





Abstract
The objective of this article is to provide evidence-based recommendations for the management of patients with herpes zoster (HZ) that take into account clinical efficacy, adverse effects, impact on quality of life, and costs of treatment. Systematic literature reviews, published randomized clinical trials, existing guidelines, and the authors' clinical and research experience relevant to the management of patients with HZ were reviewed at a consensus meeting. The results of controlled trials and the clinical experience of the authors support the use of acyclovir, brivudin (where available), famciclovir, and valacyclovir as first-line antiviral therapy for the treatment of patients with HZ. Specific recommendations for the use of these medications are provided. In addition, suggestions are made for treatments that, when used in combination with antiviral therapy, may further reduce pain and other complications of HZ.
After a primary varicella-zoster virus (VZV) infection (termed “varicella” or “chickenpox”), the virus establishes latency in dorsal root and cranial nerve ganglia. Herpes zoster (HZ), also known as “shingles,” results from reactivation of VZV and its spread from a single ganglion to the neural tissue of the affected segment and the corresponding cutaneous dermatome [1].
The objective of this supplement to Clinical Infectious Diseases is to improve the care of patients with HZ by providing practical, evidence-based recommendations that take into account clinical efficacy, adverse effects, impact on quality of life, and costs of treatment. Pharmacologic management is emphasized, because few nonpharmacologic approaches have been evaluated in randomized controlled trials. These recommendations apply only to the acute phase of HZ; detailed recommendations for the treatment of postherpetic neuralgia (PHN), the most common complication of HZ, appear elsewhere [2, 3]. We describe the pathogenesis, epidemiological aspects, clinical aspects, and complications of HZ, and then we review the literature on the treatment of HZ and present specific treatment recommendations.
Pathogenesis of Hz
Nasopharyngeal replication of VZV, which occurs immediately after primary infection, is followed by spread to adjacent lymphoid tissue, where the virus infects memory CD4+ T cells, which are abundant in tonsilar lymphoid tissue [4]. Trafficking of memory cells expressing cutaneous homing antigen and CCR4 to the skin is thought to deliver virus to cutaneous epithelia within a few days of infection [4]. The localized replication in epithelial cells is facilitated by down-regulation of IFN-α within the infected cells and failure of induction of adhesion molecules [5]. At the same time, cell-to-cell spread of virus appears to be contained for the first week by production of IFN-α in adjacent epithelial cells [5, 6]. Thereafter, the virus overcomes the innate defenses, and vesicles appear. Production of cytokines and up-regulation of capillary endothelial adhesion factors attract migratory T cells that may further spread virus before they contain viral replication [5].
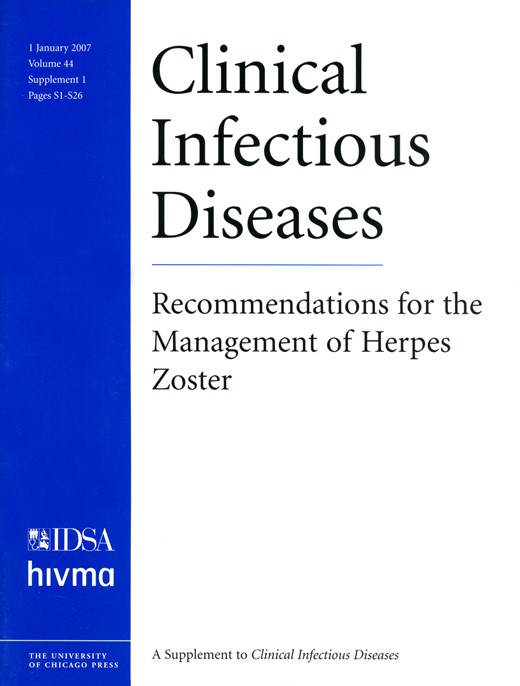
Cell-free virus, which is present only in skin vesicles, is necessary for the infection of sensory nerve endings in epithelia. This results in virus migration up sensory axons to establish latency in sensory ganglia [7]. The final assembly and envelopment of newly synthesized virions occurs within specialized wrapping cisternae located in the trans-Golgi network [8, 9]. The concave face of each wrapping cisterna is rich in VZV glycoproteins and becomes the viral envelope. The convex side is rich in cellular proteins, such as cation-independent mannose 6-phosphate receptors, and the cisterna becomes a transport vesicle containing the newly enveloped virion [8, 10]. In human embryo lung fibroblasts, the presence of cation-independent mannose 6-phosphate receptors on the convex face of the wrapping cisterna is postulated to route virions from the cell secretory pathway to endosomes where the virions are sequestered [8, 11, 12] (figure 1). VZV also spreads quickly to adjacent epidermal cells by inducing the fusion (mediated by glycoproteins H, L, B, and E) of virally infected cells with uninfected neighboring cells [9]. In contrast, the loss of cation-independent mannose 6-phosphate receptors in keratinocytes in the superficial epidermis allows for the accumulation of cell-free virions, which are necessary for transmission and establishment of latency [13].
![Intracellular transport and maturation of varicella-zoster virus (VZV). A, Primary envelopment. VZV nucleocapsids assemble in the nucleus, bud through the inner nuclear membrane, and acquire a temporary envelope before entering the perinuclear cisterna, which is continuous with the lumen of the endoplasmic reticulum. The primary virion envelope fuses with the membrane of the endoplasmic reticulum, delivering naked nucleocapsids into the cytosol. B, Glycoprotein transport and virion assembly. VZV glycoproteins are synthesized in the rough endoplasmic reticulum (RER) and become processed and transported to the Golgi complex via the intermediate compartment (IC) independently of newly assembled nucleocapsids. From the RER, the glycoproteins, together with adhered tegument proteins, are transported to the trans-Golgi network (TGN), where they concentrate in the concave membrane of specialized wrapping TGN cisternae. The viral nucleocapsids converge with the glycoproteins and tegument as the TGN sacs wrap around the nucleocapsids and fuse, giving rise to mature virions The VZV glycoprotein-rich membrane of the concave face of the wrapping cisterna becomes the viral envelope. The membrane of the convex face is rich in mannose 6-phosphate (Man-6-P) receptors and delimits a transport vesicle that encloses the newly enveloped virion. Man-6-P receptors on the membrane of the convex face of the wrapping cisterna are thought to route viral particles from the cell secretory pathway to endosomes where the virions are degraded. Illustration reproduced with permission from [8].](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/cid/44/Supplement_1/10.1086_510206/1/m_44-Supplement_1-S1-fig001.gif?Expires=1716312137&Signature=A6VLRbkvWO3PGdyesD~qpLZpPMLFT51LPggh-QxPG6XXTvGXS1UfC95BafF75I29khhUrkWQ1COrw25inRqRZwZNmVwTucib6fj9zS1OBRpbunDNNdqPx0S0cIpUxD5WPhrKd89H2MV-gVnCV0mnQH4q983SCs9vYeLU6tQrXMpHi4HMhPXN~Y3hOHTDIA8p-35N3WU2dIprehy50xyvexuPn7OSAx8CYvQl~SLSqeBPlQrpfXDla4F6Kzgb3G4Ugm5Fxu~vgR7eJX6WLhzAL6c-zfUFibJLl1Z7FbENim85ZDpzsZrb7LD0vlNpa1rA9u2eqsXL94I~nwAcxwemwQ__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Intracellular transport and maturation of varicella-zoster virus (VZV). A, Primary envelopment. VZV nucleocapsids assemble in the nucleus, bud through the inner nuclear membrane, and acquire a temporary envelope before entering the perinuclear cisterna, which is continuous with the lumen of the endoplasmic reticulum. The primary virion envelope fuses with the membrane of the endoplasmic reticulum, delivering naked nucleocapsids into the cytosol. B, Glycoprotein transport and virion assembly. VZV glycoproteins are synthesized in the rough endoplasmic reticulum (RER) and become processed and transported to the Golgi complex via the intermediate compartment (IC) independently of newly assembled nucleocapsids. From the RER, the glycoproteins, together with adhered tegument proteins, are transported to the trans-Golgi network (TGN), where they concentrate in the concave membrane of specialized wrapping TGN cisternae. The viral nucleocapsids converge with the glycoproteins and tegument as the TGN sacs wrap around the nucleocapsids and fuse, giving rise to mature virions The VZV glycoprotein-rich membrane of the concave face of the wrapping cisterna becomes the viral envelope. The membrane of the convex face is rich in mannose 6-phosphate (Man-6-P) receptors and delimits a transport vesicle that encloses the newly enveloped virion. Man-6-P receptors on the membrane of the convex face of the wrapping cisterna are thought to route viral particles from the cell secretory pathway to endosomes where the virions are degraded. Illustration reproduced with permission from [8].
A guinea pig model of latency and reactivation in vitro has been developed. Neurons dissected from the myenteric plexus are propagated in culture. In this model, infection of sensory nerve endings with cell-associated virus causes lytic infection, whereas cell-free virus establishes latency [7]. Latently infected human ganglia show restricted expression of 6 genes—ORF4, ORF21, ORF29, ORF62, ORF63, and ORF66 [14,15,16–17]—none of which code for glycoproteins, with 1 report of detection of open reading frame (ORF) 18 transcripts [16]; the same pattern of expression is found in latently infected guinea pig somatic neurons [7]. The addition of cell-associated virus, the product of the ORF61 gene, or its herpes simplex virus (HSV) homologue ICP0 to the guinea pig gut model results in VZV reactivation and lytic infection [7]. ORF 61 protein is absent from cell-free virions, which are able to establish latency in the gut ganglia. More recently, direct transfer of VZV has been demonstrated from infected peripheral blood mononuclear cells to ganglion tissue implanted into SCID-hu mice. Direct transfer of virus to the ganglion and establishment of latency by this route may, therefore, be possible [18].
In situ hybridization has shown the latent VZV genome to be localized in ∼1%–7% of sensory ganglion neurons, at <10 copies/cell [19,20–21]. In addition to detection of messenger RNA from the 6 ORFs mentioned, immunohistochemical studies have shown the presence of protein products from ORFs 4, 21, 29, 62, 63, and 66 [17, 22, 23]. Moreover, these are located in the cytoplasm of infected cells, whereas, in lytic infection, both cytoplasmic and nuclear localization is evident. A working hypothesis is that phosphorylation of immediate-early protein 62 by the protein kinase encoded by ORF66 prevents translocation of the former to the nucleus, which, in turn, interrupts the cascade of viral transcription and replication [17]. The addition of ORF 61 protein to the latently infected guinea pig neuron model results in translocation of immediate-early protein 62 and the ORF 29 protein to the nucleus. This causes transcription of α, β, and γ viral proteins and reestablishment of lytic infection [7, 22].
