





Abstract
Aims To investigate the efficacy and outcome of emergency percutaneous coronary interventions (PCI) in patients with stent thrombosis.
Methods and results Between 1995 and 2003, 6058 patients underwent bare-metal stent implantation, of which 95 (1.6%) patients suffered from stent thrombosis. The timing of stent thrombosis was acute in 10 (11%), subacute in 61 (64%), and late in 24 (25%) patients. Procedural and clinical outcomes of emergency PCI for treatment of stent thrombosis were investigated. Emergency PCI was successful in 86 (91%), complicated by death in 2 (2%), and coronary artery bypass grafting in 2 (2%) patients. Myocardial infarction occurred in 77 (81%) patients with a peak creatine kinase level of 1466±1570 U/L. Left ventricular ejection fraction declined from 0.54±0.19 prior to 0.48±0.16 (P<0.05) at the time of stent thrombosis after emergency PCI. A 6 month major adverse clinical events comprised death (11%), reinfarction (16%), and recurrent stent thrombosis (12%) after emergency PCI. Multivariable logistic regression analysis identified the achievement of TIMI 3 flow (OR=0.1, CI 95% 0.01–0.54, P<0.001) and diameter stenosis <50% (OR=0.06, CI 95% 0.01–0.32, P<0.001) during emergency PCI to be independently associated with a reduced risk of cardiac death. Recurrent stent thrombosis was independently predicted by the omission of abciximab (OR=4.3, CI 95% 1.1–17.5).
Conclusion Emergency PCI for treatment of stent thrombosis effectively restores vessel patency and flow. Patients presenting with stent thrombosis are at risk for recurrent myocardial infarction and recurrent stent thrombosis.
Introduction
Stents have improved the safety and efficacy of percutaneous coronary interventions (PCI) by reducing abrupt or threatened vessel closure1,2 and by reducing restenosis3,4 compared with conventional balloon angioplasty. In addition, coronary vasomotion has been found intact after stent implantation5 and long-term clinical and angiographic follow-up have attested to the durability of their action.6
Notwithstanding, coronary stent thrombosis has remained a serious complication of PCI.7 Although early aggressive anticoagulation schemes were associated with unacceptably high rates of stent thrombosis and bleeding complications,3,4,8 the advent of dual antiplatelet therapy had salutary effects on both adverse events.7,9–12 Despite dual antiplatelet therapy, stent thrombosis persists at a rate of 0.5–2%13–16 in elective cases, and up to 6% in patients with acute coronary syndromes.15,17 Furthermore, longer stent length, number of implanted stents,13,15 stent malapposition,18 residual dissections,13,19 reduced TIMI flow,19 gene polymorphisms,20 and resistance to the antiplatelet effects of acetylsalicylic acid (ASA)21 and potentially thienopyridines22,23 have been reported to increase the risk for stent thrombosis.
The clinical sequelae of stent thrombosis including death and myocardial infarction are grave13,15 and demand aggressive therapeutic interventions. Although emergency PCI is commonly employed, the efficacy of the procedure and long-term outcome of patients in this setting is not well established. Previous studies reported only a limited efficacy of PCI and intracoronary fibrinolysis,24 but a possibly favourable effect of the glycoprotein IIb/IIIa antagonist abciximab for the treatment of stent thrombosis.25 The purpose of the present study was to investigate the efficacy of emergency PCI in patients with stent thrombosis and to identify predictors of adverse outcome in the largest consecutive patient population reported to date.
Methods
Study design
All patients presenting with stent thrombosis undergoing emergency PCI between 1995 and 2003 were included in the analysis. Patients with stent thrombosis were identified in our database, which is kept abreast by active follow-up. Medical records and angiograms of all patients with stent thrombosis were analysed. The study, which complied with the Declaration of Helsinki, was approved by the local ethics committee, and written informed consent was obtained from patients included in the study. Patients had to fulfil clinical and angiographic criteria of ST. Clinical criteria consisted of the acute onset of chest pain persisting for >15 min and/or accompanied by ST segment elevation or depression of at least 1 mm in two contiguous leads in the distribution of the target vessel. All patients with the clinical suspicion of stent thrombosis underwent immediate coronary angiography to confirm the diagnosis followed by PCI. Angiographic criteria of stent thrombosis consisted of partial or complete occlusion within the previously implanted stent with evidence of fresh thrombus. Only patients with angiographically confirmed stent thrombosis were included in the present study. The intervention in the setting of stent thrombosis was termed emergency PCI to clearly distinguish it from primary PCI in the setting of acute ST segment elevation myocardial infarction.
Emergency PCI for treatment of stent thrombosis
All patients presenting with stent thrombosis were immediately brought to the catheterization laboratory. ASA was administered intravenously (250–500 mg) in the exceptional patient not taking ASA (100 mg). The use of a glycoprotein IIb/IIIa antagonist was left to the discretion of the operator. Intravenous weight-adjusted heparin was used to achieve an activated clotting time≥250 s. Recanalization of the occluded target vessel was performed in most cases with a recanalization wire and a low-profile balloon. Additional stent implantation was performed if residual dissections or a significant (>50%, visually estimated) stenosis was present. Distal embolization protection devices were not routinely used during this period. The post-procedural treatment consisted of dual antiplatelet therapy with daily ASA and a thienopyridine for at least 1 month.
