




Abstract
The impact of the prophylactic vaccine against human papillomavirus (HPV) types 6, 11, 16, and 18 (HPV6/11/16/18) on all HPV-associated genital disease was investigated in a population that approximates sexually naive women in that they were “negative to 14 HPV types” and in a mixed population of HPV-exposed and -unexposed women (intention-to-treat group).
This analysis studied 17 622 women aged 15–26 years who were enrolled in one of two randomized, placebo-controlled, efficacy trials for the HPV6/11/16/18 vaccine (first patient on December 28, 2001, and studies completed July 31, 2007). Vaccine or placebo was given at day 1, month 2, and month 6. All women underwent cervicovaginal sampling and Papanicolaou (Pap) testing at day 1 and every 6–12 months thereafter. Outcomes were any cervical intraepithelial neoplasia; any external anogenital and vaginal lesions; Pap test abnormalities; and procedures such as colposcopy and definitive therapy. Absolute rates are expressed as women with endpoint per 100 person-years at risk.
The average follow-up was 3.6 years (maximum of 4.9 years). In the population that was negative to 14 HPV types, vaccination was up to 100% effective in reducing the risk of HPV16/18-related high-grade cervical, vulvar, and vaginal lesions and of HPV6/11-related genital warts. In the intention-to-treat group, vaccination also statistically significantly reduced the risk of any high-grade cervical lesions (19.0% reduction; rate vaccine = 1.43, rate placebo = 1.76, difference = 0.33, 95% confidence interval [CI] = 0.13 to 0.54), vulvar and vaginal lesions (50.7% reduction; rate vaccine = 0.10, rate placebo = 0.20, difference = 0.10, 95% CI = 0.04 to 0.16), genital warts (62.0% reduction; rate vaccine = 0.44, rate placebo = 1.17, difference = 0.72, 95% CI = 0.58 to 0.87), Pap abnormalities (11.3% reduction; rate vaccine = 10.36, rate placebo = 11.68, difference = 1.32, 95% CI = 0.74 to 1.90), and cervical definitive therapy (23.0% reduction; rate vaccine = 1.97, rate placebo = 2.56, difference = 0.59, 95% CI = 0.35 to 0.83), irrespective of causal HPV type.
High-coverage HPV vaccination programs among adolescents and young women may result in a rapid reduction of genital warts, cervical cytological abnormalities, and diagnostic and therapeutic procedures. In the longer term, substantial reductions in the rates of cervical, vulvar, and vaginal cancers may follow.
Prevention of cervical cancer has focused on screening and prophylactic human papillomavirus (HPV) vaccination.
Two randomized, placebo-controlled, efficacy trials for an HPV vaccine provided data. The average follow-up was 3.6 years. All women underwent cervicovaginal sampling and Papanicolaou (Pap) testing. Outcomes were any cervical intraepithelial neoplasia, any external anogenital and vaginal lesions, any Pap test abnormality, and any procedure such as definitive therapy.
In the group representing uninfected women, vaccination was up to 100% effective in reducing the risk of HPV16/18-related high-grade cervical, vulvar, and vaginal lesions and the risk of HPV6/11-related genital warts. In the intention-to-treat group representing the general population, vaccination statistically significantly reduced the risk of any high-grade cervical lesion, vulvar and vaginal lesion, genital wart, Pap abnormality, and definitive therapy, irrespective of causal HPV type.
HPV vaccination of adolescents and young women in the general population may reduce the incidence of genital warts and cervical cytological abnormalities, the associated number of diagnostic and therapeutic procedures performed, and eventually the rates of cervical, vulvar, and vaginal cancers.
Only 14 of the 40 HPV types that infect the genital tract were assessed. The intention-to-treat population was not entirely representative of the general population because at most four sex partners and no past abnormal Pap test or external genital abnormality were required for entry.
From the Editors
Worldwide, cervical cancer is the second most common cancer in women and the second most common cause of death from cancer among women aged 14–44 years (1). One of the greatest advances in cancer research in the last two decades has been the demonstration that infection with certain types of human papillomavirus (HPV) is a necessary cause of cervical cancer (2,3). This discovery has led to great advances in the prevention of this disease on two fronts: 1) primary prevention by the use of prophylactic HPV vaccines (4–10) and 2) prevention by increasing the efficacy of cervical cancer screening (11).
HPV is one of the most common sexually transmitted infections, with one study of 45 362 Dutch women attending primary care clinics showing a peak prevalence of 24% at age 22 years (12). Although most infections will resolve, some infections with high-risk or oncogenic types of HPV will progress to cancers of the cervix, vulva, vagina, anus, penis, oropharynx, and/or oral cavity. Infections with low-risk HPV types 6 and 11 can cause genital warts, abnormal cytology, and recurrent respiratory papillomatosis, and HPV6 and 11 have also been detected in some rare cancers (13).
Multinational phase III trials of a quadrivalent HPV (types 6, 11, 16, and 18) L1 virus–like particle vaccine (referred to as the HPV6/11/16/18 vaccine hereafter) were conducted in the Females United to Unilaterally Reduce Endo/Ectocervical Disease (FUTURE) I and II trials (7,8), which enrolled approximately 17 000 women aged 15–26 years, and in two adolescent trials (14,15), which enrolled 2700 boys and girls aged 9–15 years. The safety data for these four trials have been previously described (16). In these initial reports from the FUTURE I and II trials (7,8), HPV DNA typing was not available for nonvaccine types. Since then, additional DNA typing has been done that includes 10 nonvaccine, high-risk HPV types (HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59). Furthermore, previous reports of the HPV6/11/16/18 vaccine did not assess the impact of vaccination on Papanicolaou (Pap) test abnormalities and procedures such as colposcopy, biopsy examination, and definitive therapy. In this article, we provide end-of-study data on the impact of the HPV6/11/16/18 vaccine on all clinically relative endpoints in a population that approximates prophylactic vaccination of sexually naive women and in a population of HPV-exposed and -unexposed women.
Participants, Materials, and Methods
Study Objectives
The primary objective was to determine whether administration of HPV6/11/16/18 vaccine, compared with placebo, reduced the risk of the following endpoints: 1) cervical intraepithelial neoplasia (CIN) of any grade severity; 2) external anogenital and vaginal lesions (or external genital lesions) of any grade severity; 3) Pap test abnormalities; and 4) procedures such as colposcopy and definitive therapy or excision (including biopsy examination). We measured the vaccine’s impact on endpoints that were associated with HPV6, 11, 16, and 18 specifically and on endpoints irrespective of causal HPV type.
Study Design and Populations
From December 28, 2001, through May 27, 2003, 17 622 women aged 16–26 years, including two women aged 15 years, were enrolled in one of two randomized, double-blind, placebo-controlled trials (FUTURE I and FUTURE II) (7,8). Of the 17 622 enrolled women, 99.9% received at least one dose of vaccine or placebo, 98.4% received at least two doses, and 97.2% received three doses. Baseline demographics for the individual studies (7,8) and the combined studies (17) have been described. Briefly, the baseline characteristics of the study participants were similar between the two studies with respect to age, numbers of sexual partners, prevalence of sexually transmitted infection, and other factors measured, with the exception of the country of enrollment (the FUTURE II trial enrolled more women from Europe). The countries of enrollment for the two studies included Australia, Austria, Brazil, Canada, Colombia, Czech Republic, Denmark, Finland, Germany, Hong Kong, Iceland, Italy, Mexico, New Zealand, Norway, Peru, Poland, Puerto Rico, Russia, Singapore, Sweden, Thailand, the United Kingdom, and the United States (NCT00092521 and NCT00092534).
Both studies were approved by the institutional review boards (ethical review committees) at participating centers, and informed consent was received from all subjects enrolled. The study designs and the results of the primary hypotheses have been described (7,8). The trials recruited women who, at enrollment (ie, day 1), reported having had zero to four sex partners during their lifetime, with the exception of Finland (that enrolled 872 women in the vaccine group and 873 women in the placebo group), which had no such restriction. Women with a history of an abnormal Pap test, a history of genital warts, or detection of genital warts at enrollment were excluded. Neither study included an HPV screening phase. Thus, the trials allowed the enrollment of subjects who had been previously infected with or were currently infected with at least one vaccine HPV type(s) or at least one of the HPV types that infect the anogenital tract.
The trials were designed to be of 4 years in duration. As a result of the high efficacy observed in the FUTURE I and II trials, the independent Data and Safety Monitoring Board of these studies recommended vaccination of women in the placebo group (18,19). The end-of-study data, which are reported in this article, include an average follow-up period of approximately 3.6 years (25th and 75th percentiles = 3.5 and 3.9 years, respectively) and a maximum follow-up of 4.9 years.
Vaccine
The HPV6/11/16/18 vaccine (Gardasil or Silgard; Merck and Co, Inc, Whitehouse Station, NJ) is composed of recombinant L1 major capsid proteins from HPV6 (20 μg per dose), HPV11 (40 μg per dose), HPV16 (40 μg per dose), and HPV18 (20 μg per dose), all produced in Saccharomyces cerevisiae (20). The HPV6/11/16/18 vaccine was formulated with a proprietary amorphous aluminum hydroxyphosphate sulfate adjuvant, which is currently used in other vaccines manufactured by Merck and Co, Inc, that have been distributed globally in more than 300 million doses. In both trials, women were randomly assigned to receive intramuscular injections of HPV6/11/16/18 vaccine or of a visually indistinguishable placebo, at a ratio of one to one, on day 1, month 2, and month 6.
Clinical Follow-up and Endpoints
Subjects returned to the study sites at months 3, 7, 12, 18, 24, 30, 36, and 48 (the end of study visit) in the FUTURE I trial and at months 7, 12, 24, 36, and 48 (the end of study visit) in the FUTURE II trial. Comprehensive anogenital examinations were conducted at each scheduled visit, during which we collected an endo–ectocervical swab (one specimen) and a combined labial–vulvar–perineal swab plus a perianal swab (which were pooled to become a second specimen). Pap cervical cytology was also performed with a ThinPrep kit (Cytyc, Boxborough, MA) during scheduled visits. Cytology specimens were classified by use of the Bethesda System-2001 (21).
During this examination, all genital lesions that the investigator felt were possibly, probably, or definitely HPV related or whose etiology was unknown were subjected to biopsy examination (defined as the excision of tissue and its histological examination). When multiple lesions were suspected to be HPV related, each lesion that was morphologically distinct and/or anatomically distinct was subjected to biopsy examination. Follow-up biopsy specimens were obtained only if new lesions appeared with different morphology and/or at a different location than previous lesions. All biopsy samples, regardless of location, were processed, and adjacent histological sections of each biopsy specimen were first read for clinical management by pathologists at a central laboratory (Diagnostic Cytology Laboratories, Indianapolis, IN) and then read for endpoint determination by a panel of up to four pathologists (including R. Kurman) who were blinded to central laboratory and clinical diagnoses, treatment group, and HPV status.
The following four endpoints were included in the analyses. 1) Cervical lesions (CIN1, CIN2, and CIN3), adenocarcinoma in situ (AIS), and/or cervical cancer: Protocol-specified guidelines were used to triage subjects with Pap abnormalities and to send them for examination by colposcopy (7,8). Colposcopists were trained to locate and obtain biopsy specimens from all discrete abnormal areas on the cervix. Subjects with CIN2–3 or worse or persistent CIN1, were referred for definitive therapy. 2) External anogenital or vaginal lesions: This endpoint included genital warts, vulvar intraepithelial neoplasia 1–3 (VIN1–3), vaginal intraepithelial neoplasia 1-3 (VaIN1–3), and/or vulvovaginal cancer. It should be noted that a modification of the classification of VIN1–3 and VaIN1–3 was proposed in 2004 (22) that the terms VIN1 and VaIN1 be no longer used and that VIN2 and VIN3, respectively, be replaced by “VIN usual type” and “VIN differentiated type.” In this report, however, we have retained the original nomenclature (VIN1, VaIN1, VIN2–3, and VaIN2–3), which was used by the pathology panel during the course of the studies. 3) Pap abnormalities: ThinPrep cytology specimens for Pap testing were collected at each scheduled visit and classified by use of the Bethesda System-2001 (21). Categories of Pap abnormalities included atypical squamous cells of undetermined significance that were high-risk probe positive, low-grade squamous intraepithelial lesion, high-grade squamous intraepithelial lesion, atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion, atypical glandular cells, adenocarcinoma, and squamous cell carcinoma. 4) Procedures: These procedures included colposcopy examinations and all definitive therapy and excisions (including the obtaining of biopsy specimens) performed for cervical lesions and for external genital lesions. Definitive therapy included loop electrosurgical excision procedure, laser conization (if the loop electrosurgical excision procedure was not the standard practice of care), and cold-knife conization. Management of genital warts was at the discretion of the investigator. Treatment of genital warts was performed only after completing all biopsy requirements as specified by the protocols. Treatment for VIN and VaIN was by the standards and practice of each investigational site. All tissue specimens, including those from definitive therapy and excision (including all biopsy specimens), underwent histopathological review by the blinded pathology panel for endpoint determination.
Statistical Methods
Populations.
Unless otherwise indicated, the analyses were based on the combined data from the FUTURE I and II trials. In this report, we conducted the prophylactic analyses in a population that was “negative to 14 HPV types” and thus approximated HPV-naive women (Table 1). This population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had any follow-up after day 1 and, at enrollment, were seronegative (23–25) and negative (20,26,27) for HPV6, 11, 16, and 18 DNA; were negative for DNA from all 10 nonvaccine HPV types for which polymerase chain reaction (PCR) testing was available (ie, HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59); and had a normal Pap test result. It should be noted that this is not a per-protocol analysis and that, because more than 40 HPV types are known to infect the anogenital tract, the negative to 14 HPV types population only approximates HPV-naive women. Protocol violators were included in the analysis. Follow-up for endpoint ascertainment started after day 1.