The incidence of HZ increases with age and with other causes of decreased cellular immunity. Limiting dilution experiments have established that reduced VZV T cell responder cell frequency characterizes all conditions associated with increased VZV reactivation [24]. Much of the T cell response in latently infected individuals is directed against glycoproteins E, H, B, and I, as well as against transcriptional activators encoded by ORFs 4, 10, 62, and 63. Boosting of the cell-mediated immune response has been shown in mothers of children with varicella, suggesting that exposure to antigen may be important for maintaining immunity [25]. Two studies have shown that the incidence of HZ is lower in adults with greater contact with children in their daily lives, which was considered to be a surrogate for exposure to VZV [26, 27]. Proof that exposure to exogenous antigen is protective came with the recent demonstration that a live attenuated VZV vaccine reduced the incidence of HZ and the burden of disease, compared with placebo [28].
Reducing the occurrence of HZ will be crucial to eliminating transmission of VZV. The force of infection (i.e., the rate at which individuals acquire infection after exposure) is estimated to be 20% for varicella leading to infection of children 2–4 years of age. By contrast, the estimated force of infection for HZ causing varicella is 0.1% [29]. Thus, susceptible children are more likely to develop varicella from exposure to varicella than from exposure to HZ. Nonetheless, HZ will become a more common source of varicella as immunization programs eliminate varicella; this is already evident in cases of nosocomial varicella in the United Kingdom, where many cases arise from contact with HZ rather than varicella [30].
Epidemiological Aspects of Hz
Varicella typically occurs during childhood in temperate climates and during adolescence or early adulthood in tropical areas [31]. Latency is typically lifelong, and HZ is caused by viral reactivation from the latent state. Second episodes of HZ occur in ≤5% of individuals but occur more frequently in those who are immunocompromised. Primary infection produces long-term immunity to varicella. Protection from reactivation depends on intact cell-mediated immunity, which declines with age (immunosenescence), during certain diseases (e.g., HIV infection and some malignancies), and as a result of immunosuppressive therapy (e.g., after organ transplantation, chemotherapy, or steroid treatment). The survival of VZV in humans for several million years attests to its success.
Data from a number of sources consistently show that the incidence of HZ increases with age. Although HZ is not rare in young individuals, the median age of patients with HZ is ∼64 years, whereas the median age of the US population is ∼46 years. The incidence of HZ ranges from 1.2 to 3.4 cases per 1000 person-years in studies of immunocompetent individuals in the community, but it increases to 3.9–11.8 cases per 1000 person-years among those >65 years of age [28, 32,33,34,35–36]. Some [37, 38], but not all [39, 40], recent studies have found the incidence of HZ to be increasing, although the explanation is unclear. It is likely that the incidence of HZ will change further over the coming decades, as a result of the increasing age of the population, changes in therapy for malignant and autoimmune diseases, and the increasing use of organ transplantation, and, possibly, as a consequence of childhood varicella vaccination.
In the developed world and elsewhere, significant increases are occurring in the percentage of people who are elderly. In the United Kingdom, 2001 census data showed that the population ≥65 years of age numbered ∼9 million (16%), and the projection for 2025 is 13 million. Among those ≥65 years of age, the proportion of people ≥85 years of age has increased from 7% in 1971 to 12% in 2004. Data from the Scientific Registry of Transplant Recipients draft analysis has shown a year-by-year increase in the number of solid-organ transplants in the United States, with ∼12,000 conducted in 1988 and twice that number conducted in 2003; all these patients receive immunosuppressant medications (Scientific Registry of Transplant Recipients, personal communication, 13 January 2004).
Childhood vaccination to prevent varicella was introduced in the United States in 1995, and other countries adopting this strategy include Australia, Canada, Germany, Israel, Japan, and South Korea. Epidemiological models suggest that a significant increase in HZ incidence could occur as a consequence of reduced opportunities for subclinical boosting, due to dramatic reductions in varicella incidence resulting from immunization [26, 41, 42]. To the extent that exogenous boosting enhances VZV-specific cell-mediated immunity and delays reactivation of latent virus, adults with a history of varicella in regions where varicella incidence has been markedly reduced by vaccination will be more likely to develop HZ than will those living where varicella is more common. The incidence of HZ may, therefore, increase significantly, peaking ∼20 years after the initiation of childhood vaccination programs and only returning to prevaccination levels after 40 years [42]. Although the attenuated Oka vaccine virus establishes neuronal latency in vaccine recipients, it appears to reactivate and cause HZ much less frequently than does wild-type VZV. Thus, it is expected that the incidence of HZ would decrease as the number of adults infected with latent wild-type virus decreases. Any increase in HZ incidence could be offset by adult HZ vaccination, if its use becomes widespread. In a randomized clinical trial of HZ vaccination compared with placebo among nearly 39,000 adults ≥60 years of age, the incidence of HZ was reduced by 51.3% [28].
If vaccination of adults is widely adopted and produces reductions in the incidence and burden of HZ in the community that are comparable to those found in this trial [28], there could be a dramatic reduction in HZ incidence in the decades to come. Considering the potential impact of adult HZ vaccination and the long-term effect of childhood varicella vaccination, future generations may largely be spared the most distressing complications of HZ.
Clinical Aspects of Hz
The reactivation of VZV in ganglia may be a frequent event. In the presence of adequate VZV-specific immune responses—most importantly, T cell—mediated immunity—reactivation events are either prevented or quickly aborted. The outcomes of these reactivations, thus, remain subclinical, although immunological evidence of their existence can be detected [43]. If the VZV reactivation is not contained, as can occur with iatrogenic immunosuppression or age-related immunosenescence, then viral replication ensues, resulting in ganglionitis and extensive infection and destruction of neurons and supporting cells [44, 45]. This significant infection and accompanying inflammatory response is probably the origin of the prodromal pain that precedes the characteristic dermatomal eruption of HZ. Approximately 70%–80% of patients with HZ describe prodromal pain in the dermatome where skin lesions subsequently appear. Prodromal pain may be constant or intermittent and frequent or sporadic, and it may or may not interfere with sleep. The pain often has a distinctive quality for each patient and is commonly described as “burning,” “shooting,” “stabbing,” or “throbbing.” Some patients describe the pain only when the involved area is touched, whereas others complain primarily of pruritus. The prodrome is typically 2–3 days in duration, but longer durations, of ≥1 week, are not uncommon. Significant and prolonged prodromal pain not uncommonly leads to medical investigation for diseases characterized by pain in the area of the prodrome (e.g., angina, cholecystitis, glaucoma, nephrolithiasis, and spinal nerve compression).
The cause of the dermatomal pain becomes obvious when the characteristic rash appears in that dermatome [1]. The interval from the onset of the prodrome to the appearance of rash represents the time required for reactivated VZV to replicate in the ganglion and to transit down the cutaneous nerve to the nerve endings at the dermal-epidermal junction. There is additional delay while VZV replicates in the skin and induces sufficient necrosis and inflammatory response to cause the rash.
The rash associated with HZ has a brief erythematous and macular phase, which is often missed, after which papules rapidly appear. These papules develop into vesicles within 1–2 days, and vesicles continue to appear for 3–4 days. At this point, lesions of all types may be present (see figures 2 – 4). The lesions tend to be grouped, and clusters are often seen where there are branches of the cutaneous sensory nerve (e.g., in parasternal, mid-axillary, and paraspinous areas, representing the anterior and lateral branches of the anterior primary division as well as the posterior division of a thoracic nerve). Pustulation of vesicles begins within 1 week of the onset of rash, if not sooner, and is followed 3–5 days later by lesion ulceration and crusting. The appearance of new vesicles for >1 week should raise concern about an underlying immunodeficiency syndrome. Crusts usually are gone by the end of 3 or 4 weeks, but scarring and hypo- or hyperpigmentation may persist long after the HZ resolves. Fewer than 20% of patients have significant systemic symptoms, such as fever, headache, malaise, or fatigue. Lesions on mucous membranes, where the epidermis is fragile rather than thick and keratinized, do not usually form vesicles and crusts but form shallow erythematous ulcers. Eruptions on the mucosa may go entirely unnoticed.

Thoracic herpes zoster (photograph provided by S.W.W.)
Herpes zoster ophthalmicus (photograph provided by D.P.-L.)
HZ is a dermatomal illness that does not cross the midline except where the normal representation of segmental nerves does so to a limited extent. In immunocompetent patients, only a single dermatome is typically affected; however, normal variations in innervation can lead to limited involvement of adjacent dermatomes. In typical HZ, widespread involvement of multiple dermatomes, especially those that are widely separated, does not occur. The rash is usually accompanied by the same pain experienced during the prodrome, but this acute pain can worsen, improve, or appear for the first time during the cutaneous phase of HZ. Pruritis may be as common as pain in patients with HZ, although it has received far less medical attention [46]. Some mild cases of HZ are characterized by more pruritis than pain.
In the immunocompetent patient with HZ, there are numerous additional potential findings associated with the pain and rash. Motor nerves may be involved in 5%–15% of cases in which the nerves (especially those in muscles in the extremities) can be examined adequately. By use of electromyography, it is possible to show that muscles are involved in 50% of cases [47]. Obvious paresis typically improves over time and may respond to physical therapy (figure 5). The geniculate ganglion also contains latent VZV derived from facial, aural, and oral lesions of varicella. Reactivation in the geniculate ganglion can lead to facial nerve (VII) paralysis (because sensory and motor nerves are conjoined in nerve VII), as a result of a bystander effect. VZV and HSV account for the majority of cases of Bell palsy (idiopathic facial paralysis). In the absence of skin lesions, the etiologic role of VZV or HSV reactivation is not clinically obvious and must be determined by use of laboratory methods [48,49–50]. It has been suggested that, because of the involvement of VZV or HSV, moderate or severe Bell palsy in adults should be treated with antiviral therapy as well as adjunctive administration of corticosteroids; results of controlled trials, however, have been conflicting [51,52,53,54–55].

T8 motor neuropathy in an otherwise healthy 59-year-old man who presented with vesicles in the T8 distribution 4 weeks before this photo was taken. The patient was treated with an antiviral agent for 7 days and with analgesics as needed. As the rash resolved, this bulge became apparent; it is consistent with motor damage by varicella-zoster virus to the muscles of the abdomen (photograph provided by S.K.T.).
