Article Text

Abstract
Background: The clinical benefits of domiciliary non-invasive positive pressure ventilation (NIV) have not been established in cystic fibrosis (CF). We studied the effects of nocturnal NIV on quality of life (QoL), functional and physiological outcomes in CF subjects with awake hypercapnia (arterial carbon dioxide pressure Paco2>45 mm Hg).
Methods: In a randomised, placebo controlled, crossover study, eight subjects with CF, mean (SD) age 37 (8) years, body mass index 21.1 (2.6) kg/m2, forced expiratory volume in 1 s 35 (8)% predicted and Paco2 52 (4) mm Hg received 6 weeks of nocturnal (1) air (placebo), (2) oxygen and (3) NIV. The primary outcome measures were CF specific QoL, daytime sleepiness and exertional dyspnoea. Secondary outcome measures were awake and asleep gas exchange, sleep architecture, lung function and peak exercise capacity.
Results: Compared with air, NIV improved the chest symptom score in the CF QoL Questionnaire (mean difference 10; 95% CI 5 to 16; p = 0.002) and the transitional dyspnoea index score (mean difference 3.1; 95% CI 1.2–5.0; p = 0.01). It reduced maximum nocturnal pressure of transcutaneous CO2 (Ptcco2 mean difference −17 mm Hg; 95% CI −7 to −28 mm Hg; p = 0.005) and increased exercise performance on the Modified Shuttle Test (mean difference 83 m; 95% CI 21 to 144 m; p = 0.02). NIV did not improve sleep architecture, lung function or awake Paco2.
Conclusion: 6 weeks of nocturnal NIV improves chest symptoms, exertional dyspnoea, nocturnal hypoventilation and peak exercise capacity in adult patients with stable CF with awake hypercapnia. Further studies are required to determine whether or not NIV can improve survival.
Statistics from Altmetric.com
Cystic fibrosis (CF) is characterised by a progressive decline in lung function resulting in impaired quality of life (QoL).1 Severe lung disease impairs gas exchange and increases work of breathing while awake2 and particularly during sleep.3–5 Improvements in nocturnal gas exchange and work of breathing could translate into better clinical outcomes and QoL.
Nocturnal non-invasive bi-level positive pressure ventilation (NIV) is beneficial for stable daytime hypercapnia due to kyphoscoliosis, neuromuscular disease and chronic obstructive pulmonary disease (COPD).6 Studies utilising NIV in CF have demonstrated improved gas exchange and reduced work of breathing during a single overnight session,3 4 and improved oxygenation during physiotherapy.5 7 Uncontrolled non-randomised studies suggest that NIV may bridge hypercapnic CF patients to lung transplantation.8–10 Potential complications of NIV include sleep fragmentation and drying of secretions with decreased sputum clearance. A recent Cochrane review highlighted the need for randomised controlled trials to assess the clinical effects of NIV in CF.11
We hypothesised that nocturnal NIV would improve QoL, functional and physiological outcomes in subjects with stable CF with impaired nocturnal gas exchange and daytime hypercapnia. Our aim was to perform a randomised placebo controlled trial of nocturnal NIV in these “at risk” subjects with CF to assess the effects on QoL, and functional and physiological outcomes. Some of the results of these studies have been reported previously in the form of an abstract.12
METHODS
Subjects
Written informed consent was obtained after study approval by The Alfred Hospital Institutional Ethics Committee. Patients were recruited from a cross sectional study12 of 60 consecutive adult CF outpatients with mild to severe lung disease (forced expiratory volume in 1 s (FEV1) <70% predicted) who attended The Alfred Hospital CF Service. Inclusion criteria for the current study were: FEV1 ⩽70% predicted, clinical stability (no hospitalisation or new antibiotics 2 weeks prior), positive screening overnight oximetry (Spo2 <90% for ⩾5% of the night), impaired gas exchange on polysomnography (Spo2 <90% for ⩾5% of total sleep time and/or rise in pressure of transcutaneous CO2 (Ptcco2) ⩾5 mm Hg non-rapid eye movement (NREM) to rapid eye movement (REM) sleep) and awake hypercapnia (Paco2 >45 mm Hg). Exclusion criteria were: previous domiciliary oxygen (O2) or NIV, current sedative use, cardiac or neurological disease and obstructive sleep apnoea.