Definitions, clinical follow-up, and clinical endpoints
Stent thrombosis was defined as sudden onset of typical chest pain with electrocardiographic changes, indicating acute ischaemia in the distribution of the target vessel. Acute stent thrombosis was defined as occurring during the 24 h after the intervention, subacute between 1 and 30 days, and late beyond 30 days after the intervention. Stent thrombosis was angiographically confirmed in all patients included in the present study. Angiographic definition of stent thrombosis was a complete or partial occlusion within the stented segment with evidence of thrombus. Procedural success was defined as normal flow (TIMI 3) with a stenosis <50%. Quantitative coronary analysis of the target vessel was performed in all cases on the angiogram of the index procedure and the angiogram at the time of stent thrombosis. Major adverse clinical events were assessed at the time of hospital discharge and 6 months after the intervention using a questionnaire. Long-term follow-up was completed in 98% of cases. Two patients had moved abroad and could not be located. Myocardial infarction was defined as an elevation of creatine kinase twice the upper limit of normal value and three times the upper limit of normal value of CK-MB fraction.
Statistical analysis
Continuous data were expressed as mean±standard deviation. Continuous variables were compared using the Student's t-test, and paired categorical variables were compared using the test by McNemar. The data analysed were normally distributed. Survival estimates were computed using the Kaplan–Meier method and compared with a log-rank test. Predictors of cardiac death and predictors of recurrent stent thrombosis at 6 months follow-up were assessed with a multivariable logistic regression analysis. First, an univariate analysis was performed with the following variables: age >65 years, gender, ejection fraction <40%, TIMI 3 flow before and after the intervention, use of glycoprotein IIb/IIIa (abciximab and tirofiban) antagonists, residual dissection, stenosis <50% post-PCI, diabetes, and smoking. Then, variables with a P-value <0.15 were entered into the multivariable model. The measure of predictive accuracy was assessed by receiver operating characteristic curve with an area of 0.770. A two-tailed P-value of <0.05 was considered significant. All statistical analyses were performed with the SPSS 10.0.5 program, Chicago, IL, USA.
Results
Incidence of stent thrombosis
Between November 1995 and March 2003, 95 (1.6%) of 6058 patients treated at our institution with bare-metal stents suffered from stent thrombosis. Stent thrombosis occurred after a median of 8 days following bare-metal stent implantation, with the onset ranging from 0 to 639 days. The timing of stent thrombosis was acute in 10 (11%), subacute in 61 (64%), and late in 24 (25%) patients (Figure 1A and B). Seventy (74%) patients suffering from stent thrombosis initially underwent PCI in the setting of an acute coronary syndrome, as opposed to 25 (26%) patients with an elective indication at the time of the initial procedure (Table 1). The angiographic baseline characteristics at the time of the initial procedure are summarized in Table 2. Twenty-two patients (23%) did not take thienopyridines, and five patients took neither ASA nor thienopyridines at the time of stent thrombosis. Fifty-two (55%) patients were treated with a statin at the time of stent thrombosis. Patients suffering from stent thrombosis presented with the diagnosis in our institution in 19% of cases, were referred from another hospital in 65% of cases, and presented on an outpatient basis in 16% of cases.
Procedural results of emergency PCI for treatment of stent thrombosis
All 95 patients presenting with stent thrombosis underwent emergency PCI. The duration of symptom onset to hospitalization in our institution was 170 min (median) and the door-to-balloon time was 40 min (median). Balloon angioplasty was the default treatment strategy in all (100%) patients, followed by implantation of another stent in 36 (38%) patients. Glycoprotein IIb/IIIa (18% tirofiban and 42% abciximab) antagonists were used in 57 (60%) patients, and fibrinolysis was administered in eight (8%) patients prior to the procedure. Thrombotic stent occlusion was complete in 83% and partial in 17% of patients. Emergency PCI for treatment of stent thrombosis was successful in 86 (91%) patients. Reasons for an unsuccessful procedure were an abnormal flow (TIMI 0–2) in nine patients, failure to cross the occluded stent with a guidewire in eight patients, and ostial location with inability to pass a guidewire or balloon in one patient. Angiographic data of emergency PCI for treatment of stent thrombosis are summarized in Table 3. Procedural major adverse cardiac events (MACE) consisted of death in two (2%) and coronary artery bypass grafting in two (2%) patients after unsuccessful recanalization. Myocardial infarction occurred in 77 (81%) patients with a peak creatine kinase level of 1466±1570 U/L (CK-MB 220±206 U/L). Eighteen patients did not develop myocardial infarction owing to an exceedingly short door-to-balloon time of <20 min in eight patients and a partial but not complete thrombotic stent occlusion in 16 (17%) patients. Q-wave myocardial infarction developed in 20 (26%) and non-Q-wave myocardial infarction in 57 (74%) of these patients. Left ventricular ejection fraction significantly decreased from 0.54±0.15 at the time of the initial procedure to 0.49±0.13 (P<0.05) at the time of stent thrombosis. Angiographic analysis revealed a residual dissection proximal or distal to the stent in 23 (24%) patients as a possible cause for the thrombotic occlusion.
Clinical follow-up and predictors for adverse outcome
Clinical outcome at 6 months after emergency PCI for treatment of stent thrombosis is summarized in Table 4. The actuarial freedom from cardiac death and MACE is shown in Figure 2. Multivariable logistic regression analysis identified the achievement of TIMI 3 flow (OR=0.1, CI 95% 0.01–0.54, P<0.001) and diameter stenosis <50% (OR=0.06, CI 95% 0.01–0.32, P<0.001) during emergency PCI to be independently associated with a reduced risk of cardiac death (Figure 3).
