turn, showed a direct link with self-reported functioning (63), while emotion recognition was found to be a mediator between neurocognition and social functioning in people with schizophrenia and first episode psychoses (68).
Negative symptoms have a direct and indirect impact on patient’s real-life functioning (4–6, 15, 69), and seem to mediate the effect of neurocognition on functioning (42, 47–49, 70). Negative symptoms are heterogeneous and can be categorized into two different domains, motivational deficit and expressive deficit, showing different relationships with functional impairment and possibly subtended by different pathophysiological mechanisms (26, 55, 71, 72). Motivational deficit domain was found to influence the area of interpersonal relationships, both directly and indirectly (mediated by variables such as internalized stigma, resilience and engagement with services), while expressive deficit domain was found to be indirectly and weakly related to real-life functioning by some studies (4). In a network analysis, motivational deficit domain was associated with interpersonal relationships and work skills, and expressive deficit with everyday life skills (5, 6, 73). Furthermore, only baseline motivational deficit domain predicted interpersonal functioning at four-year follow-up, while expressive deficit domain did not predict functioning (9).
Furthermore, as mentioned above, negative symptoms seem to mediate the effect of neurocognition on real-life functioning, at least in part (48). In more recent papers, these symptoms, together with general psychopathology and insight, were associated to cognition and functioning and acted as mediators in the relationship between both cognition and functioning (49, 74, 75), even in individuals at ultrahigh risk for psychosis (76). A 20-year longitudinal study found that negative symptoms had an indirect impact on work functioning through neurocognition (in particular processing speed and general knowledge) (42). The same study in the cross-sectional analysis at baseline found that negative symptoms mediated the impact of neurocognition on functioning (42).
In summary, the evidence accumulated emphasizes the central role of neurocognition, negative symptoms, and social cognition as primary determinants of functional outcome in individuals with schizophrenia. Notably, as explained above, both negative symptoms and deficits in social cognition seem to mediate the relationships between neurocognition and functioning in patients with schizophrenia and even in the early stages of the disease (42, 47, 48, 64–67).
However, most of the studies did not investigate multiple domains of functioning and the two domains of negative symptoms. In fact, some studies investigated only global functioning or work skills, which might be influenced differently by cognitive impairment and negative symptoms with respect to interpersonal and social functioning, or everyday life skills. Negative symptoms were mostly assessed using first-generation scales and particularly the PANSS which provides an inadequate assessment of negative symptoms and particularly of motivational deficit domain (26).
Within this frame, the present study aimed to evaluate the contribution of psychopathology, including the two domains of negative symptoms, as well as of processing speed (as an index of neurocognition), and emotion recognition (as an index of social cognition), to poor functional outcome in people with schizophrenia. In particular, the specific aims of the paper were to examine: 1) the contribution of psychopathology, processing speed and emotion recognition to poor functional outcome; 2) the possible role of negative symptom domains and emotion recognition as mediators in the relationship between processing speed and specific domains of functional outcome. This study was carried out within the main project “European College of Neuropsychopharmacology (ECNP) Network on Schizophrenia Study on the Assessment of Negative Symptoms” (ENSANeS).
2 Methods
In this cross-sectional study, participants were recruited from the outpatient and inpatient units of the psychiatric departments of 8 of the 12 European centers involved in the main project (see Table 1 for the list of centers and the number of patients recruited in each center). Recruitment took place from 31 October 2016 to 15 July 2017. Inclusion criteria were a diagnosis of schizophrenia according to DSM-IV, confirmed by the MINI Neuropsychiatric Interview-Plus (MINI-Plus), and an age between 18 and 65 years. Exclusion criteria were: (a) change in treatment and/or hospitalization due to exacerbation of symptoms in the previous three months; (b) a history of moderate to severe intellectual disability or neurological disease; (c) a history of alcohol and/or substance abuse in the previous six months; (d) current pregnancy, and (e) inability to provide informed consent. The study was conducted according to the ethical standard established in the 1964 Helsinki Declaration. The local ethics committee of each of the participating centers approved the study. All participants signed a written informed consent to participate in the study.
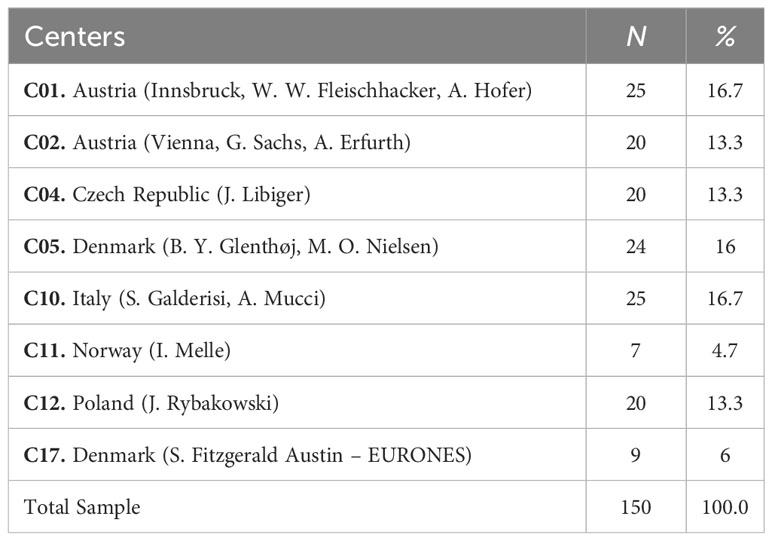
Table 1 Centers involved in the study (N and % of subjects recruited).
2.1 Assessment
2.1.1 Psychopathology
The Positive and Negative Syndrome Scale (PANSS) is clinician-rated scale, which assesses positive symptoms, negative symptoms, and general psychopathology (77); each item is rated on a seven-point Likert scale. Higher scores indicate greater severity. In the present study, the positive dimension was calculated according to Wallwork and colleagues (78) by summing the scores on the items “delusions” (P1), “hallucinatory behavior” (P3), “grandiosity” (P5), and “unusual thought” (G9); the disorganization dimension was represented by the PANSS item “conceptual disorganization” (P2), to avoid overlap with cognitive functioning as the PANSS disorganization factor includes impairment in abstract thinking and poor attention.
Negative symptoms were assessed using the Brief Negative Symptom Scale (BNSS) (79). The BNSS is a scale developed according to the current conceptualization of negative symptoms, in accordance with the NIMH-MATRICS Consensus Statement on Negative Symptoms. It assesses all domains of the negative psychopathological dimension: blunted affect, alogia, anhedonia, avolition and asociality, as well as an additional aspect, “distress”, which evaluates the absence of the normal experience of distressing and unpleasant emotions (80). The BNSS consists of 13 items organized into six subscales: anhedonia (three items), distress (one item), asociality (two items), avolition (two items), blunted affect (three items) and alogia (two items). The scale provides a total score (sum of the scores on the 13 items) and six subscale scores (sum of the scores on the items in each subscale). For all items higher scores are associated with greater impairment/presence of symptoms. In the present study, the total negative symptom score was calculated by subtracting the “distress” subscale from the total score (81). The motivational deficit domain of negative symptoms was obtained by summing the scores of the anhedonia, asociality and avolition subscales; the expressive deficit domain was obtained by summing the scores of the subscales alogia and blunted affect.
2.1.2 Processing speed
We chose processing speed as an index of neurocognition. This choice stems from the well-established evidence indicating that it is among the most frequently impaired cognitive domains in individuals with schizophrenia. Processing speed deficits are consistently observed in this population and have been linked to various aspects of functional impairment, making it a relevant and representative measure of neurocognitive functioning (37, 38, 82).
Two tests from the Brief Assessment of Cognition in Schizophrenia (BACS) were used to assess processing speed (83, 84): the Symbol Coding and the Trail Making Test (TMT) A and B. The Symbol Coding is a paper and pencil test that requires the subject to write digits corresponding to meaningless symbols below each symbol, according to a key shown on the top of the page, as quickly as possible, in a maximum time of 90 seconds.
The Trail Making Test (TMT) is made up of two parts, A and B. TMT A is a time trial (300 seconds) in which the subject has to combine randomly arranged numbers on a sheet of paper in ascending order. TMT B is a time trial (300 seconds) in which the participant has to combine numbers and letters randomly arranged on a sheet of paper in ascending and alternating order (i.e.: 1-A-2-B-3-C – etc…), thus combining the numbers (from 1 to 13) and the letters (from A to N) alternately. The TMT A and B scores are based on the number of seconds taken to complete the test; the longer the time taken, the worse the performance. A composite score for “processing speed” was obtained by averaging the Z-score (obtained as the difference between the subject’s score and the sample mean divided by the sample standard deviation) on the three tests (TMT A, TMT B and Symbol Coding, for the latter test the raw scores were inverted before calculating the Z-scores, so that for each test higher Z-scores represented higher impairment).
2.1.3 Emotion recognition
The choice to focus on emotion recognition as an index of social cognition stems from the fact that its impairment appears since the early phases of schizophrenia and has been consistently associated with poor real-life functioning (59–61).
The Facial Emotion Identification Test (FEIT) has been used to assess emotion recognition (85). The FEIT consists of black and white photographs of 55 faces of different people, each showing different emotions. The stimuli were presented in a random order. Participants had to identify the emotion presented in the stimulus (happiness, sadness, anger, fear, surprise, neutral, or disgust). One point was awarded for each correct answer and 0 for incorrect answers. The total FEIT score was calculated as the number of correct responses (0–55).
2.1.4 Functional outcome
The Personal and Social Performance Scale (PSP) was used to assess functional outcome (86). The PSP is a semi-structured interview that investigates 4 areas: self-care, socially useful activities, personal and social relationships, and disturbing and aggressive behavior. Each domain is scored from 0 (no impairment) to 5 (very severe). The scores on the four subdimensions can be combined to produce a total score on a 100-point scale, with higher scores indicating better functioning. In our study we focused on the scores for PSP total, PSP socially useful activities and PSP personal and social relationships.
2.2 Statistical analyses
For all measures, the z-score was calculated as the difference between the subject’s score and the sample mean divided by the sample standard deviation.
A preliminary correlation analysis was used to verify associations of clinical and cognitive variables with the functional outcome, using Pearson’s R correlation coefficient (Supplementary Material, Supplementary Table S1). Only variables with a significant association with functional outcome were then submitted to regression and mediation analyses.
One-way ANOVAs with center as the grouping factor were performed to evaluate significant differences between patients recruited at different participating sites on the following variables: age, education, psychopathology, TMT A, TMT B, Symbol Coding and FEIT. If the center effect was significant, the center was entered in the regression analyses.
