
Abstract
Background
Self-expanding metal stents (SEMS) are an established treatment for palliation of malignant colorectal strictures and as a bridge to surgery for acute malignant colonic obstruction. Patients with benign colonic strictures may benefit from stent placement, but little data exist for this indication.
Methods
All cases of colonic stent placement identified from a prospectively collected gastrointestinal database from April 1999 to August 2006 were reviewed. During the study period, 23 patients with benign obstructive disease underwent endoscopic SEMS placement. The etiologies of the stricture were diverticular/inflammatory (n = 16), postsurgical anastomotic (n = 3), radiation-induced (n = 3), and Crohn’s (n = 1) disease. All strictures were located in the left colon. Five patients had an associated colonic fistula. Uncovered Enteral Wallstents or Ultraflex Precision Colonic stents (Boston Scientific) were endoscopically placed in all but one patient.
Results
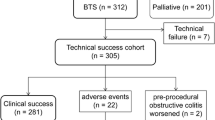
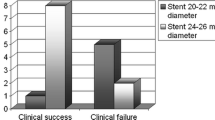
Stent placement was technically successful for all 23 patients, and obstruction was relieved for 22 patients (95%). Major complications occurred in 38% of the patients including migration (n = 2), reobstruction (n = 4), and perforation (n = 2). Of these major complications, 87% occurred after 7 days. Four patients did not undergo an operation. Of the 19 patients who underwent planned surgical resection, 16 were successfully decompressed and converted from an emergent operation to an elective one with a median time to surgical resection of 12 days (range, 2 days to 18 months). Surgery was delayed more than 30 days after stent placement for six of these patients. Of the 19 patients who underwent a colectomy, 8 (42%) did not need a stoma after stent insertion.
Conclusions
SEMS can effectively decompress high-grade, benign colonic obstruction, thereby allowing elective surgery. The use of SEMS can offer medium-term symptom relief for benign colorectal strictures, but this approach is associated with a high rate of delayed complications. Thus, if elective surgery is planned, data from this small study suggest that it should be performed within 7 days of stent placement.


Similar content being viewed by others
References
Baron TH, Rey JF, Spinelli P (2002) Expandable metal stent placement for malignant colorectal obstruction. Endoscopy 34:823–830
Baron TH, Dean PA, Yates MR 3rd, Canon C, Koehler RE (1998) Expandable metal stents for the treatment of colonic obstruction: techniques and outcomes. Gastrointest Endosc 47:7–286
Meisner S, Hensler M, Knop FK, West F, Wille-Jorgensen P (2004) Self-expanding metal stents for colonic obstruction: experiences from 104 procedures in a single center. Dis Colon Rectum 47:444–450
Suzuki N, Saunders BP, Thomas-Gibson S, Akle C, Marshall M, Halligan S (2004) Colorectal stenting for malignant and benign disease: outcomes in colorectal stenting. Dis Colon Rectum 47:1201–1207
Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M (2004) Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol 99:2051–2057
Baron TH (2005) Colonic stenting: technique, technology, and outcomes for malignant and benign disease. Gastrointest Endosc Clin North Am 15:757–771
Baron TH (2003) Colorectal stents. Tech Gastrointest Endosc 5:182–190
Deans GT, Krukowski ZH, Irwin ST (1994) Malignant obstruction of the left colon. Br J Surg 81:10–16
Tang E, Davis J, Silberman H (1995) Bowel obstruction in cancer patients. Arch Surg 130:832–836
Bhardwaj R, Parker MC (2003) Palliative therapy of colorectal carcinoma: stent or surgery? Colorectal Dis 5:518–521
Paul L, Pinto I, Gomez H, Fernandez-Lobato R, Moyano E (2002) Metallic stents in the treatment of benign diseases of the colon: preliminary experience in 10 cases. Radiology 223:715–722