Study design
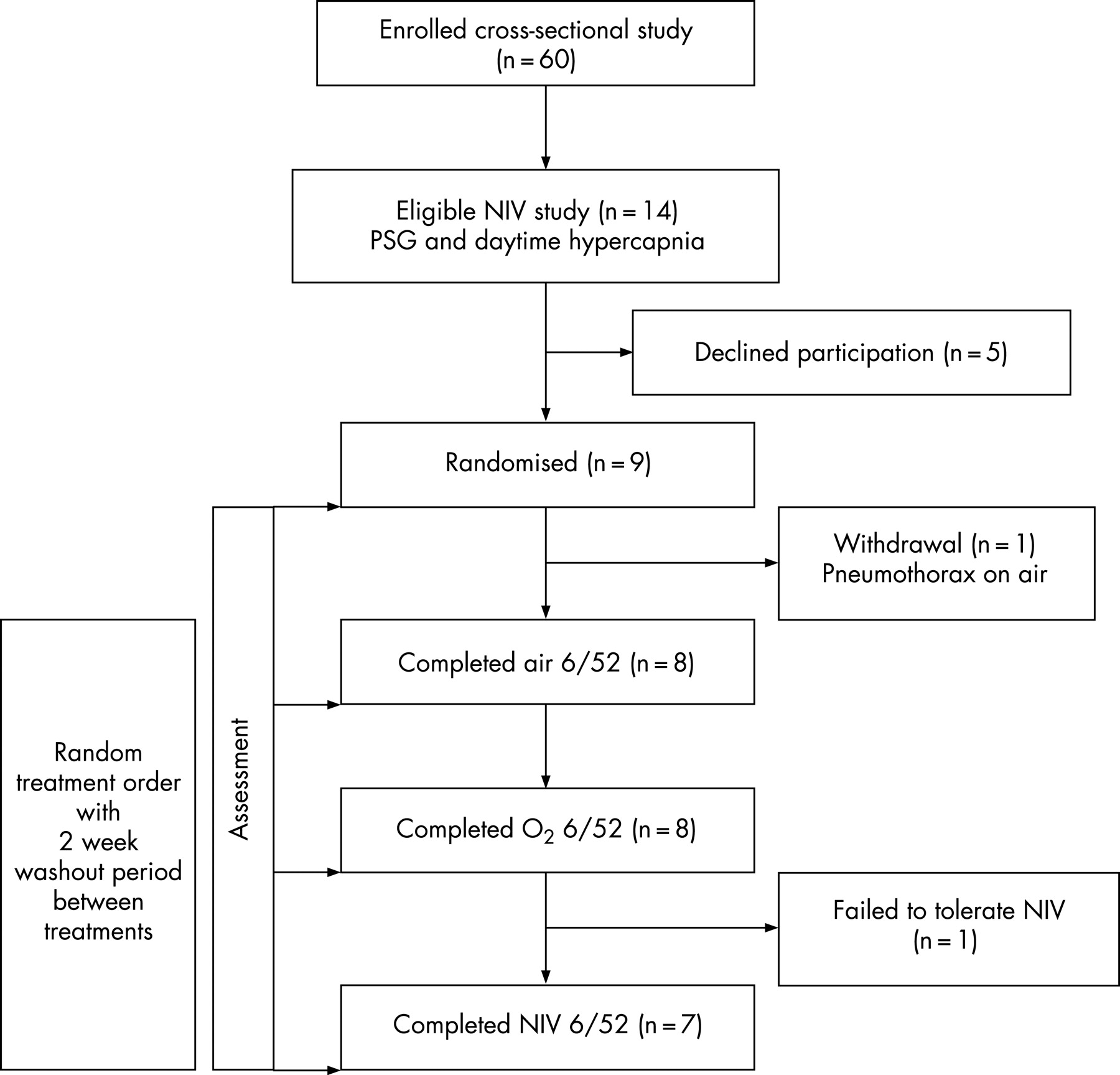
The trial design was randomised placebo controlled crossover. Each subject received 6 weeks of nocturnal (1) air (placebo), (2) O2 and (3) NIV in random order separated by a 2 week washout period. Data were collected at baseline and at the end of each treatment period (fig 1). Treatments were commenced, and post-treatment assessments were carried out during a period of clinical stability (defined as no current need for hospitalisation or intravenous antibiotics).