To explore potential variables with the highest impact on functioning, we conducted three separate stepwise hierarchical multivariate regression analyses. Specifically, we used the PSP total score, the PSP score for socially useful activities and the PSP scores for personal and social relationships as dependent variables, and age, gender, years of education, center if its effect was significant on the ANOVA, positive dimension, disorganization, MAP, EXP, processing speed and emotion recognition as independent variables. In particular, the first regression module included age, gender, years of education and center, while the second regression module included positive dimension, disorganization, MAP, EXP, processing speed and emotion recognition.
Mediation analyses were performed using PROCESS to determine the significance of the indirect effects (mediation) in six different models (Figure 1). For each model, the variable “processing speed” was considered as the independent variable or predictor, the two domains of negative symptoms (Motivational Deficit and Expressive Deficit) or social cognition were considered as mediator variables. The outcome variables, different for each model investigated, were 1) PSP total score, 2) PSP socially useful activities subscale and 3) PSP personal and social relationships subscale. To perform the mediation analyses, the predictor has to satisfy the assumption of a linear relationship with the outcome (Figure 1 - path c); the mediator has to demonstrate a linear relationship with both the predictor (Figure 1 - path a/a’) and the outcome (Figure 1 - path b/b’). Partial mediation occurs when, after introducing the mediator variable into the model (negative symptom domains in Figure 1A; emotion recognition in Figure 1B), the direct effect (Figure 1 - path c’) is reduced compared to the total direct effect (Figure 1 - path c) but is still significant. Complete mediation occurs when the direct effect (Figure 1 - path c’) is no more significant after introducing the mediator variable.
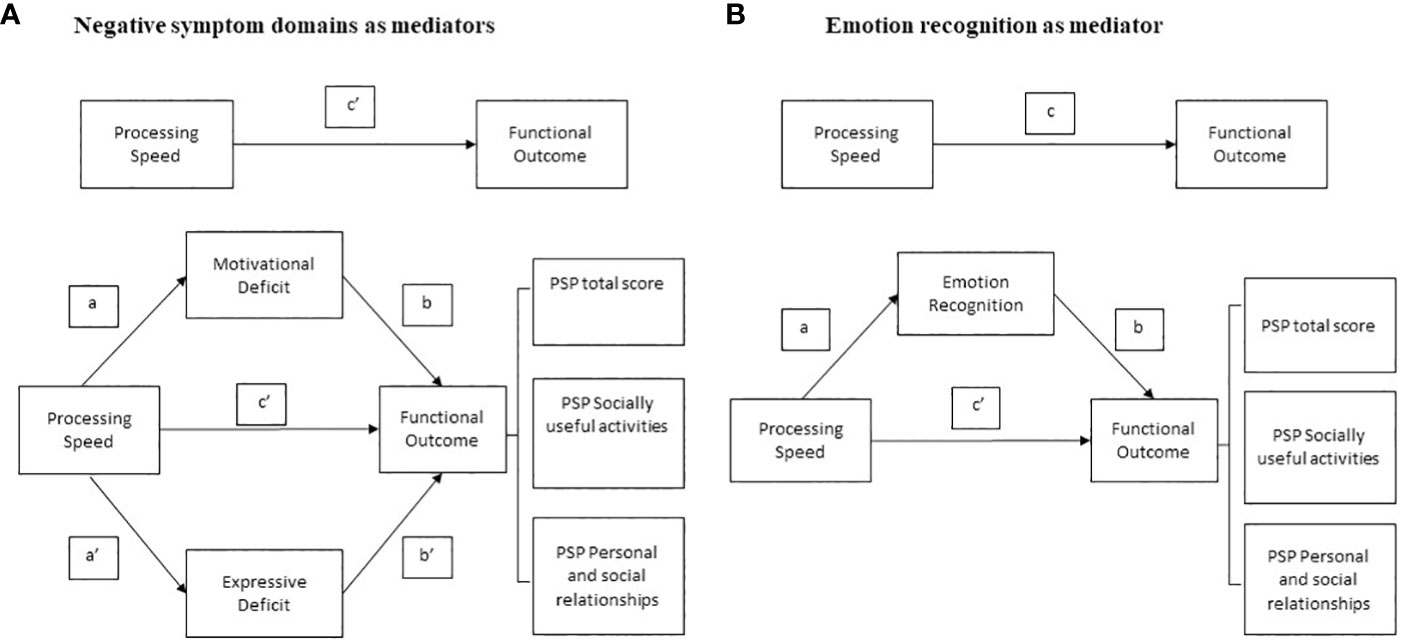
Figure 1 Basic model of mediation analyses with (A) negative symptom domains and (B) social cognition domain of emotion recognition as mediators between neurocognition and measures of functional outcome.
In our conceptual models (Figure 1), the effect of processing speed on functioning is referred to as the total effect (path c). In the three mediation analyses that considered negative symptom domains (Motivational Deficit and Expressive Deficit) as mediators (Figure 1A), the total effects included a direct effect of processing speed on functional outcome (path c’) and an indirect effect of processing speed on functioning through the two negative symptom domains (mediation paths: a/b, a’/b’). In the other three mediation analyses, in which social cognition was considered as a mediator (Figure 1B), the overall effects included a direct effect from processing speed to functional outcome (path c’) and an overall indirect effect from processing speed to functioning via social cognition (mediation path: a/b). The mediation analyses are considered valid when the significant level is maintained with 5000 bootstrapping samples and the 95% confidence interval of the indirect effect does not include zero.
All statistical analyses were performed using SPSS software version 25.
3 Results
3.1 Subjects
One hundred fifty subjects from 8 different European centers were recruited to the study. Table 2 shows the demographic and clinical characteristics of the sample. The experimental sample consists predominantly of Caucasian (94%) and male (58%) subjects, with a mean age of 38.4 years, a mean duration of education of 13 years, and a mean duration of illness of 13 years.
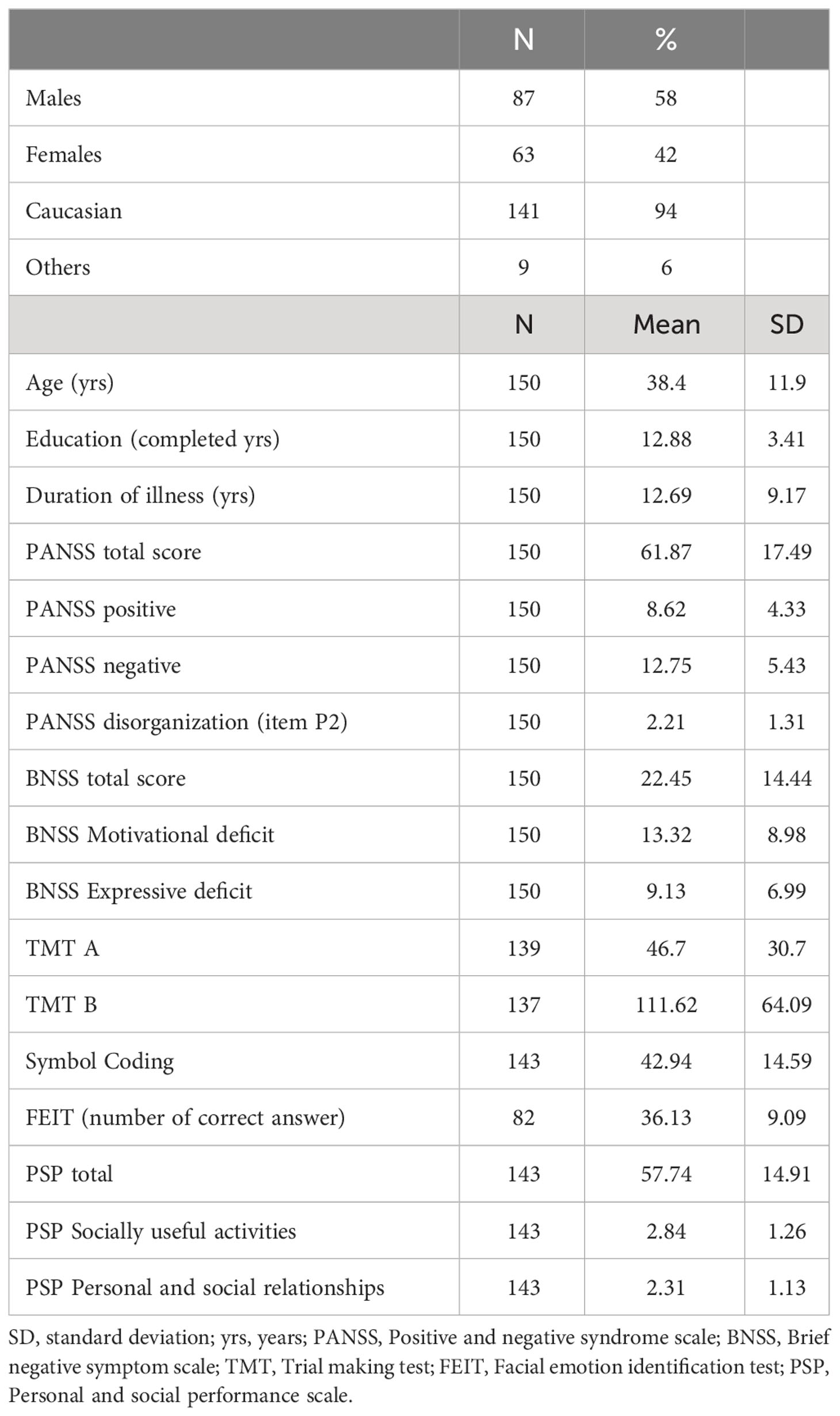
Table 2 Demographic and clinical characteristics of the study sample.
3.2 Regression analyses
The Center was entered in all regression analyses, as the ANOVAs showed a significant effect of the Center on age, psychopathology, functioning and symbol coding performance (Table 3).