Analysis populations*
| Population | Criteria | Interpretations |
| Negative to 14 HPV types | Subjects 1) received at least one vaccination; 2) were seronegative and PCR negative at day 1 to the vaccine HPV types (ie, HPV6, 11, 16, and 18), were PCR negative at day 1 to the nonvaccine high-risk HPV types that had available PCR assays (ie, HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59), and had a negative day 1 Pap test result; and 3) had any follow-up visit. | Approximation of a “real-world” population of HPV-naive women. Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
| Endpoint counting began after day 1. | ||
| Intention to treat | Subjects 1) received at least one vaccination and 2) had any follow-up visit. | Approximation of a “real-world” population of sexually active women with an average of two lifetime sex partners. It is important to note that the analysis includes both women who were exposed to HPV and those who were presumably HPV naive. |
| Endpoint counting began after day 1. | Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
| Population | Criteria | Interpretations |
| Negative to 14 HPV types | Subjects 1) received at least one vaccination; 2) were seronegative and PCR negative at day 1 to the vaccine HPV types (ie, HPV6, 11, 16, and 18), were PCR negative at day 1 to the nonvaccine high-risk HPV types that had available PCR assays (ie, HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59), and had a negative day 1 Pap test result; and 3) had any follow-up visit. | Approximation of a “real-world” population of HPV-naive women. Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
| Endpoint counting began after day 1. | ||
| Intention to treat | Subjects 1) received at least one vaccination and 2) had any follow-up visit. | Approximation of a “real-world” population of sexually active women with an average of two lifetime sex partners. It is important to note that the analysis includes both women who were exposed to HPV and those who were presumably HPV naive. |
| Endpoint counting began after day 1. | Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
HPV = human papillomavirus; Pap = Papanicolaou; PCR = polymerase chain reaction.
Analysis populations*
| Population | Criteria | Interpretations |
| Negative to 14 HPV types | Subjects 1) received at least one vaccination; 2) were seronegative and PCR negative at day 1 to the vaccine HPV types (ie, HPV6, 11, 16, and 18), were PCR negative at day 1 to the nonvaccine high-risk HPV types that had available PCR assays (ie, HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59), and had a negative day 1 Pap test result; and 3) had any follow-up visit. | Approximation of a “real-world” population of HPV-naive women. Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
| Endpoint counting began after day 1. | ||
| Intention to treat | Subjects 1) received at least one vaccination and 2) had any follow-up visit. | Approximation of a “real-world” population of sexually active women with an average of two lifetime sex partners. It is important to note that the analysis includes both women who were exposed to HPV and those who were presumably HPV naive. |
| Endpoint counting began after day 1. | Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
| Population | Criteria | Interpretations |
| Negative to 14 HPV types | Subjects 1) received at least one vaccination; 2) were seronegative and PCR negative at day 1 to the vaccine HPV types (ie, HPV6, 11, 16, and 18), were PCR negative at day 1 to the nonvaccine high-risk HPV types that had available PCR assays (ie, HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59), and had a negative day 1 Pap test result; and 3) had any follow-up visit. | Approximation of a “real-world” population of HPV-naive women. Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
| Endpoint counting began after day 1. | ||
| Intention to treat | Subjects 1) received at least one vaccination and 2) had any follow-up visit. | Approximation of a “real-world” population of sexually active women with an average of two lifetime sex partners. It is important to note that the analysis includes both women who were exposed to HPV and those who were presumably HPV naive. |
| Endpoint counting began after day 1. | Used for analyses of 1) disease related to HPV6, 11, 16, and/or 18 and 2) disease caused by any HPV type. |
HPV = human papillomavirus; Pap = Papanicolaou; PCR = polymerase chain reaction.
The second population was an intention-to-treat (ITT) population that approximates the vaccine's impact in sexually active women (Table 1). This mixed population of HPV-exposed and -unexposed women included all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had any follow-up after day 1, regardless of the presence of HPV infection or HPV-related disease at enrollment. Follow-up for endpoint ascertainment started after day 1.
Endpoint Determination.
All tissues from definitive therapy and excisions (including biopsy specimens) were tested with a PCR-based assay (20,26,27) for 14 HPV types, including the four types in the vaccine (ie, HPV6, 11, 16, and 18) and 10 other oncogenic HPV types (HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59). A woman was considered to have developed an endpoint related to HPV6, 11, 16, and/or 18 if the respective vaccine-type DNA was detected in the same lesion that was diagnosed by the pathology panel as CIN, VIN, VaIN, or genital warts. For analyses of all disease irrespective of causal HPV type, a woman was considered to have developed an endpoint of CIN, VIN, VaIN, or genital warts if she had a lesion diagnosed by the pathology panel as CIN, VIN, VaIN, or genital warts without consideration of HPV status.
A Pap test was considered to be related to HPV16 and/or HPV18 if the endo–ectocervical swab collected at the same visit was positive for HPV16 DNA and/or HPV18 DNA. For analyses of the impact of the vaccine on all Pap test abnormalities, Pap tests were defined by use of the Bethesda System-2001, irrespective of the woman's HPV DNA status.
For analyses of the impact of the vaccine on all procedures for CIN or external genital lesions, a woman developed an endpoint if she underwent one or more procedure, irrespective of her HPV DNA status. For each endpoint, a woman is counted only once, although she may have undergone one or more procedures during the trial. For example, a woman who had a treatment for genital warts and definitive therapy for CIN3 would be counted once for any external genital lesion procedure and once for any cervical definitive therapy. A woman who had more than one procedure for the same endpoint (ie, two procedures for genital warts) was counted only once at the date of the first procedure.
In the efficacy analyses in Tables 2 and 3, a woman was counted only once for each endpoint (ie, once in each row), but a woman could have developed more than one endpoint during the trial (ie, a women may appear in more than one row). For example, a woman may have developed two lesions with HPV detected in both: an HPV16-related CIN2 lesion and an HPV6-related CIN1 lesion. Overall, she would be counted once for 1) any CIN1 regardless of causal HPV type; 2) any CIN2 regardless of causal HPV type; 3) CIN1 related to HPV6, 11, 16, and/or 18; 4) CIN2 related to HPV6, 11, 16, and/or 18; 5) CIN2 related to HPV16 and/or 18; 6) CIN2 related to HPV16; and 7) CIN1 related to HPV6 and/or 11. Likewise, a woman who developed an endpoint caused by a vaccine type and a nonvaccine type of HPV, such as a single CIN2 lesion that was positive for both HPV16 and HPV31, would be counted once for 1) any CIN2 or worse regardless of causal HPV type; 2) CIN2 related to HPV6, 11, 16, and/or 18; 3) CIN2 related HPV16 and/or 18; and 4) CIN2 related to HPV16. Therefore, one cannot subtract the number of women with a disease related to HPV6, 11, 16, and/or 18 from the total number of women with that disease to obtain the number caused by a nonvaccine HPV type. Such a subtraction does not account for coinfection with vaccine and nonvaccine HPV types.
Reductions in cervical intraepithelial neoplasia (CIN) and external genital lesions related to human papillomavirus (HPV) 6, 11, 16, and/or 18*
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 3 | <0.1 | 4680 | 136 | 0.8 | 97.8 (93.4 to 99.5) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 34 | 0.2 | 100 (88.4 to 100) |
| HPV16 and/or 18 | 4616 | 3 | <0.1 | 4680 | 107 | 0.6 | 97.2 (91.5 to 99.4) |
| HPV16 | 4616 | 3 | <0.1 | 4680 | 89 | 0.5 | 96.6 (89.7 to 99.3) |
| HPV18 | 4616 | 0 | 0 | 4680 | 28 | 0.2 | 100 (85.7 to 100.0) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 48 | 0.3 | 100 (91.9 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 4 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 45 | 0.3 | 100 (91.4 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 35 | 0.2 | 100 (88.7 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 13 | 0.1 | 100 (66.8 to 100) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 2 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 40 | 0.2 | 100 (90.2 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 5 | <0.1 | 100 (<0 to 100) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 5 | <0.1 | 4735 | 140 | 0.8 | 96.4 (91.4 to 98.9) |
| HPV6 and/or 11 | 4689 | 4 | <0.1 | 4735 | 138 | 0.8 | 97.1 (92.4 to 99.2) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 26 | 0.2 | 96.1 (76.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 17 | 0.1 | 94.0 (62.0 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 11 | 0.1 | 100 (59.6 to 100) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 21 | 0.1 | 95.2 (70.0 to 99.9) |
| HPV6 and/or 11 | 4689 | 1 | <0.1 | 4735 | 12 | 0.1 | 91.6 (42.9 to 99.8) |
| HPV16 and/or 18 | 4689 | 0 | 0 | 4735 | 13 | 0.1 | 100 (66.8 to 100) |
| HPV16 | 4689 | 0 | 0 | 4735 | 9 | 0.1 | 100 (48.6 to 100) |
| HPV18 | 4689 | 0 | 0 | 4735 | 4 | <0.1 | 100 (<0 to 100) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 22 | 0.1 | 95.4 (71.5 to 99.9) |
| HPV6 and/or 11 | 4689 | 0 | 0 | 4735 | 5 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 1 | <0.1 | 100 (<0 to 100) |
| ITT population§ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 114 | 0.4 | 8598 | 366 | 1.2 | 69.0 (61.6 to 75.1) |
| HPV6 and/or 11 | 8562 | 19 | 0.1 | 8598 | 87 | 0.3 | 78.2 (63.9 to 87.5) |
| HPV16 and/or 18 | 8562 | 99 | 0.3 | 8598 | 304 | 1.0 | 67.5 (59.1 to 74.4) |
| HPV16 | 8562 | 81 | 0.3 | 8598 | 240 | 0.8 | 66.3 (56.5 to 74.1) |
| HPV18 | 8562 | 20 | 0.1 | 8598 | 91 | 0.3 | 78.0 (64.1 to 87.2) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 80 | 0.3 | 8598 | 177 | 0.6 | 54.8 (40.8 to 65.7) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 14 | <0.1 | 92.9 (53.0 to 99.8) |
| HPV16 and/or 18 | 8562 | 79 | 0.3 | 8598 | 168 | 0.6 | 53.0 (38.2 to 64.5) |
| HPV16 | 8562 | 74 | 0.2 | 8598 | 142 | 0.5 | 47.9 (30.5 to 61.2) |
| HPV18 | 8562 | 5 | <0.1 | 8598 | 40 | 0.1 | 87.5 (68.3 to 96.1) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 100 | 0.3 | 8598 | 183 | 0.6 | 45.3 (29.8 to 57.6) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 16 | 0.1 | 93.7 (59.7 to 99.9) |
| HPV16 and/or 18 | 8562 | 100 | 0.3 | 8598 | 177 | 0.6 | 43.5 (27.3 to 56.2) |