Reactivation in the geniculate ganglion can produce skin lesions in the mucocutaneous distribution of its peripheral nerves, including the ear and the side of the tongue. These findings, together with facial paralysis, constitute Ramsay Hunt syndrome, in which various vestibulocochlear manifestations occur when cranial nerve VIII is affected by a bystander effect [56, 57]. Satisfactory recovery of muscle function decreases with the age of the patient and the severity of the paralysis at onset. Symptomatic reactivation in other cranial nerves has been documented [58, 59].
Reactivation of VZV in sensory ganglia may be accompanied by extraneural spread, and viremia is frequently detected by PCR early after the onset of rash. Viremia disappears most rapidly in patients who receive antiviral therapy and is typically inconsequential, because the anamnestic immune response in the immunocompetent host limits replication to the dermatomal infection. However, when there is relative immune insufficiency, as may result from immunosenescence, there may be vesicles and other viremia-related skin manifestations at a distance from the affected dermatome. The likelihood and extent of so-called “cutaneous dissemination” increases with age (figure 6). However, even with advanced age, symptomatic infection of internal organs is very rare. In severely immunocompromised patients with HZ, viremia can lead to life-threatening visceral infection.
Disseminated herpes zoster (photograph provided by S.K.T.)
Subclinical invasion of VZV into the CNS is not uncommon in HZ. One-third of immunocompetent patients without clinical symptoms of infection of the CNS had either PCR results positive for VZV or anti-VZV IgG present when a CSF sample was obtained within the first weeks after the rash onset. Leukocytosis in the CSF was found in 46% of the patients. Subclinical HZ-associated changes in the brain stem were found on MRI in 53% of the patients with cranial or cervical HZ [60]. VZV is a common cause of aseptic meningitis, which can present with or without rash that may precede or follow the meningeal symptoms. The course of the disease is benign, with complete recovery expected in 1–2 weeks [61].
Second cases of HZ are uncommon in immunologically intact hosts, presumably because an episode of HZ will boost immunity and thereby prevent subsequent symptomatic VZV reactivations. The available data suggest that second cases of HZ occur in ≤5% of individuals, although this conclusion is limited by the duration of follow-up, uncertainty of the diagnoses, and incomplete information about comorbid disease [32,33–34].
There is great interest in the concept of VZV reactivation causing dermatomal pain in the absence of skin lesions, termed “zoster sine herpete.” This concept has been supported by serologic and PCR evidence of concurrent VZV reactivation during acute pain syndromes [62,63,64–65]. In addition, a variety of otherwise unexplained local sensory and motor abnormalities have been ascribed to VZV reactivation without skin manifestations. Consequently, it has been suggested that patients with unexplained and atypical local pain syndromes might benefit from antiviral therapy against VZV. A prospective study of 56 patients with such complaints in a general practice setting, together with 81 matched control blood donors, was undertaken; none of the study subjects developed a rash, and the presence of positive serologic test results (for IgM, IgG, and IgA) and positive PCR results from circulating leukocytes was very similar to that seen in the control group [66], indicating that the presence of unexplained dermatomal pain did not identify clinical or subclinical reactivations. Thus, the routine use of antiviral agents for this purpose is not supported, and there is the added concern that such therapy might abort appropriate investigation of the etiology of the pain.
Pediatric HZ. Although HZ incidence increases with age, as a reflection of the VZV-specific immune senescence that characterizes aging, HZ also occurs in children. It has been reported that children 10–14 years of age have a frequency of HZ (50–100 cases per 105 children per year) that is one-fifth to one-tenth that observed in adults 55–65 years of age [32,33–34, 67]. In general, HZ in children is less severe than that in older patients and is much less likely to result in severe acute and prolonged pain [67, 68]. Recognized risk factors for HZ occurring during childhood are a history of maternal varicella during the pregnancy or a history of primary varicella in the first year of life, which are situations that can be assumed to result in blunting of VZV-specific immune memory during primary exposure of the child to VZV. Presumably, HZ in children reflects some interference with the normal immune mechanisms that maintain latency of VZV—for example, transient immune suppression after Epstein-Barr–virus or cytomegalovirus infection [57].
Differential diagnosis and laboratory testing. Once the rash has appeared, the diagnosis of HZ is generally apparent from the clinical presentation. However, the recently completed trial of a vaccine to prevent HZ found that 20% of suspected cases could not be confirmed by PCR [28]. This reflects, in part, intentional overdiagnosis to include mild and atypical cases. Nevertheless, multiple studies from clinical diagnostic laboratories indicate that as many as 10% of specimens submitted from patients with presumed HZ instead contain HSV [69, 70]. Important elements in establishing the diagnosis by observation include (1) painful or abnormal sensory prodrome (not always present); (2) dermatomal distribution; (3) grouped vesicles (however, in some cases, only papules will be observed); (4) multiple sites filling the dermatome, especially where divisions of the sensory nerve are represented; (5) lack of history of a similar rash in the same distribution (to rule out recurrent zosteriform herpes simplex; see figure 7); and (6) pain and allodynia in the area of the rash. Allodynia, which is common in both HZ and PHN, is pain evoked by a stimulus that does not normally cause pain—for example, light brushing of the affected area with a cotton swab.

Zosteriform herpes simplex in an elderly woman who presented with what she called “her recurrent shingles.” Vesicles in a lumbosacral distribution had recurred many times over the past several years, and this outbreak began 1 week before the photo was taken. A viral culture demonstrated herpes simplex virus type 2. The patient was otherwise healthy, except for hypertension (photograph provided by S.K.T.).
Important alternative diagnoses that can be confused with HZ include zosteriform herpes simplex and contact dermatitis, especially toxic dermatitis from plant exposure (which tends to be seasonal). Moreover, the vaccine trial revealed that atypical disease (absence of pain or minimal pain, limited area of dermatomal involvement, failure of vesicles to appear) is not uncommon [28]. Atypical manifestations of HZ can also occur in immunocompromised patients. These features can include prolonged course, lesions that are intermittently recurrent, involvement of multiple dermatomes, and lesions that appear as chronic crusts or verrucous nodules. When atypical lesions are present (whether in an immunocompetent patient or an immunocompromised patient), or when there is potential confusion as to whether VZV or HSV is the pathogen (e.g., when there are lesions in the sacral area), diagnostic laboratory tests should be utilized.
PCR is the most sensitive and specific test, but it is expensive, and it takes at least 1 day to obtain results. However, DNA amplification is useful for the analysis of “old” and crusted lesions. Immunohistochemical analysis of a skin scraping is rapid (∼3 h) and relatively inexpensive; the sensitivity is ∼90%, and the specificity is 95%. The sensitivity decreases when the lesions are beyond the vesicular stage, and the procedure cannot be used on crusts. Specimens must be properly obtained for optimal laboratory diagnosis. Immunohistochemical analysis can be formatted to diagnose HSV infection, as well as VZV infection, from the slide submitted. Culture of the virus is very specific, but the result is delayed (1–2 weeks), and VZV is detected from only 60%–75% of specimens. It is not useful for very long beyond the vesicular stage of the rash [71, 72].
Complications of Hz
Encephalitis. Acute VZV encephalitis is a rare complication of HZ that usually occurs a few days after the onset of rash but has been reported from days to weeks before or after the skin eruption [73]. It should be recognized, however, that CSF pleocytosis is present in ∼50% of individuals with uncomplicated HZ, reflecting the local leptomeningitis that regularly accompanies the disease. Encephalitis has occasionally been documented in the absence of apparent cutaneous HZ and in patients who received appropriate antiviral therapy during the acute episode of HZ. Immunocompromised patients are clearly at increased risk for the development of encephalitis [73, 74]. Other markers of increased risk for CNS involvement include HZ in a cranial nerve dermatome or the presence of cutaneous dissemination. The clinical presentation is most often an acute or subacute delirium accompanied by few focal neurologic signs [73]. Other findings can include headache, meningismus, fever, ataxia, and seizures. The rate of death due to HZ-associated encephalitis varies from 0% to 25%, probably according to the extent of immune compromise, with an average mortality rate of ∼10% [73].
Chronic VZV encephalitis is seen almost exclusively in immunocompromised patients, especially patients with AIDS who have marked depletion of CD4+ T cells [75]. The onset of encephalitis may occur months after an episode of HZ; 30%–40% of these patients have no recognized history of cutaneous VZV infection, which makes the diagnosis more difficult. The clinical presentation is usually subacute, with headache, fever, mental status changes, and seizures. Patients may have focal neurologic defects, including aphasia, hemiplegia, and visual-field cuts [76]. MRI demonstrates plaque-like lesions in deep white matter, changes consistent with demyelination, and late development of ischemic or hemorrhagic infarcts of cortical and subcortical gray and white matter [77]. CSF examination reveals mononuclear pleocytosis. VZV DNA has been amplified by PCR from the CSF of patients with chronic encephalitis [65]. Pathologic studies reveal multifocal leukoencephalopathy, with lesions in the white matter near the gray-white junction, small-vessel vasculitis, and demyelination [78]. Patients often have a clinical course of progressive deterioration and death, although anecdotal reports have suggested some benefit from high-dose intravenous acyclovir therapy [78, 79].
HZ ophthalmicus with delayed contralateral hemiparesis. Stroke is a rare but serious complication of HZ that has been reported in both immunocompetent and immunocompromised patients [80], including both children and adults [81]. The pathogenesis of this unusual disorder is thought to be direct VZV invasion of large cerebral arteries by extension of virus from smaller vessels that traverse the trigeminal-innervated meninges. This produces a necrotizing arteritis that can result in vascular thrombosis or hemorrhage. The most frequently described presentation is headache and contralateral hemiplegia occurring in a patient with a history of recent HZ ophthalmicus, although a variety of other stroke syndromes have been reported. The mean interval from acute HZ to onset of neurologic symptoms in adults is ∼7 weeks, although intervals as long as 6 months have been reported. CSF examination reveals mononuclear cell pleocytosis, and imaging studies (CT or MRI) show changes consistent with brain infarction. Arteriography is usually diagnostic and demonstrates segmental inflammation, narrowing, and thrombosis of the proximal branches of the middle or anterior cerebral artery [82]. The mortality rate among adults is 20%–25%, with a high probability of permanent neurologic sequelae among survivors [83].