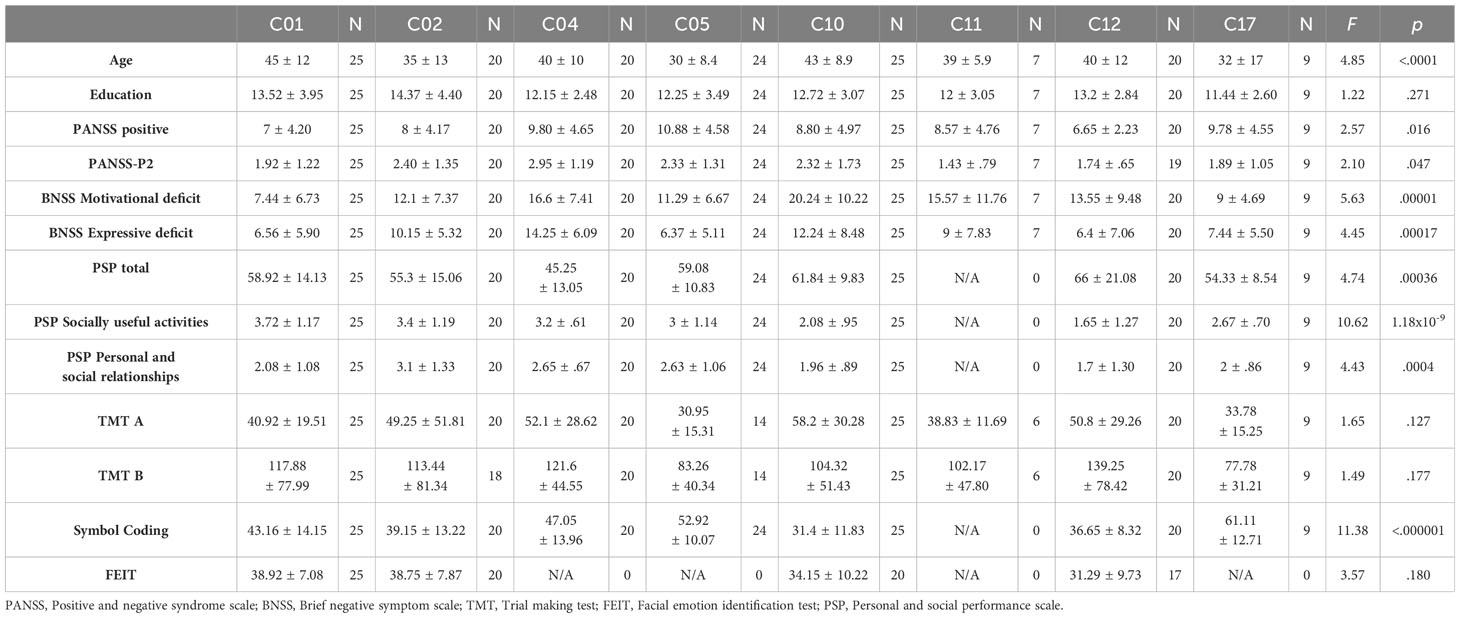
Table 3 Center-effect for age, education, psychopathological and cognitive variables.
The regression analyses demonstrated that the PSP total score was predicted by the expressive deficit domain of negative symptoms (β=-.430, p=1.3x10-5), and by the PANSS positive dimension (β=-.342, p=.001); the PSP socially useful activities score was predicted by the center (β=-.179, p=2.38x10-14), by processing speed (β=-.397, p=1.2x10-4) and by the motivational deficit (β=.270, p=.003), and the PSP personal and social relationships score was predicted by the gender (β=-.441, p=.028), by the center (β=-.109, p=2x10-6) and by the motivational deficit (β=.552, p=2.6x10-7) of negative symptoms (Table 4).
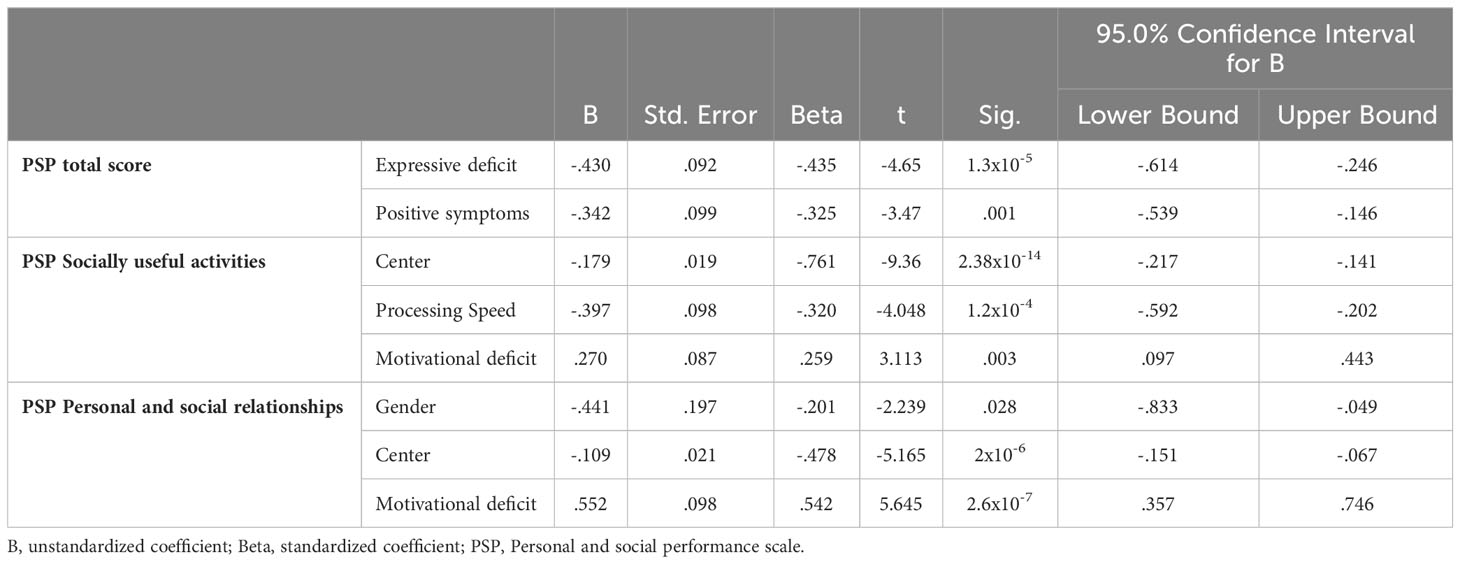
Table 4 Regression analyses to investigate factors that predict functional outcome.
3.3 Mediation analysis
The following mediation analyses illustrate the role of negative symptoms or social cognition in mediating the effects of neurocognition on functioning.
3.3.1 Negative symptoms as mediators between neurocognition and functional outcome
As reported in Table 5, the prerequisites of mediation analysis were not satisfied for the mediation role of negative symptom domains on PSP Socially useful activities.
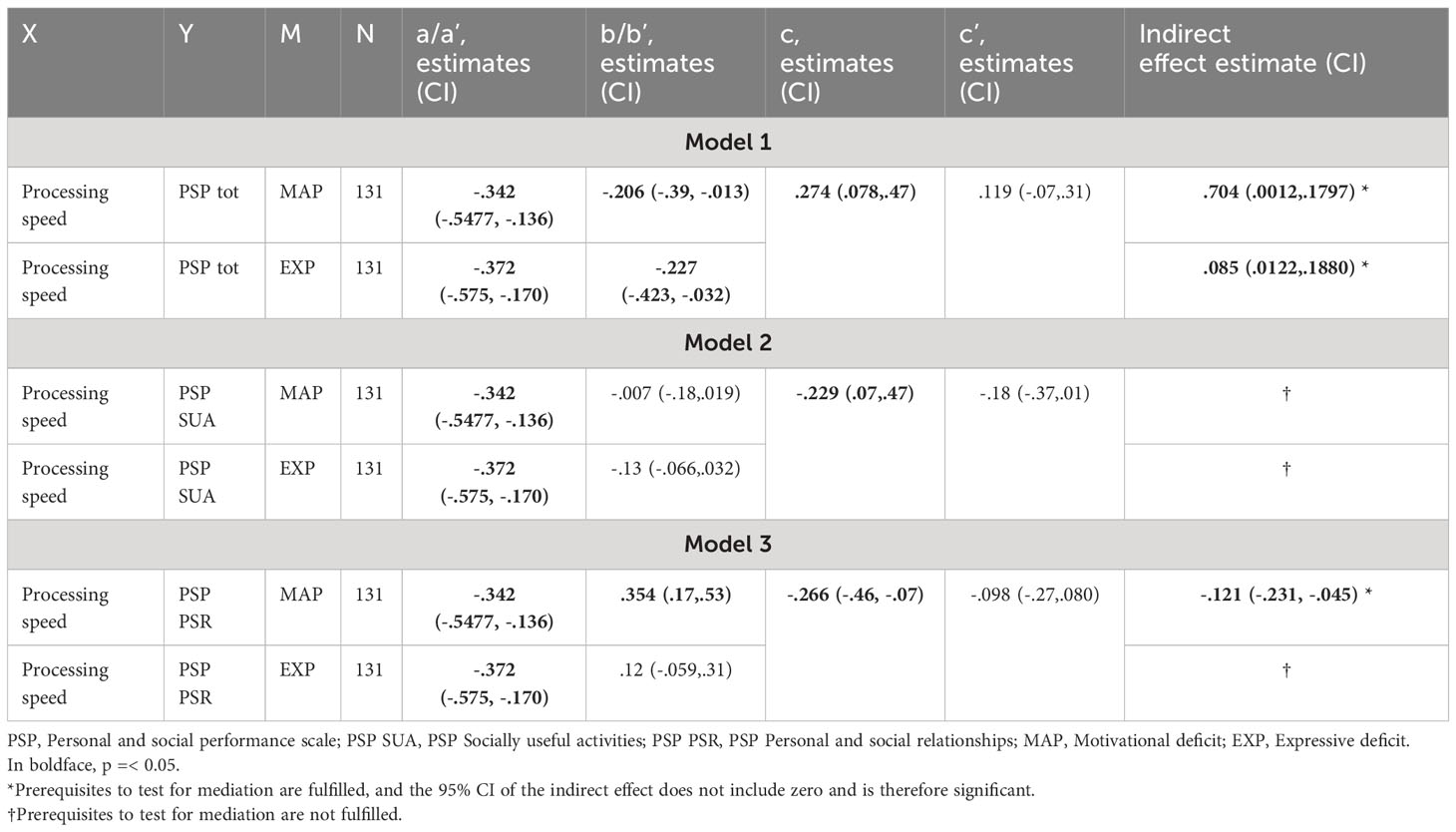
Table 5 Statistics from the mediation analyses with negative symptom domains as mediators between neurocognition and functional outcome.
3.3.1.1 Mediation analysis on PSP total score
The results showed that the simple path coefficients (path a, b, a’, b’ and c’) were statistically significant at p<0.05 (Table 5; Figure 2A). The total effect of processing speed on PSP total score was.274 (p=.006), while the direct effect on the same score was no more significant, indicating a complete mediation of the effects by both negative symptom domains.