Fifteen (16%) patients suffered from reinfarction after emergency PCI for stent thrombosis. This was largely driven by recurrent stent thrombosis of the target lesion in 11 (73%) patients occurring 5.0±8.5 days (median) after emergency PCI. Logistic regression analysis identified the omission of abciximab (OR=4.3, CI 95% 1.1–17.5, P<0.05) during emergency PCI for stent thrombosis as the only independent predictor for recurrent stent thrombosis.
Discussion
The present study summarizes the results of emergency PCI for the treatment of stent thrombosis in the largest patient population reported till date. Emergency PCI was highly effective for recanalization and restoration of TIMI 3 flow in the infarct-related artery. Notwithstanding, stent thrombosis was associated with considerable short- and long-term mortality, an important risk for recurrent myocardial infarction mainly driven by recurrent stent thrombosis, and a significant decline of left ventricular ejection fraction. The use of abciximab was associated with a lower risk for recurrent stent thrombosis. Of note, stent thrombosis after implantation of bare-metal stents occurred late (>30 days) in 25% of cases.
Procedural outcome of emergency PCI for treatment of stent thrombosis
Previous studies investigating reperfusion methods for stent thrombosis showed an unacceptably high failure rate because of residual thrombus following balloon angioplasty alone.24 Even supplementary therapy with intracoronary fibrinolysis showed no clinical benefit.24 In contrast, a small study suggested a benefit of adjunctive therapy with the glycoprotein IIb/IIIa antagonist abciximab in patients with stent thrombosis resulting in improved clinical outcome.25 A recent report of a mechanical thrombectomy device revealed a high procedural success rate in a small patient population,26 and the concomitant use of glycoprotein IIb/IIIa antagonists was associated with a lower incidence of the ‘no reflow’ phenomenon. These observations are in line with our study, where emergency PCI for treatment of stent thrombosis was highly effective in eliminating the thrombotic occlusion and restoring TIMI 3 flow in >90% of patients, especially when applied in conjunction with abciximab.27 In fact, the success rate of emergency PCI for treatment of stent thrombosis in our study mirrors the results of primary PCI in the setting of acute myocardial infarction 28 and should therefore be considered as the therapy of choice in this patient population.
Despite immediate reperfusion therapy by means of emergency PCI, patients with stent thrombosis developed a large myocardial infarction (creatine kinase elevation>5×ULN) in 37 (39%) cases. Although the size of myocardial infarction in our study compares favourably with previous reports29 of infarct size in patients with stent thrombosis, myocardial infarction related to stent thrombosis was associated with a significant decline in left ventricular function. This finding raises concern as left ventricular function has been identified as a strong and consistent predictor of long-term survival following myocardial infarction.30 The significant decline in left ventricular function related to stent thrombosis points to the serious nature of stent thrombosis as a PCI-related adverse event.
Dual antiplatelet therapy consisting of ASA and thienopyridines has been shown to be superior to treatment with aspirin alone and oral anticoagulation in the prevention of death and non-fatal myocardial infarction following coronary stenting.11,16,31 In the era of bare-metal stents, it has been customary to prescribe dual antiplatelet therapy for the duration of 1 month followed by the indefinite treatment with ASA alone. More recently, randomized clinical trials tested the benefit of extended (9–12 months) dual antiplatelet therapy compared with treatment with ASA alone. Both the Clopidogrel for the Reduction of Events During Observation (CREDO) and PCI-CURE, a prospective substudy of the Clopidogrel in Unstable angina Recurrent Events trial, revealed a significantly reduced risk (27–31% relative risk reduction) of adverse ischaemic events in favour of an extended dual antiplatelet regimen following coronary stenting.32,33 In light of these studies and the observation that one-quarter of patients in the present study suffered late (>1 month after PCI) stent thrombosis, extended dual antiplatelet therapy following coronary stenting should be considered to prevent ischaemic events. Similarly, patients who suffered from stent thrombosis are at considerable risk for recurrent stent thrombosis and might therefore benefit from prolonged (6–12 months) dual antiplatelet therapy to prevent recurrent ischemic events.
Prognosis after emergency PCI for stent thrombosis
The 6 month mortality of 11% following emergency PCI for stent thrombosis is similar to the 7–9% mortality following primary PCI in the setting of acute myocardial infarction28 and lower than in previous reports of patients with stent thrombosis.13,15 Multivariable logistic regression analysis revealed that the achievement of TIMI 3 flow during emergency PCI was associated with a reduced risk of cardiac death. This observation corroborates angiographic substudies from thrombolytic30 and primary PCI trials,34 where TIMI 3 flow directly correlated with improved survival. Accordingly, emergency PCI for treatment of stent thrombosis should aim beyond the elimination of the underlying occlusion at restoration of TIMI 3 flow.
Patients undergoing emergency PCI for stent thrombosis were found at considerable risk for recurrent myocardial infarction. This risk was driven in 75% of patients by the occurrence of recurrent stent thrombosis. Logistic regression analysis identified the omission of abciximab as a predictor for recurrent stent thrombosis. These results are in keeping with previous studies reporting an increased risk of stent thrombosis in patients with impaired TIMI flow19 and improved outcome with the use of abciximab.25 The combination of a thrombotic event and impaired flow highlights the demand for an aggressive antithrombotic regimen to prevent future events. Along this line, the use of the glycoprotein IIb/IIIa antagonist abciximab has been shown to reduce the incidence of myocardial infarction/stent thrombosis in the EPISTENT and CAPTURE trials.35,36 Accordingly, glycoprotein IIb/IIIa antagonists should be strongly considered as adjunctive pharmacological treatment in patients undergoing emergency PCI for stent thrombosis to facilitate achievement of TIMI 3 flow and decrease the risk of recurrent stent thrombosis.