Myelitis. HZ myelitis is thought to result from direct invasion of the spinal cord by VZV, with virus spreading along central axons of infected primary sensory neurons. As in the brain, close neuronal packing allows spread to adjacent neurons. Involvement of descending spinothalamic tracts or of anterior horn can cause weakness, and involvement of ascending sensory tracts (posterior column or lateral spinothalamic tract) causes sensory loss at levels below the affected dermatome [84]. In severe cases, the myelopathy can progress to a partial Brown-Séquard syndrome or total cord transection. Myelitis most often follows thoracic HZ, with weakness developing in the same spinal cord segment as the rash. Neurologic symptoms begin to develop an average of 12 days after the onset of the rash [85]. However, VZV myelitis in patients with no history of antecedent HZ has also been reported [86, 87]. Immunocompromised patients are at increased risk for post-HZ myelitis, and the syndrome is well described in patients with AIDS [88]. The most common initial manifestation is bladder dysfunction (e.g., urinary retention), which is often accompanied by weakness of the lower extremities, asymmetric reflexes, and sensory disturbances [85]. MRI has been useful in diagnosing myelitis, with abnormal signal evident in the cord at the level of inflammation [89]. However, it should be noted that subclinical MRI and CSF abnormalities have also been reported [60]. The prognosis for recovery of neurologic function is variable.
VZV retinitis. Acute retinal necrosis caused by VZV has been described in immunocompetent patients. More aggressive variants of this disease have been recognized in patients with AIDS and include VZV retinitis, progressive outer retinal necrosis, and rapidly progressive herpetic retinal necrosis (RPHRN) [90,91–92]. The RPHRN syndrome is seen almost exclusively in patients with AIDS who have CD4+ T cell counts of <100 cells/mm3 [92, 93]. This form of VZV retinitis may occur concurrently with active HZ or, more frequently, may develop weeks or months after the acute episode of HZ has resolved. RPHRN can occur after HZ ophthalmicus or after HZ involving a remote dermatome. The retinitis begins with multifocal necrotizing lesions involving the peripheral retina. Most patients present with unilateral involvement, but progression to bilateral disease occurs frequently [91, 92]. Fundoscopic examination reveals granular, yellowish, nonhemorrhagic lesions that rapidly extend and coalesce, often resulting in retinal detachment. There is a relative lack of intraocular inflammatory changes. RPHRN rapidly progresses to confluent full-thickness retinal necrosis (which differs from the slow progression seen with CMV retinitis) and results in blindness in 75%–85% of involved eyes [92, 93]. The etiologic role of VZV in most cases of RPHRN has been established by demonstrating VZV in choroid, vitreous fluid, and retinal biopsy specimens, by means of culture or PCR [90]. HSV occasionally causes an identical syndrome [92, 94].
PHN. In some patients, pain does not resolve when the HZ rash heals but, rather, continues for months or years. This persisting pain is termed PHN, and it is the most common complication of HZ. Patients typically describe several different types of pain, including continuous burning or throbbing pain, intermittent sharp or electric shock–like pain, and allodynia [95]. Although multiple definitions of PHN have been used, the results of recent studies suggest that pain persisting for at least 120 days after rash onset may be considered to be a validated definition of PHN for research purposes [96,97–98]. There have been no systematic attempts to investigate the prevalence of PHN, and estimates of the number of cases in the United States have ranged up to 1 million [99]. Numerous studies have established that older age is a potent risk factor for PHN; greater acute pain intensity, greater severity of the rash, and presence and greater severity of a painful prodrome preceding the rash are additional well-replicated risk factors [98, 100,101,102–103].
There is considerable agreement that both peripheral and central processes contribute to PHN and that PHN is a heterogeneous disorder [104,105–106]. For example, patients with prominent allodynia often have minimal sensory loss and report pain relief after local application of analgesics, which suggests that preserved, and possibly sensitized, primary afferent nociceptors that remain connected to the skin and their chronically sensitized central targets are responsible for initiating and maintaining pain and allodynia in these patients [105, 107]. Pathologic findings associated with PHN include degeneration of affected primary afferent neuronal cell bodies and axons, atrophy of the spinal cord dorsal horn, scarring of the dorsal root ganglion, and loss of epidermal innervation, all of which are more prominent on the affected side [44, 108,109–110].
Chronic pain has substantial effects on quality of life, and physical disability and emotional distress are common in patients with PHN [94]. The US Food and Drug Administration has approved 3 medications for the treatment of PHN (gabapentin, lidocaine patch 5%, and pregabalin), and the results of randomized controlled trials have also demonstrated the efficacy of tricyclic antidepressants (TCAs) and opioid analgesics in treating PHN [2, 3]. Nevertheless, a substantial percentage of patients are often refractory to these treatments used alone or in combination [111] and require treatment in settings specializing in pain management. The results of controlled trials provide no basis for the use of antiviral therapy in treating patients with PHN [112, 113], although it has been suggested that higher dosages should be studied in larger samples [114, 115].
Postherpetic itch. Like pain, pruritis not infrequently persists after HZ resolves [116]. Postherpetic itch can occur along with PHN or independently of it, which suggests different mechanisms. Patients with chronic pruritis report substantial disability, not only because of the unpleasant sensations but also because of the disruptive need to scratch that is virtually impossible to ignore. The combination of chronic pruritis and profound sensory loss after HZ leads to rare cases of severe self-injury, when the protective pain sensations that deter prolonged scratching are lost [117]. Pruritis associated with HZ is neuropathic and does not respond to antihistamines or treatments for inflammatory pruritis. There are no clinical trials, but clinical experience suggests that postherpetic itch can be resistant to most treatments that are efficacious for PHN but can respond to those that suppress ectopic neuronal firing—for example, local anesthetics.
Methods Used for Developing Treatment Recommendations
Data sources and study selection. The consensus meeting on which the treatment recommendations were based was sponsored by the International Association for the Study of Pain Neuropathic Pain Special Interest Group, the Neuropathic Pain Institute, and the VZV Research Foundation. Participants were selected on the basis of research and clinical expertise relevant to HZ and its management and represent the fields of anesthesiology, geriatrics, infectious diseases, internal medicine, neurology, ophthalmology, outcomes research, pain management, and virology. Relevant publications were identified by Medline searches, examination of reference lists of published articles and book chapters, and the personal knowledge of the authors. Before the meeting, all participants were provided copies of systematic literature reviews and meta-analyses [118,119,120–121], existing guidelines relevant to the management of HZ [122,123,124–125], and published randomized clinical trials, discussed below. This literature and the authors' clinical and research experience were reviewed during the consensus meeting, which was chaired by the first 2 authors. Information on additional randomized trials that were not identified before the meeting was provided on request after the meeting. Recommendations for practice guidelines [126], best-evidence synthesis [127], and narrative systematic reviews [128] were followed in developing recommendations for the management of HZ and summarizing the literature on which they are based. The initial version of the present article was prepared by the first 5 authors, revised by the other authors, and recirculated until all authors agreed with the text.
Recommendations for first-line pharmacologic treatments are based on positive results from multiple randomized clinical trials. The methods and results of these trials, in combination with the clinical experience of the authors, provide the basis for specific recommendations regarding these treatments. Because recommendations for first-line treatments are consistent with the results of multiple trials and the clinical experience of the authors, they are made with a high degree of confidence.
Recommendations for additional treatments that should be considered in combination with first-line treatment are based on the results of single clinical trials, inconsistent results of multiple trials, or uncontrolled trials, considered together with the clinical experience of the authors. These recommendations are made with moderate confidence that these treatments should be considered because they may provide additional benefits when used in combination with first-line treatment.
Outcome assessments. Treatment effects on viral clearance, acute pain, PHN (as reflected by the presence of either persisting pain of any intensity or persisting pain of moderate or greater intensity [129]), and other complications of HZ were considered. In developing specific treatment recommendations, these efficacy outcomes were considered together with safety and tolerability as well as drug interactions, to evaluate the overall risk-benefit ratio of treatment.
It was not possible to formally consider the cost-effectiveness of treatment, because of limited data and differences related to geographic region and third-party coverage. Clinicians should familiarize themselves with medication acquisition costs and the reimbursements provided by their patients' insurance plans, to protect their patients' finances and encourage treatment compliance.
Treatment of Immunocompetent Patients
The principal goals of the treatment of HZ are reduction of pain in immunocompetent patients and cessation of viral replication in immunocompromised patients and those with ophthalmic HZ. All patients should have a medical and psychosocial history evaluation and targeted physical examination performed to confirm the diagnosis, document comorbid illnesses, and provide a basis for treatment. Prompt referral to an ophthalmologist is required for all patients with ocular involvement, whether immunocompetent or immunocompromised. Elderly patients may be socially isolated, have cognitive impairment or depression, or have had recent adverse major life events (e.g., bereavement), all of which may impact treatment compliance and response to treatment. Anxiety or depression may also develop secondary to severe HZ, which may further complicate treatment and disease resolution.
Patient Education
The treatment of HZ should occur in conjunction with appropriate education and support from the health care provider. Careful explanation of the disease, including the risk of viral transmission to individuals who have not had chickenpox, and of the proposed treatment plan is essential for adherence to therapy and is beneficial to patient well-being; for example, providing reassurance and education can dispel myths and fears about HZ and its implications for the patient's health. Encouragement, reassurance, and advice on quality of life are also important and include supporting adequate nutrition and optimal levels of mental, physical, and social activity. Patients should be told to keep the rash clean and dry to reduce the risk of bacterial superinfection, to avoid use of topical antibiotics and of dressings with adhesive that can cause irritation and delay rash healing, and to inform their physician if a secondary increase in temperature develops, which is often an indication of bacterial infection. For some patients, discomfort may be reduced by sterile wet dressings.
Antiviral Therapy
The efficacy of antiviral therapy in patients with HZ has been demonstrated by multiple randomized controlled clinical trials. Acyclovir (800 mg 5 times daily for 7–10 days), famciclovir (500 mg 3 times daily for 7 days, the approved dosage in United States; 250 mg 3 times daily is approved in some other countries), and valacyclovir (1000 mg 3 times daily for 7 days) have been approved by the US Food and Drug Administration for the treatment of HZ. These antiviral agents are phosphorylated by viral thymidine kinase and cellular kinases to a triphosphate form that inhibits viral replication.
Acyclovir was the first antiviral agent developed to treat HZ, and 4 clinical trials examined the recommended oral dosage of 800 mg 5 times daily for 7–10 days beginning within 72 h of rash onset [130,131,132,133,134,135–136]. Two clinical trials were conducted in which various dosages of famciclovir were compared with either acyclovir [137] or placebo [138, 139]. A single published clinical trial of 2 dosages of valacyclovir compared with acyclovir in patients ≥50 years of age [140] was accompanied by an unpublished trial of valacyclovir compared with placebo in patients <50 years of age. In addition, 2 trials in which famciclovir and valacyclovir were compared with acyclovir [141, 142] and 1 trial examining various dosages of famciclovir compared with acyclovir [143] were conducted in patients with HZ who were followed for only 1 month from rash onset.