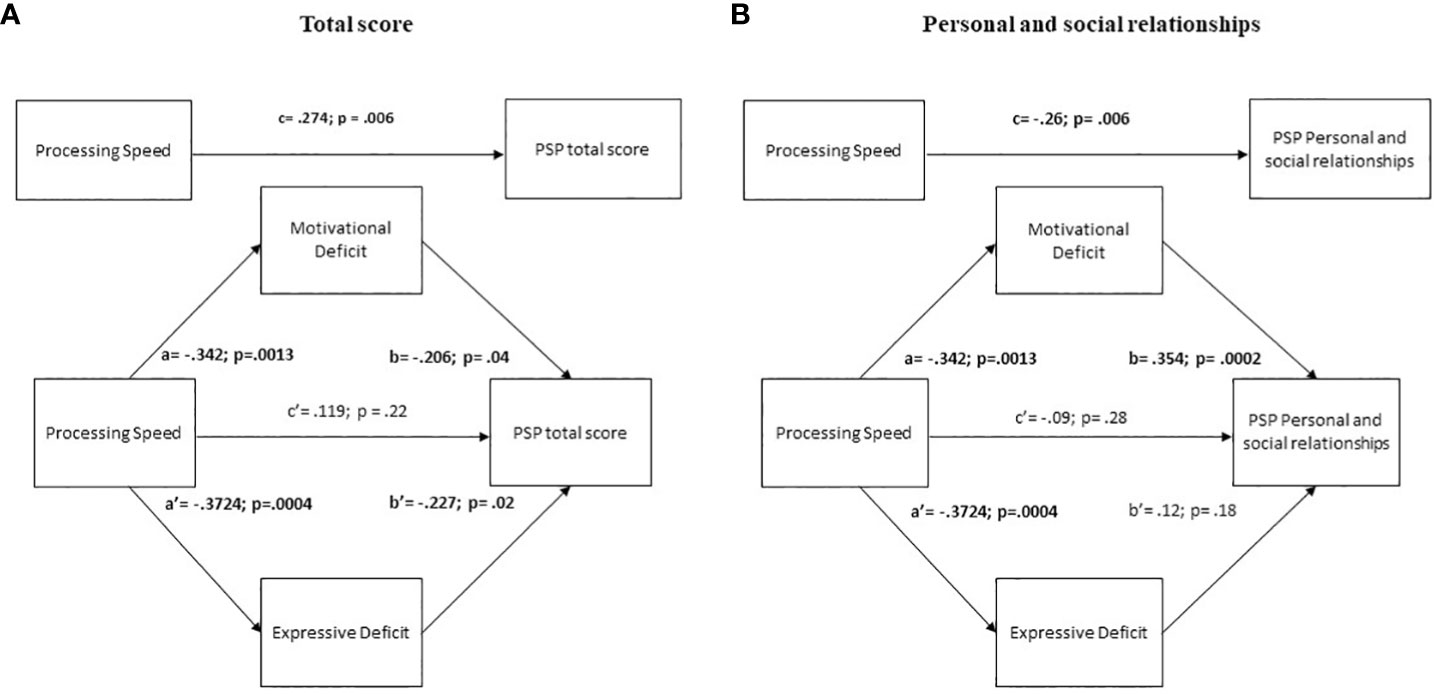
Figure 2 Mediation analyses with negative symptoms as mediator between neurocognition and the Personal and social performance scale (PSP) total score and Personal and social relationships. The negative symptom domains were both full mediators of the impact of Processing speed on PSP total score (A) while the motivational deficit domain was a full mediator of the impact of Processing speed on PSP Personal and social relationships (B).
3.3.1.2 Mediation analysis on PSP Personal and social relationships
The results showed that the simple path coefficients (path a, b and a’) were statistically significant (Table 5; Figure 2B). The total effect of processing speed on PSP Personal and social relationships was significant, while the direct effect was not indicating a full mediation effect through the motivational deficit domain of the negative symptoms.
3.3.2 Social cognition as mediator between neurocognition and functional outcome
The results showed that the prerequisites were not satisfied for the mediation role of social cognition on PSP Personal and social relationships (Table 6).
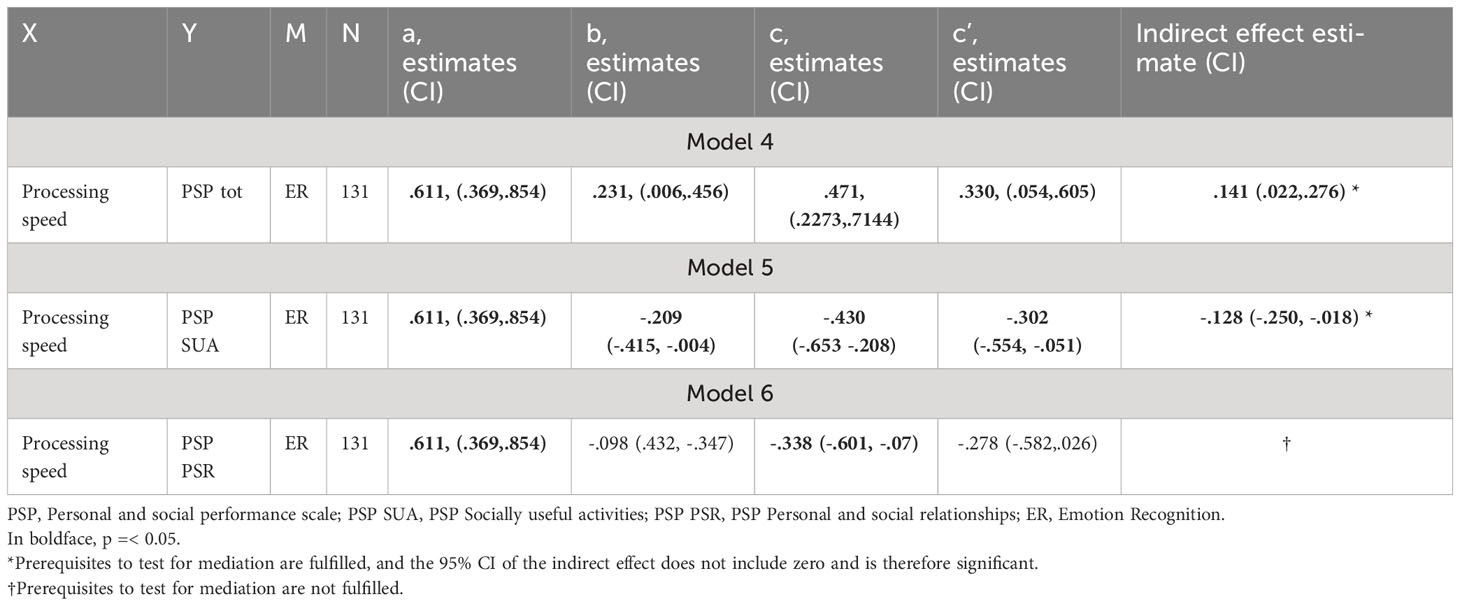
Table 6 Statistics from the mediation analyses with social cognition as mediator between neurocognition and functional outcome.
3.3.2.1 Mediation analysis on PSP total score
The results showed that the simple path coefficients (path a, b, c and c1) were statistically significant (Table 6; Figure 3A). The total effect of processing speed on PSP total score was significant and moderate, while the direct effect was reduced though still significant. These results indicate a partial mediation effect of emotion recognition.
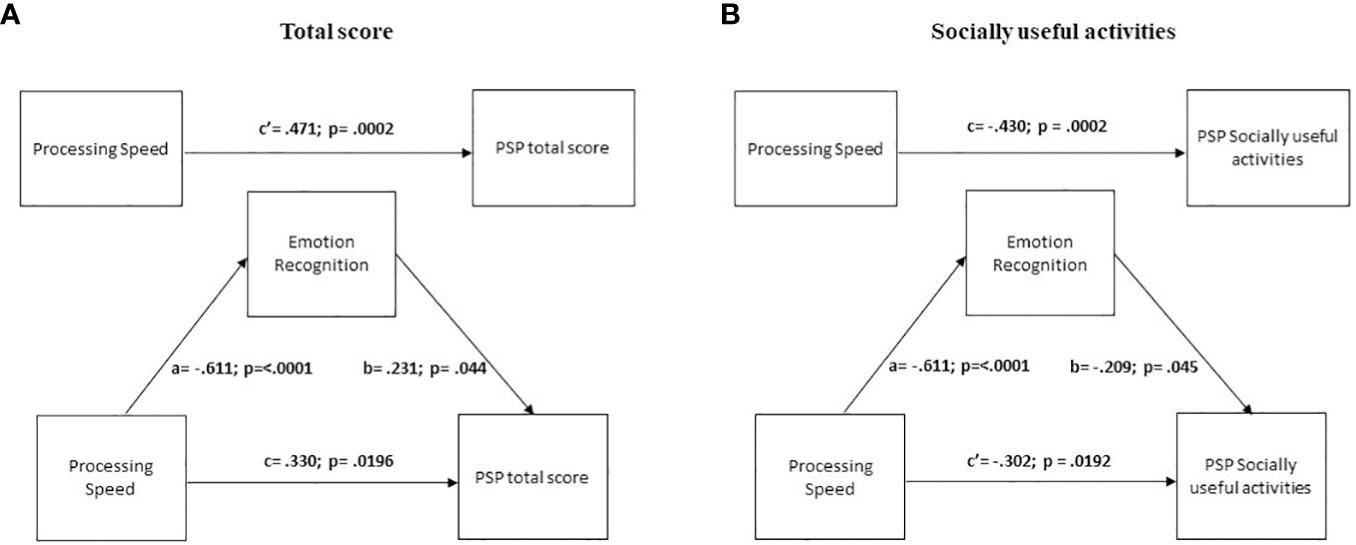
Figure 3 Mediation analyses with emotion recognition as mediator between neurocognition and the Personal and social performance scale (PSP) total score and Socially useful activities. The social cognition domain of emotion recognition partially mediates the impact of Processing speed on PSP total score (A) and of Processing speed on PSP Socially useful activities (B).
3.3.2.2 Mediation analysis on PSP Socially useful activities
The results showed that the simple path coefficients (path a, b, c and c1) were statistically significant (Table 6; Figure 3B). The total effect of processing speed on PSP Socially useful activities was significant, and the direct effect was significant but reduced, again indicating a partial mediation effect of emotion recognition.
3.4 Control analyses
To rule out the possible confounding effects of positive symptoms on negative symptoms we conducted control analyses. Methods and results of these analyses are described within the Supplementary Material, Supplementary Table S1.
4 Discussion
Our data showed that positive symptoms and the expressive deficit domain of negative symptoms predicted global functioning. Furthermore, both negative symptom domains, the expressive deficit and the motivational deficit domain, fully mediated the effects of neurocognition on global functioning. The motivational deficit domain of negative symptoms was also a predictor of personal and social functioning and fully mediated neurocognitive impairment effects on the same outcome. Both motivational deficit and neurocognitive impairment predicted socially useful activities, which include work and everyday life skills, and the emotion recognition domain of social cognition partially mediated the impact of neurocognitive deficits on this outcome.
Our results are broadly consistent with previous literature showing a relationship between psychopathology, neurocognition and social cognition with functional outcome (4–6, 9, 15, 49, 63, 65, 67, 73, 76, 87–89). In particular, as regard to positive symptoms, even when they are of subclinical severity (mild severity in our sample), might contribute to global functioning. This is in line with previous literature findings (87–89). However, the global functioning, as evaluated by the PSP total score, includes psychopathological aspects and might thus explain why the positive symptoms are associated to this outcome measure but not to specific domains of real-life functioning which do not include any psychopathological aspect.
