
Summary
Background
The psychometric properties of an instrument, the Activity Scale for Kids-performance (ASKp), were assessed which was proposed to capture physical functioning after allogeneic hematopoietic stem cell transplantation (HSCT). Additionally, this multicenter observational prospective study investigated the influence of clinical correlates focusing on chronic graft-versus-host disease (cGVHD).
Methods
Patient-reported ASKp, clinician-reported Karnofsky/Lansky status (KPS/PSS), patient characteristics and cGVHD details were assessed of 55 patients with a median age of 12 years at baseline after day +100 post-HSCT and every 3 months during the next 18 months. The psychometric properties were evaluated and ASKp and KPS/PSS status was compared using ANOVAS and multiple regression models.
Results
The German version of the ASKp showed good psychometric properties except for ceiling effects. Discrimination ability of the ASKp was good regarding the need for devices but failed to predict cGVHD patients. Both the ASKp and the KPS/PSS were associated with patients after adoptive cell therapy being in need for devices, suffering from overlap cGVHD and from steroid side effects but not with patients’ age and gender. In contrast to the KPS/PSS the ASKp only showed significant differences after merging moderate and severe cGHVD patients when comparing them to No-cGVHD (F = 4.050; p = 0.049), being outperformed by the KPS/PSS (F = 20.082; p < 0.001).
Conclusion
The ASKp showed no clear advantages compared to KPS/PSS even though economical and patients’ effort was higher. Further application range may be limited through ceiling effects. Both should be taken into consideration. Therefore, the results may not support the usage of ASKp after HSCT and rather suggest KPS/PSS, both patient and clinician reported.
Similar content being viewed by others

Introduction
Allogeneic hematopoietic stem cell transplant (HSCT) offers a curative treatment for advanced malignancies and otherwise incurable diseases of hematologic or immunologic origin. The increasing number of HSCT survivors are subject to many comorbidities [1,2,3] among which the most significant affecting survival and multidimensional aspects of quality of life (QOL) are acute (aGVHD) and chronic graft-versus-host disease (cGVHD) [4, 5]. Chronic GVHD is an extremely complex multisystemic chronic disorder with heterogeneous pathogenesis [6] and clinical manifestations resembling a variety of autoimmune diseases with involvement of many tissues and organs in adults, adolescent and pediatric patients [7, 8]. Furthermore, cGVHD is associated with decreased survival, prolonged duration of immunosuppression [9], adverse physical functioning, disability [10] and decreased QOL [11, 12].
Physical functioning is of major importance for the long-term outcome after HSCT including various aspects, such as daily activity, fatigue, distress, QOL, social role and reintegration into the community. Generally, patients experience considerable physical and functional deterioration during and after HSCT. Physical activity and exercise have been shown to clearly enhance fitness, improve symptoms of sequelae and QOL both in pediatric and adult survivors. Over the last years, the number of reports and recommendations, which support the assessment of physical functioning and the implementation of physical exercise as part of the supportive care regimens for cancer and HSCT patients have increased [10, 17].
Diagnosis of cGVHD is difficult and identification of accurate standardized instruments to measure cGVHD outcomes is very important. In 2005, the National Institutes of Health (NIH) consensus development project on criteria for clinical trials in cGvHD established standardized definitions for diagnosis, severity scoring and response measures [6, 13].
A review by Krupski e al. [14] summarized the currently available trials that have shown the association of NIH-defined overall severity of cGVHD (mild, moderate and severe) and/or clinical response to cGVHD treatment with various outcome measures and QOL. Additionally, in 2005 the NIH consensus characterized overlap cGVHD, a subtype with symptoms both of acute and cGVHD, which is associated with some degree of worse outcome [11, 15].
The association between physical function and QOL in patients with cGVHD has clearly been shown outlining the importance of collecting patient reported measures in prospective studies [11, 16, 17]. In this respect, the proposed instruments of the 2005 NIH consensus [6, 13] include the human activity profile (HAP) [16] for adults and the activity scale for kids-performance (ASKp) for children [18]. The latter is a self-report measure of childhood physical disability that has shown excellent reliability in children with musculoskeletal limitations [19]. The HAP has proved to be associated with global severity, overlap subtype of cGVHD and with change in cGVHD status [11, 16].