Limitations
The present study has several limitations. (i) It is a retrospective analysis with its inherent shortcomings. (ii) Silent stent thrombosis or patients with stent thrombosis not transferred for emergency PCI were not included in the analysis. Accordingly, a somewhat higher incidence of stent thrombosis has to be assumed. In addition, the clinical outcome of patients not immediately transferred for emergency PCI remains unknown. Notwithstanding, the focus of the present study was to analyse the procedural and clinical outcome of patients with stent thrombosis and to identify predictors of adverse outcome. (iii) Intravascular ultrasound was not routinely utilized in patients presenting with stent thrombosis. This precluded the analysis for mechanical causes of stent thrombosis such as inappropriate stent expansion and insufficient stent overlap. (iv) The use of glycoprotein IIb/IIIa antagonists was left to the discretion of the individual operator. The large-scale administration of glycoprotein IIb/IIIa antagonists commenced only in 1998, whereas the study population dates back to late 1995. Selection bias in the use of this medication cannot be ruled out and might have influenced the outcome.
Conclusions
Emergency PCI for treatment of stent thrombosis is highly effective and should be considered as the therapy of choice in this patient population. Patients undergoing emergency PCI for stent thrombosis are at risk for death, recurrent myocardial infarction, and recurrent stent thrombosis. The achievement of TIMI 3 flow is associated with a reduced risk of cardiac death following emergency PCI for treatment of stent thrombosis.
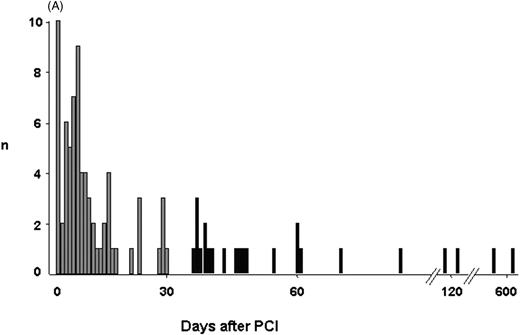
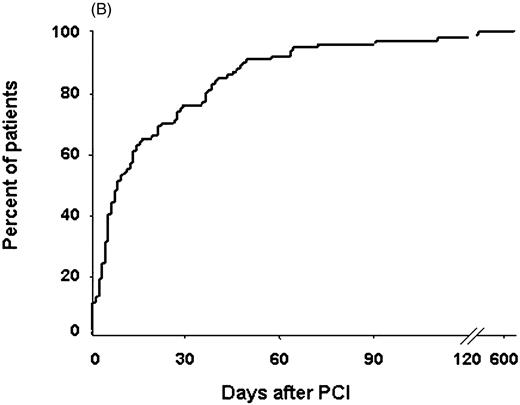
Figure 1 (A) Incidence of stent thrombosis (n=number of stent thromboses per day) following bare-metal stent implantation. Acute and subacute stent thrombosis (≤30 days) are in grey, late stent thrombosis (>30 days) in black. (B) Cumulative incidence of stent thrombosis following bare-metal stent implantation.
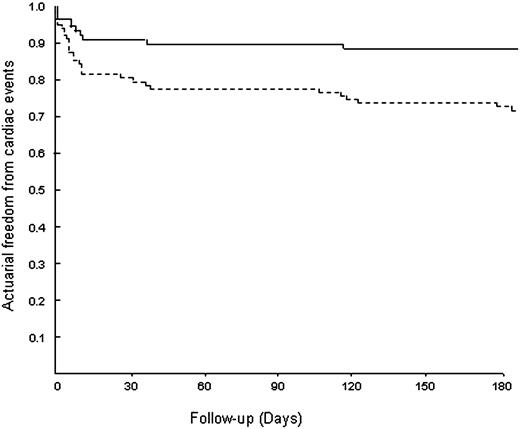
Figure 2 Actuarial freedom from cardiac death (continuous line) and MACE (dashed line) during 6 month follow-up.