Among disease-related variables, as widely reported in the literature, cognitive deficits and negative symptoms seem to represent the major predictors of poor functional outcome (26–33).
The pathways to functional outcome are very complex especially when considering the large heterogeneity of negative symptoms, cognitive impairment and also functioning itself, which includes deficits in multiple domains (16, 26, 27, 90). Our results indicate the prominent impact of neurocognition on everyday life and work skills both directly and indirectly (trough social cognition) (6, 9) and the prominent role of the motivational deficit domain of negative symptoms on the interpersonal functioning domain (6, 9, 73).
Our study was designed to better understand the pathways from processing speed to functional outcome in individuals affected by schizophrenia (27, 37, 39–43).
Consistent with previous models (42, 48, 49, 91, 92), we found that both negative symptom domains mediated the relationship between processing speed and global functioning as assessed by the total score on PSP. It is worth noticing that the total PSP score includes both symptom severity and functional disability, probably explaining the predominant role of psychopathology, in particular negative symptoms, demonstrated by the regression and mediation analysis results of our study. When the PSP domains were considered, we found that the motivational deficit domain mediated the relationship between processing speed and PSP personal and social relationships. This finding is consistent with the evidence that the motivational deficit is associated with a greater impairment in functioning compared to the expressive deficit domain, particularly in the domain of interpersonal relationships (4, 6, 9, 19). Therefore, the use of different assessment tools, both for functioning and negative symptoms, could explain the heterogeneity in the findings reported by the literature.
Our results have clinical implications as the presence of negative symptoms, especially motivational negative symptoms might limit the transfer to the interpersonal functioning of cognitive remediation (16). The prevention and treatment of negative symptoms is thus mandatory and any effort should be made to control for the severity of factors that could induce negative symptoms, such as positive symptoms, extrapyramidal side effects or depression, which are the main sources of secondary negative symptoms (28). It is important to note that, in our study, the significant contribution of positive symptoms to global functioning raises the question whether negative symptoms in our sample were partly secondary to the positive symptoms. However, the sample was characterized by low levels of positive symptoms (absent to mild severity) and, in addition, correlation analyses between positive symptoms and the two negative symptom domains did not reach the statistical significance, thus excluding the possibility that the negative symptoms in our sample were secondary to the positive ones.
Regarding social cognition, we observed that it mediated the pathway from neurocognition to PSP Socially useful activities, suggesting that deficits in social cognition are influenced by processing speed (37), and interfere with real-life functioning in people with schizophrenia. These findings are consistent with a growing literature (93–96) in individuals with early psychosis (97) and with chronic schizophrenia (65, 98, 99). Other studies reported partially concordant results but found a relationship between social cognition and other neurocognitive domains, e.g., working memory, episodic memory, attention, problem solving, and executive functioning (97, 100–102). A possible interpretation of our results comes from the evidence that slower processing speed leads to greater cognitive effort in processing information, which could lead to deterioration in social cognitive skills. For example, due to a slower processing speed, and thus to a greater cognitive effort, a patient could experience communication conflicts due to errors in interpretation, resulting in difficulty recognizing the mental states of others and a loss of motivation. As a result, individuals with schizophrenia may have more negative experiences of social interactions, which can lead to feelings of low self-efficacy, greater problems with social skills and eventually increased social isolation (65).
This evidence could have some implications for clinical practice. For instance, the relationships found in the present study between social abilities and functioning highlights the importance to target also social cognition and not only neurocognition within functional recovery programs. In fact, meta-analyses have shown that social cognition can be successfully targeted by specific social cognitive remediation interventions (103, 104).
Furthermore, as indicated by the regression and mediation analyses, we did not find an association between social cognition and personal and social relationships, a finding that has been reported in previous studies on this topic (19, 27, 105). The absence of this relationship in the present study could be due to the relatively small proportion of subjects (82 out of 150) that participated in the social cognition assessment. In addition, the inconsistency between the results of our study and those of previous studies could be mainly due to two factors: i) most previous studies considered an overall score for social cognition and did not focus on a single domain of social cognition, whereas in the present study we focused on the domain of emotion recognition assessed by the FEIT; ii) the use of different assessment tools not only for social cognition but also for patients’ functioning.
Our results should be also interpreted in the light of some strengths and limitations.
First, few studies have attempted to investigate the possible role of negative symptom domains and emotion recognition as mediators in the relationship between processing speed and functional outcome using state of the art assessment instruments. Indeed, negative symptoms have been assessed using the BNSS, a second-generation scale that evaluates negative symptoms according to their current conceptualization (26). In addition, neurocognition was assessed with tests from the BACS, one of the brief instruments (27, 84, 106) recommended in the guidance paper on the assessment of cognitive deficits in patients with schizophrenia, issued by the European Psychiatric Association (27).
In terms of limitations, the sample size was relatively small, which limits the possibility of generalizing the results. In addition, there is also a very large effect of recruitment center, demonstrated by the results of one-way ANOVAs on key variables using the center as the grouping factor. Therefore, in the light of this effect, we kept the center as an explanatory variable in the regression models: if the center effect was found to be significant, we included “center” as a predictor in the regression models. Studies with larger samples and with a careful reduction of the recruitment center effect are needed to provide a further validation of these results. Another limitation of the present study may be related to the effects of pharmacological treatments that the patients underwent. However, as some meta-analyses on this topic have shown, psychotropic drugs do not seem to have a negative impact on processing speed (107) or on emotion recognition (108). Our study was a naturalistic unfunded study which demonstrated that using only a few indices of social cognition and neurocognitive functioning it is possible to better characterize in routine clinical settings patients with schizophrenia to personalize treatments (8).
The study of variables that may mediate and explain the relationship between cognition and functioning in people with schizophrenia is of great clinical and scientific importance. Our study focused on disease-related aspects, and in particular on cognition and negative symptoms, as they were found to be the key predictors of work, interpersonal and everyday life skills (6, 9). However, the significance of exploring non-disease-related factors as potential mediators between neurocognition and functional outcome should be further investigated. The intricate interplay between these variables merits further investigation to enhance our understanding of the multifaceted determinants of functional outcomes in schizophrenia. The development of early intervention programmes for psychosis could benefit from the identification of factors and pathways that influence functioning. It should be emphasized that combining approaches targeting neurocognition and social cognition with those targeting psychopathology offer synergistic benefits and may be essential for achieving long-term improvements in patient’ functioning (109–113).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethical Committee from the 8 countries. The patients/participants provided their written informed consent to participate in this study. The studies were conducted in accordance with the local legislation and institutional requirements.
Author contributions
GG: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Methodology. PP: Writing – original draft, Writing – review & editing, Data curation, Methodology. AM: Supervision, Writing – original draft, Writing – review & editing, Conceptualization, Methodology. SA: Writing – review & editing. AE: Writing – review & editing. BG: Writing – review & editing. AH: Writing – review & editing. JH: Writing – review & editing. JL: Writing – review & editing. IM: Writing – review & editing. MN: Writing – review & editing. JR: Writing – review & editing. PW: Writing – review & editing. SG: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. GS: Conceptualization, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The European College of Neuropsychopharmacology (ECNP) supported the network standalone meetings during which the protocol was designed and results discussed by the involved researchers.
Acknowledgments
