




Summary
Leiomyoma is the most common benign tumor of the esophagus, and usually occurs as a solitary mass. We report a case of esophageal leiomyoma which shows multinodular growth pattern with bulbous serosal protrusions. The patient was a 26-year-old woman who had an esophageal ulcerated mass near the gastroesophageal junction. Clinical findings were consistent with carcinoma of the gastric cardia. Based on the clinical diagnosis, total gastrectomy with distal esophagectomy was performed. Histologic appearance of the resected specimen was consistent with leiomyoma which had a multinodular growth pattern.
Introduction
Unusual growth patterns have been usually described in benign smooth muscle tumors of uterus, such as diffuse uterine leiomyomatosis, dissecting leiomyoma, intravenous leiomyomatosis, cotyledonoid leiomyoma, and plexiform leiomyoma.1–3 Some of these unusual growth patterns have also been very rarely described in other locations.4,5
In the esophagus, diffuse leiomyomatosis has been reported occasionally6 and only two cases of plexiform leiomyoma have been reported as having an unusual growth pattern.7
We describe an esophageal leiomyoma which showed multinodular pattern with internodular hydropic degeneration and extraesophageal bulbous growth in continuity with the intramural component.
Case Report
A 26-year-old woman had a history of dysphagia and dyspepsia. She had mild anemia with a hemoglobin level of 11.5 g/dL and an elevated erythrocyte sedimentation rate of 81 mm/h. Upper gastrointestinal endoscopy revealed an ulcerated bulging mass at the gastroesophageal junction. The computed tomography scan of the lesion was a non-enhancing, homogeneously hypodense, 32 × 40 mm solid mass with ill-defined nodular contours and protruding to the gastric lumen at the gastroesophageal junction (Fig. 1). There were lymph nodes at the gastrohepatic ligament and periaortic space with a maximum size of 15 × 10 mm. Computed tomography scan also revealed a hypodense, undefined liver mass which measured less than 1 cm, and it was considered as either a metastasis or a focal steatosis.

Axial post-contrast CT scan demonstrating an ill-defined, homogeneous hypodense mass (arrows) protruding through the gastric lumen. No prominent contrast enhancement or calcification is detected within the lesion.
Endoscopic biopsy of the lesion showed necrotic exudate and edematous mesenchymal tissue which had benign-looking spindle cells and inflammatory cells. Although these histopathologic findings roused a suspicion of leiomyoma, the clinical findings were compatible with cancer of the gastric cardia. Therefore, the patient was referred to surgery and she underwent total gastrectomy with distal esophagectomy.
Results
Gross findings
On gross inspection, a large ulcerated protruding mass was seen in the right lateral abdominal portion of the esophagus just near the gastroesophageal junction. The mass traversed the esophageal wall and formed multiple nodular protruding masses on the serosal surface (Fig. 2). Numerous lymphadenopathies with a largest diameter of 2 cm were present on the perilesional area and gastric curvatures.

Gross photograph of the specimen. Arrows show large protruding serosal nodules.
Light microscopic findings
Histological examination showed numerous ill-defined tumorous nodules composed of intersecting fascicles of smooth muscle cells. The lesion had internodular edematous connective tissue which included vessels of variable size, lymphocytes, and plasmacytes. There was no evidence of mitosis, cytological atypia or tumoral necrosis (Fig. 3a,b). However, some hypoxic degenerative changes were observed in the center of the serosal protruding nodules. The surface of the intraluminal portion of the lesion had a thick cover which had intensive edema and mixed inflammatory cells admixed with spindle cells. There were thickening, fibrosis, ectatic vessels, and infiltration of lymphocytes and plasmacytes in the submucosal and serosal tissue neighboring the tumoral mass.
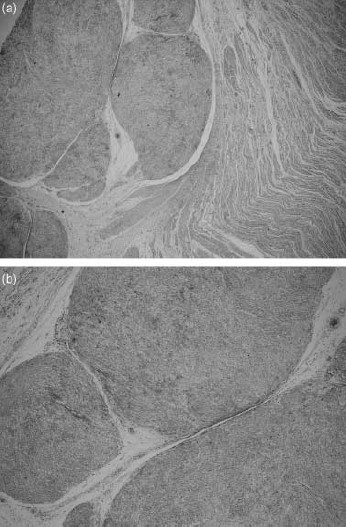
(a) Multiple nodules of neoplastic smooth muscle with internodular hypocellular edematous connective tissue which has some vessels, lymphocytes, and plasmacytes (H&E, ×20). (b) Higher magnification of (a) (H&E, ×100).
Immunohistochemical and histochemical findings
On immunohistochemical study, the tumorous cells were strongly and diffusely positive for desmin (NeoMarkers, California, US: 1 : 100), muscle specific actin (NovoCastra, Newcastle, UK: 1 : 100), and smooth muscle actin (NeoMarkers: 0.5–1 µg/mL). However, CD117 (NeoMarkers: 1 : 100), CD34 (NeoMarkers: 0.5–1 µg/mL), S-100 (NeoMarkers: 1–2 µg/mL), and NSE (NeoMarkers: 0.5–1 µg/mL) were negative. Masson trichrome staining was also compatible with leiomyoma.
Discussion
Cotyledonoid leiomyoma is a very rare variant of uterine leiomyoma, resembling the cotyledons of placenta, and it is characterized by the presence of numerous bulbous protrusions over the uterus.2 Roth and Reed8 reported a multinodular hydropic dissecting leiomyoma which showed edematous bulbous processes distorting the surface of the uterus, but it was not considered as a cotyledonoid leiomyoma because there were no discrete protruding nodules. We describe an esophageal leiomyoma with uncommon growth features of the multinodular hydropic leiomyoma. Our case also had bulbous protrusions on the serosal surface of the esophagus similar to cotyledonoid uterine leiomyoma. There were small ectatic vessels in the hydropic intranodular stroma, but this was not as prominent as in cotyledonoid uterine leiomyoma.
Although leiomyomas with unusual growth patterns have usually been described in the uterus, there are only a limited number of reported cases in the literature. They have been described very rarely in other locations such as the skin and heart.4,5 In the esophagus, leiomyomatosis has been usually described as an unusual growth pattern of the smooth muscle mass lesions.6 The present case may be considered as an esophageal leiomyomatosis. However, leiomyomatosis leads to circumferential thickening of a sizeable portion of the esophagus, which is contrary to our case.9
Only two cases of plexiform leiomyoma have been described among all esophageal leiomyomas.7 These two cases were probably consistent with the usual leiomyoma with a smooth border and were diagnosed as leiomyoma before surgical intervention. In contrast, our case clinically resembled a malignant tumor because of its irregular border, bulbous serosal protrusions, ulceration, and lymphadenopathies. The histopathological, cytological, architectural, histochemical, and immunohistochemical features of the lesion were characteristic for leiomyoma without any atypia and mitosis. The lymphadenopathies, and fibroblastic thickening and edema of peritumoral serosa and submucosa may have been due to the surface ulceration and inflammatory infiltration in our case.
Why have these unusual growth patterns been usually described in the uterus? This might be due to the fact that ordinary leiomyomas are seen very frequently in the uterus. Uterine leiomyomas occur in 20–40% of women over the age of 30 years.1 Therefore, a few leiomyomas with unusual growth patterns among millions of uterine ordinary leiomyomas may be usual. In conclusion, leiomyoma with unusual growth pattern may also be seen in the esophagus and it may be confused with malignancy.

{kind=link}
{kind=link}
{kind=link}