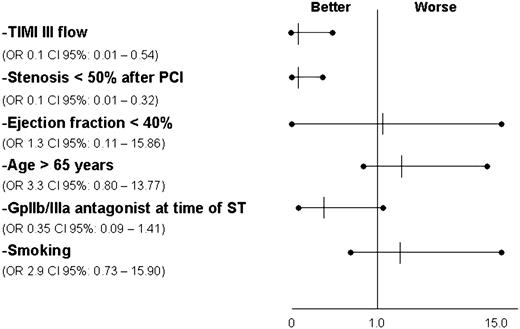
Figure 3 Predictors of cardiac death after emergency PCI for stent thrombosis
Clinical characteristics of patients undergoing emergency PCI for treatment of stent thrombosis
| 95 Patients | |
|---|---|
| Age, mean±SD | 62±12 |
| Male gender, n (%) | 72 (76) |
| Hypertension, n (%) | 43 (45) |
| Family history, n (%) | 18 (19) |
| Smoking, n (%) | 30 (32) |
| Dyslipidaemia, n (%) | 59 (62) |
| Diabetes, n (%) | 23 (24) |
| Indication for PCI, n (%) | |
| Elective | 25 (26) |
| Unstable angina | 32 (34) |
| Acute myocardial infarction | 38 (40) |
| Multivessel disease, n (%) | 54 (57) |
| Thienopyridines, n (%) | |
| Ticlopidine | 13 (14) |
| Clopidogrel | 82 (86) |
| 95 Patients | |
|---|---|
| Age, mean±SD | 62±12 |
| Male gender, n (%) | 72 (76) |
| Hypertension, n (%) | 43 (45) |
| Family history, n (%) | 18 (19) |
| Smoking, n (%) | 30 (32) |
| Dyslipidaemia, n (%) | 59 (62) |
| Diabetes, n (%) | 23 (24) |
| Indication for PCI, n (%) | |
| Elective | 25 (26) |
| Unstable angina | 32 (34) |
| Acute myocardial infarction | 38 (40) |
| Multivessel disease, n (%) | 54 (57) |
| Thienopyridines, n (%) | |
| Ticlopidine | 13 (14) |
| Clopidogrel | 82 (86) |
Clinical characteristics of patients undergoing emergency PCI for treatment of stent thrombosis
| 95 Patients | |
|---|---|
| Age, mean±SD | 62±12 |
| Male gender, n (%) | 72 (76) |
| Hypertension, n (%) | 43 (45) |
| Family history, n (%) | 18 (19) |
| Smoking, n (%) | 30 (32) |
| Dyslipidaemia, n (%) | 59 (62) |
| Diabetes, n (%) | 23 (24) |
| Indication for PCI, n (%) | |
| Elective | 25 (26) |
| Unstable angina | 32 (34) |
| Acute myocardial infarction | 38 (40) |
| Multivessel disease, n (%) | 54 (57) |
| Thienopyridines, n (%) | |
| Ticlopidine | 13 (14) |
| Clopidogrel | 82 (86) |
| 95 Patients | |
|---|---|
| Age, mean±SD | 62±12 |
| Male gender, n (%) | 72 (76) |
| Hypertension, n (%) | 43 (45) |
| Family history, n (%) | 18 (19) |
| Smoking, n (%) | 30 (32) |
| Dyslipidaemia, n (%) | 59 (62) |
| Diabetes, n (%) | 23 (24) |
| Indication for PCI, n (%) | |
| Elective | 25 (26) |
| Unstable angina | 32 (34) |
| Acute myocardial infarction | 38 (40) |
| Multivessel disease, n (%) | 54 (57) |
| Thienopyridines, n (%) | |
| Ticlopidine | 13 (14) |
| Clopidogrel | 82 (86) |
Angiographic baseline characteristics at the time of the initial PCI
| 95 Patients | |
|---|---|
| Lesion type, n (%) | |
| A | 5 (6) |
| B1 | 23 (24) |
| B2 | 44 (46) |
| C | 23 (24) |
| CTO | 4 (4) |
| Target vessel, n (%) | |
| LAD | 57 (60) |
| LCX | 17 (18) |
| RCA | 20 (21) |
| Left main coronary artery | 1 (1) |
| Quantitative coronary angiography | |
| Diameter stenosis (%) | 89±12 |
| Lesion length (mm) | 12±5 |
| MLD (mm) | 0.5±0.4 |
| RVD (mm) | 2.7±0.6 |
| Stents | |
| Total stent length (mm), mean±SD | 18.5±1.3 |
| 95 Patients | |
|---|---|
| Lesion type, n (%) | |
| A | 5 (6) |
| B1 | 23 (24) |
| B2 | 44 (46) |
| C | 23 (24) |
| CTO | 4 (4) |
| Target vessel, n (%) | |
| LAD | 57 (60) |
| LCX | 17 (18) |
| RCA | 20 (21) |
| Left main coronary artery | 1 (1) |
| Quantitative coronary angiography | |
| Diameter stenosis (%) | 89±12 |
| Lesion length (mm) | 12±5 |
| MLD (mm) | 0.5±0.4 |
| RVD (mm) | 2.7±0.6 |
| Stents | |
| Total stent length (mm), mean±SD | 18.5±1.3 |
Angiographic baseline characteristics at the time of the initial PCI
| 95 Patients | |
|---|---|
| Lesion type, n (%) | |
| A | 5 (6) |
| B1 | 23 (24) |
| B2 | 44 (46) |
| C | 23 (24) |
| CTO | 4 (4) |
| Target vessel, n (%) | |
| LAD | 57 (60) |
| LCX | 17 (18) |
| RCA | 20 (21) |
| Left main coronary artery | 1 (1) |
| Quantitative coronary angiography | |
| Diameter stenosis (%) | 89±12 |
| Lesion length (mm) | 12±5 |
| MLD (mm) | 0.5±0.4 |
| RVD (mm) | 2.7±0.6 |
| Stents | |
| Total stent length (mm), mean±SD | 18.5±1.3 |
| 95 Patients | |
|---|---|
| Lesion type, n (%) | |
| A | 5 (6) |
| B1 | 23 (24) |
| B2 | 44 (46) |
| C | 23 (24) |
| CTO | 4 (4) |
| Target vessel, n (%) | |
| LAD | 57 (60) |
| LCX | 17 (18) |
| RCA | 20 (21) |
| Left main coronary artery | 1 (1) |
| Quantitative coronary angiography | |
| Diameter stenosis (%) | 89±12 |
| Lesion length (mm) | 12±5 |
| MLD (mm) | 0.5±0.4 |
| RVD (mm) | 2.7±0.6 |
| Stents | |
| Total stent length (mm), mean±SD | 18.5±1.3 |
Angiographic data of emergency PCI for treatment of stent thrombosis
| Before | After | P-values | |
|---|---|---|---|
| QCA | |||
| MLD (mm) | 0.17±0.47 | 2.28±0.71 | <0.001 |
| RVD (mm) | 2.5±0.4 | 2.6±0.5 | 0.07 |
| Diameter stenosis (%) | 94±16 | 13±21 | <0.001 |
| TIMI flow | <0.001 | ||
| TIMI <3 (%) | 95 | 9 | |
| TIMI 3 (%) | 5 | 91 | |
| LVEF | 0.54±0.15 | 0.49±0.13 | <0.001 |
| Before | After | P-values | |
|---|---|---|---|
| QCA | |||
| MLD (mm) | 0.17±0.47 | 2.28±0.71 | <0.001 |
| RVD (mm) | 2.5±0.4 | 2.6±0.5 | 0.07 |
| Diameter stenosis (%) | 94±16 | 13±21 | <0.001 |
| TIMI flow | <0.001 | ||
| TIMI <3 (%) | 95 | 9 | |
| TIMI 3 (%) | 5 | 91 | |
| LVEF | 0.54±0.15 | 0.49±0.13 | <0.001 |
QCA, quantitative coronary angiography; MLD, minimal lumen diameter; RVD, reference vessel diameter; TIMI, Thrombolysis in Myocardial Infarction;39 LVEF, left ventricular ejection fraction.