| HPV16 | 8562 | 97 | 0.3 | 8598 | 164 | 0.6 | 40.8 (23.5 to 54.4) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 24 | 0.1 | 87.5 (58.8 to 97.6) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV6 and/or 11 | 8562 | 0 | 0 | 8598 | 0 | 0 | NA |
| HPV16 and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV16 | 8562 | 3 | <0.1 | 8598 | 12 | <0.1 | 75.0 (7.3 to 95.5) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 7 | <0.1 | 57.1 (<0 to 92.8) |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 63 | 0.2 | 8702 | 305 | 1.0 | 79.5 (73.0 to 84.6) |
| HPV6 and/or 11 | 8689 | 62 | 0.2 | 8702 | 298 | 1.0 | 79.3 (72.7 to 84.5) |
| HPV16 and/or 18 | 8689 | 4 | <0.1 | 8702 | 52 | 0.2 | 92.3 (79.1 to 98.0) |
| HPV16 | 8689 | 3 | <0.1 | 8702 | 32 | 0.1 | 90.6 (70.0 to 98.2) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 22 | 0.1 | 95.4 (71.8 to 99.9) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 12 | <0.1 | 8702 | 50 | 0.2 | 76.0 (54.2 to 88.3) |
| HPV6 and/or 11 | 8689 | 10 | <0.1 | 8702 | 31 | 0.1 | 67.6 (32.3 to 85.9) |
| HPV16 and/or 18 | 8689 | 3 | <0.1 | 8702 | 24 | 0.1 | 87.5 (58.7 to 97.6) |
| HPV16 | 8689 | 2 | <0.1 | 8702 | 18 | 0.1 | 88.9 (53.4 to 98.7) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 6 | <0.1 | 83.3 (<0 to 99.6) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 9 | <0.1 | 8702 | 42 | 0.1 | 78.5 (55.2 to 90.8) |
| HPV6 and/or 11 | 8689 | 1 | <0.1 | 8702 | 11 | <0.1 | 90.9 (37.2 to 99.8) |
| HPV16 and/or 18 | 8689 | 9 | <0.1 | 8702 | 37 | 0.1 | 75.6 (48.5 to 89.6) |
| HPV16 | 8689 | 8 | <0.1 | 8702 | 35 | 0.1 | 77.1 (49.7 to 90.8) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 3 | <0.1 | 66.5 (<0 to 99.4) |
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 3 | <0.1 | 4680 | 136 | 0.8 | 97.8 (93.4 to 99.5) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 34 | 0.2 | 100 (88.4 to 100) |
| HPV16 and/or 18 | 4616 | 3 | <0.1 | 4680 | 107 | 0.6 | 97.2 (91.5 to 99.4) |
| HPV16 | 4616 | 3 | <0.1 | 4680 | 89 | 0.5 | 96.6 (89.7 to 99.3) |
| HPV18 | 4616 | 0 | 0 | 4680 | 28 | 0.2 | 100 (85.7 to 100.0) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 48 | 0.3 | 100 (91.9 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 4 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 45 | 0.3 | 100 (91.4 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 35 | 0.2 | 100 (88.7 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 13 | 0.1 | 100 (66.8 to 100) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 2 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 40 | 0.2 | 100 (90.2 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 5 | <0.1 | 100 (<0 to 100) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 5 | <0.1 | 4735 | 140 | 0.8 | 96.4 (91.4 to 98.9) |
| HPV6 and/or 11 | 4689 | 4 | <0.1 | 4735 | 138 | 0.8 | 97.1 (92.4 to 99.2) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 26 | 0.2 | 96.1 (76.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 17 | 0.1 | 94.0 (62.0 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 11 | 0.1 | 100 (59.6 to 100) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 21 | 0.1 | 95.2 (70.0 to 99.9) |
| HPV6 and/or 11 | 4689 | 1 | <0.1 | 4735 | 12 | 0.1 | 91.6 (42.9 to 99.8) |
| HPV16 and/or 18 | 4689 | 0 | 0 | 4735 | 13 | 0.1 | 100 (66.8 to 100) |
| HPV16 | 4689 | 0 | 0 | 4735 | 9 | 0.1 | 100 (48.6 to 100) |
| HPV18 | 4689 | 0 | 0 | 4735 | 4 | <0.1 | 100 (<0 to 100) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 22 | 0.1 | 95.4 (71.5 to 99.9) |
| HPV6 and/or 11 | 4689 | 0 | 0 | 4735 | 5 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 1 | <0.1 | 100 (<0 to 100) |
| ITT population§ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 114 | 0.4 | 8598 | 366 | 1.2 | 69.0 (61.6 to 75.1) |
| HPV6 and/or 11 | 8562 | 19 | 0.1 | 8598 | 87 | 0.3 | 78.2 (63.9 to 87.5) |
| HPV16 and/or 18 | 8562 | 99 | 0.3 | 8598 | 304 | 1.0 | 67.5 (59.1 to 74.4) |
| HPV16 | 8562 | 81 | 0.3 | 8598 | 240 | 0.8 | 66.3 (56.5 to 74.1) |
| HPV18 | 8562 | 20 | 0.1 | 8598 | 91 | 0.3 | 78.0 (64.1 to 87.2) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 80 | 0.3 | 8598 | 177 | 0.6 | 54.8 (40.8 to 65.7) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 14 | <0.1 | 92.9 (53.0 to 99.8) |
| HPV16 and/or 18 | 8562 | 79 | 0.3 | 8598 | 168 | 0.6 | 53.0 (38.2 to 64.5) |
| HPV16 | 8562 | 74 | 0.2 | 8598 | 142 | 0.5 | 47.9 (30.5 to 61.2) |
| HPV18 | 8562 | 5 | <0.1 | 8598 | 40 | 0.1 | 87.5 (68.3 to 96.1) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 100 | 0.3 | 8598 | 183 | 0.6 | 45.3 (29.8 to 57.6) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 16 | 0.1 | 93.7 (59.7 to 99.9) |
| HPV16 and/or 18 | 8562 | 100 | 0.3 | 8598 | 177 | 0.6 | 43.5 (27.3 to 56.2) |
| HPV16 | 8562 | 97 | 0.3 | 8598 | 164 | 0.6 | 40.8 (23.5 to 54.4) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 24 | 0.1 | 87.5 (58.8 to 97.6) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV6 and/or 11 | 8562 | 0 | 0 | 8598 | 0 | 0 | NA |
| HPV16 and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV16 | 8562 | 3 | <0.1 | 8598 | 12 | <0.1 | 75.0 (7.3 to 95.5) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 7 | <0.1 | 57.1 (<0 to 92.8) |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 63 | 0.2 | 8702 | 305 | 1.0 | 79.5 (73.0 to 84.6) |
| HPV6 and/or 11 | 8689 | 62 | 0.2 | 8702 | 298 | 1.0 | 79.3 (72.7 to 84.5) |
| HPV16 and/or 18 | 8689 | 4 | <0.1 | 8702 | 52 | 0.2 | 92.3 (79.1 to 98.0) |
| HPV16 | 8689 | 3 | <0.1 | 8702 | 32 | 0.1 | 90.6 (70.0 to 98.2) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 22 | 0.1 | 95.4 (71.8 to 99.9) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 12 | <0.1 | 8702 | 50 | 0.2 | 76.0 (54.2 to 88.3) |
| HPV6 and/or 11 | 8689 | 10 | <0.1 | 8702 | 31 | 0.1 | 67.6 (32.3 to 85.9) |
| HPV16 and/or 18 | 8689 | 3 | <0.1 | 8702 | 24 | 0.1 | 87.5 (58.7 to 97.6) |
| HPV16 | 8689 | 2 | <0.1 | 8702 | 18 | 0.1 | 88.9 (53.4 to 98.7) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 6 | <0.1 | 83.3 (<0 to 99.6) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 9 | <0.1 | 8702 | 42 | 0.1 | 78.5 (55.2 to 90.8) |
| HPV6 and/or 11 | 8689 | 1 | <0.1 | 8702 | 11 | <0.1 | 90.9 (37.2 to 99.8) |
| HPV16 and/or 18 | 8689 | 9 | <0.1 | 8702 | 37 | 0.1 | 75.6 (48.5 to 89.6) |
| HPV16 | 8689 | 8 | <0.1 | 8702 | 35 | 0.1 | 77.1 (49.7 to 90.8) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 3 | <0.1 | 66.5 (<0 to 99.4) |
A subject is counted only once within each applicable row. AIS = adenocarcinoma in situ; CI = confidence interval; ITT = intention to treat; NA = not applicable; VaIN = vaginal intraepithelial neoplasia; VIN = vulvar intraepithelial neoplasia.
Women with an endpoint per 100 person-years at risk.
This population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and, at enrollment, were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to the 10 nonvaccine types, including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59; and had a normal Papanicolaou test result.
Intention-to-treat population was all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, regardless of the presence of HPV infection or HPV-related disease at enrollment.
Reductions in cervical intraepithelial neoplasia (CIN) and external genital lesions related to human papillomavirus (HPV) 6, 11, 16, and/or 18*
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 3 | <0.1 | 4680 | 136 | 0.8 | 97.8 (93.4 to 99.5) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 34 | 0.2 | 100 (88.4 to 100) |
| HPV16 and/or 18 | 4616 | 3 | <0.1 | 4680 | 107 | 0.6 | 97.2 (91.5 to 99.4) |
| HPV16 | 4616 | 3 | <0.1 | 4680 | 89 | 0.5 | 96.6 (89.7 to 99.3) |
| HPV18 | 4616 | 0 | 0 | 4680 | 28 | 0.2 | 100 (85.7 to 100.0) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 48 | 0.3 | 100 (91.9 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 4 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 45 | 0.3 | 100 (91.4 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 35 | 0.2 | 100 (88.7 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 13 | 0.1 | 100 (66.8 to 100) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 2 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 40 | 0.2 | 100 (90.2 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 5 | <0.1 | 100 (<0 to 100) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 5 | <0.1 | 4735 | 140 | 0.8 | 96.4 (91.4 to 98.9) |
| HPV6 and/or 11 | 4689 | 4 | <0.1 | 4735 | 138 | 0.8 | 97.1 (92.4 to 99.2) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 26 | 0.2 | 96.1 (76.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 17 | 0.1 | 94.0 (62.0 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 11 | 0.1 | 100 (59.6 to 100) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 21 | 0.1 | 95.2 (70.0 to 99.9) |
| HPV6 and/or 11 | 4689 | 1 | <0.1 | 4735 | 12 | 0.1 | 91.6 (42.9 to 99.8) |
| HPV16 and/or 18 | 4689 | 0 | 0 | 4735 | 13 | 0.1 | 100 (66.8 to 100) |
| HPV16 | 4689 | 0 | 0 | 4735 | 9 | 0.1 | 100 (48.6 to 100) |
| HPV18 | 4689 | 0 | 0 | 4735 | 4 | <0.1 | 100 (<0 to 100) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 22 | 0.1 | 95.4 (71.5 to 99.9) |
| HPV6 and/or 11 | 4689 | 0 | 0 | 4735 | 5 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 1 | <0.1 | 100 (<0 to 100) |
| ITT population§ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 114 | 0.4 | 8598 | 366 | 1.2 | 69.0 (61.6 to 75.1) |
| HPV6 and/or 11 | 8562 | 19 | 0.1 | 8598 | 87 | 0.3 | 78.2 (63.9 to 87.5) |
| HPV16 and/or 18 | 8562 | 99 | 0.3 | 8598 | 304 | 1.0 | 67.5 (59.1 to 74.4) |
| HPV16 | 8562 | 81 | 0.3 | 8598 | 240 | 0.8 | 66.3 (56.5 to 74.1) |
| HPV18 | 8562 | 20 | 0.1 | 8598 | 91 | 0.3 | 78.0 (64.1 to 87.2) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 80 | 0.3 | 8598 | 177 | 0.6 | 54.8 (40.8 to 65.7) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 14 | <0.1 | 92.9 (53.0 to 99.8) |
| HPV16 and/or 18 | 8562 | 79 | 0.3 | 8598 | 168 | 0.6 | 53.0 (38.2 to 64.5) |
| HPV16 | 8562 | 74 | 0.2 | 8598 | 142 | 0.5 | 47.9 (30.5 to 61.2) |
| HPV18 | 8562 | 5 | <0.1 | 8598 | 40 | 0.1 | 87.5 (68.3 to 96.1) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 100 | 0.3 | 8598 | 183 | 0.6 | 45.3 (29.8 to 57.6) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 16 | 0.1 | 93.7 (59.7 to 99.9) |
| HPV16 and/or 18 | 8562 | 100 | 0.3 | 8598 | 177 | 0.6 | 43.5 (27.3 to 56.2) |
| HPV16 | 8562 | 97 | 0.3 | 8598 | 164 | 0.6 | 40.8 (23.5 to 54.4) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 24 | 0.1 | 87.5 (58.8 to 97.6) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV6 and/or 11 | 8562 | 0 | 0 | 8598 | 0 | 0 | NA |
| HPV16 and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV16 | 8562 | 3 | <0.1 | 8598 | 12 | <0.1 | 75.0 (7.3 to 95.5) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 7 | <0.1 | 57.1 (<0 to 92.8) |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 63 | 0.2 | 8702 | 305 | 1.0 | 79.5 (73.0 to 84.6) |
| HPV6 and/or 11 | 8689 | 62 | 0.2 | 8702 | 298 | 1.0 | 79.3 (72.7 to 84.5) |
| HPV16 and/or 18 | 8689 | 4 | <0.1 | 8702 | 52 | 0.2 | 92.3 (79.1 to 98.0) |
| HPV16 | 8689 | 3 | <0.1 | 8702 | 32 | 0.1 | 90.6 (70.0 to 98.2) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 22 | 0.1 | 95.4 (71.8 to 99.9) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 12 | <0.1 | 8702 | 50 | 0.2 | 76.0 (54.2 to 88.3) |
| HPV6 and/or 11 | 8689 | 10 | <0.1 | 8702 | 31 | 0.1 | 67.6 (32.3 to 85.9) |
