
Abstract
Background
First implantation of a totally implantable venous access device (TIVAD) was performed in 1982 with surgical technique. Since then, these devices have permitted infusion of total parenteral nutrition, antibiotics, blood products, and, above all, they have definitively changed the quality of life of patients with cancer. However, with the increase of percutaneous procedures, we have assisted with a concomitant raise of immediate postprocedural life-threatening complications. The aim of this study was to review the literature during a 27-year period, with regard to the changes of incidence of immediate complications after percutaneous or surgical cutdown for TIVAD’s implant.
Materials and Methods
An extensive search of relevant literature was carried out by using MEDLINE (PubMed) and Google Scholar. We gathered articles from 1982 to 2009 that quoted patient’s number, type of pathology, specialist involved, number of devices implanted, site and technique of implantation (surgical cutdown or percutaneous technique), and immediate complications occurrence.
Results
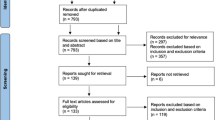
A total of 952 reports were screened, and finally only 45 articles addressing all inclusion criteria were used for the present study. A total of 11,430 TIVADs implanted in 11,381 patients were analyzed. Pneumothorax, hemothorax, arterial puncture, and hemoptysis developed only after percutaneous procedures. Atrial fibrillation, hematomas, and malpositioning were more frequent after percutaneous approach. The total amount of immediate complications in patients submitted to percutaneous implant was 4.5%, compared with 0.9% subsequent to cutdown technique.
Conclusions
Despite the increased use of percutaneous technique for TIVADs’ implantation, surgical cutdown, because of its safety, remains the best approach to avoid possible fatal immediate complications.


Similar content being viewed by others

References
Dudrick JJ, Wilmore DW, Vars HM, Rhoads JE. Long-term total parenteral nutrition with growth development and positive nitrose balance. Surgery. 1968;64:134–42.
Niederhuber JE, Ensminger W, Gyves JW, Liepman M, Doan K, Cozzi E. Totally implanted venous and arterial access system to replace external catheters in cancer treatment. Surgery. 1982;92:706–12.
Starkhammar H, Bengtsson M. Totally implanted device for venous access. Experience in tumour patients. Acta Radiol Oncol. 1985;24:173–6.
Morris SL, Jaques PF, Mauro MA. Radiology-assisted placement of implantable subcutaneous infusion ports for long-term venous access. Radiology. 1992;184:149–51.
Laurenzi L, Fimiani C, Faglieri N, Natoli S, Milasi G, Tirelli W, et al. Complications with fully implantable venous access systems in oncologic patients. Tumori. 1996;82:232–6.
Lorch H, Zwaan M, Kagel C, Weiss HD. Central venous access ports placed by interventional radiologists: experience with 125 consecutive patients. Cardiovasc Intervent Radiol. 2001;24:180–4.
Munro FD, Gillett PM, Wratten JC, Shaw MP, Thomas A, MacKinlay GA, et al. Totally implantable central venous access devices for paediatric oncology patients. Med Pediatr Oncol. 1999;33:377–81.
Deogaonkar K, Shokrollahi K, Dickson WA. Haemothorax: a potentially fatal complication of subclavian cannulation—a case report. Resuscitation. 2007;72:161–3.
Lewis CA, Allen TE, Burke DR, Cardella JF, Citron SJ, Cole PE. Quality improvement guidelines for central venous access. J Vasc Interv Radiol. 1997;8:475–9.
Lewis CA, Allen TE, Burke DR, Cardella JF, Citron SJ, Cole PE, et al. Society of Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for central venous access. J Vasc Interv Radiol. 2003;14:S231–5.
Bothe A Jr, Piccione W, Ambrosino JJ, Benotti PN, Lokich JJ. Implantable central venous access system. Am J Surg. 1984;147:565–9.
Champault G. (1985) Completely implantable catheters for anticancer chemotherapy. A French experience of 325 cases. J Chir (Paris). 122:269–72.
Stanislav GV, Fitzgibbons RJ Jr, Bailey RT Jr, Mailliard JA, Johnson PS, Feole JB. Reliability of implantable central venous access devices in patients with cancer. Arch Surg. 1987;122:1280–3.
Koonings PP, Given FT Jr. Long-term experience with a totally implanted catheter system in gynecologic oncologic patients. J Am Coll Surg. 1994;178:164–6.
Bertoglio S, Meszsaros P, Disomma C, Moresco L, Cafiero F, Gipponi M, et al. Long-term central venous access in oncology. Review of a caseload of 750 cases. Minerva Chir. 1996;51:427–31.
Aldrighetti L, Paganelli M, Caterini R, Catena M, Ronzoni M, Ferla G. Safety and efficiency of totally implantable devices for prolonged venous access. A prospective study. J Chemother. 1996;8:393–6.