Angiographic data of emergency PCI for treatment of stent thrombosis
| Before | After | P-values | |
|---|---|---|---|
| QCA | |||
| MLD (mm) | 0.17±0.47 | 2.28±0.71 | <0.001 |
| RVD (mm) | 2.5±0.4 | 2.6±0.5 | 0.07 |
| Diameter stenosis (%) | 94±16 | 13±21 | <0.001 |
| TIMI flow | <0.001 | ||
| TIMI <3 (%) | 95 | 9 | |
| TIMI 3 (%) | 5 | 91 | |
| LVEF | 0.54±0.15 | 0.49±0.13 | <0.001 |
| Before | After | P-values | |
|---|---|---|---|
| QCA | |||
| MLD (mm) | 0.17±0.47 | 2.28±0.71 | <0.001 |
| RVD (mm) | 2.5±0.4 | 2.6±0.5 | 0.07 |
| Diameter stenosis (%) | 94±16 | 13±21 | <0.001 |
| TIMI flow | <0.001 | ||
| TIMI <3 (%) | 95 | 9 | |
| TIMI 3 (%) | 5 | 91 | |
| LVEF | 0.54±0.15 | 0.49±0.13 | <0.001 |
QCA, quantitative coronary angiography; MLD, minimal lumen diameter; RVD, reference vessel diameter; TIMI, Thrombolysis in Myocardial Infarction;39 LVEF, left ventricular ejection fraction.
Clinical outcome after emergency PCI for stent thrombosis
| 95 Patients | |
|---|---|
| Procedural MACE | |
| Death, n (%) | 2 (2) |
| Myocardial infarction, n (%) | 77 (81) |
| Emergency CABG, n (%) | 2 (2) |
| Death, emergency CABG, n (%) | 4 (4) |
| In-hospital MACE (including procedural MACE) | |
| Death, n (%) | 7 (7) |
| Reinfarction, n (%) | 4 (4) |
| TVR, n (%) | 4 (4) |
| Recurrent stent thrombosis, n (%) | 4 (4) |
| 6 month MACE (including procedural and in-hospital MACE) | |
| Death, n (%) | 10 (11) |
| Reinfarction, n (%) | 15 (16) |
| TVR, n (%) | 14 (15) |
| Recurrent stent thrombosis, n (%) | 11 (12) |
| Death, MI, TVR, recurrent ST, n (%) | 28 (30) |
| 95 Patients | |
|---|---|
| Procedural MACE | |
| Death, n (%) | 2 (2) |
| Myocardial infarction, n (%) | 77 (81) |
| Emergency CABG, n (%) | 2 (2) |
| Death, emergency CABG, n (%) | 4 (4) |
| In-hospital MACE (including procedural MACE) | |
| Death, n (%) | 7 (7) |
| Reinfarction, n (%) | 4 (4) |
| TVR, n (%) | 4 (4) |
| Recurrent stent thrombosis, n (%) | 4 (4) |
| 6 month MACE (including procedural and in-hospital MACE) | |
| Death, n (%) | 10 (11) |
| Reinfarction, n (%) | 15 (16) |
| TVR, n (%) | 14 (15) |
| Recurrent stent thrombosis, n (%) | 11 (12) |
| Death, MI, TVR, recurrent ST, n (%) | 28 (30) |
TVR, target vessel revascularization; MI, myocardial infarction; CABG, coronary artery bypass grafting. MI denotes an infarction at the time of stent thrombosis. Reinfarction denotes a recurrent myocardial infarction after emergency PCI for stent thrombosis.