{kind=link}
Interventions
NIV (BiPAP Synchrony S/T; Respironics, Pennsylvania, USA) with humidification (HC 150; Fisher and Paykel, Laguna Hills, California, USA) was delivered via nasal or full face mask fitted to patient comfort. Acclimatisation involved an afternoon session of several hours with an experienced respiratory therapist and sleep physician to optimise mask fit and ensure patients could tolerate therapy. Polysomnography (PSG) was used to titrate NIV settings thus: inspiratory positive airway pressure (IPAP) was increased in 2 cm H2O increments to attenuate any rise in Ptcco2 ⩾5 mm Hg from NREM to REM sleep, expiratory positive airway pressure was increased in 1 cm H2O increments to eliminate any obstructive events, a backup rate was added if the patient failed to trigger the ventilator. Oxygen therapy was not added to NIV as the hypothesis being tested was that NIV alone would improve outcomes.
The 6 weeks of O2 therapy was delivered from an O2 concentrator (Elite; AirSep, New York, USA) via nasal cannulae. At commencement, therapy was titrated using overnight oximetry. O2 was increased in 1 l/min increments to maintain Spo2 >90% for the entire night. The 6 weeks of air (placebo) was delivered through a disabled O2 concentrator and the flow rate was increased from 1 to 2 l/min during a sham “titration” session with overnight oximetry. Thus patients remained blinded as to whether they were receiving O2 or air. NIV and concentrator hours of usage for the entire treatment period were recorded.
Primary outcome measures
Validated QoL measures assessed CF specific domains (CF QoL Questionnaire),13 sleepiness (Epworth Sleepiness Scale, Pittsburgh Sleep Quality Index)14 15 and dyspnoea (Medical Research Council Dyspnoea Scale, Baseline and Transitional Dyspnoea Index).16 17 A priori, four domains of the CF QoL were selected (physical functioning, treatment issues, chest symptoms, emotional responses) based on our clinical experience of symptoms that might be expected to improve with nocturnal NIV. The CF Subjective Sleep Disturbance Questionnaire was developed inhouse and assessed six subjective symptoms of sleep disturbance. We have previously reported an association between higher/worse scores and nocturnal hypoxia in the form of an abstract.12 Subjects were asked “which treatment was most comfortable?” and “which treatment would you prefer to continue?” at study end.
Secondary outcome measures
PSG (Compumedics E-series, Abbottsford, Australia) was manually scored, blinded to the patient’s treatment, using standard criteria. Spirometry and lung volumes (Profiler and Elite Series, Medgraphics, Minnesota, USA) meeting American Thoracic Society criteria, awake supine arterial blood gases (model 865; Bayer HealthCare, New York, USA) and the validated Modified Shuttle Test18 were performed.
Neurocognitive testing was performed at the same time of day after abstinence from caffeine and alcohol. The Psychomotor Vigilance Task,19 Stroop Color and Word Test,20 Trail Making Test,21 Controlled Oral Word Association Test22 and Digit Span Test23 were undertaken (see online data supplement for further information regarding subjects, study design, interventions and outcome measures).
Statistics
Results are presented as mean (SD). Analysis was performed using SAS V.8.2 (SAS Institute Inc, North Carolina, USA). Data were analysed as difference from baseline. A repeated measures analysis of variance or Freidman two way analysis of variance assessed differences between treatments, with a two sided p value of 0.05 considered significant. Where a significant difference was identified, the paired t test or Wilcoxon signed rank test was used for post hoc analysis, with a p value of 0.017 considered significant to adjust for multiple comparisons. Assuming an SD of 15 points for the physical function domain of the CF QoL,24 a sample size of 18 subjects was needed to demonstrate a 10 point improvement (clinically important difference)1 in mean score with treatment, with a power of 0.8 and a two sided α of 0.05.