| HPV16 and/or 18 | 8689 | 3 | <0.1 | 8702 | 24 | 0.1 | 87.5 (58.7 to 97.6) |
| HPV16 | 8689 | 2 | <0.1 | 8702 | 18 | 0.1 | 88.9 (53.4 to 98.7) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 6 | <0.1 | 83.3 (<0 to 99.6) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 9 | <0.1 | 8702 | 42 | 0.1 | 78.5 (55.2 to 90.8) |
| HPV6 and/or 11 | 8689 | 1 | <0.1 | 8702 | 11 | <0.1 | 90.9 (37.2 to 99.8) |
| HPV16 and/or 18 | 8689 | 9 | <0.1 | 8702 | 37 | 0.1 | 75.6 (48.5 to 89.6) |
| HPV16 | 8689 | 8 | <0.1 | 8702 | 35 | 0.1 | 77.1 (49.7 to 90.8) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 3 | <0.1 | 66.5 (<0 to 99.4) |
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 3 | <0.1 | 4680 | 136 | 0.8 | 97.8 (93.4 to 99.5) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 34 | 0.2 | 100 (88.4 to 100) |
| HPV16 and/or 18 | 4616 | 3 | <0.1 | 4680 | 107 | 0.6 | 97.2 (91.5 to 99.4) |
| HPV16 | 4616 | 3 | <0.1 | 4680 | 89 | 0.5 | 96.6 (89.7 to 99.3) |
| HPV18 | 4616 | 0 | 0 | 4680 | 28 | 0.2 | 100 (85.7 to 100.0) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 48 | 0.3 | 100 (91.9 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 4 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 45 | 0.3 | 100 (91.4 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 35 | 0.2 | 100 (88.7 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 13 | 0.1 | 100 (66.8 to 100) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 2 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 41 | 0.2 | 100 (90.5 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 40 | 0.2 | 100 (90.2 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 5 | <0.1 | 100 (<0 to 100) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV6 and/or 11 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| HPV16 and/or 18 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV16 | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| HPV18 | 4616 | 0 | 0 | 4680 | 0 | 0 | NA |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 5 | <0.1 | 4735 | 140 | 0.8 | 96.4 (91.4 to 98.9) |
| HPV6 and/or 11 | 4689 | 4 | <0.1 | 4735 | 138 | 0.8 | 97.1 (92.4 to 99.2) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 26 | 0.2 | 96.1 (76.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 17 | 0.1 | 94.0 (62.0 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 11 | 0.1 | 100 (59.6 to 100) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 21 | 0.1 | 95.2 (70.0 to 99.9) |
| HPV6 and/or 11 | 4689 | 1 | <0.1 | 4735 | 12 | 0.1 | 91.6 (42.9 to 99.8) |
| HPV16 and/or 18 | 4689 | 0 | 0 | 4735 | 13 | 0.1 | 100 (66.8 to 100) |
| HPV16 | 4689 | 0 | 0 | 4735 | 9 | 0.1 | 100 (48.6 to 100) |
| HPV18 | 4689 | 0 | 0 | 4735 | 4 | <0.1 | 100 (<0 to 100) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 4689 | 1 | <0.1 | 4735 | 22 | 0.1 | 95.4 (71.5 to 99.9) |
| HPV6 and/or 11 | 4689 | 0 | 0 | 4735 | 5 | <0.1 | 100 (<0 to 100) |
| HPV16 and/or 18 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV16 | 4689 | 1 | <0.1 | 4735 | 20 | 0.1 | 94.9 (68.3 to 99.9) |
| HPV18 | 4689 | 0 | 0 | 4735 | 1 | <0.1 | 100 (<0 to 100) |
| ITT population§ | |||||||
| CIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 114 | 0.4 | 8598 | 366 | 1.2 | 69.0 (61.6 to 75.1) |
| HPV6 and/or 11 | 8562 | 19 | 0.1 | 8598 | 87 | 0.3 | 78.2 (63.9 to 87.5) |
| HPV16 and/or 18 | 8562 | 99 | 0.3 | 8598 | 304 | 1.0 | 67.5 (59.1 to 74.4) |
| HPV16 | 8562 | 81 | 0.3 | 8598 | 240 | 0.8 | 66.3 (56.5 to 74.1) |
| HPV18 | 8562 | 20 | 0.1 | 8598 | 91 | 0.3 | 78.0 (64.1 to 87.2) |
| CIN2 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 80 | 0.3 | 8598 | 177 | 0.6 | 54.8 (40.8 to 65.7) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 14 | <0.1 | 92.9 (53.0 to 99.8) |
| HPV16 and/or 18 | 8562 | 79 | 0.3 | 8598 | 168 | 0.6 | 53.0 (38.2 to 64.5) |
| HPV16 | 8562 | 74 | 0.2 | 8598 | 142 | 0.5 | 47.9 (30.5 to 61.2) |
| HPV18 | 8562 | 5 | <0.1 | 8598 | 40 | 0.1 | 87.5 (68.3 to 96.1) |
| CIN3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 100 | 0.3 | 8598 | 183 | 0.6 | 45.3 (29.8 to 57.6) |
| HPV6 and/or 11 | 8562 | 1 | <0.1 | 8598 | 16 | 0.1 | 93.7 (59.7 to 99.9) |
| HPV16 and/or 18 | 8562 | 100 | 0.3 | 8598 | 177 | 0.6 | 43.5 (27.3 to 56.2) |
| HPV16 | 8562 | 97 | 0.3 | 8598 | 164 | 0.6 | 40.8 (23.5 to 54.4) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 24 | 0.1 | 87.5 (58.8 to 97.6) |
| AIS related to | |||||||
| HPV6, 11, 16, and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV6 and/or 11 | 8562 | 0 | 0 | 8598 | 0 | 0 | NA |
| HPV16 and/or 18 | 8562 | 6 | <0.1 | 8598 | 15 | 0.1 | 60.0 (<0 to 87.3) |
| HPV16 | 8562 | 3 | <0.1 | 8598 | 12 | <0.1 | 75.0 (7.3 to 95.5) |
| HPV18 | 8562 | 3 | <0.1 | 8598 | 7 | <0.1 | 57.1 (<0 to 92.8) |
| Genital warts related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 63 | 0.2 | 8702 | 305 | 1.0 | 79.5 (73.0 to 84.6) |
| HPV6 and/or 11 | 8689 | 62 | 0.2 | 8702 | 298 | 1.0 | 79.3 (72.7 to 84.5) |
| HPV16 and/or 18 | 8689 | 4 | <0.1 | 8702 | 52 | 0.2 | 92.3 (79.1 to 98.0) |
| HPV16 | 8689 | 3 | <0.1 | 8702 | 32 | 0.1 | 90.6 (70.0 to 98.2) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 22 | 0.1 | 95.4 (71.8 to 99.9) |
| VIN1 or VaIN1 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 12 | <0.1 | 8702 | 50 | 0.2 | 76.0 (54.2 to 88.3) |
| HPV6 and/or 11 | 8689 | 10 | <0.1 | 8702 | 31 | 0.1 | 67.6 (32.3 to 85.9) |
| HPV16 and/or 18 | 8689 | 3 | <0.1 | 8702 | 24 | 0.1 | 87.5 (58.7 to 97.6) |
| HPV16 | 8689 | 2 | <0.1 | 8702 | 18 | 0.1 | 88.9 (53.4 to 98.7) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 6 | <0.1 | 83.3 (<0 to 99.6) |
| VIN2–3 or VaIN2–3 related to | |||||||
| HPV6, 11, 16, and/or 18 | 8689 | 9 | <0.1 | 8702 | 42 | 0.1 | 78.5 (55.2 to 90.8) |
| HPV6 and/or 11 | 8689 | 1 | <0.1 | 8702 | 11 | <0.1 | 90.9 (37.2 to 99.8) |
| HPV16 and/or 18 | 8689 | 9 | <0.1 | 8702 | 37 | 0.1 | 75.6 (48.5 to 89.6) |
| HPV16 | 8689 | 8 | <0.1 | 8702 | 35 | 0.1 | 77.1 (49.7 to 90.8) |
| HPV18 | 8689 | 1 | <0.1 | 8702 | 3 | <0.1 | 66.5 (<0 to 99.4) |
A subject is counted only once within each applicable row. AIS = adenocarcinoma in situ; CI = confidence interval; ITT = intention to treat; NA = not applicable; VaIN = vaginal intraepithelial neoplasia; VIN = vulvar intraepithelial neoplasia.
Women with an endpoint per 100 person-years at risk.
This population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and, at enrollment, were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to the 10 nonvaccine types, including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59; and had a normal Papanicolaou test result.
Intention-to-treat population was all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, regardless of the presence of HPV infection or HPV-related disease at enrollment.
Reductions in any cervical intraepithelial neoplasia (CIN) and any external genital lesion irrespective of causal human papillomavirus (HPV) type*
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 4616 | 272 | 1.7 | 4680 | 390 | 2.4 | 29.7 (17.7 to 40.0) |
| Any CIN2 or worse irrespective of causal HPV type | 4616 | 77 | 0.5 | 4680 | 136 | 0.8 | 42.7 (23.7 to 57.3) |
| By lesion severity | |||||||
| CIN1 | 4616 | 241 | 1.5 | 4680 | 346 | 2.1 | 29.7 (16.9 to 40.6) |
| CIN2 | 4616 | 57 | 0.3 | 4680 | 101 | 0.6 | 42.9 (20.2 to 59.5) |
| CIN3 | 4616 | 36 | 0.2 | 4680 | 64 | 0.4 | 43 (13.0 to 63.2) |
| AIS | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| Any genital wart irrespective of causal HPV type | 4689 | 29 | 0.2 | 4735 | 169 | 1.0 | 82.8 (74.3 to 88.8) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 4689 | 25 | 0.2 | 4735 | 56 | 0.3 | 54.8 (26.4 to 73.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 4689 | 7 | <0.1 | 4735 | 31 | 0.2 | 77.1 (47.1 to 91.5) |
| ITT population§ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 8562 | 975 | 3.4 | 8598 | 1199 | 4.2 | 19.1 (11.9 to 25.7) |
| Any CIN2 or worse irrespective of causal HPV type | 8562 | 421 | 1.4 | 8598 | 520 | 1.8 | 19.0 (7.7 to 28.9) |
| By lesion severity | |||||||
| CIN1 | 8562 | 778 | 2.7 | 8598 | 984 | 3.4 | 20.3 (12.4 to 27.5) |
| CIN2 | 8562 | 296 | 1.0 | 8598 | 367 | 1.2 | 19.3 (5.7 to 31.0) |
| CIN3 | 8562 | 237 | 0.8 | 8598 | 284 | 1.0 | 16.4 (0.4 to 30.0) |
| AIS | 8562 | 6 | <0.1 | 8598 | 16 | 0.1 | 62.5 (<0 to 88.0) |
| Any genital wart irrespective of causal HPV type | 8689 | 134 | 0.4 | 8702 | 351 | 1.2 | 62.0 (53.5 to 69.1) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 8689 | 89 | 0.3 | 8702 | 127 | 0.4 | 29.7 (7.2 to 47.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 8689 | 30 | 0.1 | 8702 | 61 | 0.2 | 50.7 (22.5 to 69.3) |
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 4616 | 272 | 1.7 | 4680 | 390 | 2.4 | 29.7 (17.7 to 40.0) |
| Any CIN2 or worse irrespective of causal HPV type | 4616 | 77 | 0.5 | 4680 | 136 | 0.8 | 42.7 (23.7 to 57.3) |
| By lesion severity | |||||||
| CIN1 | 4616 | 241 | 1.5 | 4680 | 346 | 2.1 | 29.7 (16.9 to 40.6) |
| CIN2 | 4616 | 57 | 0.3 | 4680 | 101 | 0.6 | 42.9 (20.2 to 59.5) |
| CIN3 | 4616 | 36 | 0.2 | 4680 | 64 | 0.4 | 43 (13.0 to 63.2) |
| AIS | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| Any genital wart irrespective of causal HPV type | 4689 | 29 | 0.2 | 4735 | 169 | 1.0 | 82.8 (74.3 to 88.8) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 4689 | 25 | 0.2 | 4735 | 56 | 0.3 | 54.8 (26.4 to 73.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 4689 | 7 | <0.1 | 4735 | 31 | 0.2 | 77.1 (47.1 to 91.5) |
| ITT population§ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 8562 | 975 | 3.4 | 8598 | 1199 | 4.2 | 19.1 (11.9 to 25.7) |
| Any CIN2 or worse irrespective of causal HPV type | 8562 | 421 | 1.4 | 8598 | 520 | 1.8 | 19.0 (7.7 to 28.9) |
| By lesion severity | |||||||
| CIN1 | 8562 | 778 | 2.7 | 8598 | 984 | 3.4 | 20.3 (12.4 to 27.5) |
| CIN2 | 8562 | 296 | 1.0 | 8598 | 367 | 1.2 | 19.3 (5.7 to 31.0) |
| CIN3 | 8562 | 237 | 0.8 | 8598 | 284 | 1.0 | 16.4 (0.4 to 30.0) |
| AIS | 8562 | 6 | <0.1 | 8598 | 16 | 0.1 | 62.5 (<0 to 88.0) |
| Any genital wart irrespective of causal HPV type | 8689 | 134 | 0.4 | 8702 | 351 | 1.2 | 62.0 (53.5 to 69.1) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 8689 | 89 | 0.3 | 8702 | 127 | 0.4 | 29.7 (7.2 to 47.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 8689 | 30 | 0.1 | 8702 | 61 | 0.2 | 50.7 (22.5 to 69.3) |
A subject is counted only once within each applicable row. There were no cases of cervical cancer. There was one case of vulvar cancer in the negative to 14 HPV types population (vaccine arm) diagnosed 18 months post-dose 3 that is not included in this table. The lesion was negative to all tested HPV types, as described previously (7,10). AIS = adenocarcinoma in situ; CI = confidence interval; ITT = intention to treat; VaIN = vaginal intraepithelial neoplasia; VIN = vulvar intraepithelial neoplasia.
Women with an endpoint per 100 person-years at risk.
This population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and, at enrollment, were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 nonvaccine HPV types, including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59; and had a normal Papanicolaou test result.
Intention-to-treat population was all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, regardless of the presence of HPV infection or HPV-related disease at enrollment.