Ballarini C, Intra M, Pisani Ceretti A, Cordovana A, Prestipino F, Farina G, et al. Le complicanze precoci e tardive dei sistemi venosi impiantabili per chemioterapia a lungo termine nei pazienti oncologici. Osp Ital Chir. 1997;6:517–23.
Miller K, Buchanan GR, Zappa S, Cochran C, Laufenberg J, Medeiros D, et al. Implantable venous access devices in children with hemophilia: a report of low infection rates. J Pediatr. 1998;132:934–8.
Domingo P, Fontanet A, Sánchez F, Allende L, Vazquez G. Morbidity associated with long-term use of totally implantable ports in patients with AIDS. Clin Infect Dis. 1999;29:346–51.
Boussen H, Mtaallah M, Dhiab T, Khalfallah S, Jerbi G, Hechiche M, et al. Evaluation of implantable sites in medical oncology in Tunisia. Prospective study of 205 cases. Ann Fr Anesth Reanim. 2001;20:509–13.
Lorenz JM, Funaki B, Van Ha T, Leef JA. Radiologic placement of implantable chest ports in pediatric patients. AJR Am J Roentgenol. 2001;176:991–4.
Yip D, Funaki B. Subcutaneous chest ports via the internal jugular vein. A retrospective study of 117 oncology patients. Acta Radiol. 2002;43:371–5.
Carlo JT, Lamont JP, McCarty TM, Livingston S, Kuhn JA. A prospective randomized trial demonstrating valved implantable ports have fewer complications and lower overall cost than nonvalved implantable ports, Am J Surg. 2004;188:722–7.
Biffi R, Pozzi S, Agazzi A, Pace U, Floridi A, Cenciarelli S, et al. Use of totally implantable central venous access ports for high-dose chemotherapy and peripheral blood stem cell transplantation: results of a monocentre series of 376 patients. Ann Oncol. 2004;15:296–300.
Charvát J, Linke Z, Horáèková M, Prausová J. Implantation of central venous ports with catheter insertion via the right internal jugular vein in oncology patients: single center experience. Support Care Cancer. 2006;14:1162–5.
Cil BE, Canyiğit M, Peynircioğlu B, Hazirolan T, Carkaci S, Cekirge S, et al. Subcutaneous venous port implantation in adult patients: a single center experience. Diagn Interv Radiol. 2006;12:93–8.
Araújo C, Silva JP, Antunes P, Fernandes JM, Dias C, Pereira H, et al. A comparative study between two central veins for the introduction of totally implantable venous access devices in 1201 cancer patients. Eur J Surg Oncol. 2008;34:222–6.
Gebauer B, El-Sheik M, Vogt M, Wagner HJ. Combined ultrasound and fluoroscopy guided port catheter implantation—high success and low complication rate. Eur J Radiol. 2009;69:517–22.
Vandoni RE, Guerra A, Sanna P, Bogen M, Cavalli F, Gertsch P. Randomised comparison of complications from three different permanent central venous access systems. Swiss Med Wkly. 2009;139:313–6.
Bobin JY. Implantable chambers for intravenous cytotoxic chemotherapy. Experience of 9 anticancer centers. Presse Med. 1986;15:911–4.
Fraioli JP, Schwarzenberg L. Implantable direct intravenous access: technic, complications, outcome. Apropos of 237 cases. J Chir (Paris). 1988;125:638–41.
Harvey WH, Pick TE, Reed K, Solenberger RI. A prospective evaluation of the Port-A-Cath implantable venous access system in chronically ill adults and children. Surg Gynecol Obstet. 1989;169:495–500.
Comandella MG, Rossi M, Finco C, Pittoni G, Pianalto S, Cadamuro MC, et al. The use of totally implantable systems (TIS) for long-term endovenous therapy. G Chir. 1993;14:185–9.
Tazzioli G, Roncaglia G. Impiego dei sitemi venosi totalmente impiantabili nelle terapie infusive di lunga durata. Chir. 1995;8:93–5.
Di Giorgio A, Bargrazi C, Canavese A, Arnone P, Barberio Corsetti F, et al. Sistemi totalmente impiantabili in oncologia: la vena cefalica come via d’accesso di elezione. Ann Ital Chir. 1997;68:529–37.
Kariyawasam HH, Pepper JR, Hodson ME, Geddes DM. Experience of totally implantable venous access devices (TIV ADs) in adults with cystic fibrosis over a 13-year period. Respir Med. 2000;94:1161–5.
Stas M, Mulier S, Pattyn P, Vijgen J, De Wever I. Peroperative intravasal electrographic control of catheter tip position in access ports placed by venous cut-down technique. Eur J Surg Oncol. 2001;27:316–20.
Johansson E, Björkholm M, Björvell H, Hast R, Takolander R, Olofsson P, et al. Totally implantable subcutaneous port system versus central venous catheter placed before induction chemotherapy in patients with acute leukaemia—a randomized study. Support Care Cancer. 2004;12:99–105.