Clinical outcome after emergency PCI for stent thrombosis
| 95 Patients | |
|---|---|
| Procedural MACE | |
| Death, n (%) | 2 (2) |
| Myocardial infarction, n (%) | 77 (81) |
| Emergency CABG, n (%) | 2 (2) |
| Death, emergency CABG, n (%) | 4 (4) |
| In-hospital MACE (including procedural MACE) | |
| Death, n (%) | 7 (7) |
| Reinfarction, n (%) | 4 (4) |
| TVR, n (%) | 4 (4) |
| Recurrent stent thrombosis, n (%) | 4 (4) |
| 6 month MACE (including procedural and in-hospital MACE) | |
| Death, n (%) | 10 (11) |
| Reinfarction, n (%) | 15 (16) |
| TVR, n (%) | 14 (15) |
| Recurrent stent thrombosis, n (%) | 11 (12) |
| Death, MI, TVR, recurrent ST, n (%) | 28 (30) |
| 95 Patients | |
|---|---|
| Procedural MACE | |
| Death, n (%) | 2 (2) |
| Myocardial infarction, n (%) | 77 (81) |
| Emergency CABG, n (%) | 2 (2) |
| Death, emergency CABG, n (%) | 4 (4) |
| In-hospital MACE (including procedural MACE) | |
| Death, n (%) | 7 (7) |
| Reinfarction, n (%) | 4 (4) |
| TVR, n (%) | 4 (4) |
| Recurrent stent thrombosis, n (%) | 4 (4) |
| 6 month MACE (including procedural and in-hospital MACE) | |
| Death, n (%) | 10 (11) |
| Reinfarction, n (%) | 15 (16) |
| TVR, n (%) | 14 (15) |
| Recurrent stent thrombosis, n (%) | 11 (12) |
| Death, MI, TVR, recurrent ST, n (%) | 28 (30) |
TVR, target vessel revascularization; MI, myocardial infarction; CABG, coronary artery bypass grafting. MI denotes an infarction at the time of stent thrombosis. Reinfarction denotes a recurrent myocardial infarction after emergency PCI for stent thrombosis.
References
Roubin GS, Cannon AD, Agrawal SK, Macander PJ, Dean LS, Baxley WA, Breland J. Intracoronary stenting for acute and threatened closure complicating percutaneous transluminal coronary angioplasty.
Schomig A, Kastrati A, Mudra H, Blasini R, Schuhlen H, Klauss V, Richardt G, Neurmann FJ. Four-year experience with Palmaz-Schatz stenting in coronary angioplasty complicated by dissection with threatened or present vessel closure.
Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. Benestent Study Group.
Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M. A randomized comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators.
Maier W, Windecker S, Kung A, Lutolf R, Eberli FR, Meier B, Hess OM. Exercise-induced coronary artery vasodilation is not impaired by stent placement.
Kimura T, Yokoi H, Nakagawa Y, Tamura T, Kaburagi S, Sawada Y, Sato Y, Hamasaki N, Nosaka H. Three-year follow-up after implantation of metallic coronary-artery stents.
Urban P, Macaya C, Rupprecht HJ, Kiemeneij F, Emanuelsson H, Fontanelli A, Pieper M, Wesseling T, Sagnard L. Randomized evaluation of anticoagulation versus antiplatelet therapy after coronary stent implantation in high-risk patients: the multicenter aspirin and ticlopidine trial after intracoronary stenting (MATTIS).
Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty.
Schomig A, Neumann FJ, Kastrati A, Schuhlen H, Blasini R, Hadamitzky M, Walter H, Zitzmann-Roth EM, Richardt G, Alt E, Schmitt C, Ulm K. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents.
Bertrand ME, Legrand V, Boland J, Fleck E, Bonnier J, Emmanuelson H, Vrolix M, Missault L, Chierchia S, Casaccia M, Niccoli L, Oto A, White C, Webb-Peploe M, Van Belle E, McFadden EP. Randomized multicenter comparison of conventional anticoagulation versus antiplatelet therapy in unplanned and elective coronary stenting. The full anticoagulation versus aspirin and ticlopidine (fantastic) study.
Leon MB, Baim DS, Popma JJ, Gordon PC, Cutlip DE, Ho KK, Giambartolomei A, Diver DJ, Lasorda DM, Williams DO, Pocock SJ, Kuntz RE. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. Stent Anticoagulation Restenosis Study Investigators.
Bertrand ME, Rupprecht HJ, Urban P, Gershlick AH, Investigators FT. Double-blind study of the safety of clopidogrel with and without a loading dose in combination with aspirin compared with ticlopidine in combination with aspirin after coronary stenting: the clopidogrel aspirin stent international cooperative study (CLASSICS).
Cutlip DE, Baim DS, Ho KK, Popma JJ, Lansky AJ, Cohen DJ, Carrozza JP, Jr., Chauhan MS, Rodriguez O, Kuntz RE. Stent thrombosis in the modern era: a pooled analysis of multicenter coronary stent clinical trials.
Taniuchi M, Kurz HI, Lasala JM. Randomized comparison of ticlopidine and clopidogrel after intracoronary stent implantation in a broad patient population.
Orford JL, Lennon R, Melby S, Fasseas P, Bell MR, Rihal CS, Holmes DR, Berger PB. Frequency and correlates of coronary stent thrombosis in the modern era: analysis of a single center registry.
Mueller C, Roskamm H, Neumann FJ, Hunziker P, Marsch S, Perruchoud A, Buettner HJ. A randomized comparison of clopidogrel and aspirin versus ticlopidine and aspirin after the placement of coronary artery stents.