Reductions in any cervical intraepithelial neoplasia (CIN) and any external genital lesion irrespective of causal human papillomavirus (HPV) type*
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 4616 | 272 | 1.7 | 4680 | 390 | 2.4 | 29.7 (17.7 to 40.0) |
| Any CIN2 or worse irrespective of causal HPV type | 4616 | 77 | 0.5 | 4680 | 136 | 0.8 | 42.7 (23.7 to 57.3) |
| By lesion severity | |||||||
| CIN1 | 4616 | 241 | 1.5 | 4680 | 346 | 2.1 | 29.7 (16.9 to 40.6) |
| CIN2 | 4616 | 57 | 0.3 | 4680 | 101 | 0.6 | 42.9 (20.2 to 59.5) |
| CIN3 | 4616 | 36 | 0.2 | 4680 | 64 | 0.4 | 43 (13.0 to 63.2) |
| AIS | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| Any genital wart irrespective of causal HPV type | 4689 | 29 | 0.2 | 4735 | 169 | 1.0 | 82.8 (74.3 to 88.8) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 4689 | 25 | 0.2 | 4735 | 56 | 0.3 | 54.8 (26.4 to 73.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 4689 | 7 | <0.1 | 4735 | 31 | 0.2 | 77.1 (47.1 to 91.5) |
| ITT population§ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 8562 | 975 | 3.4 | 8598 | 1199 | 4.2 | 19.1 (11.9 to 25.7) |
| Any CIN2 or worse irrespective of causal HPV type | 8562 | 421 | 1.4 | 8598 | 520 | 1.8 | 19.0 (7.7 to 28.9) |
| By lesion severity | |||||||
| CIN1 | 8562 | 778 | 2.7 | 8598 | 984 | 3.4 | 20.3 (12.4 to 27.5) |
| CIN2 | 8562 | 296 | 1.0 | 8598 | 367 | 1.2 | 19.3 (5.7 to 31.0) |
| CIN3 | 8562 | 237 | 0.8 | 8598 | 284 | 1.0 | 16.4 (0.4 to 30.0) |
| AIS | 8562 | 6 | <0.1 | 8598 | 16 | 0.1 | 62.5 (<0 to 88.0) |
| Any genital wart irrespective of causal HPV type | 8689 | 134 | 0.4 | 8702 | 351 | 1.2 | 62.0 (53.5 to 69.1) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 8689 | 89 | 0.3 | 8702 | 127 | 0.4 | 29.7 (7.2 to 47.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 8689 | 30 | 0.1 | 8702 | 61 | 0.2 | 50.7 (22.5 to 69.3) |
| Vaccine group | Placebo group | ||||||
| Endpoint and population | No. of women | No. of women with a lesion | Rate† | No. of women | No. of women with a lesion | Rate† | % Reduction (95% CI) |
| Negative to 14 HPV types population‡ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 4616 | 272 | 1.7 | 4680 | 390 | 2.4 | 29.7 (17.7 to 40.0) |
| Any CIN2 or worse irrespective of causal HPV type | 4616 | 77 | 0.5 | 4680 | 136 | 0.8 | 42.7 (23.7 to 57.3) |
| By lesion severity | |||||||
| CIN1 | 4616 | 241 | 1.5 | 4680 | 346 | 2.1 | 29.7 (16.9 to 40.6) |
| CIN2 | 4616 | 57 | 0.3 | 4680 | 101 | 0.6 | 42.9 (20.2 to 59.5) |
| CIN3 | 4616 | 36 | 0.2 | 4680 | 64 | 0.4 | 43 (13.0 to 63.2) |
| AIS | 4616 | 0 | 0 | 4680 | 3 | <0.1 | 100 (<0 to 100) |
| Any genital wart irrespective of causal HPV type | 4689 | 29 | 0.2 | 4735 | 169 | 1.0 | 82.8 (74.3 to 88.8) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 4689 | 25 | 0.2 | 4735 | 56 | 0.3 | 54.8 (26.4 to 73.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 4689 | 7 | <0.1 | 4735 | 31 | 0.2 | 77.1 (47.1 to 91.5) |
| ITT population§ | |||||||
| Any CIN1 or worse irrespective of causal HPV type | 8562 | 975 | 3.4 | 8598 | 1199 | 4.2 | 19.1 (11.9 to 25.7) |
| Any CIN2 or worse irrespective of causal HPV type | 8562 | 421 | 1.4 | 8598 | 520 | 1.8 | 19.0 (7.7 to 28.9) |
| By lesion severity | |||||||
| CIN1 | 8562 | 778 | 2.7 | 8598 | 984 | 3.4 | 20.3 (12.4 to 27.5) |
| CIN2 | 8562 | 296 | 1.0 | 8598 | 367 | 1.2 | 19.3 (5.7 to 31.0) |
| CIN3 | 8562 | 237 | 0.8 | 8598 | 284 | 1.0 | 16.4 (0.4 to 30.0) |
| AIS | 8562 | 6 | <0.1 | 8598 | 16 | 0.1 | 62.5 (<0 to 88.0) |
| Any genital wart irrespective of causal HPV type | 8689 | 134 | 0.4 | 8702 | 351 | 1.2 | 62.0 (53.5 to 69.1) |
| Any VIN1 or VaIN1 irrespective of causal HPV type | 8689 | 89 | 0.3 | 8702 | 127 | 0.4 | 29.7 (7.2 to 47.0) |
| Any VIN2–3 or VaIN2–3 irrespective of causal HPV type | 8689 | 30 | 0.1 | 8702 | 61 | 0.2 | 50.7 (22.5 to 69.3) |
A subject is counted only once within each applicable row. There were no cases of cervical cancer. There was one case of vulvar cancer in the negative to 14 HPV types population (vaccine arm) diagnosed 18 months post-dose 3 that is not included in this table. The lesion was negative to all tested HPV types, as described previously (7,10). AIS = adenocarcinoma in situ; CI = confidence interval; ITT = intention to treat; VaIN = vaginal intraepithelial neoplasia; VIN = vulvar intraepithelial neoplasia.
Women with an endpoint per 100 person-years at risk.
This population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and, at enrollment, were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 nonvaccine HPV types, including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59; and had a normal Papanicolaou test result.
Intention-to-treat population was all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, regardless of the presence of HPV infection or HPV-related disease at enrollment.
A point estimate of vaccine efficacy (ie, percentage reduction of the relevant endpoint) and its 95% confidence interval (CI) were calculated on the basis of the observed number of women who had reached various endpoints in the vaccine and placebo groups, adjusted for the accrued person-time in each group. The statistical criterion for success (P < .05) was equivalent to requiring that the lower bound of the 95% confidence interval for vaccine efficacy exclude 0%. An exact conditional procedure was used to evaluate vaccine efficacy under the assumption that the numbers of women who reached an endpoint in the vaccine and placebo groups were independent Poisson random variables (28).
Kaplan–Meier estimates of incidence rates (and their 95% confidence intervals) over time were plotted (29). The plots were not part of a survival analysis and so provide only a visual demonstration of the divergence of the incidence rates between the two vaccine and placebo groups over time. The 95% confidence intervals for the Kaplan–Meier incidence at 6-month time intervals rates are not directly comparable to vaccine efficacy estimates and so vaccine efficacy cannot be inferred. Vaccine efficacy was calculated from the exact conditional procedure after 1.5 and 2.5 years of follow-up and at the end of the study and was included in the Kaplan–Meier plots as a reference.
We also summarized the efficacy in the negative to 14 HPV types and ITT populations in terms of risk reduction, or risk difference, by subtracting the rate in the vaccine group from the rate in the placebo group. The rates were taken directly from the number of women who had reached each endpoint per 100 person-years at risk in each treatment group and were used to estimate the numbers of each endpoint that were prevented annually per 100 000 women vaccinated.
Results
Baseline Characteristics
Day 1 Pap test results, stratified by day 1 PCR status, are shown in Figure 1. Among the 17 114 women with a satisfactory day 1 Pap test result, 5552 (32.4%) were positive for at least one of the 14 tested HPV types. Positivity to an HPV type belonging to the alpha-papillomavirus-9 species (ie, HPV16, 31, 33, 35, 52, and 58) was more common than positivity to an HPV type belonging to the alpha-papillomavirus-7 species (ie, HPV18, 39, 45, and 59), with the former detected in 134 (84%) of 159 women with high-grade squamous intraepithelial lesions. As expected, detection of HPV16 and HPV18 increased with increasing severity of the Pap test result (negative = 1333 [8.8%] of 15 159 women; atypical squamous cells of undetermined significance = 169 [21.3%] of 794 women; low-grade squamous intraepithelial lesion = 376 [37.5%] of 1002 women; and high-grade squamous intraepithelial lesion = 96 [60.4%] of 159 women). HPV6 or HPV11 was detected in 3.6%, 8.7%, 16.2%, and 10.1% of women with negative, atypical squamous cells of undetermined significance, low-grade squamous intraepithelial lesions, and high-grade squamous intraepithelial lesions, respectively.
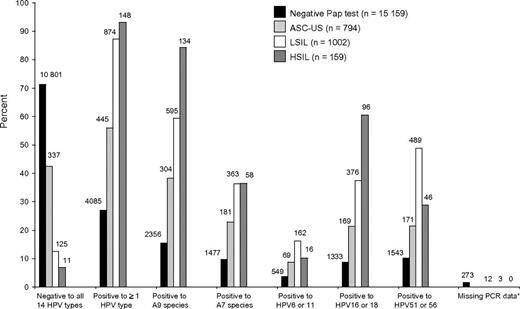
Day 1 Papanicolaou (Pap) test result by day 1 polymerase chain reaction (PCR) status (vaccine and placebo groups combined). Numbers above each bar indicate the number of subjects with a respective Pap diagnosis that was DNA positive or negative, as determined by PCR, to the indicated human papillomavirus (HPV) type or species that was detected in the anogenital swab collected at the same visit. Percent is calculated as the number of subjects with the indicated Pap diagnosis that were DNA positive or negative by PCR to the indicated HPV type or species divided by the number of subjects with the respective Pap diagnosis. ASC-US = atypical squamous cells of undetermined significance; HSIL = high-grade squamous intraepithelial lesion; LSIL = low-grade squamous intraepithelial lesion. Asterisk indicates that subject was missing a PCR test result for at least one HPV type and was negative to all HPV types for which testing was available. A9 and A7 refer to alpha-papillomavirus species 9 and 7, respectively.
Vaccine Efficacy in the Population Negative to 14 HPV Types
The negative to 14 HPV types population (Table 1) included approximately 53% of the enrolled subjects (Supplementary Figure 1, available online). Efficacy for CIN related to HPV6, 11, 16, and/or 18 (Table 2) ranged from 97.8% for CIN1 to 100% for CIN2, CIN3, and AIS, although the data were not statistically significant for AIS alone (ie, zero cases in the vaccine group and three cases in the placebo group). For the CIN3 endpoint, all CIN3 lesions among the 41 women were positive for HPV16 and/or HPV18 DNA and two also were positive for HPV6 and/or HPV11 DNA. Two of the three women in the placebo group who reached an AIS endpoint had lesions that were positive for HPV16 only and the third AIS lesion was positive for HPV16 and HPV39.
For external genital lesions, efficacy for disease related to HPV6, 11, 16, and/or 18 (Table 2) ranged from 95.2% for VIN1 and/or VaIN1 to 96.4% for genital warts. In the placebo group, we observed 22 women who reached an endpoint of VIN2–3 or VaIN2–3, whereby the lesion was positive for HPV6, 11, 16, and/or 18 (20 were positive for HPV16 and/or HPV18 and five were positive for HPV6 and/or HPV11). Thus, three of these VIN2–3 or VaIN2–3 lesions were positive to both HPV16 or 18 and HPV6 or 11 and two were positive for HPV6 and/or HPV11 and negative for HPV16 and HPV18 (a VIN2–3 lesion that was positive for HPV6 and HPV31 and a VaIN2–3 lesion that was positive for HPV6 only). One HPV16-related VIN2–3 was found in the vaccine group in a woman who was naive to HPV16 at day 1 but became infected with HPV16 before receiving all three doses of vaccine. In previously published per-protocol analyses, efficacy for VIN2–3 related to HPV6, 11, 16, and/or 18 was 100% (95% CI = 67% to 100.0%) (30). In the placebo group, 140 women were diagnosed with a genital wart positive to a vaccine HPV type (138 related to HPV6 or HPV11 and 26 related to HPV16 or HPV18). Thus, 24 women had lesions with both HPV6 and/or 11 and HPV16 and/or 18, and two women had lesions that were positive for either HPV16 or HPV18 and negative for HPV6 and 11. Because we did not test for other low-risk types of HPV that infect the anogenital tract, it is possible that another low-risk type was present and that neither HPV16 nor HPV18 was the causal HPV type in these two genital warts that were positive for HPV16 and/or 18. There was also one woman in the vaccine group who had an HPV16-related genital wart that was negative for HPV6 and HPV11.
Prophylactic vaccination statistically significantly reduced the incidence of all CIN and all external genital lesions, irrespective of causal HPV type (Table 3). For any CIN3, the reduction was 43% (95% CI = 13.0% to 63.2%). Figure 2, A and C, shows the divergence of incidence rates over time for CIN3 or AIS related to HPV6, 11, 16, and/or 18 and all CIN3 and AIS irrespective of causal HPV type in the negative to 14 HPV types population. During the follow-up period, the incidence of all CIN3 and AIS lesions, irrespective of causal HPV type, continued to increase among the women in the placebo group, whereas the incidence began to plateau among women in the vaccine group (Figure 2, C).
![Kaplan–Meier time to event curves (estimates and 95% confidence intervals [CIs] at 6-month intervals) for cervical intraepithelial neoplasia 3 (CIN3) or adenocarcinoma in situ (AIS). A) CIN3 or AIS related to human papillomavirus (HPV) 6, 11, 16, and/or 18 in the negative to 14 HPV types group. B) CIN3 or AIS related to HPV6, 11, 16, and/or 18 in the intention-to-treat (ITT) group. C) All CIN3 and AIS irrespective of causal HPV type in the negative to 14 HPV types group. D) All CIN3 and AIS irrespective of causal HPV type in the ITT group. In panels A and C, the negative to 14 HPV types population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and who at enrollment were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 of the nonvaccine HPV types (including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59); and had a normal Papanicolaou test result. In panels B and D, the ITT population was composed of all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and returned for follow-up visits, regardless of the presence of HPV infection or HPV-related disease at enrollment.](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/jnci/102/5/10.1093_jnci_djp534/3/m_jncidjp534f02_lw.jpeg?Expires=1716397774&Signature=rszmtHd6lHuCD~QGK3N3AihwciQtZH-zUQAeR6-ft9EiPKiIKJvewTbZLjkqbYLSnrQCCY2otr1yJMdBTR115AehygZaoYCadX8jDIFvda~0xJyCpIJ0OvjcjtsBxDZnOO471A3w1qLpYNH8zrBeAGFf~aDPEDhDnew0swfd6j~IFdsAJcqDWVyVWYtVtgqFLDJjzvLmKlvKAYn12Cm1b8ZF~AVoHD7j17wN4gtbJU0fYArhuXd9t~VYnWRNV8azvz2osTTAazr9rmaqnQv6bWn2ksg6n3efr0enSMu6MB5uwDkmKHzFXvNrDew~AmPtytCAD00bqWlZS17FlYbG5w__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Kaplan–Meier time to event curves (estimates and 95% confidence intervals [CIs] at 6-month intervals) for cervical intraepithelial neoplasia 3 (CIN3) or adenocarcinoma in situ (AIS). A) CIN3 or AIS related to human papillomavirus (HPV) 6, 11, 16, and/or 18 in the negative to 14 HPV types group. B) CIN3 or AIS related to HPV6, 11, 16, and/or 18 in the intention-to-treat (ITT) group. C) All CIN3 and AIS irrespective of causal HPV type in the negative to 14 HPV types group. D) All CIN3 and AIS irrespective of causal HPV type in the ITT group. In panels A and C, the negative to 14 HPV types population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and who at enrollment were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 of the nonvaccine HPV types (including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59); and had a normal Papanicolaou test result. In panels B and D, the ITT population was composed of all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and returned for follow-up visits, regardless of the presence of HPV infection or HPV-related disease at enrollment.