Law WL, Choi HK, Chu KW, Tung HM (2002) Radiation stricture of rectosigmoid treated with self-expanding metallic stent. Surg Endosc 16:1106–1107
Dormann AJ, Deppe H, Wigginghaus B (2001) Self-expanding metallic stents for continuous dilatation of benign stenoses in gastrointestinal tract: first results of long-term follow-up in interim stent application in pyloric and colonic obstructions. Z Gastroenterol 39:957–960
King DW, Lubowski DZ, Armstrong AS (1990) Sigmoid stricture at colonoscopy: an indication for surgery. Int J Colorectal Dis 5:161–163
Rutgeerts P, Geboes K, Vantrappen G, Kerremans R, Coenegrachts JL, Coremans G (1984) Natural history of recurrent Crohn’s disease at the ileocolonic anastomosis after curative surgery. Gut 25:665–672
Schlegel RD, Dehni N, Parc R, Caplin S, Tiret E (2001) Results of reoperations in colorectal anastomotic strictures. Dis Colon Rectum 44:1464–1468
Constantinides VA, Tekkis PP, Athanasiou T, Aziz O, Purkayastha S, Remzi FH, Fazio VW, Aydin N, Darzi A, Senapati A (2006) Primary resection with anastomosis vs Hartmann’s procedure in nonelective surgery for acute colonic diverticulitis: a systematic review. Dis Colon Rectum 49:966–981
Harris GJ, Senagore AJ, Lavery IC, Fazio VW (2001) The management of neoplastic colorectal obstruction with colonic endolumenal stenting devices. Am J Surg 181:499–506
Baxter NN, Novotny PJ, Jacobson T, Maidl LJ, Sloan J, Young-Fadok TM (2006) A stoma quality of life scale. Dis Colon Rectum 49:205–212
Nugent KP, Daniels P, Stewart B, Patankar R, Johnson CD (1999) Quality of life in stoma patients. Dis Colon Rectum 42:1569–1574
Park JJ, Del Pino A, Orsay CP, Nelson RL, Pearl RK, Cintron JR, Abcarian H (1999) Stoma complications: the Cook County Hospital experience. Dis Colon Rectum 42:1575–1580
Carne PW, Frye JN, Robertson GM, Frizelle FA (2004) Stents or open operation for palliation of colorectal cancer: a retrospective, cohort study of perioperative outcome and long-term survival. Dis Colon Rectum 47:1455–1461
Goyal A, Schein M (2001) Current practices in left-sided colonic emergencies: a survey of U.S. gastrointestinal surgeons. Dig Surg 18:399–402
Ng KC, Law WL, Lee YM, Choi HK, Seto CL, Ho JW (2006) Self-expanding metallic stent as a bridge to surgery versus emergency resection for obstructing left-sided colorectal cancer: a case-matched study. J Gastrointest Surg 10:798–803
Martinez-Santos C, Lobato RF, Fradejas JM, Pinto I, Ortega-Deballon P, Moreno-Azcoita M (2002) Self-expandable stent before elective surgery vs emergency surgery for the treatment of malignant colorectal obstructions: comparison of primary anastomosis and morbidity rates. Dis Colon Rectum 45:401–406
Law WL, Choi HK, Chu KW (2003) Comparison of stenting with emergency surgery as palliative treatment for obstructing primary left-sided colorectal cancer. Br J Surg 90:1429–1433
Binkert CA, Ledermann H, Jost R, Saurenmann P, Decurtins M, Zollikofer CL (1998) Acute colonic obstruction: clinical aspects and cost effectiveness of preoperative and palliative treatment with self-expanding metallic stents: a preliminary report. Radiology 206:199–204
Adler DG, Baron TH (2002) Endoscopic palliation of colorectal cancer. Hematol Oncol Clin North Am 16:1015–1029
Yates MR III, Baron TH (1999) Treatment of a radiation-induced sigmoid stricture with an expandable metal stent. Gastrointest Endosc 50:422–426
Author information
Authors and Affiliations
Corresponding author
Additional information
Podium presentation at the annual meeting of the Society of American Gastrointestinal and Esophageal Surgeons (SAGES), 18–22 April 2007 at Las Vegas, NV, USA
Rights and permissions
About this article
Cite this article
Small, A.J., Young-Fadok, T.M. & Baron, T.H. Expandable metal stent placement for benign colorectal obstruction: outcomes for 23 cases. Surg Endosc 22, 454–462 (2008). https://doi.org/10.1007/s00464-007-9453-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-007-9453-z