RESULTS
Patient characteristics
Sixty patients were screened during the cross sectional study (lung function, overnight oximetry, arterial blood gases) of whom 14 met the entry criteria for the current study. Nine patients consented to randomisation. There was one withdrawal because of pneumothorax (while on air) and one patient did not tolerate NIV as a result of mask discomfort. Data analysis for the effects of NIV and O2 included the seven and eight patients, respectively, who completed these treatment arms (fig 1).
The group (n = 8) mean age was 37 (8) years with a body mass index (BMI) of 21.1 (2.6) kg/m2 and FEV1 35 (8)% predicted. There was evidence of gas trapping (residual volume/total lung capacity ratio 59 (8)%), chronic hypercapnia (pH 7.39 (0.02), Paco2 52 (4) mm Hg) and moderate hypoxaemia (arterial oxygen pressure (Pao2) 63 (5) mm Hg). Compared with patients who were randomised, the five patients declining participation had similar FEV1 (27 (9)% predicted), BMI (18.0 (2.9) kg/m2) and Pao2 (60 (5) mm Hg). However, they were younger (24 (5) years) with a milder degree of chronic hypercapnia (Paco2 47 (4) mm Hg) (table 1).
Treatment settings and compliance
Air was delivered at a flow rate of 2 l/min (as per the protocol) with mean usage 7.2 (2) h/night. Oxygen was delivered at a flow rate of 1.3 (0.5) l/min with mean usage 6.5 (3) h/night. Seven of eight patients tolerated NIV (87.5%). Mean IPAP was 12 (1) cm H2O, expiratory positive airway pressure 5 (0.4) cm H2O and backup rate 14 (3) breaths/min. Mean NIV usage was 4.3 (2.7) h/night.
Quality of Life questionnaires
NIV significantly increased the chest symptom score in the CF QoL (mean difference 10; 95% CI 5 to 16; p = 0.002) and the Transition Dyspnoea Index (TDI) total score (mean difference 3.1; 95% CI 1.2–5.0; p = 0.01) compared with air. Six of seven patients who tolerated NIV increased their chest symptom score by ⩾5 points (range 5–20) compared with air, and five patients increased their TDI by ⩾2 points (range 2–9). There were no significant changes in these parameters with air or supplemental O2. There were no changes with any therapeutic manoeuvre in the other QOL measures (CF Subjective Sleep Disturbance Questionnaire, Epworth Sleepiness Scale, Pittsburgh Sleep Quality Index, Medical Research Council Dyspnoea Scale) (table 2).
Comfort, preference
Four patients rated O2 the most comfortable while two rated O2 and air equally comfortable. Only one patient rated NIV as the most comfortable. Four patients preferred O2 as long term therapy while three patients preferred NIV. No patients selected air as their preferred long term therapy.
Polysomnography, arterial blood gases, lung function, exercise testing
At baseline, sleep efficiency (86 (6)%), sleep latency (20 (23) min) and distribution of sleep stages were normal (table 3). However, there was significant nocturnal hypoxia (38 (43)% total sleep time with Spo2 <90%), hypercapnia (mean Ptcco2 58 (3) mm Hg, maximum Ptcco2 68 (12) mm Hg), tachypnoea (mean respiratory rate during slow wave sleep 23 (6) breaths/min) and tachycardia (mean heart rate 78 (15) beats/min) (table 4).