Prophylactic vaccination resulted in a 92% reduction in HPV16-related Pap test abnormalities (ie, atypical squamous cells of undetermined significance high-risk probe positive or worse) and a 97% reduction in HPV18-related Pap test abnormalities (Figure 3, A). The impact on Pap test abnormalities irrespective of causal HPV type as expected was less, with an overall reduction of 17.1% (Figure 3, B). However, there were statistically significant reductions for all categories of Pap test diagnoses. The observed reductions generally increased with increasing lesion severity (ie, low-grade squamous intraepithelial lesion = 17.0% reduction, 95% CI = 8.8% to 24.4%; high-grade squamous intraepithelial lesion = 44.5% reduction, 95% CI = 4.3% to 68.6%).
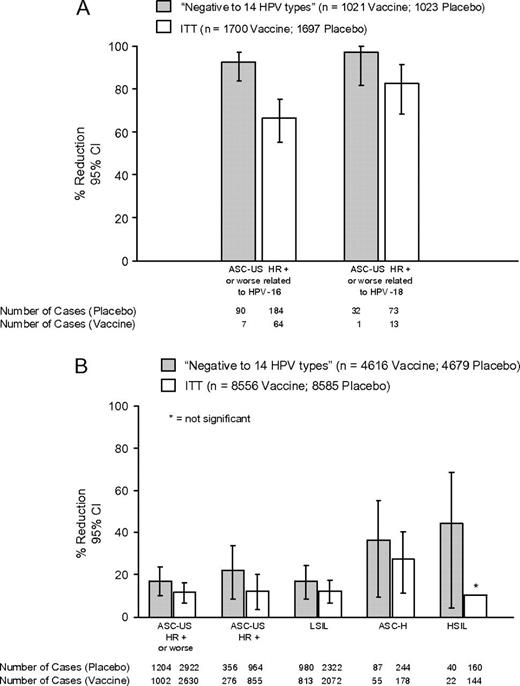
Reductions in Papanicolaou (Pap) test abnormalities. A) Related to HPV16 and HPV18. This analysis included only a subset of Females United to Unilaterally Reduce Endo/Ectocervical Disease (FUTURE) I subjects because these women were the only subjects whose swabs after the month 7 visit were tested for HPV16 and HPV18 DNA. In addition, a Pap test was considered HPV16 and/or HPV18 related if the endo–ectocervical swab collected at the same visit was positive for HPV16 DNA and/or HPV18 DNA. B) Related to any HPV type. Error bars = 95% confidence intervals. In both panels, the negative to 14 HPV types population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and who at enrollment were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 of the nonvaccine HPV types (including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59); and had a normal Pap test result. The intention-to-treat (ITT) population was composed of all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and returned for follow-up visits, regardless of the presence of HPV infection or HPV-related disease at enrollment. ASC-H = atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion; ASC-US HR+ = atypical squamous cells of undetermined significance high-risk probe positive; HSIL = high-grade squamous intraepithelial lesion; LSIL = low-grade squamous intraepithelial lesion.
Prophylactic vaccination also statistically significantly reduced the risk of any colposcopy by 19.8%, any cervical biopsy examination by 22.0%, and any cervical definitive therapy by 42.3% (Figure 4, A). The reduction in all procedures for external genital lesions (genital warts, VIN1–3, or VaIN1–3) was 43.3% (95% CI = 24.4% to 57.8%) (Figure 4, B).
![Reductions in procedures for all human papillomavirus (HPV)–associated genital diseases. A) All cervical procedures irrespective of causal HPV type. B) All procedures for external genital lesions (EGL; including genital warts, vulvar intraepithelial neoplasia [VIN] 1–3, or vaginal intraepithelial neoplasia [VaIN] 1–3), irrespective of causal HPV type. In panel B, the analyses for EGL procedures include Females United to Unilaterally Reduce Endo/Ectocervical Disease (FUTURE) I subjects only, because treatment for VIN and VaIN were generally not recorded in FUTURE II. In both panels, the negative to 14 HPV types population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and who at enrollment were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 of the nonvaccine HPV types (including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59); and had a normal Papanicolaou test result. The intention-to-treat (ITT) population was composed of all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and returned for follow-up visits, regardless of the presence of HPV infection or HPV-related disease at enrollment. Error bars = confidence intervals.](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/jnci/102/5/10.1093_jnci_djp534/3/m_jncidjp534f04_ht.jpeg?Expires=1716397774&Signature=420xHx5tr8YOchPylQ46vkzJlw~ZdFkb1nztqMYRCFVdKCvfK~g6yWYbOVY7Y-kcgXR~fWApZ2Ljugc2Zxf7-blNUILB~OUC4o-1Vc2fDcQ8Phl2U-qJcxYhr4qkASl7a~n2qpQG0fWlshYJnI-0r-VlSDRccnAoMyI9U8LDTtI5KLWvg6cP707BXu-1YaD7RkuY-t9s6SigcWmR2ZsITj6sq5m0JXcIE74tlrU4tgNU5iVFck2HGc0IqCU8gj99J02YapjOd0tTp6V1jJpXAfwfOhv9y9oaPmiuxptopvrZ47lxAmd17PB6JpUCOmEP13qCr2pBJ00yV-26sI2oRg__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Reductions in procedures for all human papillomavirus (HPV)–associated genital diseases. A) All cervical procedures irrespective of causal HPV type. B) All procedures for external genital lesions (EGL; including genital warts, vulvar intraepithelial neoplasia [VIN] 1–3, or vaginal intraepithelial neoplasia [VaIN] 1–3), irrespective of causal HPV type. In panel B, the analyses for EGL procedures include Females United to Unilaterally Reduce Endo/Ectocervical Disease (FUTURE) I subjects only, because treatment for VIN and VaIN were generally not recorded in FUTURE II. In both panels, the negative to 14 HPV types population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and who at enrollment were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 of the nonvaccine HPV types (including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59); and had a normal Papanicolaou test result. The intention-to-treat (ITT) population was composed of all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and returned for follow-up visits, regardless of the presence of HPV infection or HPV-related disease at enrollment. Error bars = confidence intervals.
Vaccine Efficacy in the ITT Population
Women in the ITT population were previously exposed or unexposed to HPV. In the ITT group, vaccination statistically significantly reduced the risk of any high-grade cervical lesions, irrespective of causal HPV type (19.0% reduction, 95% CI = 7.7% to 28.9%, rate vaccine = 1.43, rate placebo = 1.76, difference = 0.33, 95% CI = 0.13 to 0.54). In the ITT population, statistically significant reductions were observed for all disease endpoints irrespective of causal HPV type (Table 3), with the exception of AIS (six cases of AIS in the vaccine group and 16 in the placebo group; 62.5% reduction, 95% CI = <0% to 88.0%). Of the 16 women with an AIS endpoint in the placebo group, 15 had lesions that were associated with HPV16 and/or HPV18. There were six women with a CIN3 endpoint in the placebo group who had lesions that were associated with HPV6 and/or HPV11, with no coinfection with HPV16 or HPV18. Of these six women, four had a coinfection with a nonvaccine high-risk HPV type in the same lesion, one had a coinfection with two nonvaccine high-risk types in swabs only (before receiving all three doses of vaccine), and one had no coinfections detected in lesions or swabs.
The percent reduction observed for genital warts and the precursor lesions to HPV-related vulvar and vaginal cancers (VIN2–3 and VaIN2–3) irrespective of causal HPV type (Table 3) was 62% (95% CI = 53.5% to 69.1%, rate vaccine = 0.44, rate placebo = 1.17, difference = 0.72, 95% CI = 0.58 to 0.87) and 50.7% (95% CI = 22.5% to 69.3%, rate vaccine = 0.10, rate placebo = 0.20, difference = 0.10, 95% CI = 0.04 to 0.16). Four women in the placebo group who reached a VIN2–3 endpoint and one who reached a VaIN2–3 endpoint had lesions that were positive for HPV6 and negative for the other three vaccine HPV types (ie, two VIN2–3 lesions and one VaIN2–3 lesion were positive for HPV6 only, one woman with a VIN2–3 lesion had HPV16 and HPV31 detected in a swab at her day 1 visit and had HPV16 detected later in a VIN1 lesion, and one woman with a VIN2–3 lesion was positive for HPV31).
Figure 2, B and D, shows the divergence of incidence rates over time for CIN3 and AIS related to HPV6, 11, 16, and/or 18 and all CIN3 and AIS irrespective of causal HPV type in the ITT population. The incidence of disease related to HPV6, 11, 16, and/or 18 had not reached a plateau in the placebo group by the end of the study (Figure 2, B). For any CIN3 or AIS irrespective of causal HPV type (Figure 2, D), the divergence of incidence rates between the vaccine group and the placebo group increased at each 6-month interval. The percent reduction at the end of the study for any CIN3 or AIS was 18.0% (95% CI = 2.4% to 31.2%). As shown in Figure 2, D, the vaccine's impact on the risk of having any CIN3 or AIS doubled between 2.5 years and the end of the study and might be expected to increase with longer follow-up, as the prevalent infection and/or disease is treated in both the vaccine group and the placebo group and as vaccine recipients are protected from disease caused by new HPV infections.
Statistically significant reductions were observed in the ITT population for all categories of Pap test diagnoses (11.3% reduction, 95% CI = 6.5% to 15.9%, rate vaccine = 10.36, rate placebo = 11.68, difference = 1.32, 95% CI = 0.74 to 1.90, Figure 3, B), cervical definitive therapy (23.0% reduction, 95% CI = 14.2% to 31.0%, rate vaccine = 1.97, rate placebo = 2.56, difference = 0.59, 95% CI = 0.35 to 0.83, Figure 4, A), and procedures for external genital lesions (28.3% reduction, 95% CI = 14.5% to 40.0%, Figure 4, B), with the exception of high-grade squamous intraepithelial lesions (Figure 3, B). No Pap diagnoses of adenocarcinoma and squamous cell carcinoma were observed.
We summarized the efficacy of the vaccine in the negative to 14 HPV types and ITT populations in terms of risk reduction, or risk difference, by subtracting the rate in the vaccine group from the rate in the placebo group. As shown in Table 4, vaccination of 100 000 HPV-naive (negative to 14 HPV types population) or 100 000 mixed HPV-naive and HPV-infected women (ITT population) would prevent a similar number of CIN3 and AIS lesions, abnormal Pap results, and procedures (for cervical or external genital lesions) over 1 year in both populations, irrespective of the HPV type involved.