This study was carried out within the European College of Neuropsychopharmacology (ECNP) Network on Schizophrenia Study on the Assessment of Negative Symptoms (ENSANeS). The following researchers collaborated to the study: Klaudia Domowicz, Department of Adult Psychiatry, Poznan University of Medical Sciences, Poznan, Poland; Ann Faerden, NORMENT Centre, Institute of Clinical Psychiatry, University of Oslo and Oslo University Hospital, Oslo, Norway; Johannes Gehr, Center for Neuropsychiatric Schizophrenia Research (CNSR) and Center for Clinical Intervention and Neuropsychiatric Schizophrenia Research (CINS), Mental Health Center Glostrup, Glostrup, Denmark; University of Copenhagen, Faculty of Health and Medical Sciences, Department of Clinical Medicine, Copenhagen, Denmark; Jens Lysgaard Jørgensen, Clinical Nurse Man- ager, Psychiatric Center Køge, Psychiatry Region Zealand, Denmark; Ilja Kunz, Medical University Innsbruck, Department of Psychiatry, Psychotherapy and Psychosomatics, Division of Psychiatry I, Innsbruck, Austria; Siv Hege Lyngstad, NORMENT Centre, Institute of Clinical Psychiatry, University of Oslo and Oslo University Hospital, Oslo, Norway; Eva Maihofer, 6th Psychiatric Department, Otto-Wagner-Spital, Vienna, Austria; Francesco Brando, University of Campania Luigi Vanvitelli, Naples, Italy; Luigi Giuliani, University of Campania Luigi Vanvitelli, Naples, Italy; Patricia Rößler, Department of Psychiatry and Psychotherapy, Medical University of Vienna, Vienna, Austria; Erik Simonsen, Psychiatric Research Unit, Psychiatry Region Zealand, Denmark, Institute of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
Conflict of interest
GG has been a consultant for Angelini. AM has been a consultant and/or advisor to or has received honoraria from Angelini, Gedeon. Richter Bulgaria, Janssen Pharmaceuticals, Lundbeck, Otsuka Pharmaceutical, Pfizer, Pierre Fabre, Rovi. Pharma and Boehringer Ingelheim. AE received consulting fees and/or honoraria for speeches within the last 3 years from Angelini, AOP Orphan, Germania, Janssen, Krka, Lundbeck, Mylan, Neuraxpharm, Recordati, and Sandoz. BG has been the leader of a Lundbeck Foundation Centre of Excellence for Clinical Intervention and Neuropsychiatric Schizophrenia Research CINS January 2009 – December 2021, which was partially financed by an independent grant from the Lundbeck Foundation based on international review and partially financed by the Mental Health Services in the Capital Region of Denmark, the University of Copenhagen, and other foundations. All grants are the property of the Mental Health Services in the Capital Region of Denmark and administrated by them. She has no other conflicts to disclose. AH has been a consultant for Recordati and Boehringer Ingelheim and Newron Pharmaceuticals and participated in educational conferences for Janssen and Lundbeck. JH received consulting fees and/or honoraria for speeches within the last 3 years from Angelini, Lundbeck, Janssen and Servier. SG has been a consultant and/or advisor to or has received honoraria from Angelini, Boehringer Ingelheim, Gedeon Richter-Recordati, Innova Pharma-Recordati Group, Janssen, Lundbeck, Otsuka, Recordati Pharmaceuticals, Rovi Pharma and Sunovion Pharmaceuticals. GS is president of the Austrian Society of Neuropsychopharmacology and Biological Psychiatry, which is partially financed by the support from pharmaceutical companies. GS received consulting fees and/or honoraria for speeches within the last 3 years from Janssen, Lundbeck, Mylan, Recordati, and Schwabe.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer CM declared a past co-authorship with the authors AM and SG to the handling editor.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1333711/full#supplementary-material
References
1. GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet (London England) (2017) 390(10100):1211–59. doi: 10.1016/S0140-6736(17)32154-2
2. Correll CU, Solmi M, Croatto G, Schneider LK, Rohani-Montez SC, Fairley L, et al. Mortality in people with schizophrenia: a systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry (2022) 21(2):248–71. doi: 10.1002/wps.20994
3. Sass L. Subjectivity, psychosis and the science of psychiatry. World Psychiatry (2022) 21(2):165–6. doi: 10.1002/wps.20986
4. Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, et al. The influence of illness-related variables, personal resources and context-related factors on real-life functioning of people with schizophrenia. World Psychiatry (2014) 13(3):275–87. doi: 10.1002/wps.20167
5. Galderisi S, Rucci P, Kirkpatrick B, Mucci A, Gibertoni D, Rocca P, et al. Interplay among psychopathologic variables, personal resources, context-related factors, and real-life functioning in individuals with schizophrenia: A network analysis. JAMA Psychiatry (2018) 75(4):396–404. doi: 10.1001/jamapsychiatry.2017.4607
6. Galderisi S, Rucci P, Mucci A, Rossi A, Rocca P, Bertolino A, et al. The interplay among psychopathology, personal resources, context-related factors and real-life functioning in schizophrenia: stability in relationships after 4 years and differences in network structure between recovered and non-recovered patients. World Psychiatry (2020) 19(1):81–91. doi: 10.1002/wps.20700
7. Rapoport JL, Giedd JN, Gogtay N. Neurodevelopmental model of schizophrenia: update 2012. Mol Psychiatry (2012) 17(12):1228–38. doi: 10.1038/mp.2012.23
8. Maj M, van Os J, De Hert M, Gaebel W, Galderisi S, Green MF, et al. The clinical characterization of the patient with primary psychosis aimed at personalization of management. World Psychiatry (2021) 20(1):4–33. doi: 10.1002/wps.20809
9. Mucci A, Galderisi S, Gibertoni D, Rossi A, Rocca P, Bertolino A, et al. Factors associated with real-life functioning in persons with schizophrenia in a 4-year follow-up study of the italian network for research on psychoses. JAMA Psychiatry (2021) 78(5):550–9. doi: 10.1001/jamapsychiatry.2020.4614
10. Giordano GM, Bucci P, Mucci A, Pezzella P, Galderisi S. Gender differences in clinical and psychosocial features among persons with schizophrenia: A mini review. Front Psychiatry (2021) 12:789179. doi: 10.3389/fpsyt.2021.789179
11. Watson D, Levin-Aspenson HF, Waszczuk MA, Conway CC, Dalgleish T, Dretsch MN, et al. Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): III. Emotional dysfunction superspectrum. World Psychiatry (2022) 21(1):26–54. doi: 10.1002/wps.20943
12. Mesholam-Gately RI, Johnston D, Keshavan MS. What's in the name "schizophrenia"? A clinical, research and lived experience perspective. World Psychiatry (2023) 22(1):156–7. doi: 10.1002/wps.21033
13. Galderisi S. Promoting schizophrenia research in Europe: the contribution of the European Group for Research in Schizophrenia. World Psychiatry (2023) 22(3):486–7. doi: 10.1002/wps.21100
14. Fusar-Poli P, Estradé A, Stanghellini G, Venables J, Onwumere J, Messas G, et al. The lived experience of psychosis: a bottom-up review co-written by experts by experience and academics. World Psychiatry (2022) 21(2):168–88. doi: 10.1002/wps.20959
15. Galderisi S, Rossi A, Rocca P, Bertolino A, Mucci A, Bucci P, et al. Pathways to functional outcome in subjects with schizophrenia living in the community and their unaffected first-degree relatives. Schizophr Res (2016) 175(1-3):154–60. doi: 10.1016/j.schres.2016.04.043
16. Giordano GM, Brando F, Pezzella P, De Angelis M, Mucci A, Galderisi S. Factors influencing the outcome of integrated therapy approach in schizophrenia: A narrative review of the literature. Front Psychiatry (2022) 13:970210. doi: 10.3389/fpsyt.2022.970210
17. Harvey PD, Strassnig M. Predicting the severity of everyday functional disability in people with schizophrenia: cognitive deficits, functional capacity, symptoms, and health status. World Psychiatry (2012) 11(2):73–9. doi: 10.1016/j.wpsyc.2012.05.004
18. Rocca P, Brasso C, Montemagni C, Bellino S, Rossi A, Bertolino A, et al. Accuracy of self-assessment of real-life functioning in schizophrenia. NPJ Schizophrenia (2021) 7(1):11. doi: 10.1038/s41537-021-00140-9
19. Giuliani L, Giordano GM, Bucci P, Pezzella P, Brando F, Galderisi S. Improving knowledge on pathways to functional outcome in schizophrenia: main results from the italian network for research on psychoses. Front Psychiatry (2021) 12:791117. doi: 10.3389/fpsyt.2021.791117
20. Vita A, Barlati S, Deste G, Rocca P, Rossi A, Bertolino A, et al. The influence of autistic symptoms on social and non-social cognition and on real-life functioning in people with schizophrenia: Evidence from the Italian Network for Research on Psychoses multicenter study. Eur Psychiatry J Assoc Eur Psychiatrists. (2020) 63(1):e98. doi: 10.1192/j.eurpsy.2020.99
21. McDonald S, Pica S, Hayes RL, Baglioni AJ Jr. Stress and coping in early psychosis: Role of symptoms, self-efficacy, and social support in coping with stress. Br J Psychiatry (1998) 172(S33):122–7.
22. Rossi A, Galderisi S, Rocca P, Bertolino A, Mucci A, Rucci P, et al. The relationships of personal resources with symptom severity and psychosocial functioning in persons with schizophrenia: results from the Italian Network for Research on Psychoses study. Eur Arch Psychiatry Clin Neurosci (2017) 267(4):285–94. doi: 10.1007/s00406-016-0710-9
23. Ritsner MS, Ratner Y. The long-term changes in coping strategies in schizophrenia: temporal coping types. J Nerv Ment Dis (2006) 194(4):261–7. doi: 10.1097/01.nmd.0000207361.81947.52
24. Colizzi M, Cullen AE, Martland N, Di Forti M, Murray R, Schoeler T, et al. Association between stressful life events and psychosis relapse: a 2-year prospective study in first-episode psychosis. World Psychiatry (2023) 22(1):159–60. doi: 10.1002/wps.21046
25. Giordano GM, Galderisi S, Pezzella P, Perrottelli A, Bucci P. Determinants of clinical recovery in schizophrenia. In: Carpiniello B, Vita A, Mencacci C, editors. Recovery and major mental disorders. Cham: Springer International Publishing (2022). p. 23–43.
26. Galderisi S, Mucci A, Dollfus S, Nordentoft M, Falkai P, Kaiser S, et al. EPA guidance on assessment of negative symptoms in schizophrenia. Eur Psychiatry J Assoc Eur Psychiatrists (2021) 64(1):e23. doi: 10.1192/j.eurpsy.2021.11
27. Vita A, Gaebel W, Mucci A, Sachs G, Erfurth A, Barlati S, et al. European Psychiatric Association guidance on assessment of cognitive impairment in schizophrenia. Eur Psychiatry J Assoc Eur Psychiatrists (2022) 65(1):e58. doi: 10.1192/j.eurpsy.2022.2316
28. Galderisi S, Kaiser S, Bitter I, Nordentoft M, Mucci A, Sabé M, et al. EPA guidance on treatment of negative symptoms in schizophrenia. Eur Psychiatry J Assoc Eur Psychiatrists. (2021) 64(1):e21. doi: 10.1192/j.eurpsy.2021.13
29. Killaspy H, Harvey C, Brasier C, Brophy L, Ennals P, Fletcher J, et al. Community-based social interventions for people with severe mental illness: a systematic review and narrative synthesis of recent evidence. World Psychiatry (2022) 21(1):96–123. doi: 10.1002/wps.20940
