Article Text

Statistics from Altmetric.com
Physical activity (PA) is well documented to improve health. However, this documentation is restricted to leisure time physical activity (LTPA; eg, sports, recreation and transportation). Increasing evidence shows that occupational physical activity (OPA) does not improve health.1 Actually, OPA can be detrimental. These contrasting health effects of LTPA and OPA constitute the so-called PA health paradox.2
For a considerable fraction of the adult population, work constitutes the main setting for PA. Workers in many occupations, such as construction, cleaning, refuse collection, elderly care, farming and manufacturing, are physically active for large parts of their working days, for most of the year. Despite this PA at work, these and other manual workers have relatively poor health.
Many epidemiological studies document that high OPA increases the risk for cardiovascular disease (CVD) and mortality outcomes, even after extensive adjustments for other risk factors including socioeconomic status, LTPA and other health behaviours.1 This increased risk from high OPA has been shown to be particularly pronounced among workers with low job resources, low cardiorespiratory fitness3 or pre-existing atherosclerosis, hypertension and coronary heart disease.4 Moreover, if workers with existing cardiovascular conditions and high OPA ought to be recommended to perform high LTPA is debated.
For the development of effective interventions, it is necessary to determine the mechanisms behind the PA health paradox. Different typical characteristics of OPA and LTPA may play a role. LTPA often includes dynamic movements at conditioning intensity levels sufficient to improve cardiorespiratory fitness and metabolism and is mostly performed voluntarily over short time periods with enough recovery time. In contrast, work often requires static loading, heavy lifting, monotonous and awkward working postures and other non-conditioning OPA performed over long periods with insufficient recovery time.2 Specifically, we propose the following hypotheses for potential underlying mechanisms for the PA health paradox:
OPA is of too low intensity or too long duration for maintaining or improving cardiorespiratory fitness and cardiovascular health
Improvement of cardiorespiratory fitness requires a high intensity of PA (>60%–80% of maximal aerobic capacity) for short periods of time. However, average OPA intensities over an 8-hour working day exceeding recommended levels for these longer periods (>30%–35% of maximal aerobic capacity) may actually impair cardiovascular health.5
OPA elevates 24-hour heart rate
Heart rate is elevated during and subsequent to performing PA. High OPA over long time periods increases 24-hour heart rate, while high LTPA over short time periods does not. Prolonged elevated heart rate is an independent risk factor for CVD and mortality.6
OPA including heavy lifting or static postures elevates 24-hour blood pressure
Muscle contractions during manual material handling and prolonged static working postures instantaneously elevate blood pressure. Prolonged exposure to static OPA may cause sustained elevated blood pressure, even after working hours. Sustained elevated blood pressure is an important CVD risk factor. LTPA might also involve heavy lifting, but normally during shorter time periods and under controlled conditions, not increasing 24-hour blood pressure.
OPA is often performed without sufficient recovery time
Long periods of PA without sufficient recovery (eg, long weekly working hours, extreme endurance training) can cause fatigue and exhaustion and may increase CVD risk.7 In sports medicine, this would be considered overtraining. In many occupations, however, work requires being physically active for 7–12 hours per day, for several consecutive days, with limited frequency and duration of rest periods within and between working days.
OPA is often performed with low worker control
Limited control over work tasks, speed, schedule, protective clothing, psychosocial stressors and the surrounding environment may contribute to the detrimental effects of OPA. For example, about 50% of the global working population works outdoors with little control over climate, shade, hydration and access to rest, leading to increased heat stress, risk of fatal heat stroke and CVD. In contrast, LTPA can be performed under safer self-regulated conditions. Lack of worker control over OPA can lead to overexhaustion, which may explain the particularly increased risk in such vulnerable groups.