Number of disease cases prevented annually per 100 000 women*
| Vaccine group | Placebo group | |||||
| Endpoint and population | No. of women | Rate† | No. of women | Rate† | Difference‡ (95% CI) | No. of disease cases prevented annually per 100 000 vaccinated women (95% CI) |
| Negative to 14 HPV types population§ | ||||||
| Any CIN (CIN1–3 or AIS) | 4616 | 1.68 | 4680 | 2.39 | 0.71 (0.40 to 1.02) | 710 (400 to 1020) |
| Any CIN3 or AIS | 4616 | 0.22 | 4680 | 0.39 | 0.17 (0.05 to 0.28) | 170 (50 to 280) |
| Any Pap test abnormality | 4616 | 6.65 | 4679 | 8.03 | 1.38 (0.76 to 1.99) | 1380 (760 to 1990) |
| Any colposcopy | 4616 | 5.47 | 4680 | 6.82 | 1.35 (0.80 to 1.90) | 1350 (800 to 1900) |
| Any cervical biopsy examination | 4616 | 4.63 | 4680 | 5.94 | 1.30 (0.80 to 1.81) | 1300 (800 to 1810) |
| Any cervical definitive therapy | 4616 | 0.79 | 4680 | 1.37 | 0.58 (0.36 to 0.80) | 580 (360 to 800) |
| Any genital wart, VIN1–3, or VaIN1–3 | 4689 | 0.35 | 4735 | 1.38 | 1.02 (0.82 to 1.22) | 1020 (820 to 1220) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 1462 | 1.53 | 1473 | 2.70 | 1.17 (0.60 to 1.74) | 1170 (600 to 1740) |
| ITT population‖ | ||||||
| Any CIN (CIN1–3 or AIS) | 8562 | 3.39 | 8598 | 4.19 | 0.80 (0.48 to 1.12) | 800 (480 to 1120) |
| Any CIN3 or AIS | 8562 | 0.81 | 8598 | 0.98 | 0.18 (0.03 to 0.33) | 180 (30 to 330) |
| Any Pap test abnormality | 8557 | 10.36 | 8587 | 11.68 | 1.32 (0.74 to 1.90) | 1320 (740 to 1900) |
| Any colposcopy | 8565 | 9.59 | 8600 | 10.87 | 1.28 (0.73 to 1.83) | 1280 (730 to 1830) |
| Any cervical biopsy examination | 8565 | 8.13 | 8600 | 9.28 | 1.15 (0.65 to 1.65) | 1150 (650 to 1650) |
| Any cervical definitive therapy | 8565 | 1.97 | 8600 | 2.56 | 0.59 (0.35 to 0.83) | 590 (350 to 830) |
| Any genital wart, VIN1–3, or VaIN1–3 | 8689 | 0.76 | 8702 | 1.59 | 0.83 (0.66 to 1.00) | 830 (660 to 1000) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 2673 | 2.50 | 2672 | 3.49 | 0.99 (0.48 to 1.50) | 990 (480 to 1500) |
| Vaccine group | Placebo group | |||||
| Endpoint and population | No. of women | Rate† | No. of women | Rate† | Difference‡ (95% CI) | No. of disease cases prevented annually per 100 000 vaccinated women (95% CI) |
| Negative to 14 HPV types population§ | ||||||
| Any CIN (CIN1–3 or AIS) | 4616 | 1.68 | 4680 | 2.39 | 0.71 (0.40 to 1.02) | 710 (400 to 1020) |
| Any CIN3 or AIS | 4616 | 0.22 | 4680 | 0.39 | 0.17 (0.05 to 0.28) | 170 (50 to 280) |
| Any Pap test abnormality | 4616 | 6.65 | 4679 | 8.03 | 1.38 (0.76 to 1.99) | 1380 (760 to 1990) |
| Any colposcopy | 4616 | 5.47 | 4680 | 6.82 | 1.35 (0.80 to 1.90) | 1350 (800 to 1900) |
| Any cervical biopsy examination | 4616 | 4.63 | 4680 | 5.94 | 1.30 (0.80 to 1.81) | 1300 (800 to 1810) |
| Any cervical definitive therapy | 4616 | 0.79 | 4680 | 1.37 | 0.58 (0.36 to 0.80) | 580 (360 to 800) |
| Any genital wart, VIN1–3, or VaIN1–3 | 4689 | 0.35 | 4735 | 1.38 | 1.02 (0.82 to 1.22) | 1020 (820 to 1220) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 1462 | 1.53 | 1473 | 2.70 | 1.17 (0.60 to 1.74) | 1170 (600 to 1740) |
| ITT population‖ | ||||||
| Any CIN (CIN1–3 or AIS) | 8562 | 3.39 | 8598 | 4.19 | 0.80 (0.48 to 1.12) | 800 (480 to 1120) |
| Any CIN3 or AIS | 8562 | 0.81 | 8598 | 0.98 | 0.18 (0.03 to 0.33) | 180 (30 to 330) |
| Any Pap test abnormality | 8557 | 10.36 | 8587 | 11.68 | 1.32 (0.74 to 1.90) | 1320 (740 to 1900) |
| Any colposcopy | 8565 | 9.59 | 8600 | 10.87 | 1.28 (0.73 to 1.83) | 1280 (730 to 1830) |
| Any cervical biopsy examination | 8565 | 8.13 | 8600 | 9.28 | 1.15 (0.65 to 1.65) | 1150 (650 to 1650) |
| Any cervical definitive therapy | 8565 | 1.97 | 8600 | 2.56 | 0.59 (0.35 to 0.83) | 590 (350 to 830) |
| Any genital wart, VIN1–3, or VaIN1–3 | 8689 | 0.76 | 8702 | 1.59 | 0.83 (0.66 to 1.00) | 830 (660 to 1000) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 2673 | 2.50 | 2672 | 3.49 | 0.99 (0.48 to 1.50) | 990 (480 to 1500) |
A subject is counted only once within each applicable row. CI = confidence interval; CIN = cervical intraepithelial neoplasia; HPV = human papillomavirus; ITT = intention to treat; Pap = Papanicolaou; VaIN = vaginal intraepithelial neoplasia; VIN = vulvar intraepithelial neoplasia.
The rates were taken directly from the number of women with a lesion that qualified as an endpoint observed per 100 person-years at risk in each treatment group and were used to estimate the number of cases of disease prevented annually per 100 000 vaccinated women.
Difference equals the rate in the placebo group minus the rate in the vaccine group.
This population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and, at enrollment, were seronegative and DNA negative to each of HPV6, 11, 16, and 18; were DNA negative to all 10 nonvaccine HPV types, including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59; and had a normal Pap test result.
Intention-to-treat population was all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, regardless of the presence of HPV infection or HPV-related disease at enrollment.
Number of disease cases prevented annually per 100 000 women*
| Vaccine group | Placebo group | |||||
| Endpoint and population | No. of women | Rate† | No. of women | Rate† | Difference‡ (95% CI) | No. of disease cases prevented annually per 100 000 vaccinated women (95% CI) |
| Negative to 14 HPV types population§ | ||||||
| Any CIN (CIN1–3 or AIS) | 4616 | 1.68 | 4680 | 2.39 | 0.71 (0.40 to 1.02) | 710 (400 to 1020) |
| Any CIN3 or AIS | 4616 | 0.22 | 4680 | 0.39 | 0.17 (0.05 to 0.28) | 170 (50 to 280) |
| Any Pap test abnormality | 4616 | 6.65 | 4679 | 8.03 | 1.38 (0.76 to 1.99) | 1380 (760 to 1990) |
| Any colposcopy | 4616 | 5.47 | 4680 | 6.82 | 1.35 (0.80 to 1.90) | 1350 (800 to 1900) |
| Any cervical biopsy examination | 4616 | 4.63 | 4680 | 5.94 | 1.30 (0.80 to 1.81) | 1300 (800 to 1810) |
| Any cervical definitive therapy | 4616 | 0.79 | 4680 | 1.37 | 0.58 (0.36 to 0.80) | 580 (360 to 800) |
| Any genital wart, VIN1–3, or VaIN1–3 | 4689 | 0.35 | 4735 | 1.38 | 1.02 (0.82 to 1.22) | 1020 (820 to 1220) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 1462 | 1.53 | 1473 | 2.70 | 1.17 (0.60 to 1.74) | 1170 (600 to 1740) |
| ITT population‖ | ||||||
| Any CIN (CIN1–3 or AIS) | 8562 | 3.39 | 8598 | 4.19 | 0.80 (0.48 to 1.12) | 800 (480 to 1120) |
| Any CIN3 or AIS | 8562 | 0.81 | 8598 | 0.98 | 0.18 (0.03 to 0.33) | 180 (30 to 330) |
| Any Pap test abnormality | 8557 | 10.36 | 8587 | 11.68 | 1.32 (0.74 to 1.90) | 1320 (740 to 1900) |
| Any colposcopy | 8565 | 9.59 | 8600 | 10.87 | 1.28 (0.73 to 1.83) | 1280 (730 to 1830) |
| Any cervical biopsy examination | 8565 | 8.13 | 8600 | 9.28 | 1.15 (0.65 to 1.65) | 1150 (650 to 1650) |
| Any cervical definitive therapy | 8565 | 1.97 | 8600 | 2.56 | 0.59 (0.35 to 0.83) | 590 (350 to 830) |
| Any genital wart, VIN1–3, or VaIN1–3 | 8689 | 0.76 | 8702 | 1.59 | 0.83 (0.66 to 1.00) | 830 (660 to 1000) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 2673 | 2.50 | 2672 | 3.49 | 0.99 (0.48 to 1.50) | 990 (480 to 1500) |
| Vaccine group | Placebo group | |||||
| Endpoint and population | No. of women | Rate† | No. of women | Rate† | Difference‡ (95% CI) | No. of disease cases prevented annually per 100 000 vaccinated women (95% CI) |
| Negative to 14 HPV types population§ | ||||||
| Any CIN (CIN1–3 or AIS) | 4616 | 1.68 | 4680 | 2.39 | 0.71 (0.40 to 1.02) | 710 (400 to 1020) |
| Any CIN3 or AIS | 4616 | 0.22 | 4680 | 0.39 | 0.17 (0.05 to 0.28) | 170 (50 to 280) |
| Any Pap test abnormality | 4616 | 6.65 | 4679 | 8.03 | 1.38 (0.76 to 1.99) | 1380 (760 to 1990) |
| Any colposcopy | 4616 | 5.47 | 4680 | 6.82 | 1.35 (0.80 to 1.90) | 1350 (800 to 1900) |
| Any cervical biopsy examination | 4616 | 4.63 | 4680 | 5.94 | 1.30 (0.80 to 1.81) | 1300 (800 to 1810) |
| Any cervical definitive therapy | 4616 | 0.79 | 4680 | 1.37 | 0.58 (0.36 to 0.80) | 580 (360 to 800) |
| Any genital wart, VIN1–3, or VaIN1–3 | 4689 | 0.35 | 4735 | 1.38 | 1.02 (0.82 to 1.22) | 1020 (820 to 1220) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 1462 | 1.53 | 1473 | 2.70 | 1.17 (0.60 to 1.74) | 1170 (600 to 1740) |
| ITT population‖ | ||||||
| Any CIN (CIN1–3 or AIS) | 8562 | 3.39 | 8598 | 4.19 | 0.80 (0.48 to 1.12) | 800 (480 to 1120) |
| Any CIN3 or AIS | 8562 | 0.81 | 8598 | 0.98 | 0.18 (0.03 to 0.33) | 180 (30 to 330) |
| Any Pap test abnormality | 8557 | 10.36 | 8587 | 11.68 | 1.32 (0.74 to 1.90) | 1320 (740 to 1900) |
| Any colposcopy | 8565 | 9.59 | 8600 | 10.87 | 1.28 (0.73 to 1.83) | 1280 (730 to 1830) |
| Any cervical biopsy examination | 8565 | 8.13 | 8600 | 9.28 | 1.15 (0.65 to 1.65) | 1150 (650 to 1650) |
| Any cervical definitive therapy | 8565 | 1.97 | 8600 | 2.56 | 0.59 (0.35 to 0.83) | 590 (350 to 830) |
| Any genital wart, VIN1–3, or VaIN1–3 | 8689 | 0.76 | 8702 | 1.59 | 0.83 (0.66 to 1.00) | 830 (660 to 1000) |
| Any procedure for genital warts, VIN1–3, or VaIN1–3 | 2673 | 2.50 | 2672 | 3.49 | 0.99 (0.48 to 1.50) | 990 (480 to 1500) |
A subject is counted only once within each applicable row. CI = confidence interval; CIN = cervical intraepithelial neoplasia; HPV = human papillomavirus; ITT = intention to treat; Pap = Papanicolaou; VaIN = vaginal intraepithelial neoplasia; VIN = vulvar intraepithelial neoplasia.
The rates were taken directly from the number of women with a lesion that qualified as an endpoint observed per 100 person-years at risk in each treatment group and were used to estimate the number of cases of disease prevented annually per 100 000 vaccinated women.
Difference equals the rate in the placebo group minus the rate in the vaccine group.
This population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and, at enrollment, were seronegative and DNA negative to each of HPV6, 11, 16, and 18; were DNA negative to all 10 nonvaccine HPV types, including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59; and had a normal Pap test result.
Intention-to-treat population was all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, regardless of the presence of HPV infection or HPV-related disease at enrollment.
In both populations, coinfections (in the same lesion or in different lesions) with an HPV type in the vaccine and with an HPV type that is not included in the vaccine was more common in the placebo group than in the vaccine group (as illustrated in Figure 5). However, it should be noted that this is an underestimation of coinfection because we only tested for 14 of 40 genital HPV types. In the ITT population, there were a total of 284 women with CIN3 in the placebo group and 237 women with CIN3 in the vaccine groups, of whom, 183 (in the placebo group) and 100 (in the vaccine group) had a CIN3 lesion that was associated with HPV6, 11, 16, and/or 18. As illustrated in Figure 5, one cannot subtract the number of women with a CIN1, 2, or 3 lesion that is associated with HPV6, 11, 16, and/or 18 from the total number of women with a CIN3 lesion to obtain the number of women with a CIN3 lesion caused by a HPV type not included in the vaccine. Such a subtraction does not account for women with coinfections (ie, women having both vaccine and nonvaccine type in the CIN3 lesion). There were 83 women with a CIN3 lesion in the placebo group and 44 women with a CIN3 lesion in the vaccine group that had both a vaccine and a nonvaccine HPV type.
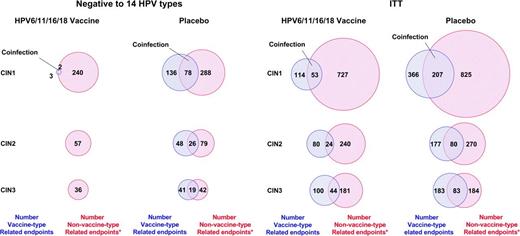
Illustration of vaccine-type and nonvaccine human papillomavirus (HPV)–type coinfections among cervical intraepithelial neoplasia (CIN) lesions. The vaccine and nonvaccine HPV types may have been detected in the same lesion or different lesions. The negative to 14 HPV types population was restricted to subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and had follow-up, and who at enrollment were seronegative and DNA negative to HPV6, 11, 16, and 18; were DNA negative to all 10 of the nonvaccine HPV types (including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59); and had a normal Papanicolaou test result. The intention-to-treat (ITT) population was composed of all subjects who received at least one injection of HPV6/11/16/18 vaccine or placebo and returned for follow-up visits, regardless of the presence of HPV infection or HPV-related disease at enrollment. Asterisk indicates that the lesion was positive for at least one tested nonvaccine type (including HPV31, 33, 35, 39, 45, 51, 52, 56, 58, and 59) or the lesion was negative for all 14 tested HPV types (including HPV6, 11, 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59).