Karrillon GJ, Morice MC, Benveniste E, Bunouf P, Aubry P, Cattan S, Chevalier B, Commeau P, Cribier A, Eiferman C, Grollier G, Guerin Y, Henry M, Lefevre T, Livarek B, Louvard Y, Marco J, Makowski S, Monassier JP, Pernes JM, Rioux P, Spaulding C, Zemour G. Intracoronary stent implantation without ultrasound guidance and with replacement of conventional anticoagulation by antiplatelet therapy. 30-day clinical outcome of the French Multicenter Registry.
Uren NG, Schwarzacher SP, Metz JA, Lee DP, Honda Y, Yeung AC, Fitzgerald PJ, Yock PG. Predictors and outcomes of stent thrombosis: an intravascular ultrasound registry.
Moussa I, Di Mario C, Reimers B, Akiyama T, Tobis J, Colombo A. Subacute stent thrombosis in the era of intravascular ultrasound-guided coronary stenting without anticoagulation: frequency, predictors and clinical outcome.
Kastrati A, Koch W, Gawaz M, Mehilli J, Bottiger C, Schomig K, von Beckerath N, Schomig A. PlA polymorphism of glycoprotein IIIa and risk of adverse events after coronary stent placement.
Gum PA, Kottke-Marchant K, Welsh PA, White J, Topol EJ. A prospective, blinded determination of the natural history of aspirin resistance among stable patients with cardiovascular disease.
Barragan P, Bouvier JL, Roquebert PO, Macaluso G, Commeau P, Comet B et al. Resistance to thienopyridines: clinical detection of coronary stent thrombosis by monitoring of vasodilator-stimulated phosphoprotein phosphorylation.
Gurbel PA, Bliden KP, Hiatt BL, O'Connor CM. Clopidogrel for coronary stenting: response variability, drug resistance, and the effect of pretreatment platelet reactivity.
Hasdai D, Garratt KN, Holmes DR Jr, Berger PB, Schwartz RS, Bell MR. Coronary angioplasty and intracoronary thrombolysis are of limited efficacy in resolving early intracoronary stent thrombosis.
Casserly IP, Hasdai D, Berger PB, Holmes DR Jr, Schwartz RS, Bell MR. Usefulness of abciximab for treatment of early coronary artery stent thrombosis.
Silva JA, White CJ, Ramee SR, Collins TJ, Jenkins JS, Ho K, Baim DS, Carrozza JP, Rinfret S, Setum CM, Popma JJ, Kuntz RE. Treatment of coronary stent thrombosis with rheolytic thrombectomy: results from a multicenter experience.
Tcheng JE, Kandzari DE, Grines CL, Cox DA, Effron MB, Garcia E, Griffin JJ, Guagliumi G, Stuckey T, Turco M, Fahy M, Lansky AJ, Mehran R, Stone GW. Benefits and risks of abciximab use in primary angioplasty for acute myocardial infarction: the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications (CADILLAC) trial.
Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials.
Silva JA, Nunez E, White CJ, Collins TJ, Jenkins JS, Zhang S, Jain SP, Ramee SR. Predictors of stent thrombosis after primary stenting for acute myocardial infarction.
Ross AM, Coyne KS, Moreyra E, Reiner JS, Greenhouse SW, Walker PL, Simoons ML, Draoui YC, Califf RM, Topol EJ, Van de Werf F, Lundergan CF. Extended mortality benefit of early postinfarction reperfusion. GUSTO-I Angiographic Investigators. Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries Trial.
Berger PB, Bell MR, Rihal CS, Ting H, Barsness G, Garratt K, Bellot V, Mathew V, Melby S, Hammes L, Grill D, Holmes DR, Jr. Clopidogrel versus ticlopidine after intracoronary stent placement.
Steinhubl SR, Berger PB, Mann JT, 3rd, Fry ET, DeLago A, Wilmer C, Topol EJ. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA
Mehta SR, Yusuf S, Peters RJ, Bertrand ME, Lewis BS, Natarajan MK, Malmberg K, Rupprecht H, Zhao F, Chrolavicius S, Copland I, Fox KA. Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention: the PCI-CURE study.
Stone GW, Cox D, Garcia E, Brodie BR, Morice MC, Griffin J, Mattos L, Lansky AJ, O'Neill WW, Grines CL. Normal flow (TIMI-3) before mechanical reperfusion therapy is an independent determinant of survival in acute myocardial infarction: analysis from the primary angioplasty in myocardial infarction trials.
Randomised placebo-controlled and balloon-angioplasty-controlled trial to assess safety of coronary stenting with use of platelet glycoprotein-IIb/IIIa blockade. The EPISTENT Investigators. Evaluation of Platelet IIb/IIIa Inhibitor for Stenting.
van den Brand M, Laarman GJ, Steg PG, De Scheerder I, Heyndrickx G, Beatt K, Kootstra J, Simoons ML. Assessment of coronary angiograms prior to and after treatment with abciximab, and the outcome of angioplasty in refractory unstable angina patients. Angiographic results from the CAPTURE trial.
Ryan TJ, Faxon DP, Gunnar RM, Kennedy JW, King SB, 3rd, Loop FD, Peterson KL, Reeves TJ, Williams DO, Winters WL, Jr., et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty).
Ellis SG, Guetta V, Miller D, Whitlow PL, Topol EJ. Relation between lesion characteristics and risk with percutaneous intervention in the stent and glycoprotein IIb/IIIa era: An analysis of results from 10,907 lesions and proposal for new classification scheme.


{kind=link}
{kind=link}
{kind=link}