OPA increases levels of inflammation
Markers of inflammation (eg, C reactive protein) increase during PA and remain elevated until the body has recovered.8 High OPA over long time periods over consecutive days without sufficient recovery time can cause sustained inflammation, which is one hypothesised pathway in the aetiology of atherosclerosis and other CVDs.8
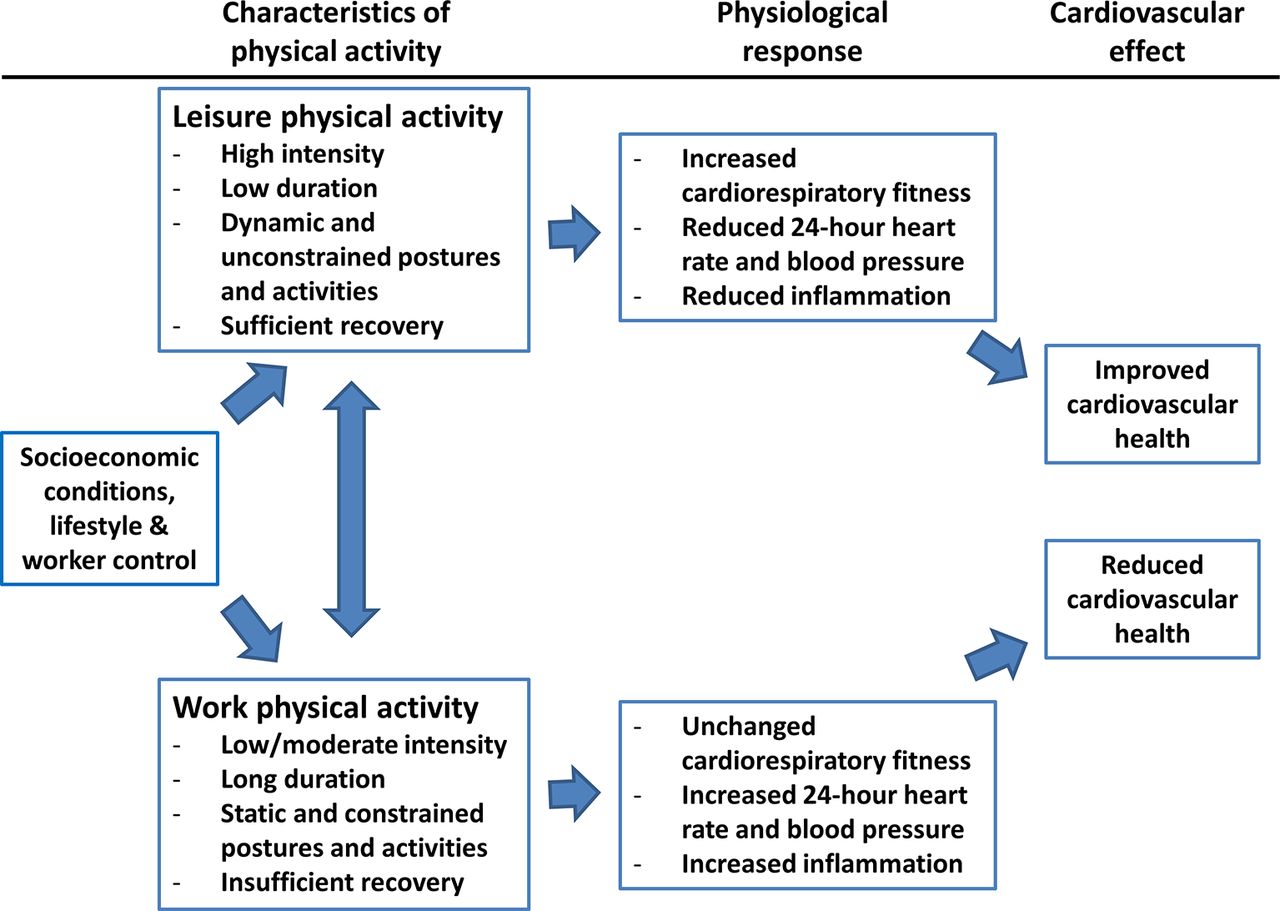
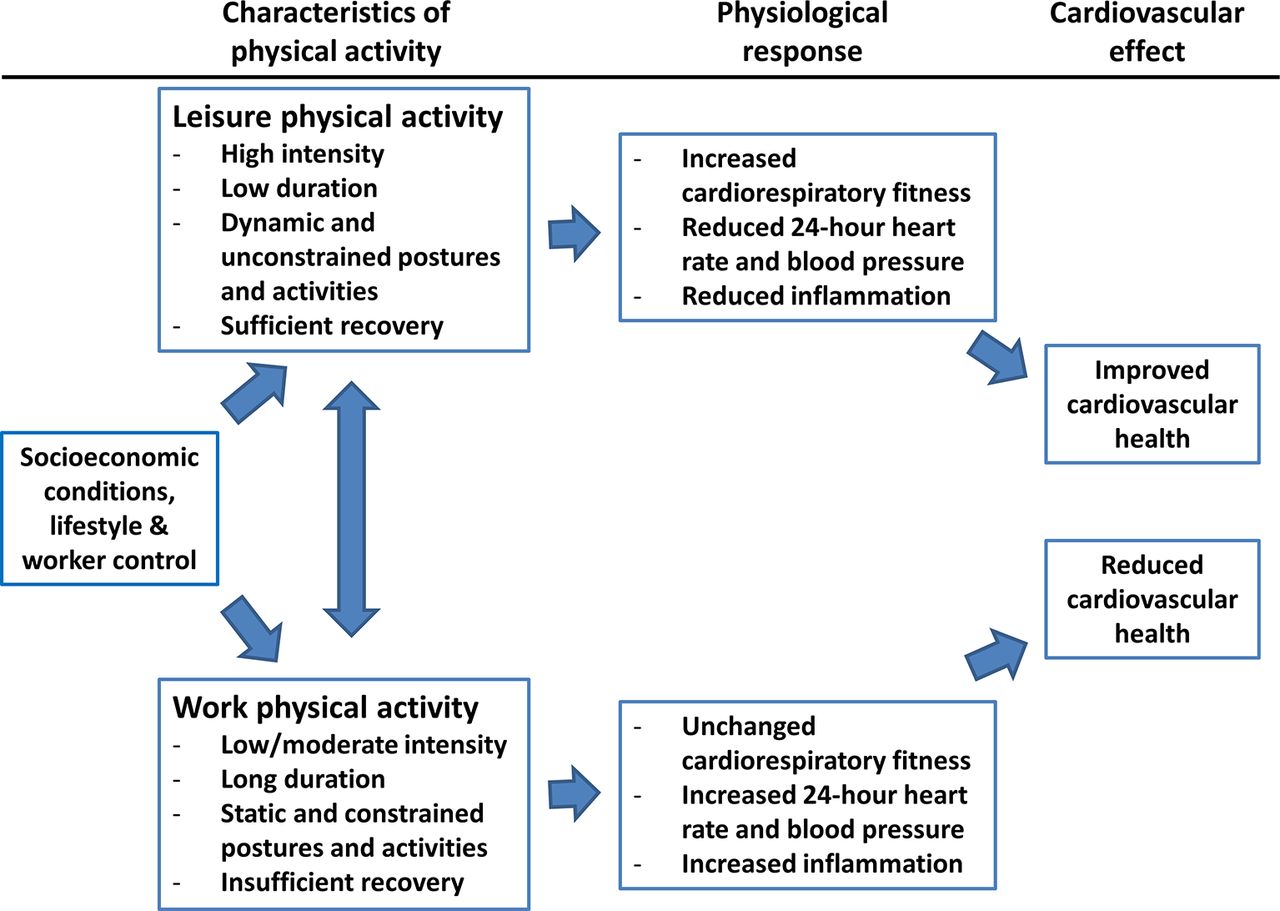
A conceptual diagram of the proposed mechanisms behind the PA health paradox is illustrated in figure 1. Because the majority of workers with high OPA have a low socioeconomic position, improving our understanding of the underlying mechanisms behind the PA health paradox and identifying new intervention targets along those pathways will be an important step to reduce socioeconomic health inequalities across the globe.
{kind=link}
Conceptual diagram of the proposed mechanisms behind the physical activity health paradox.
Acknowledgments
None
Footnotes
Contributors All authors contributed to the development of the idea, the conceptualization, the writing and haveaccepted the final version of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.