Discussion
Our results demonstrate that prophylactic administration of a quadrivalent HPV vaccine against HPV types 6, 11, 16, and 18 was highly efficacious in preventing cervical, vulvar, and vaginal intraepithelial neoplasia and genital warts in women who were negative to 14 HPV types (12 high-risk and two low-risk types) and who had normal cytology at baseline; that is, these women approximated HPV-unexposed women in this analysis. Prophylactic vaccination was 95%–100% effective in reducing HPV16/18-related high-grade cervical, vulvar, and vaginal lesions, including CIN3, AIS, VIN2–3, and VaIN2–3, and 97% effective in reducing HPV6/11-related genital warts. In addition, the HPV6/11/16/18 vaccine was very efficacious in reducing the number of abnormal Pap results that were related to HPV16 and HPV18, of abnormal Pap results irrespective of causal HPV type, and of diagnostic and treatment procedures related to cervical, vulvar, and vaginal intraepithelial neoplasia and genital warts, irrespective of the causal HPV type. These are, to our knowledge, the first results on the overall population impact beyond cervical disease for any HPV vaccine to date (31).
As expected, the prophylactic efficacy of the vaccine was lower when all genital lesions irrespective of HPV causal type were considered. For CIN3 and AIS, which are the immediate precursors of invasive squamous cell carcinoma and adenocarcinoma, the observed end-of-study efficacy was 43% in the negative to 14 HPV types population. We found that HPV16 or HPV18 DNA could be identified in 177 (62%) of the 284 CIN3 lesions in the placebo group. However, this efficacy of 43% was observed with only 3.6 years of follow-up and the data indicate that it might increase with time. As shown in Figure 2, C, the incidence of any CIN3 and AIS lesion continued to increase in the placebo group but had reached a plateau in the vaccine group. It is not possible, therefore, to determine exactly the overall impact of the vaccine on any CIN3 or AIS lesion with the clinical trial data that are available to date.
This study has several limitations. For example, our estimates of vaccine efficacy for CIN of any grade in the negative to 14 HPV types population may be a substantial underestimation, because our population was negative to only 14 of the approximately 40 HPV types that are known to infect the genital tract. For example, of the approximately 26 HPV types that were not tested for, some, such as HPV53 and HPV66, are found in 9%–10% of low-grade squamous intraepithelial lesions (32). Therefore, there may have been prevalent HPV infections or disease that was not detected by the day 1 Pap or PCR testing. The observed reductions in procedures may also be underestimated by our data, as the analyses reflect a single treatment for each endpoint. For example, recurrence rates after definitive or excisional treatment of genital warts range from 5% to 65% (33,34). As expected, vaccine efficacy in the ITT population, which included all women regardless of the presence of HPV infection or HPV-related disease at baseline, was lower than that in the negative to 14 HPV types population. This ITT population approximated sexually active women, and so this analysis investigated the vaccine's impact in such women. However, another limitation is that the ITT population is not entirely representative of the general population of women aged 16–26 years because of the exclusion and inclusion criteria of the trials (eg, low lifetime number of sex partners and no past history of abnormal Pap test or external genital abnormality), and our results, therefore, cannot be generalized to other populations with different background risks. In addition, the 6-month screening intervals in the FUTURE I trial does not correspond to the usual diagnostic process of an opportunistic screening program; thus, we were more likely to detect incipient and transient lesions, many of which would not evolve to an invasive cancer. However, results in the FUTURE I trial were similar to those in the FUTURE II trial, which included annual screening. The efficacy (ie, percent reduction) for any CIN3 or AIS lesion in the ITT population was a statistically significant 18% (95% CI = 2% to 31%). As illustrated in Figure 2, D, the efficacy estimates increased with longer follow-up. These findings underscore the importance of administering the HPV vaccine before initiation of sexual activity to have a greater public health impact.
We analyzed the difference in efficacy within the two populations in terms of risk reduction or prevented risk (Table 4). The risk reduction for CIN3 and AIS irrespective of causal HPV type in the negative to 14 HPV types population was estimated as 0.17 per 100 person-years at risk. In the ITT population, the risk reduction for CIN3 and AIS irrespective of causal HPV type was 0.18 per 100 person-years at risk. Even though the vaccine efficacy estimates were different (the prevented fraction of CIN3 and AIS was 17% in the ITT population and 44% in the negative to 14 HPV types population), the risk reduction estimates appear to be similar, indicating that if we vaccinated 100 000 HPV-naive women or 100 000 mixed HPV-naive and HPV-infected women, we would prevent approximately 200 CIN3 and AIS lesions over the next year in both situations. For disease that is caused by HPV6, 11, 16, or 18, vaccination of the ITT population doubled the number of CIN3 lesions prevented in the ITT population compared with that in the negative to 14 HPV types population (ie, 83 vs 41 lesions) (Figure 5 and Table 2). The additional lesions prevented in the ITT population come mainly from women who were infected at baseline with one, two, or three vaccine HPV types and who benefited from protection against the HPV type(s) to which they were naive. However, the number of lesions prevented for nonvaccine HPV types was relatively the same in both populations. Concerning cross-protection, we have previously shown that vaccination of the negative to 14 HPV types population reduced the incidence of high-grade lesions (ie, CIN2-3 and AIS) associated with the 10 tested nonvaccine HPV types by 32.5% (95% CI = 6.0% to 51.9%) (18,19). In the ITT population, reductions in CIN2-3 and AIS lesions associated with the 10 tested nonvaccine HPV types were not statistically different between vaccine and placebo recipients (18,19). These observations are the primary reason for recommending catch-up programs in young women for a limited time period after the introduction of a new vaccine. However, it is important to note that a comparable risk reduction between HPV-naive and ITT populations might not hold true for populations of older women or in populations with a lifetime number of sex partners that is greater than four. Decisions on catch-up vaccination will be dependent on the prevailing sexual practices in the young populations, as has been recently reported from the Icelandic subgroups of the FUTURE II trial (31).
Vaccine effectiveness in the ITT population was driven by the prevalence of HPV infection before vaccination. Most cases of disease that were observed in the vaccine group of the ITT population were caused by infections that were present at baseline. The HPV6/11/16/18 vaccine has been shown to not affect the course of already established infections (7,8), although the HPV6/11/16/18 vaccine has recently been shown to induce an anamnestic response in women who are seropositive before vaccination (35). In addition, the HPV6/11/16/18 vaccine has been shown to prevent reinfection or reactivation of disease that is related to a vaccine HPV type. For example, women who had cleared an HPV16 infection in the past were protected from developing HPV16-related disease (36). The higher efficacy in the ITT population that was observed for external genital lesions than for cervical disease is likely attributable to the study design. Although women with any history of cervical disease (eg, abnormal Pap results and CIN) were excluded from trial enrollment, those with abnormal Pap results or CIN that was detected at the enrollment visit were not excluded. In contrast, those who had genital warts that were detected at the enrollment visit were excluded. Unlike cervical disease, which can be caused by several different HPV types, genital warts are primarily associated with HPV6 and HPV11 (37).
Coinfection with a vaccine HPV type and a nonvaccine HPV type was more common in the placebo group than in the vaccine group. Assignment of causality in the case of multiple HPV infections is not straightforward. Population-based studies have shown that women in the age range of the clinical trial population (ie, age 16–26 years) have the highest prevalence of any HPV type and are more likely to have multiple high-risk HPV infections, including those that are less pathogenic than HPV16 and HPV18 and more likely to regress (38). In the ITT population, if the number of women with CIN lesions that had both a vaccine and a nonvaccine HPV type detected in the lesion was subtracted from the total number of women with a nonvaccine HPV type–related lesion, then the vaccine group would have a higher number of nonvaccine type–related endpoints than the placebo group (Figure 5). This result is not unexpected because the vaccine group should be protected from disease related to HPV6, 11, 16, and/or 18, so that a disproportionately smaller number of lesions with a vaccine HPV type should be diagnosed in the vaccine group than in the placebo group. This “unmasking effect” (18,39) is not a result of type replacement, that is, the potential for other HPV types to become more widespread or more virulent as protection against HPV16 and 18 increases after vaccination. Type replacement could not be observed in the context of a 4-year clinical trial. Papillomaviruses have a high genetic stability and have little or no capacity for mutation (ie, as few as one mutation or single nucleotide substitution in 300 base pairs over several thousands of years) (40). Nonetheless, there are several ongoing surveillance studies designed to assess HPV type replacement (41,42).
In conclusion, our results provide strong evidence to suggest that the ongoing HPV vaccination programs in adolescent girls and young women will result within a few years in a notable reduction of genital warts, cervical cytological abnormalities, and diagnostic and therapeutic procedures related to precursor lesions in the cervix, vulva, and vagina. It is anticipated that these reductions will eventually translate into lower rates of cancer of the cervix, vulva, and vagina and lower rates of genital warts. Ultimately, the population-based impact of HPV vaccines will require longer term surveillance beyond the present clinical trials. Several non–placebo-controlled postmarketing studies are ongoing (41,42).
Funding
Merck and Co, Inc.
References
As corresponding author, Dr Muñoz assumes full responsibility for the overall content and integrity of the manuscript.
N. Muñoz has received lecture fees, advisory board fees, and consultancy fees from Merck and Co, Inc, and Sanofi Pasteur MSD. S. K. Kjaer has received consultancy fees and has received funding through her institution to conduct human papillomavirus (HPV) vaccine studies for Sanofi Pasteur MSD and Digene. K. Sigurdsson received consultancy fees from Merck and Co, Inc, as a steering group member of Females United to Unilaterally Reduce Endo/Ectocervical Disease trial II. O.-E. Iversen has received lecture fees from Merck and Co, Inc, and GlaxoSmithKline. M. Hernandez-Avila has received advisory board fees and grant support from Merck and Co, Inc. C. M. Wheeler has received funding through her institution for reagents and equipment from Roche Molecular Systems in support of HPV genotyping studies and to conduct HPV vaccine studies for GlaxoSmithKline. G. Perez has received lecture fees and consultancy fees from Merck and Co, Inc, and Sanofi Pasteur MSD and is now an employee of Merck and Co, Inc. D. R. Brown has received royalties, consulting fees, and research support from Merck and Co, Inc. P. Garcia is a member of the advisory board for Merck and Co, Inc. K. Ault has received consultancy and advisory board fees from Merck and Co, Inc, and has received funding through his institution to conduct HPV vaccine studies for GlaxoSmithKline. S. Garland has received advisory board fees and grant support from Commonwealth Serum Laboratories and GlaxoSmithKline and lecture fees from Merck and Co, Inc. S. Leodolter has received lecture fees from Merck and Co, Inc, and Sanofi Pasteur MSD. S. E. Olsson has received lecture fees from Merck and Co, Inc, and given lectures sponsored by Merck and Co, Inc. D. G. Ferris has received consultancy fees and funding through his institution to conduct HPV vaccine studies for GlaxoSmithKline and lecture fees from Merck and Co, Inc. J. Paavonen has received consultancy fees and travel grants from Merck and Co, Inc, and GlaxoSmithKline. M. Steben has received lecture fees and grant support from Merck and Co, Inc. F. X. Bosch has received lecture fees from Merck and Co, Inc, and GlaxoSmithKline and has received funding through his institution to conduct HPV vaccine studies for GlaxoSmithKline and Sanofi Pasteur MSD and has received unrestricted research grants for epidemiological studies from GlaxoSmithKline and Sanofi Pasteur MSD. J. Dillner has received consultancy fees, lecture fees, and research grants from Merck and Co, Inc, and Sanofi Pasteur MSD. W. K. Huh has received lectures fees and advisory board fees from Merck and Co, Inc, and research and consultancy fees from GlaxoSmithKline. E. Joura has received lecture fees from Merck and Co, Inc, Sanofi Pasteur MSD, and GlaxoSmithKline. R. Kurman reports that Johns Hopkins has received financial support from Merck and Co, Inc, related to this project. S. Majewski has received lecture fees and advisory board fees from Merck and Co, Inc. E. R. Myers has served on the steering committees for Gardasil clinical trials and has been reimbursed by Merck and Co, Inc; he has served as a consultant and has received research funding from GlaxoSmithKline; and he has also served as a consultant for non–HPV vaccine–related work for GlaxoSmithKline. Additionally, S.-E. Olsson, C. M. Wheeler, M. Hernandez-Avila, L. L. Villa, O.-E. Iverson, G. Tang, X. Bosch, J. Paavonen, J. Dillner, E. H. Tay, K. Ault, S. Leodolter, E. A. Joura, S. K. Kjaer, G. Perez, D. G. Ferris, K. Sigurdsson, M. Steben, W. K. Huh, L. Koutsky, S. Garland, and D. R. Brown have received funding through their institutions to conduct HPV vaccine studies for Merck and Co, Inc. F. J. Taddeo, C. Roberts, A. Tadesse, J. T. Bryan, L. Lupinacci, K. Giacoletti, H. L. Sings, M. K. James, T. M. Hesley, E. Barr, and R. M. Haupt are employees of Merck and Co, Inc, and potentially own stock and/or stock options in the company.
The studies were designed by the sponsor (Merck and Co, Inc, Whitehouse Station, NJ) in collaboration with a steering committee (NM, SKK, KS, O-EI, MH-A, G.P, DB, LAK, EHT, PJG, KAA, S-EO, DGF, JP, MS, FXB, JD, RJK, SM, ERM, and LLV) and an external data and safety monitoring board. The sponsor collated the data, monitored the conduct of the study, performed the statistical analysis, and coordinated the writing of the manuscript with all authors. Only persons listed as authors took part in writing the manuscript. The authors were actively involved in the collection, analysis, or interpretation of the data and the revising of the manuscript for intellectual content. They also approved the final manuscript.
We thank Kathy Harkins, Carolyn Maass, MaryAnne Rutkowski, and Shuang Lu for statistical and programming support. We also thank all study personnel and participants.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}