VZV replication is also inhibited by brivudin, an antiviral agent that has been compared with acyclovir in 2 clinical trials [144, 145] and with famciclovir in a recent large trial [146]. Brivudin (125 mg once daily for 7 days) has been approved for the treatment of HZ in several countries.
These clinical trials demonstrated that orally administered acyclovir, brivudin, famciclovir, or valacyclovir reduces the duration of viral shedding and new lesion formation and accelerates rash healing in patients with HZ. In general, these agents decrease the severity and duration of acute pain, and it is therefore also likely that antiviral therapy reduces the adverse impact of the acute phase of HZ on quality of life.
The effect of antiviral therapy on the development of PHN has attracted particular attention because of the clinical importance of preventing chronic pain. By inhibiting viral replication, antiviral therapy likely reduces neural damage, which is thought to contribute prominently to the development of PHN. For this reason, the delay in instituting antiviral therapy should be as short as possible, to limit additional neural damage beyond what may have occurred before rash onset.
The results of meta-analyses [119, 120, 147] and many [133, 135,136,137,138,139–140, 145, 146], but not all [130, 131, 134], randomized controlled trials have demonstrated that antiviral therapy for HZ significantly reduces the duration or incidence of prolonged pain. For example, in controlled trials using the recommended dosages, the median time to complete loss of pain in patients with pain at rash healing was 63 days with famciclovir, versus 119 days with placebo [138]; the median time to complete cessation of pain was 38 days for valacyclovir, versus 51 days for acyclovir [140]. Although the effect of acyclovir on chronic pain has been less clear because of negative results from some trials [131, 148], the results of 2 meta-analyses suggest that it may be superior to placebo in reducing the overall duration of pain and the incidence of PHN [119, 120].
Although the results of each of the antiviral clinical trials taken singly can be challenged, the preponderance of the findings provides strong support for the use of antiviral therapy not only to hasten resolution of the acute phase but also to attenuate the development of chronic pain in patients with HZ. Acyclovir, famciclovir, and valacyclovir are well tolerated and safe [1]. However, brivudin (which is not available in the United States) must not be used to treat patients receiving 5-fluorouracil (or other 5-fluoropyrimidines), because its main metabolite inhibits catabolism of fluorinated pyrimidine derivatives. This drug interaction can cause severe and potentially fatal bone marrow suppression. The most common adverse effects associated with antiviral therapy are nausea (occasionally with vomiting) and headache, which occur in no more than 10%–20% of patients, a rate generally similar to that found in patients treated with placebo [138, 140, 144].
In head-to-head comparisons of effects on cutaneous and pain end points, no differences were found between famciclovir and valacyclovir [149] and brivudin and famciclovir [146]. Some evidence suggests that these 3 agents may be somewhat superior to acyclovir in reducing the likelihood of prolonged pain [137, 140, 145]. In choosing among antiviral agents, factors in addition to efficacy should be considered. Acyclovir, which is available in generic forms, is less expensive than the antiviral agents still protected by patent. However, dosing for brivudin is once daily, and dosing for famciclovir and valacyclovir is 3 times daily, making these 3 antiviral agents considerably more convenient than acyclovir, the optimal use of which requires dosing every 5 h because of its pharmacokinetics. Furthermore, when choosing an antiviral agent, it is also important to consider the higher and more reliable levels of antiviral activity achieved in blood with the use of oral brivudin, famciclovir, or valacyclovir, compared with oral acyclovir. The existence of barriers to the entry of antiviral agents from the bloodstream into tissues that are sites of HZ complications and the lower sensitivity of VZV compared with HSV make higher blood levels of antiviral medications important.
All of the controlled clinical trials of antiviral therapy have initiated treatment within 72 h of rash onset, an arbitrary inclusion criterion that does not necessarily reflect the cessation of viral replication. Because patients often do not recognize the significance of their symptoms or because there are delays in scheduling their evaluation, HZ is often not diagnosed this rapidly in clinical practice; obtaining medication can be an additional delay. Thus, patients are often unable to initiate treatment within this narrow window. Unfortunately, because the efficacy of antiviral therapy initiated ≥4 days after rash onset has not been systematically studied, there is no evidence base for such treatment. However, there is no difference in pain outcomes when antiviral therapy is initiated before 48 h versus 48–72 h after rash onset [150], and the results of 2 uncontrolled studies revealed no significant differences in the persistence of pain between patients who initiated treatment within 72 h and those who initiated treatment at a later time [151, 152]. Considered together, these data are not inconsistent with there being a benefit from antiviral therapy initiated beyond 72 h after rash onset.
A few studies have examined whether the benefit of antiviral therapy is augmented when its duration is extended beyond 7 days [140, 153, 154]. The results of these studies suggest that any benefit of extending treatment duration beyond 7 days may be minimal, but this conclusion requires further investigation.
Recommendations for Antiviral Therapy
Topical antiviral therapy lacks efficacy in patients with HZ and is not recommended. Systemic antiviral therapy is strongly recommended as first-line treatment for all immunocompetent patients with HZ who fulfill any of the following criteria (see table 1): (1) ≥50 years of age; (2) have moderate or severe pain; (3) have moderate or severe rash; or (4) have nontruncal involvement. In patients who have a low risk for complications of HZ—for example, those who are younger with mild acute pain and rash and truncal involvement—the potential benefits of treatment are unknown but may be meaningful because such patients can still develop PHN. Acyclovir, famciclovir, and valacyclovir are all exceptionally safe, which contributes to a favorable balance of potential benefit versus risk. It is, therefore, recommended that antiviral therapy be considered even for patients whose risk of developing PHN and other complications of HZ is likely to be low.
Oral antiviral medications for herpes zoster.
There are no systematic data addressing the effectiveness of antiviral therapy administered outside of the clinical trial setting. Nevertheless, in clinical practice, brivudin, famciclovir, and valacyclovir can be expected to have greater overall effectiveness than acyclovir, on the basis of their potentially superior efficacy [137, 140, 145], the greater patient compliance associated with their more convenient dosing, and their higher and more reliable levels of antiviral activity in blood, which is important because of the existence of barriers to the entry of antiviral agents from the bloodstream into tissues that are sites of HZ complications.
In patients presenting >72 h after rash onset, the potential benefits of initiating antiviral therapy are unknown but might be meaningful, given the minimal risks of treatment with acyclovir, famciclovir, and valacyclovir. The presence of new vesicles or complications of HZ may identify patients with continuing viral replication who could benefit from treatment. It is, therefore, recommended that the initiation of antiviral therapy be considered for patients presenting >72 h after rash onset with continued new vesicle formation or when there are cutaneous, motor, neurologic, or ocular complications. Advanced age and severe pain (which are potent risk factors for PHN) are additional factors that can prompt consideration of initiating antiviral therapy >72 h after rash onset.
In patients who still have new vesicles forming or who have cutaneous, motor, neurologic, or ocular complications after 7 days of antiviral therapy, close monitoring is recommended to assess the need for further evaluation. Because the potential benefits are unknown but may be meaningful, and given the minimal risks of treatment, it is also recommended that consideration be given to extending the duration of antiviral therapy for >7 days for these patients. In patients who have been given an incorrect diagnosis or who develop toxicity, antiviral therapy should be discontinued immediately.
When rash healing has not occurred in a normal fashion in an immunocompetent patient with HZ, further evaluation by an infectious diseases specialist is recommended. Infection with VZV resistant to acyclovir (mediated by absent or altered expression of thymidine kinase) has been reported in immunocompromised but not in immunocompetent patients.
Supplementing Antiviral Therapy
Although the reduction in chronic pain demonstrated by most antiviral trials is both statistically and clinically significant, antiviral therapy does not prevent PHN in all patients. In antiviral trials, ∼20% of patients >50 years of age continue to have pain 6 months after their rash, despite treatment beginning within 72 h of rash onset [119, 139, 140, 149]. Although it is possible that new antivirals with greater efficacy will be developed, a different strategy for preventing PHN is to supplement antiviral therapy.
Oral corticosteroids. Two well-designed clinical trials demonstrated that the addition of a 3-week tapering dosage of a corticosteroid did not contribute significantly, beyond the benefits achieved by acyclovir alone, in reducing prolonged pain [148, 153]. However, the addition of the corticosteroid did have beneficial effects on acute pain and some cutaneous end points in both of these trials; in one of the trials, the times to uninterrupted sleep, return to normal daily activity, and cessation of analgesic therapy were all significantly accelerated in patients who received combination therapy [148]. Individuals with contraindications to the use of corticosteroids, including hypertension, diabetes, and peptic ulcer disease, were excluded from these studies. Nevertheless, adverse effects of corticosteroids were reported, including gastrointestinal symptoms, edema, and granulocytosis.
Analgesic treatments. No randomized placebo-controlled trials of oral treatments for acute pain in patients with HZ have been published. However, the well-replicated finding that more-severe acute pain is a risk factor for PHN, as well as research on the pathophysiologic mechanisms of PHN, provide the basis for hypothesizing that the combination of antiviral therapy with effective relief of acute pain may further lessen the risk of PHN beyond that achieved with antiviral therapy alone [155]. TCAs have well-established efficacy in the treatment of PHN and other neuropathic pain syndromes [156, 157], and TCAs may, therefore, have an analgesic effect in HZ. The results of a placebo-controlled trial of amitriptyline (25 mg once daily for 3 months beginning within 48 h of rash onset) and a reanalysis examining the subgroup of patients also treated with an antiviral suggested that amitriptyline reduced the incidence of PHN at 6 months by at least 50% [158, 159].
The effect of amitriptyline on acute pain was not assessed in this study, and because treatment continued for 3 months after rash onset, it cannot be determined whether the reduction in PHN incidence was the result of early treatment. Amitriptyline and other TCAs have generally poor tolerability and a potential for serious adverse effects, including sudden cardiac death [160, 161]. A screening electrocardiogram is recommended to assess cardiac conduction abnormalities before beginning TCA treatment of patients >40 years of age who have neuropathic pain [162]. Two selective serotonin and norepinephrine reuptake inhibitors—venlafaxine and duloxetine—are better tolerated than TCAs and have recently been demonstrated to have efficacy in patients with diabetic polyneuropathy [163, 164]. However, until the efficacy of these antidepressants is demonstrated for patients with PHN, there is little basis for predicting that they would prevent its development when used in patients with HZ.