Air had no significant effect on any PSG parameter, awake arterial blood gas measurements, lung function or exercise performance. Similarly, supplemental O2 had no significant effect on sleep architecture, awake arterial blood gas, lung function or exercise performance. However, during sleep there was a trend for supplemental O2 to increase mean Spo2 (mean difference 4.6%; 95% CI 0.9 to 8.3%; p = 0.03) and cause a rise in Paco2 overnight (mean difference 4.1 mm Hg; 95% CI 0.1 to 8 mm Hg; p = 0.07), compared with air. There was no significant change in Ptcco2 with O2 therapy. NIV had no significant effect on sleep architecture, awake arterial blood gas measurements or lung function. NIV increased mean Spo2 (mean difference 3%; 95% CI 0.7 to 6.7%; p = 0.13) by a similar degree as supplemental O2 but this did not reach statistical significance. NIV produced a significant reduction in maximum Ptcco2 (mean difference −17 mm Hg; 95% CI −7 to −28 mm Hg; p = 0.005), attenuated the rise in Ptcco2 from NREM to REM sleep (mean difference −2.4 mm Hg; 95% CI −0.6 to −4.2 mm Hg; p = 0.017) and trended towards a reduction in mean nocturnal heart rate (mean difference −6.6 beats/min; 95% CI 0.5 to 12.6 beats/min; p = 0.05) compared with air. NIV also reduced maximum Ptcco2 (mean difference −15 mm Hg; 95% CI −4 to −25 mm Hg; p = 0.015), decreased the rise in Ptcco2 from NREM to REM sleep (mean difference −3.1 mm Hg; 95% CI −1.2 to −4.9 mm Hg; p = 0.006) and attenuated the rise in Paco2 overnight (mean difference −8 mm Hg; 95% CI −4 to −12 mm Hg; p = 0.003) compared with O2 (tables 4, 5). Furthermore, NIV produced a significant increase in shuttle distance (mean difference 83 m; 95% CI 21 to 144 m; p = 0.016) compared with air (table 5). Six of seven patients who tolerated NIV increased their shuttle distance by ⩾50 m (range 50–160) compared with air.
Neurocognitive testing
There were no significant changes in neurocognitive function with any intervention (see online data supplement for further details).
Adverse effects
There were no significant side effects with air or O2 therapy. One patient developed a spontaneous pneumothorax while on air which was considered to be coincidental. Two patients complained of aerophagia with NIV which resolved with a reduction in IPAP by 2 cm H2O. There was no significant skin breakdown related to mask usage. No patients reported any worsening of mucus plugging or drying of secretions with NIV.
DISCUSSION
This is the first randomised placebo controlled trial of domiciliary NIV in CF subjects with hypercapnia. The results of this study indicate that 6 weeks of nocturnal NIV improves nocturnal hypoventilation, chest symptoms, exertional dyspnoea and peak exercise capacity, compared with placebo.
Our findings are consistent with published NIV data in CF on several levels. Our NIV tolerance rate of 87.5% (seven out of eight patients) was similar to the 62–83% seen in medium term observational NIV studies 25 26 in CF. Our ventilator measured compliance was 4.3 h per night. Attenuation of the rise in Ptcco2 with NIV and worsening of Paco2 with O2 therapy has been reported in single overnight sessions in CF.3 4 A meaningful improvement in dyspnoea score was reported in three of eight subjects during a 2 month trial with NIV.26 We demonstrated an increase in TDI of 3.1 units with NIV compared with placebo, which exceeds the minimally important clinical difference of 1 unit for this test.27 Five of seven subjects (71%) improved their TDI by a margin of ⩾2 points demonstrating that the majority of subjects experienced a significant improvement.
We were unable to demonstrate a fall in awake hypercapnia with NIV, despite a sustained reduction in nocturnal CO2 levels. Uncontrolled studies of NIV in CF have shown a reduction in daytime Paco2,25 but results have been conflicting.26 Our results may be due to a type II error, low levels of IPAP or a short treatment period with mild baseline hypercapnia. Patients underwent rigorous in-lab titration of IPAP and checking for mask leaks. Aerophagia was seen in two patients, indicating that higher pressures were not likely to be tolerated. Our protocol duration of 5 months was chosen to maximise recruitment, minimise dropouts as a result of lung transplantation and decrease baseline fluctuations which can weaken a crossover study.
This is the first study to demonstrate an improvement in exercise performance using nocturnal NIV in CF. Compared with placebo, NIV increased mean shuttle distance by 83 m, which exceeds the 40 m cut-off representative of a significant improvement in exercise performance.28 Six of seven subjects (86%) improved their shuttle distance by ⩾50 m which is considerable given this is an incremental test. It is important to note that some of this difference was explained by a fall in exercise capacity while on placebo, as the absolute increase in mean shuttle distance from baseline with NIV was 25 m. A possible explanation is that NIV prevented the deterioration in exercise capacity seen with placebo. However, this hypothesis requires further study before any firm conclusions can be drawn.
