
Abstract
Objective: The purpose of the present analysis of a series of controlled clinical studies was to evaluate the efficacy and tolerability of the fixed-combination preparation Arlevert® (ARL; cinnarizine 20mg/dimenhydrinate 40mg) in the treatment of central, peripheral or combined central/peripheral vestibular vertigo.
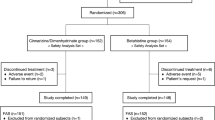
Participants: Six hundred and thirty-five patients participated in five randomised, double-blind, active-and/or placebo-controlled clinical studies carried out in nine European clinics.
Interventions: The patients received one of the following treatments three times daily for 4 weeks, according to randomisation: ARL, cinnarizine 20mg (CZ 20), cinnarizine 50mg (CZ 50), dimenhydrinate 40mg (DH 40), dimenhydrinate 100mg (DH 100), betahistine 12mg (BH) or placebo.
Results: After 4 weeks’ treatment, the fixed-combination ARL led to statistically significantly better improvements in vertigo symptoms (the primary efficacy variable) than monotherapy with its active constituents at the same dosage (p = 0.021 vs CZ 20; p = 0.018 vs DH 40) or at 2.5-fold higher dosage (p < 0.001 vs both CZ 50 and DH 100); ARL was also significantly more effective than BH and placebo (p < 0.001 vs both). Vestibulospinal testing by craniocorpography showed that ARL produced significantly greater decreases in lateral sway (Unterberger test) than CZ 50, DH 100, placebo (p < 0.001 vs all), DH 40 (p = 0.027) and BH (p = 0.039). ARL also markedly reduced vegetative concomitant symptoms. Across treatment groups, 70 to 98% of the patients judged the tolerability as ‘good’ or ‘very good’ (ARL = 90.3%). The rate of adverse events with ARL was similar to or lower than that with the standard treatments. Reported adverse events corresponded to those already recognised for each drug. No serious adverse events were observed.
Conclusion: The analysis demonstrates that the fixed combination of cinnarizine 20mg and dimenhydrinate 40mg given three times daily is an effective and well tolerated treatment for central, peripheral and combined central/peripheral vertigo. Because of a significantly superior efficacy in comparison with its active constituents given alone, as well as compared with the standard monotherapies using CZ 50, DH 100 and BH, the fixed-combination ARL can be considered as a first-line treatment option for vertigo.
Similar content being viewed by others


References
Honrubia V, Bell TS, Harris MR, et al. Quantitative evaluation of dizziness characteristics and impact on quality of life. Am J Otol 1996; 17: 595–602
Aschoff JC. Diagnostic problems in dizziness or vertigo [in German]. HNO 1978; 26: 149–54
Bird JC, Beynon GJ, Prevost AT, et al. An analysis of referral patterns for dizziness in the primary care setting. Br J Gen Pract 1998; 48: 1828–32
Overstall PW. Rehabilitation of elderly patients with disorders of balance. In: Hinchcliffe R, editor. Hearing and balance in the elderly. Edinburgh: Churchill Livingstone, 1983
Oosterveld WJ. Vertigo. Current concepts in management. Drugs 1985; 30: 275–83
Godfraind T, Towse G, van Nueten JM. Cinnarizine —a selective calcium entry blocker. Drugs Today 1982; 18: 27–42
Oosterveld WJ. Cinnarizine in the vertiginous syndrome. In: Towse G, editor. Cinnarizine and the vertiginous syndrome. International Congress and Symposium Series No. 33. London: Royal Society of Medicine and Academic Press Inc., 1979: 29–37
Jaju BP, Wang SC. Effects of diphenhydramine and dimenhydrinate on vestibular neuronal activity of cat: a search for the locus of their antimotion sickness action. J Pharmacol Exp Ther 1971; 176: 718–24
Kukwa L. Selektive pharmakotherapeutische Stammhirndämpfung. 2nd ed. Hamburg, Neu-Isenburg: edition m + p dr. werner rudat, 1981: 9-14
Ben-David J, Podoshin L, Fradis M. A comparative craniocorpography study on the findings in the Romberg standing test versus the Unterberger/Fukuda stepping test in vertigo patients. Acta Otorhinolaryngol Belg 1985; 39(6): 924–32
Jongkees LBW. Which is the preferable method of performing the caloric test? Arch Otolaryngol 1949; 49: 594
Stoll, W, Matz DR, Most, E, et.al. Schwindel und Gleichgewichtsstörungen. 3. überarbeitete und erweiterte Auflage. Stuttgart: Thieme Verlag, 1998
McClure JA, Lycett P. Vestibular asymmetry. Some theoretical and practical considerations. Arch Otolaryngol 1983; 109: 682–7
Aust G. Vestibular disturbances in the elderly [in German]. HNO 1991; 39: 460–6
Luxon L. Comparison of assessment of caloric nystagmus by observation of duration and by electronystagmographic measurement of slow-phase velocity. Br J Audiol 1995; 29: 107–16
Nilles R. A direct effect of calcium antagonists in the inner ear: blockade of abnormal calcium increase in outer hair cells of the guinea pig [in German]. HNO 1995; 43: 716–23
Martinez DM. The effect of Serc (betahistine hydrochloride) on the circulation of the inner ear in experimental animals. Acta Otolaryngol Suppl. (Stockh) 1972; 305: 29–47
Snow JB, Suga F. Control of the microcirculation of the inner ear. Otolaringol. Clin North Am 1975; 8: 455–66
Fischer AJEM. Histamine in the treatment of vertigo. Acta Otolaryngol Suppl. (Stockh) 1991; 479: 24–8
Kostriza R, Novotný M, Skutil J, et al. The influence of the vasoactive drugs on the blood flow in cochleovestibular diseases. In: Claussen CF, Virtane MV, Constantinescu L, et al., editors. Giddiness & vestibulo-spinal investigations. Combined audio-vestibular investigations. Experimental neurootology. Amsterdam: Elsevier; 1996: 149–52
Luxon LM. Disturbances of balance in the elderly. Br J Hosp Med 1991; 45: 22–6
Keßler L. Treatment of vertigo with a combination of cinnarizine and dimenhydrinate [abstract]. Eur Arch Otorhinolaryngol 1998; 255: 80
Dollery C, editor. Therapeutic drugs. Edinburgh: Churchill Livingstone, 1991; 1: D164–68
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schremmer, D., Bognar-Steinberg, I., Baumann, W. et al. Efficacy and Tolerability of a Fixed Combination of Cinnarizine and Dimenhydrinate in Treatment of Vertigo. Clin. Drug Investig. 18, 355–368 (1999). https://doi.org/10.2165/00044011-199918050-00003
Published:
Issue Date:
DOI: https://doi.org/10.2165/00044011-199918050-00003