30. Leichsenring F, Steinert C, Rabung S, Ioannidis JPA. The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry (2022) 21(1):133–45. doi: 10.1002/wps.20941
31. Ostuzzi G, Bertolini F, Tedeschi F, Vita G, Brambilla P, Del Fabro L, et al. Oral and long-acting antipsychotics for relapse prevention in schizophrenia-spectrum disorders: a network meta-analysis of 92 randomized trials including 22,645 participants. World Psychiatry (2022) 21(2):295–307. doi: 10.1002/wps.20972
32. Siskind D, Yung A. After the acute crisis - engaging people with psychosis in rehabilitation-oriented care. World Psychiatry (2022) 21(2):246–7. doi: 10.1002/wps.20970
33. Vita A, Gaebel W, Mucci A, Sachs G, Barlati S, Giordano GM, et al. European Psychiatric Association guidance on treatment of cognitive impairment in schizophrenia. Eur Psychiatry J Assoc Eur Psychiatrists. (2022) 65(1):e57. doi: 10.1192/j.eurpsy.2022.2315
34. McCutcheon RA, Pillinger T, Efthimiou O, Maslej M, Mulsant BH, Young AH, et al. Reappraising the variability of effects of antipsychotic medication in schizophrenia: a meta-analysis. World Psychiatry (2022) 21(2):287–94. doi: 10.1002/wps.20977
35. Leucht S, Schneider-Thoma J, Burschinski A, Peter N, Wang D, Dong S, et al. Long-term efficacy of antipsychotic drugs in initially acutely ill adults with schizophrenia: systematic review and network meta-analysis. World Psychiatry (2023) 22(2):315–24. doi: 10.1002/wps.21089
36. Kern RS, Gold JM, Dickinson D, Green MF, Nuechterlein KH, Baade LE, et al. The MCCB impairment profile for schizophrenia outpatients: results from the MATRICS psychometric and standardization study. Schizophr Res (2011) 126(1-3):124–31. doi: 10.1016/j.schres.2010.11.008
37. Dickinson D, Ramsey ME, Gold JM. Overlooking the obvious: a meta-analytic comparison of digit symbol coding tasks and other cognitive measures in schizophrenia. Arch Gen Psychiatry (2007) 64(5):532–42. doi: 10.1001/archpsyc.64.5.532
38. Knowles EE, David AS, Reichenberg A. Processing speed deficits in schizophrenia: reexamining the evidence. Am J Psychiatry (2010) 167(7):828–35. doi: 10.1176/appi.ajp.2010.09070937
39. Bosia M, Bechi M, Bosinelli F, Politi E, Buonocore M, Spangaro M, et al. From cognitive and clinical substrates to functional profiles: Disentangling heterogeneity in schizophrenia. Psychiatry Res (2019) 271:446–53. doi: 10.1016/j.psychres.2018.12.026
40. Fusar-Poli P, Deste G, Smieskova R, Barlati S, Yung AR, Howes O, et al. Cognitive functioning in prodromal psychosis: a meta-analysis. Arch Gen Psychiatry (2012) 69(6):562–71. doi: 10.1001/archgenpsychiatry.2011.1592
41. Gold S, Arndt S, Nopoulos P, O'Leary DS, Andreasen NC. Longitudinal study of cognitive function in first-episode and recent-onset schizophrenia. Am J Psychiatry (1999) 156(9):1342–8. doi: 10.1176/ajp.156.9.1342
42. Luther L, Suor JH, Rosen C, Jobe TH, Faull RN, Harrow M. Clarifying the direction of impact of negative symptoms and neurocognition on prospective work functioning in psychosis: A 20-year longitudinal study. Schizophr Res (2020) 220:232–9. doi: 10.1016/j.schres.2020.03.012
43. Wykes T, Reeder C, Corner J. The prevalence and stability of an executive processing deficit, response inhibition, in people with chronic schizophrenia. Schizophr Res (2000) 46(2-3):241–53. doi: 10.1016/S0920-9964(99)00233-9
44. Green MF, Kern RS, Braff DL, Mintz J. Neurocognitive deficits and functional outcome in schizophrenia: are we measuring the “Right stuff”? Schizophr Bull (2000) 26(1):119–36. doi: 10.1093/oxfordjournals.schbul.a033430
45. Green MF, Horan WP, Lee J. Nonsocial and social cognition in schizophrenia: current evidence and future directions. World Psychiatry (2019) 18(2):146–61. doi: 10.1002/wps.20624
46. Harvey PD, Strassnig MT. Cognition and disability in schizophrenia: cognition-related skills deficits and decision-making challenges add to morbidity. World Psychiatry (2019) 18(2):165–7. doi: 10.1002/wps.20647
47. Schmidt SJ, Mueller DR, Roder V. Social cognition as a mediator variable between neurocognition and functional outcome in schizophrenia: empirical review and new results by structural equation modeling. Schizophr Bull (2011) 37 Suppl 2(Suppl 2):S41–54. doi: 10.1093/schbul/sbr079
48. Ventura J, Hellemann GS, Thames AD, Koellner V, Nuechterlein KH. Symptoms as mediators of the relationship between neurocognition and functional outcome in schizophrenia: a meta-analysis. Schizophr Res (2009) 113(2-3):189–99. doi: 10.1016/j.schres.2009.03.035
49. Smelror RE, Rund BR, Lonning V, Jorgensen KN, Wedervang-Resell K, Andreassen OA, et al. Negative and disorganized symptoms mediate the relationship between verbal learning and global functioning in adolescents with early-onset psychosis. Eur Child Adolesc Psychiatry (2020) 29(12):1693–703. doi: 10.1007/s00787-020-01479-7
50. Deste G, Vita A, Nibbio G, Penn DL, Pinkham AE, Harvey PD. Autistic symptoms and social cognition predict real-world outcomes in patients with schizophrenia. Front Psychiatry (2020) 11:524. doi: 10.3389/fpsyt.2020.00524
51. Halverson TF, Orleans-Pobee M, Merritt C, Sheeran P, Fett AK, Penn DL. Pathways to functional outcomes in schizophrenia spectrum disorders: Meta-analysis of social cognitive and neurocognitive predictors. Neurosci Biobehav Rev (2019) 105:212–9. doi: 10.1016/j.neubiorev.2019.07.020
52. Sachs G, Steger-Wuchse D, Kryspin-Exner I, Gur RC, Katschnig H. Facial recognition deficits and cognition in schizophrenia. Schizophr Res (2004) 68(1):27–35. doi: 10.1016/S0920-9964(03)00131-2
53. Sachs G, Winklbaur B, Jagsch R, Lasser I, Kryspin-Exner I, Frommann N, et al. Training of affect recognition (TAR) in schizophrenia–impact on functional outcome. Schizophr Res (2012) 138(2-3):262–7. doi: 10.1016/j.schres.2012.03.005
54. Glenthøj LB, Albert N, Fagerlund B, Kristensen TD, Wenneberg C, Hjorthøj C, et al. Emotion recognition latency, but not accuracy, relates to real life functioning in individuals at ultra-high risk for psychosis. Schizophr Res (2019) 210:197–202. doi: 10.1016/j.schres.2018.12.038
55. Pinkham AE, Penn DL, Green MF, Buck B, Healey K, Harvey PD. The social cognition psychometric evaluation study: results of the expert survey and RAND panel. Schizophr Bull (2014) 40(4):813–23. doi: 10.1093/schbul/sbt081
56. Green MF, Bearden CE, Cannon TD, Fiske AP, Hellemann GS, Horan WP, et al. Social cognition in schizophrenia, Part 1: performance across phase of illness. Schizophr Bull (2012) 38(4):854–64. doi: 10.1093/schbul/sbq171
57. Horan WP, Green MF, DeGroot M, Fiske A, Hellemann G, Kee K, et al. Social cognition in schizophrenia, Part 2: 12-month stability and prediction of functional outcome in first-episode patients. Schizophr Bull (2012) 38(4):865–72. doi: 10.1093/schbul/sbr001
58. Corcoran CM, Keilp JG, Kayser J, Klim C, Butler PD, Bruder GE, et al. Emotion recognition deficits as predictors of transition in individuals at clinical high risk for schizophrenia: a neurodevelopmental perspective. Psychol Med (2015) 45(14):2959–73. doi: 10.1017/S0033291715000902
59. Fett AK, Viechtbauer W, Dominguez MD, Penn DL, van Os J, Krabbendam L. The relationship between neurocognition and social cognition with functional outcomes in schizophrenia: a meta-analysis. Neurosci Biobehav Rev (2011) 35(3):573–88. doi: 10.1016/j.neubiorev.2010.07.001
60. Irani F, Seligman S, Kamath V, Kohler C, Gur RC. A meta-analysis of emotion perception and functional outcomes in schizophrenia. Schizophr Res (2012) 137(1-3):203–11. doi: 10.1016/j.schres.2012.01.023
61. Addington J, Saeedi H, Addington D. Influence of social perception and social knowledge on cognitive and social functioning in early psychosis. Br J Psychiatry J Ment science. (2006) 189:373–8. doi: 10.1192/bjp.bp.105.021022
62. Ventura J. Computer-based virtual reality assessment of functional capacity in primary psychosis. World Psychiatry (2022) 21(3):464–5. doi: 10.1002/wps.21024
63. Couture SM, Penn DL, Roberts DL. The functional significance of social cognition in schizophrenia: a review. Schizophr Bull (2006) 32 Suppl 1(Suppl 1):S44–63. doi: 10.1093/schbul/sbl029
64. González-Ortega I, González-Pinto A, Alberich S, Echeburúa E, Bernardo M, Cabrera B, et al. Influence of social cognition as a mediator between cognitive reserve and psychosocial functioning in patients with first episode psychosis. Psychol Med (2020) 50(16):2702–10. doi: 10.1017/S0033291719002794
65. Ruiz-Toca A, Fernández-Aragón C, Madrigal A, Halverson T, Rodríguez-Jiménez R, Lahera G. Social cognition mediates the impact of processing speed and sustained attention on global functioning in schizophrenia. Psicothema. (2023) 35(1):87–97. doi: 10.7334/psicothema2022.8
66. Sergi MJ, Rassovsky Y, Nuechterlein KH, Green MF. Social perception as a mediator of the influence of early visual processing on functional status in schizophrenia. Am J Psychiatry (2006) 163(3):448–54. doi: 10.1176/appi.ajp.163.3.448
67. Uchino T, Okubo R, Takubo Y, Aoki A, Wada I, Hashimoto N, et al. Mediation effects of social cognition on the relationship between neurocognition and social functioning in major depressive disorder and schizophrenia spectrum disorders. J Personalized Med (2023) 13(4):683. doi: 10.3390/jpm13040683
68. Addington J, Saeedi H, Addington D. Facial affect recognition: a mediator between cognitive and social functioning in psychosis? Schizophr Res (2006) 85(1-3):142–50. doi: 10.1016/j.schres.2006.03.028
69. Giordano GM, Caporusso E, Pezzella P, Galderisi S. Updated perspectives on the clinical significance of negative symptoms in patients with schizophrenia. Expert Rev Neurotherapeutics (2022) 22(7):541–55. doi: 10.1080/14737175.2022.2092402
70. Starzer M, Hansen HG, Hjorthøj C, Albert N, Nordentoft M, Madsen T. 20-year trajectories of positive and negative symptoms after the first psychotic episode in patients with schizophrenia spectrum disorder: results from the OPUS study. World Psychiatry (2023) 22(3):424–32. doi: 10.1002/wps.21121
71. Marder SR, Galderisi S. The current conceptualization of negative symptoms in schizophrenia. World Psychiatry (2017) 16(1):14–24. doi: 10.1002/wps.20385
72. Rocca P, Montemagni C, Zappia S, Pitera R, Sigaudo M, Bogetto F. Negative symptoms and everyday functioning in schizophrenia: a cross-sectional study in a real world-setting. Psychiatry Res (2014) 218(3):284–9. doi: 10.1016/j.psychres.2014.04.018
