
Abstract
Background
Ideal perioperative management of pheochromocytomas/paragangliomas (pheo) is a subject of debate and can be highly variable. The purpose of this study was to identify potential predictive factors of hemodynamic instability during pheo resection.
Methods
A retrospective review of pheo resections from 1992 to 2013 was undertaken. Intraoperative hemodynamics, patient demographics, tumor characteristics, and perioperative management were examined. Postoperative intensive-care admission, myocardial infarction, stroke, and 30-day mortality were reviewed. Linear regression was used to analyze factors influencing intraoperative hemodynamics.
Results
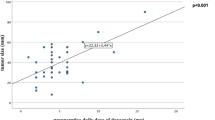
During the 20-year study period, 100 patients underwent pheo resection. Postoperative morbidity and mortality was significantly reduced (p = 0.003) in the last 10 years of practice, and there was a trend towards greater morbidity and mortality with intraoperative hemodynamic instability (p = 0.06). The preoperative dose of phenoxybenzamine and the number of laparoscopic procedures has increased in the last decade [59 mg (95 % CI 32–108) to 106 mg (95 % CI 91–124), p = 0.008, and 27 vs. 54 %, p = 0.05, respectively]. Increased preoperative phenoxybenzamine dose was a significant predictor of improved intraoperative hemodynamic stability (p = 0.01). Lack of intraoperative magnesium use resulted in greater hemodynamic instability as preoperative systolic blood pressure increased (p = 0.002).
Conclusions
Postoperative outcomes following pheo resection have improved over the last two decades. Preoperative α-blockade plays a significant role in improving intraoperative hemodynamics and post-op outcomes. Increased doses of phenoxybenzamine and utilization of laparoscopic approaches have likely contributed to improved outcomes in the last decade. Intraoperative magnesium use may provide protection against hemodynamic instability and warrants further study.

Similar content being viewed by others


References
Hull C. Pheochromocytoma: diagnosis, preoperative preparation and anaesthetic management. Br J Anaesth. 1986;58:1453–68.
Kinney M, Warner M, vanHeerden J, Horlocker T, Young W, Schroeder D, et al. Perianesthetic risks and outcomes of pheochromocytoma and paraganglioma resection. Anesth Analg. 2000;91:1118–23.
Apgar V, Papper EM. Pheochromocytoma: anesthetic management during surgical treatment. Arch Surg. 1951;62:634–48.
Desmonts JM, le Houelleur J, Remond P, Duvaldestin P. Anaesthetic management of patients with pheochromocytoma: a review of 102 cases. Br J Anaesth. 1977;49:991–7.
Van Heerden HA, Roland CF, Carney JA, et al. Long-term evaluation following resection of apparently benign pheochromocytoma(s)/paraganglioma(s). World J Surg. 1990;14:325–9.
Warner MA, vanHeerden JA. Anesthetic and surgical management at the May Clinic. In: Manager WM, Gifford RW (eds). Clinical and experimental pheochromocytoma. 2nd ed. Cambridge: Blackwell Science;1996; 388–407.
Pacak K, Eisenhofer G, Ahlman H et al. Pheochromocytoma: recommendations for clinical practice from the first international symposium. Nat Clin Pract Endocrinol Metab. 2007; 3:92–102.
Wellbourn RB. Early surgical history of phaeochromocytoma. Br J Surg. 1987;74:594–6.
Boutros A, Bravo E, Zenettin G, et al. Perioperative management of 63 patients with pheochromocytoma. Cleve Clin J Med. 1990;57:613–617.
Steinsapir J, Carr A, Prisant M, et al. Metyrosin and pheochromocytoma. Arch Intern Med. 1997;157:901–6.
Horst-Schrivers A, Kerstens M, Wolffenbuttel B. Preoperative pharmacological management of phaeochromocytoma. Neth J Med. 2006;64(8):290–5.
Agrawal R, Mishra S, Bhatia E, et al. Prospective study to compare the perioperative hemodynamic alterations following preparation for pheochromocytoma surgery by phenoxybenzamine or prazosin. World J Surg. 2014;38:716–23.
Bruynzeel H, Feelders A, Groenland T, et al. Risk factors for hemodynamic instability during surgery for pheochromocytoma. J Clin Endorcinol Metab. 2010;95:678–85.
Gagner M, Pomp A, Neniford B, et al. Laparoscopic adrenalectomy: lessons learned from 100 consecutive procedures. Ann Surg. 1997;226:238–46.
Kim H, Kim G, Sung G. Laparoscopic adrenalectomy for pheochromoctyoma: comparison with conventional open adrenalectomy. J Endourol. 2004;18:251–5.
Jankovic R, Konstantinovic S, Milic D, et al. Can a patient be successfully prepared for pheochromocytoma surgery in three days? A case report. Minerva Anestesiol. 2007;73:245–8.
James M. Use of magnesium sulphate in the anaesthetic management of pheochromocytoma: a review of 17 anaesthetics. Br J Anaesth. 1989;62:616–23.
James M. Clinical use of magnesium infusions in anesthesia. Anesth Analg. 1992;74:129–36.
Evan G. Magnesium sulfate and epidural anesthesia in pheochromocytoma and severe coronary artery disease. Anesth Analg. 1995;81:414–6.
Lord M, Augoustides J. Perioperative management of pheochromocytoma: focus on magnesium, clevidipine, and vasopressin. J Cardiothor Vasc Anesth. 2012;26(3):526–31.
Cook R, McDonald J, Nunziata E. Differences between hand-written and automatic blood pressure records. Anesthesiology 1989;71:385–90.
Conflict of interest
Margaret Livingstone, Kaylene Duttchen, Jenny Thompson, Zahid Sunderani, Geoffrey Hawboldt, M. Sarah Rose, and Janice Pasieka have no financial or commercial interests to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Livingstone, M., Duttchen, K., Thompson, J. et al. Hemodynamic Stability During Pheochromocytoma Resection: Lessons Learned Over the Last Two Decades. Ann Surg Oncol 22, 4175–4180 (2015). https://doi.org/10.1245/s10434-015-4519-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4519-y