Opioid analgesics would be expected to reduce acute pain in patients with HZ because of their diverse mechanisms of action in the peripheral nervous system and CNS as well as their demonstrated efficacy in patients with both inflammatory and neuropathic pain [165, 166], including PHN [167, 168]. Opioid analgesics are often used in combination with weak analgesics, such as acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs), but the efficacy of such combinations has not been systematically studied in patients with HZ or chronic neuropathic pain. Preliminary analyses of a recent randomized trial showed that controlled-release oxycodone was superior to placebo in relieving acute pain in patients with HZ within the first 2–3 weeks after rash onset, but the sample size precluded an evaluation of the effect of treatment on PHN [169]. Tramadol, a weak µ-opioid agonist that also inhibits the reuptake of norepinephrine and serotonin, is efficacious in patients with PHN [170] but has not been studied as a treatment for HZ.
Gabapentin and pregabalin act at the α2-δ subunit of voltage-gated calcium channels to reduce neurotransmitter release, and multiple studies have demonstrated their efficacy in patients with chronic neuropathic pain [157], including PHN [171,172,173,174,175–176]. The US Food and Drug Administration has approved gabapentin for the treatment of PHN and pregabalin for the treatment of PHN and painful diabetic polyneuropathy. The combination of their generally satisfactory tolerability, safety, and lack of drug interactions distinguish them from other oral medications used in the treatment of neuropathic pain. A recent proof-of-concept study has demonstrated analgesic effects of a single 900-mg dose of gabapentin versus placebo in patients during the acute phase of HZ [177], and it has also been reported that open-label treatment of a sample of 64 patients with HZ, by use of the combination of gabapentin and the antiviral agent valacyclovir, appeared to reduce the incidence of PHN at 3 and 6 months after rash onset, compared with the results of published studies of antiviral monotherapy [178]. Further evidence that these medications have the potential to reduce acute pain in HZ is provided by the results of studies of acute postoperative pain, in which perioperative administration of gabapentin, compared with placebo, reduced pain or opioid requirements [179].
Considered together, the efficacy of gabapentin and pregabalin for the treatment of PHN and other chronic neuropathic pain syndromes, the beneficial effects of gabapentin on a variety of acute pain conditions, and recent animal model data [180], suggest that these medications might reduce acute pain in patients with HZ and possibly further reduce the risk of PHN beyond that achieved with antiviral therapy administered alone. However, in preliminary data analyses from a randomized trial [169], gabapentin titrated to a maximum dosage of 1800 mg daily did not differ from placebo in reducing acute pain in HZ within the first 2–3 weeks after rash onset. This may suggest that dosages of gabapentin higher than the 1800 mg administered daily in this study are necessary for treatment of HZ or that treatment with pregabalin would be preferable because it can be titrated to an effective dosage more rapidly than gabapentin [181], which is an important consideration when treating patients whose acute pain can begin suddenly and can often be severe. Although both gabapentin and pregabalin are used in the treatment of epilepsy, other anticonvulsant medications are not recommended for patients with HZ, because of their lack of proven efficacy in PHN, poor tolerability, or risks of clinically significant adverse events.
Neural blockade. Sympathetic and epidural nerve blocks have been used for the treatment of severe pain in patients with HZ for many years, but few controlled studies have examined their effects on acute pain or PHN [182,183–184]. The results of a recent randomized trial involving patients with HZ treated with oral antiviral therapy demonstrated that a single epidural injection of steroids and local anesthetics relieved acute pain within the first month after rash onset significantly better than did the standard of care but did not reduce the risk of developing PHN [185]. Treatment with multiple epidural injections of local anesthetic and methylprednisolone without antiviral therapy during HZ was associated with a reduction in the incidence of PHN, compared with that associated with intravenous acyclovir and prednisolone [186]. Given the well-established efficacy of antiviral therapy in patients with HZ, however, the results of this study have limited clinical relevance, because antiviral therapy was withheld from the patients who received epidural injections. Continuous epidural infusion of local anesthetic with intermittent additional epidural anesthetic boluses was superior to continuous infusion of saline and intermittent anesthetic boluses in reducing the time to complete cessation of pain in patients with HZ treated with acyclovir [187]. Although treatment of patients with HZ by use of multiple epidural injections or continuous epidural infusions is unlikely to be feasible in most settings, these data suggest that aggressive analgesia can be efficacious in patients with HZ.
Other treatments. A trial of intravenous VZV hyperimmune globulin versus placebo in patients >50 years of age with a dermatologic diagnosis of HZ treated with intravenous acyclovir found a reduction in the incidence of pain 5 weeks after rash onset; however, the effect of treatment on chronic pain could not be determined because of the short follow-up duration [188]. Percutaneous electrical nerve stimulation administered 3 times each week for 2 weeks in patients with HZ was superior to famciclovir for some but not all cutaneous and acute pain end points, and for PHN severity but not incidence [189], but the absence of adequate blinding in this study limits interpretation of the data. Although topical capsaicin may have benefit in some patients with PHN [190], there is no basis for its use in patients with HZ, in whom it can be expected to exacerbate pain.
Recommendations for Supplementing Antiviral Therapy
Even if the risk of developing PHN is not reduced by combining antiviral therapy with analgesic or corticosteroid treatment in patients with HZ, effective relief of acute pain is a very desirable treatment goal. Pain should be assessed and treated promptly, and the choice of treatment approaches depends on the patient's pain severity and underlying conditions and on any prior response to specific medications. The principles of state-of-the-art pain management, such as the use of standardized pain measures, scheduled analgesia, and consistent and frequent follow-up to adjust dosing to the needs of the patient, should be applied to the management of pain in patients with HZ. It is important to recognize that HZ pain changes over time and can become more severe as the acute infection progresses [191].
Patients with mild to moderate pain may be managed with acetaminophen or NSAIDs, alone or in combination with a weak opioid analgesic (e.g., codeine) or tramadol. It is important to prescribe these medications to achieve a constant level of analgesia (e.g., every 6 h) rather than to use as-needed dosing for increased levels of pain. These commonly used medications, however, have not been studied for the treatment of HZ. For pain that is moderate to severe in intensity, which is often accompanied by disturbed sleep, treatment with a strong opioid analgesic (e.g., oxycodone or morphine) is recommended on the basis of the consistent efficacy of this class of medications in patients with inflammatory and neuropathic pain (table 2). Various approaches may be used to treat HZ-associated pain with the numerous short- and long-acting opioid analgesics that are available. One approach is to begin treatment with a short-acting medication at an oxycodone equianalgesic dosage of 5 mg given 4 times daily as needed. Commonly used short-acting opioid analgesics include oxycodone alone or in combination with acetaminophen or aspirin. Once an effective dosage is determined, treatment can be switched from a short-acting to a long-acting medication, which is more convenient for patients and may also provide a more consistent level of pain relief; for exacerbations of pain, treatment with a short-acting opioid can be continued on an as-needed basis, in combination with the long-acting opioid. One of the most common adverse effects of opioid analgesics is constipation, which can be managed with preemptive laxative and stool-softener therapy. The risk that substance abuse will develop in patients who do not have a history of substance abuse is unknown, but is thought to be low in older individuals with HZ.
Corticosteroid and analgesic medications that can be considered for treatment of patients with herpes zoster.
If moderate to severe pain in patients with HZ has not responded rapidly to treatment with an opioid analgesic, the prompt addition of one of the following 3 classes of oral medications in combination with the opioid analgesic should be considered, even though few studies have examined whether the risk of PHN is reduced by such treatment: (1) gabapentin or pregabalin; (2) TCAs, especially nortriptyline; or (3) corticosteroids (e.g., prednisone), if there are no contraindications (table 2). For those patients with moderate or severe pain who are unable to tolerate an opioid analgesic, treatment with these 3 classes of medications, alone and in combination, can be considered.
Gabapentin and pregabalin can both cause sedation, and tolerability may be improved with initial doses given only at bedtime and subsequent dosage increases administered 3 times daily for gabapentin and twice daily for pregabalin. The first 2 weeks after rash onset can be expected to be associated with the greatest benefit of treatment. Aggressive titration to rapidly reach the maximum dosages of 3600 mg of gabapentin daily and 600 mg of pregabalin daily must be balanced against the risk of greater adverse effects. Final dosages of gabapentin and pregabalin should be determined by relief of pain or the development of unacceptable adverse effects that do not resolve within 1 or 2 days.
Although most clinical trials of TCAs for the treatment of neuropathic pain have examined amitriptyline, it is not recommended for elderly patients, because of the risk of significant adverse events. In a randomized double-blind trial, nortriptyline was found to provide equivalent analgesic benefits for patients with PHN, when directly compared with amitriptyline, but was better tolerated [192]. Nortriptyline is, therefore, preferable, although desipramine can be considered for patients with excessive sedation from nortriptyline. Nortriptyline treatment can be initiated at a dosage of 25 mg (or less for frail or elderly patients) at bedtime and then titrated by 25 mg daily every 2–3 days as tolerated, until relief of pain or a maximum dosage of 150 mg daily is reached. Patients must understand that TCAs have an analgesic effect that is independent of their antidepressant effect.
Corticosteroids can be considered as soon as possible after diagnosis for patients with at least moderately severe pain and no contraindications. In addition, corticosteroids should be considered for patients with VZV-induced facial paralysis and cranial polyneuritis to improve motor outcomes, peripheral nerve damage from foraminal compression, or evidence of CNS involvement, although the benefit of such treatment has not been systematically studied. Contraindications (e.g., hypertension, diabetes, gastritis, osteoporosis, and psychosis) and risks associated with the use of corticosteroids must be carefully evaluated. Treatment with corticosteroids should be initiated only in combination with antiviral therapy. There is no evidence base for the use of topical corticosteroids for treatment of patients with HZ, and such treatment is not recommended.
For patients with pain that is inadequately controlled by antiviral agents in combination with oral analgesic medications and/or corticosteroids, referral to a pain specialist or pain center is recommended to evaluate eligibility for neural blockade. Although long-term benefits of neural blockade in HZ have not been established, these procedures can reduce severe acute pain, and their risk-benefit ratio is therefore likely to be favorable. Patients with the most severe lesions and pain may benefit from hospitalization and administration of epidural analgesics.
Treatment of Immunocompromised Patients
Patients with disorders of cell-mediated immunity (due to disease or medical interventions) are at increased risk for development of HZ. Those patients with the greatest degree of immunosuppression are at highest risk for VZV dissemination and visceral organ involvement. Populations at special risk include patients with lymphoproliferative malignancies, organ transplant recipients, patients receiving systemic corticosteroids, and patients with AIDS.
HZ in the setting of malignancy or organ transplantation. Initial clinical trials with intravenous acyclovir for localized or disseminated HZ in immunocompromised patients demonstrated that treatment halts disease progression and reduces the duration of viral replication [193, 194]. Subsequent studies of bone marrow transplant recipients proved that acyclovir, in addition to promoting faster disease resolution, is highly effective at preventing VZV dissemination [195, 196]. Because most VZV-related fatalities result from disseminated infection, the ability to prevent dissemination has markedly reduced the rate of death due to HZ in transplant recipients.