Marcy PY, Magné N, Castadot P, Bailet C, Macchiavello JC, Namer M, et al. Radiological and surgical placement of port devices: a 4-year institutional analysis of procedure performance, quality of life and cost in breast cancer patients. Breast Cancer Res Treat. 2005;92:61–7.
Di Carlo I, Barbagallo F, Toro A, Sofia M, Lombardo R, Cordio S. External jugular vein cutdown approach, as a useful alternative, supports the choice of the cephalic vein for totally implantable access device placement. Ann Surg Oncol. 2005;12:570–3.
Bruni R, Bartolucci R, Chirco L. I sistemi d’accesso venoso totalmente impiantabili. Chir. 1996;9:146–9.
D’Angelo FA, Ramacciato G, Aurello P, Lauro S, Caramitti A, Lalle M, et al. Alternative insertion sites for permanent central venous access devices. Eur J Surg Oncol. 1997;23:547–9.
Kock HJ, Pietsch M, Krause U, Wilke H, Eigler FW. Implantable vascular access systems: experience in 1500 patients with totally implanted central venous port systems. World J Surg. 1998;22:12–16.
Sarzo G, Finco C, Parise P, Savastano S, Portale G, Vecchiato M, et al. Immediate and long-term complication of prolonged venous access device (PVAD): a comparison between surgical cutdown and percutaneous techniques. Int J Angiol. 2004;13:203–9.
Wolosker N, Yazbek G, Nishinari K, Malavolta LC, Minia MA, Langer M, et al. Totally implantable venous catheters for chemotherapy: experience in 500 patients. Sao Paulo Med J. 2004;122:147–51.
Povoski SP. External jugular vein cutdown approach for chronic indwelling central venous access in cancer patients: a potentially useful alternative. World J Surg Oncol. 2004;2:7.
Chang HM, Hsieh CB, Hsieh HF, Chen TW, Chen CJ, Chan DC, Yet al. An alternative technique for totally implantable central venous access devices. A retrospective study of 1311 cases. Eur J Surg Oncol. 2006;32:90–3.
Seiler CM, Frohlich BE, Dorsam UJ, Kienle P, Buchler MW, Knaebel HP. Surgical technique for totally implantable access ports (TIAP) needs improvement: a multivariate analysis of 400 patients. J Surg Oncol. 2006;93:24–9.
Jablon LK, Ugolini KR, Nahmias NC. Cephalic vein cut-down verses percutaneous access: a retrospective study of complications of implantable venous access devices. Am J Surg. 2006;192:63–7.
Chen PT, Sung CS, Wang CC, Chan KH, Chang WK, Hsu WH. Experience of anesthesiologists with percutaneous nonangiographic venous access. J Clin Anesth. 2007;19:609–15.
Broviac JW, Cole JJ, Scribner BH. A silicone rubber atrial catheter for prolonged parenteral alimentation. Surg Gynecol Obstet. 1973;136:602–6.
Hall P, Cedermark B, Swedendorg J. Implantable catheter system for long-term intravenous chemotherapy. J Surg Oncol. 1989;41:39–41.
Grannan KJ, Taylor PH. Early and late complications of totally implantable venous access devices. J Surg Oncol. 1990;44:52–4.
Mansfield PF, Hohn DC, Fornage BD, Gregurich MA, Ota DM. Complications and failures of subclavian-vein catheterization. N Engl J Med. 1994;331:1735–8.
Biffi R, Pozzi S, Cenciarelli S, Zambelli M, Andreoni B. Treatment of pneumothorax as a complication of long-term central venous port placement in oncology patients. An observational study. J Vasc Access. 2001;2:129–36.
Biffi R, de Braud F, Orsi F, Possi S, Mauri S, Golhirsch A, et al. Totally implantable central venous access ports for long-term chemotherapy. Ann Oncol. 1998;9:767–73.
Nicholson T, Ettles D, Robinson G. Managing inadvertent arterial catheterization during central venous access procedures. Cardiovasc Intervent Radiol. 2004;27:21–5.
Bernard RW, Stahl WM. Subclavian vein catheterizations: a prospective study. I. Non-infectious complications. Ann Surg. 1971;173:184–90.
Povoski SP. A prospective analysis of the cephalic vein cutdown approach for chronic indwelling central venous access in 100 consecutive cancer patients. Ann Surg Oncol. 2000;7:496–502.
Brothers TE, Von Moll LK, Niederhuber JE, Roberts JA, Walker-Andrews S, Ensminger WD. Experience with subcutaneous infusion ports in three hundred patients. Surg Gynecol Obstet. 1988;166:295–301.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Di Carlo, I., Pulvirenti, E., Mannino, M. et al. Increased Use of Percutaneous Technique for Totally Implantable Venous Access Devices. Is It Real Progress? A 27-Year Comprehensive Review on Early Complications. Ann Surg Oncol 17, 1649–1656 (2010). https://doi.org/10.1245/s10434-010-1005-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-010-1005-4