Performance scales, such as the Karnofsky performance scale (KPS) [20] for adolescents and adults over 16 years of age, and the Lansky play performance scale (PSS) for children below 16 years of age [21] are also in use to assess functional status after HSCT [22,23,24]. Some studies have shown a negative correlation with global severity of cGVHD and with joint and fascial involvement of cGVHD [25, 26].
To our knowledge, no study has examined the performance of the ASKp in pediatric HSCT patients so far. The aim of this project was to fill this gap and to determine the psychometric properties of a German-language version of the ASKp.
Patients and methods
Patients
A German version of the ASKp was evaluated in pediatric HSCT survivors in a multicenter observational prospective study in four German HSCT centers and one Austrian center. Written informed consent in accordance with the Declaration of Helsinki and the institutional review board of the Medical University of Vienna and the St. Anna Children’s Hospital was obtained. Furthermore, the project was reviewed and approved by the institutional ethics board at each center. Patients were enrolled during regular visits at the HSCT centers. All patients and parents were informed that they were not given the individual results of the project evaluations. Inclusion criteria were a life expectancy of more than 3 months, at least 2 years of age and no evidence of recurrence of primary disease. The assessments were performed after day +100 every 3 months for 18 months (i.e. T‑0, 3, 6, 9, 12, 15 and 18 months) and when clinically indicated. A physician routinely documented patient and transplant characteristics at study entry; In addition, at all study time points the i) clinical status including KPS/PSS, relevant comorbidities such as the need for devices, gastrointestinal (GI, like nausea and malabsorption) and endocrine comorbidity (such as diabetes, hypothyroidism, adrenal dysfunction, hypogonadism), ii) corticosteroid side effects (such as Cushing syndrome and myopathy) and iii) according to the NIH consensus criteria on cGVHD global severity (mild-moderate-severe) and cGVHD severity assessment (10-point scale) [6, 13]. Patient cohorts were grouped into no cGVHD and classical cGVHD; the latter only incorporated patients with moderate and severe cGVHD as there were too few patients with mild cGVHD to analyze. Additionally, classical cGVHD included overlap subtype, presenting symptoms both of acute and cGVHD. Late acute or recurrent acute GVHD was excluded from the analyses. In accordance with the NIH criteria cGVHD-associated symptoms (cGVHD-ASS, such as eosinophilia, thrombocytopenia, (poly)serositis, nephrotic syndrome, myasthenia gravis, peripheral neuropathy) [6] were also evaluated at the time of testing. The need of help in answering the questionnaire at time of testing was categorized using a 4-point scale (1 = no help needed, 2 = questions were read to the child, 3 = help with some questions, 4 = help with most of the questions).
Activity Scale for Kids-performance (ASKp)
The ASKp is a self-reported measure of childhood physical function and physical disability, which has excellent reliability and validity [18]. The ASKp contains 30 items which are rated from 0 = never to 4 = always and covers 9 different domains. It has shown excellent measurement properties in children with musculoskeletal limitations [19] but has not been tested in HSCT patients. The ASKp domains, items and response options are displayed in Fig. 1. Possible summary scores of the ASKp range from 0 to 120 points.

ASK©-Performance SCORE SHEET. The ASKp domains, items and response options
Biostatistical methods
All statistical analyses of data accuracy, measurement properties, descriptive statistics, multiple regressions and discrimination analysis were conducted with the statistical package for Social Sciences 22.0 (SPSS Inc., Chicago, IL, USA). Corresponding assumptions for the statistical procedures were checked. The Wilcoxon sign rank test was used to analyze changes over time. Furthermore, we used aggregated data to test our other hypothesis.
Two main issues emerged out of different sample structure at each time point. First, sample composition was different at the various measurement time points. Second, aggregated individual ASKp values were affected by differences between time points. To control this, we created two different mean values across time points: we computed the ASKp mean for each patient across all time points. These mean values are not affected by different sample compositions, but by convalescence, training and other differences between time points. To control convalescence and other differences we standardized patient values at every time point by the sample mean and standard deviation at this time point. Then we computed standardized mean values across all time points. In contrast to the unstandardized mean the standardized value is not affected by time point differences but by different sample compositions at the time points. We analyzed the performance of the ASKp to predict the need of devices to measure validity. Thereby we used the receiver operating characteristic curve. The area under the curve (AUC) summarizes the power of the prediction model. The AUC values are between 0 and 1. Higher AUC values than 0.5 indicate a better prediction than expected by change and lower values vice versa. To examine the predictive value of ASKp scores and the associations of the ASKp with cGVHD we used multiple regression techniques.
Results
Of 92 HSCT study patients the ASKp was completed by 71 patients at least at 1 time point, with a complete data set of 55 patients with a median age of 12 years (range 4–23 years). Of the patients 64% were male. The underlying diseases as indication for HSCT were malignant in 78% (non-malignant in 22%) and detailed patient and HSCT characteristics at study enrolment are displayed in Table 1. Including the one patient with mild cGVHD, the no-cGVHD group consisted of 35 patients. The cohort of cGVHD patients (19) included classic chronic GVHD in 9/19 and overlap cGVHD in 10/19 patients. The NIH overall severity was moderate in 11 (58%) and severe in 7 (37%) patients. Most commonly involved organs were skin, mouth and eyes. Of note, 9/19 (47%) of cGVHD patients suffered from joint involvement. The onset type was quiescent in 6/19, progressive in 9/19 and de novo in 4/19 patients. Of the 19 cGVHD patients 17 (90%) had a history of prior aGVHD.
During the study period the ratio of patients with cGVHD to those without (no-cGVHD) was about 1:3 until time point T9 and 1:4 later. Overall, severe cGVHD was evident at 38 study points, moderate in 22 and mild cGVHD in 11 study points.
Of 8 patients with a history of adoptive cell therapy (donor-lymphocyte infusion 2/8, mesenchymal stem cells 2/8, donor-lymphocyte infusions plus mesenchymal stem cells 1/8, stem cell boost 2/8, virus-specific T cells 1/8 patients) at study enrolment, 4 patients experienced moderate or severe cGVHD (50%), all of them classified as the subtype of overlap cGVHD and 3/4 experiencing steroid side effects. Of 47 patients without adoptive cell therapy, 15 patients suffered from moderate or severe cGVHD (32%), 6 of these 15 patients presented with an overlap subtype of cGVHD and 5/15 with steroid side effects.
Item characteristics and ceiling effects
The item “I took care of my medical needs” was excluded from all further analyses because weighted mean corrected item-scale correlation across time points was low (rit = 0.18) and the reliability of the ASKp scale was higher without this item. All other items showed good item characteristics with weighted mean corrected item-scale correlations of rit = 0.44 to rit = 0.74. Ceiling effects increased with time: 1 patient gave the highest possible rating of 130 points at T0 (2%), 3 patients at T3 (7%) and T6 (9%), 6 patients at T9 (23%), 9 patients at T12 (35%) and T18 (33%) and 5 patients at T15 (22%).
Reliability
Internal consistency and retest-reliability values of the ASKp for different time points and time lags are shown in Table 2. The internal consistency was above average at all time points with Cronbach’s alpha ranging from α = 0.91 to α = 0.97. Moreover, the intraclass correlation coefficient was good (ICC = 0.90) and even better when excluding T9 results (ICC = 0.96). Furthermore, we compared re-test reliability for every single time point and every single time lag. Associations were low for T0 and T9 with all other time points, except for T9 with T12. For all other time points and time lags re-test reliability was good ranging from r = 0.74 to r = 0.93. The deviation in T9 was caused by one single patient, who had a very low ASKp score at this time point (mean = 0.17) compared to the other time points (average mean = 3.11). Of note, Cronbach’s α was assessed for patients who answered all questions only. For 17 patients at least 1 question was reported as not relevant to them and we excluded them from the reliability analysis.
Validity: convergent and discriminant validity measure
Convergent validity was good, with a moderate correlation between the ASKp and the KPS/PSS score (r = 0.599; p < 0.001) (Table 3).
We analyzed the discriminability of the ASKp in patients who needed devices versus patients without devices. In a discriminant analysis ASKp correctly classified 90% of the patients. Of the group that needed devices 50% (n = 5/10) were correctly classified, whereas of the group that needed no devices 98% (n = 44/45) were correctly classified. Fig. 2a shows the corresponding receiver operating curve containing all possible pairs of true and false positive rates for the ASKp.

Receiver operating characteristics (ROC) curve when using ASKp scores to predict patients that need devices and patients with cGVHD. a Need of devices: ROC curve when using ASKp scores to predict patients thatneed devices; b cGVHD: ROC curve when using ASKp scores to predict patients with cGVHD
Finally, we analyzed discriminability in patients with cGVHD versus patients without cGVHD (No-cGVHD). The ASKp correctly classified 71% of patients, while 97% (n = 35/36) of the No-cGVHD patients were correctly assigned to their group, only 21% (n = 4/19) of patients with cGVHD where correctly classified (Fig. 2b).
Ability to detect change over time
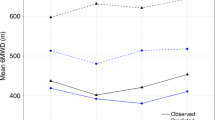
To make the patient-reported ASKp and the clinician-reported KPS/PSS comparable we standardized the measurements by their average mean at every time point by the sample mean and standard deviation at this time point (MASK and MKPS/PSS). Fig. 3 demonstrates the development of the ASKp with and without the outlier in T9 and the KPS/PSS scores. The outlier in T9 did not affect the KPS/PSS (KPS/PSSwith outlier at T9 = 8.85, KPS/PSSwithout outlier at T9 =8.84). Therefore, we did not include a separate calculation of the KPS/PSS scores without the outlier in T9. ASKp values increased more than a half standard deviation from T0 to T12 and the KPS/PSS scores increased nearly a half standard deviation between T0 and T3.

Standardized means of ASKp and KPS/PSS across time points. ASKp = MASK = solid line, MASK without outlier in T9 = dashed line, KPS/PSS = MKPS/PSS = dotted line
Accordingly, Wilcoxon sign rank test results were significant between T0 and T3 (n = 37, p = 0.001) and between T3 and T6 (n = 24, p = 0.004) for the ASKp and between T0 and T3 (n = 43, p < 0.001) for the KPS/PSS.
Furthermore, when we computed the standardized mean values across all time points (SMASK) we found that the ASKp and standardized ASKp values were highly associated (r = 0.981; p < 0.001), even though the ASKp scores increased with time. This indicates that there are no systematic differences the groups of patients assessed at different time points. Results for both were nearly the same in all statistical analyses. Therefore, the focus will be on the further analysis of unstandardized ASKp scores.
Detailed comparison of the patient-reported ASKp and the clinician-reported KPS/PSS
Table 3 presents ASKp and KPS/PSS scores in correlation with patients’ clinical parameters. Comparable associations for both the ASKp and the KPS/PSS were found regarding: a) no correlation with age or gender; b) a low significant correlation with patients with endocrine and GI comorbidities and c) highly significant lower scores for patients who were in the need of devices (ASKp: F = 22.298; p < 0.001 and KPS/PSS: F = 20.132; p < 0.001) and patients who suffered from steroid side effects (ASKp: F = 17.229; p < 0.001 and KPS/PSS: F = 15,063; p < 0.001). Significantly lower scores for the ASKp were found in patients after adoptive cell therapy (F = 11.837; p < 0.001) and in patients with overlap cGVHD (F = 8.198; p < 0.01) with less significant correlations in the KPS/PSS.
Similar to the discriminability analysis we found no differences between the subgroups No-cGVHD, moderate- and severe cGVHD in ASKp (F = 2.014; p = 0.077), whereas, differences in the KPS/PSS were highly significant (F = 9.721; p < 0.001). When analyzing scores of moderate and severe cGVHD patients as one group the ASKp scores showed a slightly significant correlation with cGVHD but again, a highly significant correlation in the KPS/PSS (ASKp: F = 4.050; p = 0.049 and KPS/PSS F = 20.082; p < 0.001). Moreover, only KPS/PSS scores correlated with joint and fascia manifestations of cGVHD (F = 18.246; p < 0.001).
Multiple regression analyses with possible predictors of ASKp
To further evaluate the associations of clinical data with ASKp scores, we used multiple regression analyses as shown in Table 4. Considering the sample size (n = 55) we did not include more than five moderators at the same time into a single analysis. First, we controlled the multiple regression models for age and amount of needed help in answering the questionnaire (M1–M3). Age was not a significant predictor of ASKp. Therefore, we did not included age in further analyses. On the other side the amount of help needed in answering the questions was significantly associated with ASKp in all models no matter which moderators were included.
Interestingly, patients with moderate and severe cGVHD had lower ASKp scores compared to patients with no and mild cGVHD when the regression was controlled for amount of help needed and age (M2; β = −0.604; p < 0.001) as well as when overlap cGVHD was additionally included (M3; β = −0.604; p < 0.001), but not when overlap cGVHD, steroid side effects and cGVHD-associated symptoms were additionally included (see M4; β = 0.092; p = 0.505). Overlap cGVHD was negatively associated with ASKp in all models in which it was included (M3–M5). The KPS/PSS showed the highest association with ASKp (M5, β = 0.501; p < 0.001) besides the amount of help needed answering the questions. Both steroid side effects and cGVHD-associated symptoms were also significantly associated with ASKp score (M5, β = −0.239; p = 0.011; β = −0.367; p = 0.011).
Associations with severity of cGVHD on a 10-point scale
Finally, we used three regression models to compare the prediction value of the ASKp and the KSP/PSS scores for cGVHD severity on a 10-point scale. Firstly, in separated simple regressions both predictors were significant. Overall, the KPS/PSS, with R2 = 0.346 (p <0.001), could explain more variance than the ASKp with R2 = 0.148 (p = 0.004). Secondly, when ASKp and KPS/PSS were included simultaneously in the model they explained less variance together R2 = 0.325 (p < 0.001), than the KPS/PSS alone R2 = 0.346 (p < 0.001). Furthermore, the ASKp failed to explain a significant amount of variance (β = 0.053; p = 0.709) whereas the KPS/PSS remained a significant predictor of cGVHD severity (β = −0.554; p <0.001).
Discussion
Overall, the German version of the ASKp showed good psychometric properties except for ceiling effects both for less affected patients and over time. Even at study time point T9 23% scored the maximum amount of points in the ASKp and at time point T18 33% of patients scored the maximum. As stated by Klepper et al. [19] these ceiling effects may limit the usefulness for longitudinal and comparative studies including healthy control groups. Our results show that this also may apply for post-HSCT patients.
Criterion and convergent validity as well as reliability were good. One item (“I took care of my medical needs”) did not fit the scale. We assume that this is caused by the specific sample than by a translation error. Medical needs of HSCT survivors may be too complex and may vary too much between patients to fit in a physical function scale. Moreover, instruments based on self-reports are vulnerable to confounders like social desirability, cognitive development and learning effects, and other environmental and temporal influences [27]. For example, the amount of help needed answering questions was highly negatively associated with the ASKp score. Parents may compare current functioning to prior function and Hedeker et al. reported that parents rated their children’s QOL lower than the children did [2].
When we compared the patient-reported ASKp with the clinician-reported KPS/PSS regarding the association with comorbidities and steroid side effects the results were quite similar. But importantly, we did not observe a significant correlation of the ASKp with most details of cGVHD: both for severity (global severity and cGVHD severity on a 10-point scale) and joint involvement of cGVHD KPS/PSS we found a higher significant correlation with the KPS/PSS. In this regard, it seems worth considering the patient-reported KPS/PSS as an instrument to capture functional status, similar to a recent publication by Lee et al. [25].
Only differences between patients with and without overlap cGVHD were higher in ASKp than in the KPS/PSS. Specific confounders may appear in HSCT patients, which often are unable to participate in age-appropriate activities with peers. One reason for our findings could be that adolescents and children may be less aware of the implications if the clinical status is not associated with major altered functions [2].
In contrast to the HAP for adults [16] and although the ASKp was developed to assess physical disability in children with musculoskeletal impairments, our study results do not support the ASKp being appropriate to measure the impact of cGVHD severity on physical functioning so far. Consistent with the finding of another study by Christakou et al. [28] we observed that the lack of a pain scale within the ASKp is worth mentioning as many cGVHD patients especially with joint and fascia involvement and/or steroid side effects have pain along with their symptoms of cGVHD. We have previously published results from a prospective study on health-related quality of life after pediatric HSCT that most problems were detected within the domains of physical functioning and pain [12].
Of note, we observed that steroid side effects were negatively associated with the ASKp in line with findings of others that the use of steroids impact on QOL and activity scores [14].
The main limitation of this study is related to the fact that we could not conduct a linear mixed model or other more complex statistical analysis because of missing data, small sample size and, in part, non-normality of the data. Therefore, the study lacks power. The probability that even moderate effect sizes did not reach significance is rather high; however, it has been shown by other authors that the downfall of studies using patient-reported outcome measures is missing data and small sample sizes [29, 30]. Furthermore, we made multiple comparisons, which increases the possibility of random significances. Another important lesson we have learned is that the implementation of a study adjudication committee would improve the accuracy of NIH-defined cGVHD diagnosis as outlined by the study of Cuvelier et al. [30].
Apart from previously addressed problems, the recall period and the length of the self-report measure should also be considered: it may be important to use shorter recall periods with adolescents and children than with adults because this patient group may have more difficulties remembering health-related events over extended periods of time. Also, the length of the questionnaires requires careful consideration because of the wide variation in children’s ability to maintain attention to tasks. Therefore, other specific measures of physical functioning could be investigated, too. For example, we have shown in a prospective pilot study aiming to evaluate health-related QOL with the PedsQL™ and a newly developed PedsQL HSCT module to capture transplant and, specifically, cGVHD-related problems that the summary scores of the generic PedsQL and the PedsQL HSCT module showed high correlations (r = 0.89 in patients’ and r = 0.81 in parents’ assessments). Moreover, both tools discriminated between patients with and without cGVHD. The PedsQL HSCT-module was practical to use and suitable across a broad age range (2–18 years) both in patients with and without cGVHD [12]; however, it is still a pilot instrument and needs further development also regarding physical functioning and testing in a larger patient population.
Conclusion
The ASKP patient self-report demonstrated good psychometric properties for severely impaired patients with ceiling effects in others and during the course of the study. Therefore, patients’ further progress and smaller differences may not have been detected. Moreover, the ASKp showed no significant differences for NIH-defined cGVHD severity both in global severity and on a 10-point cGVHD severity scale. In conclusion, our study was not able to prove advantages of the ASKp when compared to the KPS/PSS even though economical and patients’ effort was higher. Further prospective studies could focus on the usage of patient-reported and clinician-reported KPS/PSS in addition to physical domains of QOL instruments. Accordingly, application range of ASKp in adolescent and pediatric HSCT patients seems limited especially given the need for pediatric tools for measurement of physical functioning as an endpoint in randomized clinical trials.
Change history
01 July 2021
A Correction to this paper has been published: https://doi.org/10.1007/s00508-021-01902-2
References
Duell T, et al. Health and functional status of long-term survivors of bone marrow transplantation. EBMT Working Party on Late Effects and EULEP Study Group on Late Effects. European Group for Blood and Marrow Transplantation. Ann Intern Med. 1997;126(3):184–92.
Parsons SK, Phipps S, Sung L, Baker KS, Pulsipher MA, Ness KK. NCI, NHLBI/PBMTC first international conference on late effects after pediatric hematopoietic cell transplantation: health-related quality of life, functional, and neurocognitive outcomes. Biol Blood Marrow Transplant. 2012;18(2):162–71.
Lawitschka A, Peters C. Long-term effects of myeloablative allogeneic hematopoietic stem cell transplantation in pediatric patients with acute Lymphoblastic leukemia. Curr Oncol Rep. 2018;20(9):74.
Fraser CJ, et al. Impact of chronic graft-versus-host disease on the health status of hematopoietic cell transplantation survivors: a report from the Bone Marrow Transplant Survivor Study. Blood. 2006;108(8):2867–73.
Sun C‑L, et al. Burden of morbidity in 10+ year survivors of hematopoietic cell transplantation: report from the bone marrow transplantation survivor study. Biol Blood Marrow Transplant. 2013;19(7):1073–80.
Filipovich AH, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005;11(12):945–56.
Ferrara JLM, Levine JE, Reddy P, Holler E. Graft-versus-host disease. Lancet. 2009;373(9674):1550–61.
Baird K, Cooke K, Schultz KR. Chronic graft-versus-host disease (GVHD) in children. Pediatr Clin North Am. 2010;57(1):297–322.
Vigorito AC, et al. Evaluation of NIH consensus criteria for classification of late acute and chronic GVHD. Blood. 2009;114(3):702–8.
Mitchell SA, et al. Determinants of functional performance in long-term survivors of allogeneic hematopoietic stem cell transplantation with chronic graft-versus-host disease (cGVHD). Bone Marrow Transplant. 2010;45(4):762–9.
Pidala J, et al. Overlap subtype of chronic graft-versus-host disease is associated with an adverse prognosis, functional impairment, and inferior patient-reported outcomes: a Chronic Graft-versus-Host Disease Consortium study. Haematologica. 2012;97(3):451–8.
Lawitschka A, et al. Health-related quality of life in pediatric patients after allogeneic SCT: development of the PedsQL Stem Cell Transplant module and results of a pilot study. Bone Marrow Transplant. 2014;49(8):1093–7.
Pavletic SZ, et al. Measuring therapeutic response in chronic graft-versus-host disease: National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: IV. Response Criteria Working Group report. Biol Blood Marrow Transplant. 2006;12(3):252–66.
Krupski C, Jagasia M. Quality of life in the chronic GVHD consortium cohort: lessons learned and the long road ahead. Curr Hematol Malig Rep. 2015;10(3):183–91.
Jagasia M, et al. Incidence and outcome of chronic graft-versus-host disease using National Institutes of Health consensus criteria. Biol Blood Marrow Transplant. 2007;13(10):1207–15.
Herzberg PY, et al. Validation of the human activity profile questionnaire in patients after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2010;16(12):1707–17.
Fiuza-Luces C, Simpson RJ, Ramirez M, Lucia A, Berger NA. Physical function and quality of life in patients with chronic GvHD: a summary of preclinical and clinical studies and a call for exercise intervention trials in patients. Bone Marrow Transplant. 2016;51(1):13–26.
Young NL, Yoshida KK, Williams JI, Bombardier C, Wright JG. The role of children in reporting their physical disability. Arch Phys Med Rehabil. 1995;76(10):913–8.
Klepper SE. Measures of pediatric function: Child Health Assessment Questionnaire (C-HAQ), Juvenile Arthritis Functional Assessment Scale (JAFAS), Pediatric Outcomes Data Collection Instrument (PODCI), and Activities Scale for Kids (ASK). Arthritis Care Res. 2011;63(1):S371–82.
Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: reliability, validity, and guidelines. J Clin Oncol. 1984;2(3):187–93.
Lansky SB, List MA, Lansky LL, Ritter-Sterr C, Miller DR. The measurement of performance in childhood cancer patients. Cancer. 1987;60(7):1651–6.
Forinder U, Lof C, Winiarski J. Quality of life and health in children following allogeneic SCT. Bone Marrow Transplant. 2005;36(2):171–6.
Inagaki J, et al. Long-term morbidity and mortality in children with chronic graft-versus-host disease classified by national institutes of health consensus criteria after Allogeneic Hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2015;21(11):1973–80.
Cesaro S, et al. Second allogeneic stem cell transplant for aplastic anaemia: a retrospective study by the Severe Aplastic Anaemia Working Party of the European Society for Blood and Marrow Transplantation. Br J Haematol. 2015;171(4):606–14.
Lee SJ, et al. Patient-reported outcomes and health status associated with chronic graft-versus-host disease. Haematologica. 2018;103(9):1535–41.
Vukic T, et al. Joint and fascial chronic graft-vs-host disease: correlations with clinical and laboratory parameters. Croat Med J. 2016;57(3):266–75.
Garcia J, Gustavson A. The science of self-report. APS Obs. 1997;10:35–38.
Christakou A, Laiou A. Comparing the psychometric properties of the pediatric outcomes data collection instrument and the activities scales for kids: a review. J Child Health Care. 2014;18(3):207–14.
Jagasia MH, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. The 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. 2015;21(3):389–401.
Cuvelier GDE, et al. Benefits and challenges with diagnosing chronic and late acute GVHD in children using the NIH consensus criteria. Blood. 2019;134(3):304–16.
Acknowledgements
The authors would like to thank all children and parents who agreed to participate in this study. Furthermore, the authors would like to thank Steven Pavletic from the chronic GVHD study group, National Cancer Institute, NIH.
Funding
This study was supported in parts by the “Jubiläumsfonds der Österreichischen Nationalbank”, Number 13215.
Funding
Open access funding provided by Medical University of Vienna.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Lawitschka, M. Brunmair, D. Bauer, N. Zubarovskaya, R. Felder-Puig, B. Strahm, P. Bader, G. Strauss, M. Albert, I.von Luettichau, H. Greinix, D. Wolff, and C. Peters declare that they have no competing interests.
Ethical standards
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975, as revised in 2008. Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: Due to a breach of copyright.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lawitschka, A., Brunmair, M., Bauer, D. et al. Psychometric properties of the Activities Scale for Kids-performance after allogeneic hematopoietic stem cell transplantation in adolescents and children. Wien Klin Wochenschr 133, 41–51 (2021). https://doi.org/10.1007/s00508-020-01641-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00508-020-01641-w