Intravenous acyclovir remains the therapy of choice for VZV disease in severely immunocompromised patients, including (1) allogeneic hematopoietic stem cell transplant recipients within 4 months of transplantation, (2) hematopoietic stem cell transplant recipients with moderate to severe acute or chronic graft-versus-host disease, or (3) any transplant recipient receiving aggressive antirejection therapy. In addition, any transplant recipient with suspected visceral dissemination (e.g., encephalitis or pneumonitis) should receive intravenous acyclovir. The recommended dose is 10 mg/kg (or 500 mg/m2) every 8 h. When the infection is controlled, intravenous administration can be stopped, and oral antiviral medication can be initiated for the remainder of the course of therapy.
For immunocompromised patients, treating HZ with oral antiviral agents on an outpatient basis is an attractive approach, although data are limited. One small study randomized 27 allogeneic hematopoietic stem cell transplant recipients with HZ to receive either oral or intravenous acyclovir. No VZV dissemination occurred in either group, and no differences in healing or clinical outcome were apparent [197]. Published data from clinical trials of famciclovir and valacyclovir for the treatment of HZ in immunocompromised patients remain limited, but a growing body of clinical experience suggests that these medications are safe and effective in this setting [198, 199]. For less severely immunosuppressed patients, oral therapy with acyclovir (800 mg 5 times daily), valacyclovir (1000 mg 3 times daily), or famciclovir (500 mg 3 times daily), coupled with close clinical observation, is a reasonable option. The higher plasma drug concentrations achievable with famciclovir and valacyclovir, along with their simplified dosing schedule, favor the use of these medications rather than oral acyclovir. Brivudin is not recommended for immunocompromised patients, even though it is effective [200], because of its potentially fatal interaction with 5-fluorouracil and other 5-fluoropyrimidines used in cancer chemotherapy. Because of the risk of ocular involvement, intravenous acyclovir and evaluation by an ophthalmologist is recommended for highly immunocompromised patients who present with HZ ophthalmicus [201].
HZ in HIV-seropositive patients. Prospectively acquired data to guide clinicians when selecting antiviral therapy for HZ in HIV-seropositive patients are currently limited. Nearly 300 HIV-infected patients with HZ were enrolled in controlled studies comparing orally administered acyclovir (800 mg 5 times daily) with sorivudine (40 mg once daily) [202, 203]. Times to cessation of new vesicle formation, total crusting, and resolution of HZ-associated pain were 3–4 days, 7–8 days, and ∼60 days, respectively [203]. Although sorivudine was never marketed, these studies clearly confirmed the efficacy and safety of oral antiviral therapy for HZ in patients with HIV infection. Famciclovir was judged to be effective and safe for treatment of HZ in patients with AIDS when evaluated in a small, open-label clinical trial [204]. Valacyclovir has not been systematically evaluated as a treatment for HZ in HIV-infected patients, although preliminary data [199] and anecdotal clinical experience suggest therapeutic benefit. Patients who have HZ ophthalmicus should always be treated to reduce the risk of serious ocular complications, even when presenting >72 h after rash onset [205, 206]. Because of the documented risk of relapsing infection, VZV disease in HIV-seropositive patients should be treated until all lesions have healed, which is often longer than the standard 7- to 10-day course. What impact VZV therapy may have on the risk of subsequent complications, such as CNS infection or retinitis, is unknown. Adjunctive therapy for HZ with corticosteroids has not been evaluated in HIV-infected patients and is not currently recommended. Long-term administration of anti-VZV medications to prevent recurrences of HZ is not routinely recommended for HIV-infected patients.
Although rare, acyclovir-resistant VZV has been reported in immunocompromised patients, especially those with HIV infection, and results from mutations in the thymidine kinase gene. The presence of atypical lesions or a failed clinical response should prompt evaluation for drug susceptibility to determine whether resistance has developed. When acyclovir resistance occurs, treatment with alternative medications (e.g., intravenous foscarnet or cidofovir) is required.
Management of acute pain in HZ and PHN is similar in immunocompromised and immunocompetent patients, although NSAIDs that are not cyclooxygenase II–specific inhibitors are contraindicated in thrombocytopenic patients.
Treatment of Complicated Presentations of Hz
HZ ophthalmicus and VZV retinitis. HZ ophthalmicus is second only to thoracic HZ in frequency [207]. Two surveys of all cases of HZ occurring between 1935 and 1959 in Rochester, Minnesota, found a trigeminal HZ incidence of 9%–16% [208, 209], which is within the 8%–56% range found in other studies [32, 210, 211]; some of these estimates, however, may have been biased by a greater tendency for patients with facial or periocular rashes to seek medical attention. A trigeminal HZ incidence of ∼10.7% was found for the 660 evaluable cases of HZ in the placebo group of the Shingles Prevention Study [212]. Without antiviral therapy, 50%–72% of patients with periocular HZ will have involvement of the ocular structures and develop chronic disease; in one recent study, 20% of patients with HZ uveitis were found to be legally blind in the involved eye [213].
The list of complications is protean: scarred lid malfunction or loss; paralytic ptosis; conjunctivitis; episcleritis; scleritis; infectious or neurotrophic keratitis; iridocyclitis; hemorrhagic retinitis; acute retinal necrosis; choroiditis; papillitis; retrobulbar neuritis; optic atrophy; Argyll Robertson pupil; partial or complete third, fourth, or sixth nerve palsy (always self-resolving); isolated pupillary paralysis; internuclear ophthalmoplegia; acute and chronic glaucoma; orbital apex syndrome; PHN; and sympathetic ophthalmia [210, 214,215,216,217–218].
Therapy for HZ ophthalmicus is similar to that for HZ elsewhere in the body but should include the care of an ophthalmologist familiar with the disease. Treatment includes the following [217, 218]: (1) approved dosages of famciclovir or valacyclovir for 7–10 days, preferably started within 72 h of rash onset (with intravenous acyclovir given as needed for retinitis), to resolve acute disease and inhibit late inflammatory recurrences [136, 219,220,221–222]; (2) pain medications, as discussed above; (3) cool to tepid wet compresses (if tolerated); (4) antibiotic ophthalmic ointment administered twice daily (e.g., bacitracin-polymyxin), to protect the ocular surface; (5) topical steroids (e.g., 0.125%–1% prednisolone 2–6 times daily) prescribed and managed only by an ophthalmologist for corneal immune disease, episcleritis, scleritis, or iritis; (6) no topical antivirals, because they are ineffective; (7) mydriatic/cycloplegia as needed for iritis (e.g., 5% homatropine twice daily); and (8) ocular pressure–lowering drugs given as needed for glaucoma (e.g., latanaprost once daily and/or timolol maleate ophthalmic gel forming solution every morning). Systemic steroids are indicated in the presence of moderate to severe pain or rash, particularly if there is significant edema, which may cause orbital apex syndrome through pressure on the nerves entering the orbit [218]. The dosage is commonly 20 mg of prednisone administered (together with an oral antiviral agent) orally 3 times daily for 4 days, twice daily for 6 days, and then once daily every morning for 4 days.
Therapy for chronic problems includes the following: (1) lubricating, preservative-free artificial tear gels or tears administered 4 times daily, antibiotic ointment administered once daily, and, possibly, lateral tarsorrhaphy to protect the corneas (which are often hypesthetic/anesthetic as a result of neuronal damage) from breakdown; (2) continuous-wear, therapeutic soft contact lenses and antibiotic drops (e.g., polymyxin-trimethoprim given 4 times daily as needed for corneal ulceration); (3) topical steroids and antibiotics for inflammatory disease (iritis, episcleritis, scleritis, and immune keratitis); (4) dilation for iritis; (5) glaucoma therapy as needed; and (6) surgical management as needed—for example, for amniotic membrane transplantation, tissue-adhesive seal ulcers, keratoprosthesis, and glaucoma trabeculectomy. Chronic pain management is generally similar to that for PHN in other dermatomes and includes gabapentin or pregabalin, TCAs, opioid analgesics, and lidocaine gel (which is preferable to the lidocaine patch for periophthalmic use). Local nerve blocks or sympathetic blocks can be used for pain that is refractory to first-line therapy, although there are no controlled studies of these treatments [223,224–225].
The optimal antiviral therapy for VZV-induced, rapidly progressive herpetic retinal necrosis in immunocompromised patients remains undefined. Responses to intravenous acyclovir or ganciclovir have been inconsistent and disappointing, with 49%–67% of involved eyes progressing to no light perception [91, 226]. Several case reports have reported improved preservation of vision in patients treated with a combination of intravenous ganciclovir plus foscarnet, with or without intravitreal antivirals [227,228,229,230,231–232]. Cidofovir has also been used successfully in a small number of patients [233, 234]. The optimal duration of induction therapy and options for long-term maintenance therapy have not been established.
Acute retinal necrosis in immunocompetent patients is a less virulent disease and responds better to antiviral therapy. For such patients, acyclovir is clearly beneficial for preserving useful vision [235]. A suggested antiviral regimen for acute retinal necrosis in the otherwise healthy host is intravenous acyclovir (10–15 mg/kg every 8 h for 10–14 days) followed by oral valacyclovir (1 g 3 times daily for 4–6 weeks), although this treatment approach has not been studied in a controlled fashion.
Vulnerable and frail elderly patients. The health status of older adults varies widely, from well elderly individuals who have no diseases or functional problems to chronically ill elderly individuals who have multiple comorbidities and disabilities. Vulnerable elderly individuals are people ≥65 years of age who are at increased risk for death or functional decline in a 2-year period, as defined by older age, poor self-rated health, and decreased functional status [236]. Frail elderly individuals, a subset of vulnerable elderly individuals, are at the highest risk for death and functional decline and are characterized clinically by weakness, easy exhaustion, low levels of physical activity, slow walking speed, undernutrition/weight loss, and functional decline [237]. Importantly, functional status is a more important predictor of death and functional decline than are specific clinical conditions. These individuals have markedly diminished physiologic reserves for responding to stressors, including such acute illnesses as HZ. Cutaneous dissemination and, possibly, visceral dissemination seem to be more common in elderly individuals. Moreover, the pain and acute inflammation of HZ puts vulnerable and frail elderly individuals at risk for physical inactivity, poor oral intake with resultant undernutrition, cognitive impairment, depression, and functional decline. The insult of HZ can trigger a change of living environment in a frail elderly individual who is living alone and experiences functional decline.