Exercise performance with NIV has rarely undergone objective assessment in previous studies. Improvements in dyspnoea and exercise performance have been observed in COPD with the application of nocturnal, daytime and exercise NIV.29–31 In CF, improved muscle strength and oxygenation during chest physiotherapy has been achieved with the addition of inspiratory pressure support.7 The mechanism is likely to relate to improved gas exchange due to a reduction in the work of breathing. In CF patients with severe lung disease, NIV reduces diaphragmatic work while awake32 33 and improves alveolar ventilation while asleep.4 We postulate that unloading of the respiratory muscles overnight leads to the improved exercise capacity during the day. However, this concept requires further investigation. We found no improvement in lung function or nutritional status to account for these improvements. However, measurement of exercise flow volume loops and inspiratory capacity could further assess changes in lung mechanics. The importance of this finding cannot be underestimated as peak exercise capacity is an independent predictor of survival in both adults and children with CF.34 35
There was a strong trend towards a fall in mean nocturnal heart rate with NIV suggesting improved sympathovagal balance during sleep. A reduction in tachycardia is used clinically as a measure of success with NIV during acute exacerbations of COPD. Whether heart rate could be used as a marker of nocturnal work of breathing in CF remains untested.
The main strengths of this study were the inclusion of a placebo arm, random allocation of treatment order, the crossover design and objective assessment of treatment adherence. The crossover design increased the power of the study and matched baseline characteristics, which are major difficulties associated with clinical trials in CF. Nevertheless, the sample size limits further interpretation of our study and introduces the possibility of type II errors (ie, erroneously concluding no difference exists when one really does). In this context, our positive results are encouraging, given we corrected for multiple comparisons in statistical analysis to minimise type I errors (ie, erroneously concluding a difference when none exists). In addition, there was little more that could be done to increase recruitment. We are a large adult centre with 250 patients and we screened a significant proportion of our population. Most patients who declined participation cited time constraints and unwillingness to undergo multiple sleep studies and arterial blood gas measurements. This highlights the difficulty of powering studies with invasive and time consuming outcome measures in CF patients with advanced disease. Our study is of comparable size to published uncontrolled studies of NIV in CF.9 10 25 26
A potential weakness of the crossover design is a change in baseline characteristics over the study period due to deteriorating health, exacerbations or carry over effects from treatment. Ideally, reassessment (eg, QoL questionnaires, lung function testing) at the start of each treatment period could have been performed but, as alluded to previously, would have been extremely onerous for patients already undertaking multiple investigations. We attempted to address these issues by ensuring clinical stability at the start and end of each treatment period and incorporating a 2 week washout period in the study design. The absence of change in lung function with any treatment argues against pulmonary exacerbations being the explanation for the observed differences. However, we cannot be certain that some of the observed changes were not due to changes in underlying disease status or carry over effects from treatment.
In conclusion, we have shown that 6 weeks of nocturnal NIV can significantly improve nocturnal hypoventilation, chest symptoms, exertional dyspnoea and peak exercise capacity in CF subjects with daytime hypercapnia. However, there is a need for larger multicentre trials to further extend these findings, clarify which subgroups may benefit most and, in particular, determine whether NIV can improve survival.
Acknowledgments
The authors would like to thank all subjects for their participation. We are also grateful to the staff of the sleep unit, cystic fibrosis unit and lung function laboratory at the Alfred Hospital for their assistance. In particular, Teanau Roebuck, Sally Ho, Seymone Doyle, Pavlina Toman, Catherine Buchan, Jo Toghill, Felicity Finlayson, Bruce Thompson and Brigitte Borg. We thank Michael Bailey and Rory Wolf for their assistance with statistical analysis.
REFERENCES
Supplementary materials
web only appendix 63/1/72
Files in this Data Supplement:
Footnotes
Funding: ACY was supported by scholarships from the National Health and Medical Research Council of Australia, Monash University and The Australian Cystic Fibrosis Research Trust.
Competing interests: None.