
Abstract
Purpose
Epidemiologic and clinical research suggests important gender-related differences in the prevalence, presentation, associated conventional and non-conventional risk factors, management and outcomes of coronary heart disease (CHD) patients. Adequate data is not available for Indian population where prevalence of CHD and depression is high.
Method
We conducted an observational, single-center, study from January 2010 to December 2011 on 10450 consecutive patients visiting a tertiary care center, Ahmedabad, Gujarat, India who presented with complaints related to CHD.
Results
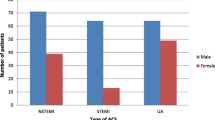
Of these, 6867 patients had coronary artery disease (CAD) as confirmed by angiographic investigation; 5678 were males, and 1189 were females with similar mean age. As compared to males, females had higher prevalence of hypertension, diabetes and obesity while males had higher prevalence of smoking. Invasive treatment options like Coronary Artery Bypass Grafting (p < 0.001) and Percutaneous Coronary Intervention (p = 0.001) were used less often to treat females, and medical therapy (p < 0.001) was the preferred treatment option irrespective of the contributing risk factors/extent of CAD. Depression was observed in 39.8 % of acute coronary syndrome patients (n = 1648) as assessed by MARDS scale. It was higher in female patients and in low socioeconomic strata (p < 0.001).At 12 and 36 months, rates of revascularization (p < 0.001) and mortality (p < 0.005) were higher with poor quality of life (QoL) (P < 0.001) in depressed CAD patients.
Conclusion
In India, women appear to have a higher prevalence of hypertension, diabetes, obesity, and family history of CHD. Yet women get invasive treatments less often than men. Depression is also more common in women and is associated with poor QoL and early mortality than men.


Similar content being viewed by others


References
National Cardiovascular Disease Database. http://www.whoindia.org/LinkFiles/NMH_Resources_National_CVD_database-Final_Report.pdf. Accessed 17 Oct 2015.
National Programme for Prevention and Control of Diabetes, Cardiovascular Diseases and Stroke (NPDCS) 2009. Ministry of Health & Family Welfare, Government of India Press, New Delhi, India. http://www.searo.who.int/india/topics/cardiovascular_diseases/NCD_Resources_Training_module_for_NPDCS_for_health_workers.pdf. Accessed 23 Dec 2015.
Regitz-Zagrosek V. Therapeutic implications of the gender-specific aspects of cardiovascular disease. Nat Rev Drug Discov. 2006;5(5):425–38.
Keyhani S, Scobie JV, Hebert PL, McLaughlin MA. Gender disparities in blood pressure control and cardiovascular care in a national sample of ambulatory care visits. Hypertension. 2008;51:1149–55.
Judith HL, Thomas B, James AB, Nancy FS, Peter GK, François L. Depression and Coronary Heart Disease. Circulation. 2008;118:1768–75.
Carlos VS, Karina TS, Erica S, Anna MA, Renério F. Association between depression and development of coronary artery disease: pathophysiologic and diagnostic implications. Vasc Health Risk Manag. 2011;7:159–64.
Mark H, Gerard JM, Emmanuel S. Psychological distress as a risk factor for cardiovascular events: pathophysiological and behavioral mechanisms. J Am Coll Cardiol. 2008;52(25):2163–5.
Danielle BL, Itamar SS, Ana MC, Almeida Ribeiro MC. Cardiovascular risk in individuals with depression. Rev Assoc Med Bras. 2013;59(3):298–304.
von Käne R. Psychosocial stress and cardiovascular risk – current opinion. Swiss Med Wkly. 2012;142:w13502.
Socioeconomic review of Gujarat 2012-2013.directorate of economics and statistics. Govt. of Gujarat, India. http://www.indiaenvironmentportal.org.in/files/file/Gujaratc20Socio20Economic20Review202012-13.pdf. Accessed 25 Jan 2015.
Global Status Report of NCD. Geneva: World Health Organization; 2011. ISBN: 978 92 4 156422 9; 2010.
Lett HS, Blumenthal JA, Babyak MA, Catellier DJ, Carney RM, Berkman LF, et al. Social support and prognosis in patients at increased psychosocial risk recovering from myocardial infarction. Health Psychol. 2007;26(4):418–27.
Carney RM, Freedland KE, Miller GE, Jaffe AS. Depression as a risk factor for cardiac mortality and morbidity: a review of potential mechanisms. J Psychosom Res. 2002;53:897–902. doi:10.1186/1741-7015-11-131.
Thomas AJ, Kalaria RN, O’Brien JT. Depression and vascular disease: what is the relationship? J Affect Disord. 2004;79:81–95.
Kubzansky LD, Kawachi I. Going to the heart of the matter: do negative emotions cause coronary heart disease? J Psychosom Res. 2000;48:323–37.
Everson-Rose SA, Lewis TT. Psychosocial factors and cardiovascular diseases. Annu Rev Public Health. 2005;26:469–500.
Appels A. Depression and coronary heart disease: observations and questions. J Psychosom Res. 1997;43:443–52.
Parashar S, Rumsfeld JS, Spertus JA, Reid KJ, Wenger NK, Krumholz HM, et al. Time course of depression and outcome of myocardial infarction. Arch Intern Med. 2006;166:2035–43. doi:10.1001/archinte.166.18.2035.
Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case–control study. Lancet. 2004;364:937–52.
O’Donnell MJ, Xavier D, Liu L, Zhang H, Chin SL, Rao-Melacini P, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case–control study. Lancet. 2010;376:112–23.
Judith HL, Bigger JT, Blumenthal JA, Smith NF, Kaufmann PG, François L, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the american heart association prevention committee of the council on cardiovascular nursing, council on clinical cardiology, council on epidemiology and prevention, and interdisciplinary council on quality of care and outcomes research: endorsed by the american psychiatric association. Circulation. 2008;118:1768–75.
Rajeev G, Soneil G, Krishna Kumar S, Arvind G, Prakash D. Regional variations in cardiovascular risk factors in India: India heart watch. World J Cardiol. 2012;4(4):112–20.
Thombs BD, Bass EB, Ford DE. Prevalence of depression in survivors of acute myocardial infarction and review of evidence. J Gen Intern Med. 2006;21:30–8.
Kessler RC. Epidemiology of women and depression. J Affect Disord. 2003;74:5–13.
Pilote L, Dasgupta K, Guru V, Humphries KH, McGrath J, Norris C, et al. A comprehensive view of sex-specific issues related to cardiovascular disease. CMAJ. 2007;176:S1–44.
Erica C, Leifheit L, Kimberly JR, Stanislav VK, Haiqun L, Philip GJ, et al. The role of social support in health status and depressive symptoms after acute myocardial infarction: evidence for a stronger relationship among women. Circ Cardiovasc Qual Outcomes. 2010;3(2):143–50.
Shah AJ, Ghasemzadeh N, Zaragoza Macias E, Patel R, Eapen DJ, Neeland IJ, et al. Sex and age differences in the association of depression with obstructive coronary artery disease and adverse cardiovascular events. Am Heart Assoc. 2014;3:e0007414.
Conflict of Interest
The authors have no conflict of interest to disclose
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Bhatt, P., Parikh, P., Patel, A. et al. Unique Aspects of Coronary Artery Disease in Indian Women. Cardiovasc Drugs Ther 29, 369–376 (2015). https://doi.org/10.1007/s10557-015-6594-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10557-015-6594-5