73. Moura BM, Isvoranu AM, Kovacs V, Van Rooijen G, Van Amelsvoort T, Simons CJP, et al. The puzzle of functional recovery in schizophrenia-spectrum disorders-replicating a network analysis study. Schizophr Bull (2022) 48(4):871–80. doi: 10.1093/schbul/sbac018
74. Lee EHM, Hui CLM, Chan KPK, Chan PY, Law EYL, Chong CSY, et al. The role of symptoms and insight in mediating cognition and functioning in first episode psychosis. Schizophr Res (2019) 206:251–6. doi: 10.1016/j.schres.2018.11.009
75. Lin CH, Huang CL, Chang YC, Chen PW, Lin CY, Tsai GE, et al. Clinical symptoms, mainly negative symptoms, mediate the influence of neurocognition and social cognition on functional outcome of schizophrenia. Schizophr Res (2013) 146(1-3):231–7. doi: 10.1016/j.schres.2013.02.009
76. Glenthøj LB, Jepsen JR, Hjorthøj C, Bak N, Kristensen TD, Wenneberg C, et al. Negative symptoms mediate the relationship between neurocognition and function in individuals at ultrahigh risk for psychosis. Acta psychiatrica Scandinavica (2017) 135(3):250–8. doi: 10.1111/acps.12682
77. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull (1987) 13(2):261–76. doi: 10.1093/schbul/13.2.261
78. Wallwork RS, Fortgang R, Hashimoto R, Weinberger DR, Dickinson D. Searching for a consensus five-factor model of the Positive and Negative Syndrome Scale for schizophrenia. Schizophr Res (2012) 137(1-3):246–50. doi: 10.1016/j.schres.2012.01.031
79. Kirkpatrick B, Strauss GP, Nguyen L, Fischer BA, Daniel DG, Cienfuegos A, et al. The brief negative symptom scale: psychometric properties. Schizophr Bull (2011) 37(2):300–5. doi: 10.1093/schbul/sbq059
80. Kirkpatrick B, Fenton WS, Carpenter WT Jr., Marder SR. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr Bull (2006) 32(2):214–9. doi: 10.1093/schbul/sbj053
81. Mucci A, Galderisi S, Merlotti E, Rossi A, Rocca P, Bucci P, et al. The Brief Negative Symptom Scale (BNSS): Independent validation in a large sample of Italian patients with schizophrenia. Eur Psychiatry J Assoc Eur Psychiatrists (2015) 30(5):641–7. doi: 10.1016/j.eurpsy.2015.01.014
82. Karbasforoushan H, Duffy B, Blackford JU, Woodward ND. Processing speed impairment in schizophrenia is mediated by white matter integrity. Psychol Med (2015) 45(1):109–20. doi: 10.1017/S0033291714001111
83. Keefe RS, Goldberg TE, Harvey PD, Gold JM, Poe MP, Coughenour L. The Brief Assessment of Cognition in Schizophrenia: reliability, sensitivity, and comparison with a standard neurocognitive battery. Schizophr Res (2004) 68(2-3):283–97. doi: 10.1016/j.schres.2003.09.011
84. Sachs G, Winklbaur B, Jagsch R, Keefe RS. Validation of the German version of the brief assessment of cognition in Schizophrenia (BACS) - preliminary results. Eur Psychiatry J Assoc Eur Psychiatrists (2011) 26(2):74–7. doi: 10.1016/j.eurpsy.2009.10.006
85. Kerr SL, Neale JM. Emotion perception in schizophrenia: specific deficit or further evidence of generalized poor performance? J Abnormal Psychol (1993) 102(2):312–8. doi: 10.1037/0021-843X.102.2.312
86. Nasrallah H, Morosini P, Gagnon DD. Reliability, validity and ability to detect change of the Personal and Social Performance scale in patients with stable schizophrenia. Psychiatry Res (2008) 161(2):213–24. doi: 10.1016/j.psychres.2007.11.012
87. Bowie CR, Leung WW, Reichenberg A, McClure MM, Patterson TL, Heaton RK, et al. Predicting schizophrenia patients' real-world behavior with specific neuropsychological and functional capacity measures. Biol Psychiatry (2008) 63(5):505–11. doi: 10.1016/j.biopsych.2007.05.022
88. Bowie CR, Reichenberg A, Patterson TL, Heaton RK, Harvey PD. Determinants of real-world functional performance in schizophrenia subjects: correlations with cognition, functional capacity, and symptoms. Am J Psychiatry (2006) 163(3):418–25. doi: 10.1176/appi.ajp.163.3.418
89. Leifker FR, Bowie CR, Harvey PD. Determinants of everyday outcomes in schizophrenia: the influences of cognitive impairment, functional capacity, and symptoms. Schizophr Res (2009) 115(1):82–7. doi: 10.1016/j.schres.2009.09.004
90. García-Portilla MP, García-Álvarez L, González-Blanco L, Dal Santo F, Bobes-Bascarán T, Martínez-Cao C, et al. Real-world functioning in patients with schizophrenia: beyond negative and cognitive symptoms. Front Psychiatry (2021) 12:700747. doi: 10.3389/fpsyt.2021.700747
91. Meyer EC, Carrión RE, Cornblatt BA, Addington J, Cadenhead KS, Cannon TD, et al. The relationship of neurocognition and negative symptoms to social and role functioning over time in individuals at clinical high risk in the first phase of the North American Prodrome Longitudinal Study. Schizophr Bull (2014) 40(6):1452–61. doi: 10.1093/schbul/sbt235
92. Nakagami E, Xie B, Hoe M, Brekke JS. Intrinsic motivation, neurocognition and psychosocial functioning in schizophrenia: testing mediator and moderator effects. Schizophr Res (2008) 105(1-3):95–104. doi: 10.1016/j.schres.2008.06.015
93. Brittain P, Ffytche DH, McKendrick A, Surguladze S. Visual processing, social cognition and functional outcome in schizophrenia. Psychiatry Res (2010) 178(2):270–5. doi: 10.1016/j.psychres.2009.09.013
94. Horton HK, Silverstein SM. Social cognition as a mediator of cognition and outcome among deaf and hearing people with schizophrenia. Schizophr Res (2008) 105(1):125–37. doi: 10.1016/j.schres.2008.07.003
95. Rassovsky Y, Horan WP, Lee J, Sergi MJ, Green MF. Pathways between early visual processing and functional outcome in schizophrenia. Psychol Med (2011) 41(3):487–97. doi: 10.1017/S0033291710001054
96. Sergi MJ, Rassovsky Y, Nuechterlein KH, Green MF. Social perception as a mediator of the influence of early visual processing on functional status in schizophrenia. Am J Psychiatry (2006) 163(3):448–54. doi: 10.1176/appi.ajp.163.3.448
97. Ayesa-Arriola R, Setién-Suero E, Neergaard KD, Ferro A, Fatjó-Vilas M, Ríos-Lago M, et al. Evidence for trait related theory of mind impairment in first episode psychosis patients and its relationship with processing speed: A 3 year follow-up study. Front Psychol (2016) 7:592. doi: 10.3389/fpsyg.2016.00592
98. Tsotsi S, Bozikas VP, Kosmidis MH. The role of attention processes in facial affect recognition in schizophrenia. Cogn Neuropsychiatry (2015) 20(6):526–41. doi: 10.1080/13546805.2015.1110517
99. Andrade-González N, Sarasa M, García-López A, Leonés I, Halverson TF, Lahera G. Mentalizing errors in patients with schizophrenia who received psychosocial rehabilitation: a case-control study. Psychiatr Quarterly (2021) 92(3):947–59. doi: 10.1007/s11126-020-09863-x
100. Thibaudeau É, Achim AM, Parent C, Turcotte M, Cellard C. A meta-analysis of the associations between theory of mind and neurocognition in schizophrenia. Schizophr Res (2020) 216:118–28. doi: 10.1016/j.schres.2019.12.017
101. Catalan A, Angosto V, Díaz A, Martínez N, Guede D, Pereda M, et al. The relationship between theory of mind deficits and neurocognition in first episode-psychosis. Psychiatry Res (2018) 268:361–7. doi: 10.1016/j.psychres.2018.06.066
102. Sjølie C, Meyn EK, Raudeberg R, Andreassen OA, Vaskinn A. Nonsocial cognitive underpinnings of theory of mind in schizophrenia. Psychiatry Res (2020) 289:113055. doi: 10.1016/j.psychres.2020.113055
103. Grant N, Lawrence M, Preti A, Wykes T, Cella M. Social cognition interventions for people with schizophrenia: a systematic review focussing on methodological quality and intervention modality. Clin Psychol Review (2017) 56:55–64. doi: 10.1016/j.cpr.2017.06.001
104. Kurtz MM, Gagen E, Rocha NBF, MaChado S, Penn DL. Comprehensive treatments for social cognitive deficits in schizophrenia: A critical review and effect-size analysis of controlled studies. Clin Psychol Review (2016) 43:80–9. doi: 10.1016/j.cpr.2015.09.003
105. Pinkham AE, Penn DL. Neurocognitive and social cognitive predictors of interpersonal skill in schizophrenia. Psychiatry Res (2006) 143(2):167–78. doi: 10.1016/j.psychres.2005.09.005
106. Sachs G, Lasser I, Purdon SE, Erfurth A. Screening for cognitive impairment in schizophrenia: Psychometric properties of the German version of the Screen for Cognitive Impairment in Psychiatry (SCIP-G). Schizophr Res Cognition. (2021) 25:100197. doi: 10.1016/j.scog.2021.100197
107. Schaefer J, Giangrande E, Weinberger DR, Dickinson D. The global cognitive impairment in schizophrenia: Consistent over decades and around the world. Schizophr Res (2013) 150(1):42–50. doi: 10.1016/j.schres.2013.07.009
108. Kohler CG, Walker JB, Martin EA, Healey KM, Moberg PJ. Facial emotion perception in schizophrenia: A meta-analytic review. Schizophr Bulletin (2009) 36(5):1009–19. doi: 10.1093/schbul/sbn192
109. Emsley R, Dunn G, White IR. Mediation and moderation of treatment effects in randomised controlled trials of complex interventions. Stat Methods Med Res (2010) 19(3):237–70. doi: 10.1177/0962280209105014
110. MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Annu Rev Psychol (2007) 58:593–614. doi: 10.1146/annurev.psych.58.110405.085542
111. Keshavan MS, Eack SM. Cognitive enhancement interventions are effective for schizophrenia: why not provide them early? World Psychiatry (2023) 22(2):326–7. doi: 10.1002/wps.21091
112. Schäfer SK, Thomas LM, Lindner S, Lieb K. World Health Organization's low-intensity psychosocial interventions: a systematic review and meta-analysis of the effects of Problem Management Plus and Step-by-Step. World Psychiatry (2023) 22(3):449–62. doi: 10.1002/wps.21129
Keywords: schizophrenia, negative symptoms, expressive deficit, motivational deficit, emotion recognition, processing speed, mediation analysis
Citation: Giordano GM, Pezzella P, Mucci A, Austin SF, Erfurth A, Glenthøj B, Hofer A, Hubenak J, Libiger J, Melle I, Nielsen MØ, Rybakowski JK, Wojciak P, Galderisi S and Sachs G (2024) Negative symptoms and social cognition as mediators of the relationship between neurocognition and functional outcome in schizophrenia. Front. Psychiatry 15:1333711. doi: 10.3389/fpsyt.2024.1333711
Received: 05 November 2023; Accepted: 15 January 2024;
Published: 31 January 2024.
Edited by:
Wing Chung Chang, The University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Stefano Barlati, University of Brescia, ItalyCristiana Montemagni, Università Degli Studi di Torino, Italy
Matthias Kirschner, University of Zurich, Switzerland
Copyright © 2024 Giordano, Pezzella, Mucci, Austin, Erfurth, Glenthøj, Hofer, Hubenak, Libiger, Melle, Nielsen, Rybakowski, Wojciak, Galderisi and Sachs. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Armida Mucci, armida.mucci@gmail.com
†These authors have contributed equally to this work