Hence, when HZ occurs in this population, it is important to modify pharmacotherapeutic approaches and augment nonpharmacotherapeutic approaches to management. Starting dosages of medications should be lower than those recommended for younger individuals, and the dosage should be titrated more slowly, particularly for opioid analgesics, gabapentin, pregabalin, TCAs, and NSAIDs. These individuals experience significant age- and disease-related declines in glomerular filtration rate, so the dosages of renally excreted medications (e.g., antiviral agents, gabapentin, and pregabalin) must be adjusted, as is discussed further below [238]. Furthermore, these individuals are at high risk for adverse drug effects because of multiple comorbidities, age-related changes in pharmacokinetics and dynamics, use of multiple medications, and frequent inappropriate prescribing [239]. The choice of medications should take into account the patient's diseases, medication regimen, and adverse event experiences. For example, NSAIDs should be avoided in elderly individuals with congestive heart failure and chronic kidney disease. For nonpharmacotherapeutic approaches, it is critically important for the practitioner to recognize that these treatments are just as important as the use of medications. Nonpharmacologic approaches include maintaining physical activity, enhancing nutrition, maintaining or increasing social contact, and providing assistance for problems with basic and instrumental activities of daily living during the acute episode. These interventions usually require a multidisciplinary approach that involves nursing, social work, physical therapy, occupational therapy, and the family.
The clinical course of vulnerable and frail elderly individuals needs to be monitored more closely than does that of well elderly individuals, to detect inadequate responses to therapy and early functional decline and to step up interventions, if needed. Pharmacotherapeutic and nonpharmacologic approaches require particular attention in individuals with dementia. HZ pain and acute inflammation may worsen cognition in these individuals with dementia, who then may require additional assistance in obtaining proper treatment and performing activities of daily living. The management of HZ pain is more complicated in patients with dementia, because of the risk for adverse cognitive effects of opioid analgesics, gabapentin, pregabalin, and TCAs. In addition, traditional pain measures (e.g., the 0–10 numerical rating scale) used to track response to analgesics are not useful in assessing patients with advanced dementia [240]. Finally, when frail elderly individuals are residents of nursing homes, prompt recognition and initiation of antiviral treatment of HZ can prevent the spread of VZV to susceptible individuals, such as younger nurses and aides in the facility [241].
Pregnant and nursing patients. Maternal varicella can be transmitted to the fetus and cause significant morbidity, but congenital varicella has never been documented in association with maternal HZ. There are no adequate studies of the effects that antiviral therapy during pregnancy has on the developing child, although rates of birth defects reported in registry data for acyclovir and valacyclovir are reassuring (similar data are not available for famciclovir and brivudin) [242]. Because the safety of antiviral therapy during pregnancy has not been firmly established, pregnant women with HZ should be treated only in cases in which the potential benefits of antiviral therapy to the mother outweigh the potential risks to the fetus. The majority of pregnant women with HZ are expected to have a relatively low risk of developing PHN, because of their age. However, patients with severe rash, severe acute pain, or HZ ophthalmicus can be treated with acyclovir and valacyclovir, especially during the late stages of pregnancy, when any potential risks to the fetus should be lower. However, during the early stages of pregnancy, the potential benefit of antiviral therapy to the mother must be great enough to outweigh the unknown but potentially greater risk to the fetus. Antiviral therapy is not routinely recommended for eclamptic, preeclamptic, or diabetic pregnant women.
Because acyclovir is excreted in breast milk, antiviral therapy should be administered to nursing mothers with caution and only in circumstances in which the benefits are well established (e.g., within 72 h of rash onset). Severe acute pain in pregnant patients with HZ can be safely treated with opioid analgesics, but this must then be considered in the management of the neonate.
Neurologic complications of HZ. The role of antiviral agents in the management of neurologic complications of HZ has not been evaluated in a controlled fashion. For those diseases in which viral replication likely plays an important role in pathogenesis (e.g., meningitis, encephalitis, and myelitis), therapy with intravenous acyclovir is recommended; this approach is supported by benefits noted in anecdotal experience. For such conditions as delayed contralateral hemiparesis, in which the role of active viral replication is less clear, the value of antiviral therapy is uncertain, but the potential benefits of antiviral therapy outweigh any potential risks [243].
Renal failure. Dosages should be adjusted if renal insufficiency is present when acyclovir (creatinine clearance, <25 mL/min), famciclovir (creatinine clearance, <60 mL/min), or valacyclovir (creatinine clearance, <50 mL/min) is used. Because brivudin undergoes hepatic as well as renal excretion, dosage reduction for renal insufficiency is less critical, but hepatic function must be considered when this antiviral agent is used. Dosages of gabapentin and pregabalin should be reduced when renal function is impaired.
Recommendations for Future Research
Major advances have been made in the prevention and treatment of HZ and PHN. To further reduce the personal and social burden of HZ, additional research on the natural history of HZ is necessary and should include studies of the following: (1) the impact of varicella and HZ vaccination on epidemiological aspects of HZ and its complications; (2) the risk factors for HZ and its complications—for example, the role of immunosenescence, nervous system senescence, greater HZ severity, and medical comorbidity in explaining why older patients with HZ have a greater risk of developing PHN; (3) methods for the early identification of HZ by patients and health care providers, so that treatment is initiated as promptly as possible in those who are at risk for the development of complications; (4) methods for identifying HZ before the rash appears and in patients with very mild rashes; (5) methods for identifying patients with zoster sine herpete; (6) the mechanisms of pain in HZ and PHN and of the transition from acute pain to PHN; and (7) the role of VZV in neurologic and other diseases.
Additional research on the prevention and treatment of HZ and on the prevention of its complications, especially PHN, is also necessary and should include studies of the following: (1) improved (e.g., lipophilic) antiviral therapy for HZ; (2) treatments for acute pain in patients with HZ (e.g., to determine whether NSAIDs are efficacious); (3) strategies to prevent PHN, ideally based on improved knowledge of pain mechanisms; (4) novel strategies to block reactivation of VZV or to eliminate latent infection within neurons; (5) research on extending the use of the live attenuated HZ vaccine to frail elderly individuals, immunocompromised patients, and individuals <60 years of age; (6) the development of noninfectious (inactivated) HZ vaccines for use in immunocompromised individuals; (7) the development and evaluation of epitope-specific recombinant DNA vaccines for HZ that would selectively stimulate VZV-specific cell-mediated immune responses; (8) methods for identifying which patients would benefit from antiviral therapy initiated >72 h after rash onset; and (9) methods for identifying which patients would benefit from antiviral therapy extending for >7 days. Both of the latter 2 objectives should be a priority for research on HZ.
We anticipate that ongoing and planned research will address these questions and that clinical trials will identify additional treatments with efficacy in the prevention and treatment of HZ and PHN, and we therefore recommend that these clinical recommendations be updated within 5 years.
acknowledgments
We dedicate these recommendations to the memory of Richard T. Perkin, whose passion for supporting research and education to reduce the suffering caused by chickenpox, herpes zoster, and postherpetic neuralgia is an enduring inspiration. We thank Paul Lambiase and Mary Gleichauf of the University of Rochester Office of Professional Education for invaluable support.
Financial support. The consensus meeting on which these recommendations are based was supported by unrestricted grants to the University of Rochester Office of Professional Education from the International Association for the Study of Pain Neuropathic Pain Special Interest Group, the Neuropathic Pain Institute, and the VZV Research Foundation.
Supplement sponsorship. This article was published as part of a supplement entitled “Recommendations for the Management of Herpes Zoster,” sponsored by the International Association for the Study of Pain Neuropathic Pain Special Interest Group, the Neuropathic Pain Institute, and the VZV Research Foundation.
Potential conflicts of interest. All authors received an honorarium for participation in the consensus meeting from the University of Rochester Office of Professional Education. R.H.D. has received research support, consulting fees, or honoraria in the past year from Allergan, Astellas Pharma, Cephalon, Dov Pharmaceuticals, Eli Lilly, Endo Pharmaceuticals, EpiCept Corporation, Fralex Therapeutics, Johnson & Johnson, Merck, NeurogesX (also stock options), Novartis, Pfizer, Schwarz Pharma, US Food and Drug Administration, US National Institutes of Health, and US Veterans Administration; R.W.J. has received consulting or lecture fees from DepoMed, Merck, Novartis, Sanofi Pasteur MSD, and Yamanouchi; J.B. has served on advisory boards for GlaxoSmithKline, Merck, and Sanofi Pasteur; J.W.G. has received research support, consulting fees, or honoraria from Astellas Pharma, GlaxoSmithKline, Merck, and Novartis; M.J.L. has received consulting fees from GlaxoSmithKline and Merck and shares a patent with Merck for the herpes zoster vaccine; M.B. has received research support, consulting fees, or honoraria in the past year from Allergan, Astellas Pharma, Cephalon, Eli Lilly, Eisai, Johnson & Johnson, Merck, NeurogesX, Pfizer, Schwarz Pharma, and Xenoport; A.A.G. has received consulting or lecture fees from GlaxoSmithKline and Merck; M.L.H. has received consulting fees or honoraria in the past year from AstraZeneca, Mundipharma MSD, and Pfizer; M.W.M has served on an advisory board for Sanofi Pasteur MSD in the past year; T.J.N. has received research support, consulting fees, or honoraria in the past year from Eli Lilly, GW Pharma, Medtronic, Merck, Pfizer, Schwarz BioSciences, and UCB Pharma; K.L.P. has received consulting fees or honoraria in the past year from CV Therapeutics, Eli Lilly, Evotech, NeurogesX, Neuromed, Organon, and Roche; M.C.R. has received consulting fees or royalties in the past 12 months from Alnylam, Biogen, Eli Lilly, Hind Health Care, Metaphore, and NeuroMolecular; K.E.S. has received research support and consulting fees from Merck; B.R.S. has received consulting fees or honoraria in the past year from Pfizer, Lilly, and Depomed; S.K.T has received research support, consulting fees, or honoraria from Astellas Pharma, Catalyst, GlaxoSmithKline, Merck, and Novartis; A.J.M.vW. has received honoraria from Pfizer and Sanofi Pasteur MSD; S.W.W. has received consulting fees or honoraria in the past year from Berlin Chemie, GlaxoSmithKline, Menarini Group, Sanofi Pasteur MSD, and Stockhausen Degussa; M.S.W. has received consulting fees from Endo Pharmaceuticals and honoraria from Pfizer in the past year; R.J.W. is on the Scientific Advisory Board for Gilead and the speakers bureaus for GlaxoSmithKline and Novartis. All other authors: no conflicts.
references
Figures and Tables

Cervical herpes zoster (photograph provided by A.L.O.)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments