
Abstract
Background
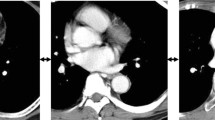
Minimally invasive esophagectomy (MIE) is being increasingly performed worldwide. When performing MIE, we sometimes experienced difficulties due to a narrow upper mediastinum or a middle to lower thoracic esophagus hidden by the projection of the vertebral body. However, there were no reports regarding the influence of anatomical factors on the difficulty of performing MIE. The aim of this study was to evaluate whether anatomical factors could be related to the difficulty of the thoracic procedure in MIE.
Methods
We investigated 87 consecutive patients undergoing MIE for primary esophageal cancer between 2013 and 2015 and created novel indices to assess the upper mediastinal narrowness and vertebral body projection at middle thoracic part on preoperative computed tomography images. We assessed clinicopathological and anatomical factors and determined the factors influencing the thoracic procedural difficulty in MIE. The thoracic procedure duration was selected as the variable representing technical difficulty.
Results
The mean thoracic procedure duration was 280.2 ± 52.5 min. There were no significant correlations between the indices and patient factors such as age, sex, and body mass index. Meanwhile, there was a significant correlation between the upper mediastinal narrowness and the vertebral body projection (p < 0.01). Of the clinicopathological and anatomical factors, blood loss during the thoracic procedure, thoracic duct resection, and vertebral body projection independently were related to the prolonged thoracic procedure duration in multiple linear regression analysis (p = 0.01, 0.03, and <0.01, respectively). The other factors including upper mediastinal narrowness were not statistically significant.
Conclusions
This is the first study to reveal the influence of anatomical factors on the difficulty of the thoracic procedure in MIE. The vertebral body projection at middle thoracic part appears to be a useful tool for predicting the thoracic procedural difficulty in MIE preoperatively.


Similar content being viewed by others


References
Cuschieri A, Shimi S, Banting S (1992) Endoscopic oesophagectomy through a right thoracoscopic approach. J R Coll Surg Edinb 37:7–11
Watanabe M, Baba Y, Nagai Y, Baba H (2013) Minimally invasive esophagectomy for esophageal cancer: an updated review. Surg Today 43:237–244
Takeuchi H, Miyata H, Gotoh M, Kitagawa Y, Baba H, Kimura W et al (2014) A risk model for esophagectomy using data of 5354 patients included in a Japanese nationwide web-based database. Ann Surg 260:259–266
Biere SS, van Berge Henegouwen MI, Maas KW, Bonavina L, Rosman C, Garcia JR et al (2012) Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet 379:1887–1892
Takeuchi H, Kawakubo H, Kitagawa Y (2013) Current status of minimally invasive esophagectomy for patients with esophageal cancer. Gen Thorac Cardiovasc Surg 61:513–521
Kawakubo H, Takeuchi H, Kitagawa Y (2013) Current status and future perspectives on minimally invasive esophagectomy. Korean J Thorac Cardiovasc Surg 46:241–248
Baik SH, Kim NK, Lee KY, Sohn SK, Cho CH, Kim MJ et al (2008) Factors influencing pathologic results after total mesorectal excision for rectal cancer: analysis of consecutive 100 cases. Ann Surg Oncol 15:721–728
Akiyoshi T, Kuroyanagi H, Oya M, Konishi T, Fukuda M, Fujimoto Y et al (2009) Surgery 46:483–489
Kim JY, Kim YW, Kim NK, Hur H, Lee K, Min BS et al (2011) Pelvic anatomy as a factor in laparoscopic rectal surgery: a prospective study. Surg Laparosc Endosc Percutan Tech 21:334–339
Shinozaki K, Ajiki T, Okazaki T, Ueno K, Matsumoto T, Ohtsubo I et al (2013) Gallbladder bed pocket score as a preoperative measure for assessing the difficulty of laparoscopic cholecystectomy. Asian J Endosc Surg 6:285–291
Mamidanna R, Bottle A, Aylin P, Faiz O, Hanna GB (2012) Short-term outcomes following open versus minimally invasive esophagectomy for cancer in England: a population-based national study. Ann Surg 255:197–203
Haga Y, Beppu T, Doi K, Nozawa F, Mugita N, Ikei S et al (1997) Systemic inflammatory response syndrome and organ dysfunction following gastrointestinal surgery. Crit Care Med 25:1994–2000
Okamura A, Takeuchi H, Matsuda S, Ogura M, Miyasho T, Nakamura R et al (2015) Factors affecting cytokine change after esophagectomy for esophageal cancer. Ann Surg Oncol 22:3130–3135
Sato N, Endo S, Kimura Y, Ikeda K, Aoki K, Iwaya T et al (2002) Influence of a human protease inhibitor on surgical stress induced immunosuppression. Dig Surg 19:300–305
Ogawa K, Hirai M, Katsube T, Murayama M, Hamaguchi K, Shimakawa T et al (2000) Suppression of cellular immunity by surgical stress. Surgery 127:329–336
Shakhar G, Ben-Eliyahu S (2003) Potential prophylactic measures against postoperative immunosuppression: could they reduce recurrence rates in oncological patients? Ann Surg Oncol 10:972–992
Hogan BV, Peter MB, Shenoy HG, Horgan K, Hughes TA (2011) Surgery induced immunosuppression. Surgeon 9:38–43
Ogiso S, Yamaguchi T, Hata H, Kuroyanagi H, Sakai Y (2010) Introduction of laparoscopic low anterior resection for rectal cancer early during residency: a single institutional study on short-term outcomes. Surg Endosc 24:2822–2829
Kelly M, Bhangu A, Singh P, Fitzgerald JE, Tekkis PP (2014) Systematic review and meta-analysis of trainee- versus expert surgeon-performed colorectal resection. Br J Surg 101:750–759
Palanivelu C, Prakash A, Senthilkumar R, Senthilnathan P, Parthasarathi R, Rajan PS et al (2006) Minimally invasive esophagectomy: thoracoscopic mobilization of the esophagus and mediastinal lymphadenectomy in prone position–experience of 130 patients. J Am Coll Surg 203(1):7–16
Fabian T, Martin J, Katigbak M, McKelvey AA, Federico JA (2008) Thoracoscopic esophageal mobilization during minimally invasive esophagectomy: a head-to-head comparison of prone versus decubitus positions. Surg Endosc 22:2485–2491
Kaburagi T, Takeuchi H, Kawakubo H, Omori T, Ozawa S, Kitagawa Y (2014) Clinical utility of a novel hybrid position combining the left lateral decubitus and prone positions during thoracoscopic esophagectomy. World J Surg 38:410–418
Higashihara E, Baba S, Nakagawa K, Murai M, Go H, Takeda M et al (1998) Learning curve and conversion to open surgery in cases of laparoscopic adrenalectomy and nephrectomy. J Urol 159:650–653
Ogiso S, Yamaguchi T, Hata H, Fukuda M, Ikai I, Yamato T et al (2011) Evaluation of factors affecting the difficulty of laparoscopic anterior resection for rectal cancer: “narrow pelvis” is not a contraindication. Surg Endosc 25:1907–1912
Doyle GJ, Simpson W (1994) Technical report: prone scanning in the CT assessment of oesophageal carcinoma. Clin Radiol 49:209–210
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Akihiko Okamura, Masayuki Watanabe, Shinji Mine, Koujiro Nishida, Yu Imamura, Takanori Kurogochi, Yuko Kitagawa, and Takeshi Sano have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Okamura, A., Watanabe, M., Mine, S. et al. Factors influencing difficulty of the thoracic procedure in minimally invasive esophagectomy. Surg Endosc 30, 4279–4285 (2016). https://doi.org/10.1007/s00464-015-4743-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4743-3