
Abstract
Background
Laparoscopic Nissen fundoplication (LNF) is the preferred operation for the control of gastroesophageal reflux disease (GERD). The use of a full fundoplication for patients with esophageal dysmotility is controversial. Although LNF is known to be superior to a partial wrap for patients with weak peristalsis, its efficacy for patients with severe dysmotility is unknown. We hypothesized that LNF is also acceptable for patients with severe esophageal dysmotility.
Methods
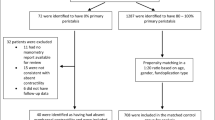
A multicenter retrospective review of consecutive patients with severe esophageal dysmotility who underwent an LNF was performed. Severe dysmotility was defined by manometry showing an esophageal amplitude of 30 mmHg or less and/or 70% or more nonperistaltic esophageal body contractions.
Results
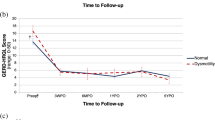
In this study, 48 patients with severe esophageal dysmotility underwent LNF. All the patients presented with symptoms of GERD, and 19 (39%) had preoperative dysphagia. A total of 10 patients had impaired esophageal body contractions, whereas 32 patients had an abnormal esophageal amplitude, and 6 patients had both. The average abnormal esophageal amplitude was 24.9 ± 5.2 mmHg (range, 6.0–30 mmHg). The mean percentage of nonperistaltic esophageal body contractions was 79.4% ± 8.3% (range, 70–100%). There were no intraoperative complications and no conversions. Postoperatively, early dysphagia occurred in 35 patients (73%). Five patients were treated with esophageal dilation, which was successful in three cases. One patient required a reoperative fundoplication. Overall, persistent dysphagia was found in two patients (4.2%), including one patient with severe preoperative dysphagia, which improved postoperatively. Abnormal peristalsis and/or distal amplitude improved postoperatively in 12 (80%) of retested patients. There were no cases of Barrett’s progression to dysplasia or carcinoma. During an average follow-up period of 25.4 months (range, 1–46 months), eight patients (16%) were receiving antireflux medications, with six of these showing normal esophageal pH study results.
Conclusion
The LNF procedure provides low rates of reflux recurrence with little long-term postoperative dysphagia experienced by patients with severely disordered esophageal peristalsis. Effective fundoplication improved esophageal motility for most of the patients. A 360° fundoplication should not be contraindicated for patients with severe esophageal dysmotility.

Similar content being viewed by others

References
Laparoscopic antireflux surgery for gastroesophageal reflux disease (GERD) (1997) Results of a Consensus Development Conference. Held at the Fourth International Congress of the European Association for Endoscopic Surgery (E.A.E.S.), Trondheim, Norway, 21–24 June 1996. Surg Endosc 11: 413–426
Anvari M, Allen C (2003) Five-year comprehensive outcomes evaluation in 181 patients after laparoscopic Nissen fundoplication. J Am Coll Surg 196: 51–57; discussion 57–58, author reply 58–59
Baigrie RJ, Watson DI, Myers JC, Jamieson GG (1997) Outcome of laparoscopic Nissen fundoplication in patients with disordered preoperative peristalsis. Gut 40: 381–385
Beckingham IJ, Cariem AK, Bornman PC, Callanan MD, Louw JA (1998) Oesophageal dysmotility is not associated with poor outcome after laparoscopic Nissen fundoplication. Br J Surg 85: 1290–1293
Bell RC, Hanna P, Mills MR, Bowrey D (1999) Patterns of success and failure with laparoscopic Toupet fundoplication. Surg Endosc 13: 1189–1194
Biertho L, Sebajang H, Anvari M (2006) Effects of laparoscopic Nissen fundoplication on esophageal motility: long-term results. Surg Endosc 20: 619–623
Catarci M, Gentileschi P, Papi C, Carrara A, Marrese R, Gaspari AL, Grassi GB (2004) Evidence-based appraisal of antireflux fundoplication. Ann Surg 239: 325–337
DeMeester TR, Stein HJ (1992) Minimizing the side effects of antireflux surgery. World J Surg 16: 335–336
Diaz de Liano A, Oteiza F, Ciga MA, Aizcorbe M, Trujillo R, Cobo F (2003) Nonobstructive dysphagia and recovery of motor disorder after antireflux surgery. Am J Surg 185: 103–107
Farrell TM, Archer SB, Galloway KD, Branum GD, Smith CD, Hunter JG (2000) Heartburn is more likely to recur after Toupet fundoplication than Nissen fundoplication. Am Surg 66: 229–236; discussion 236–237
Fibbe C, Layer P, Keller J, Strate U, Emmermann A, Zornig C (2001) Esophageal motility in reflux disease before and after fundoplication: a prospective, randomized, clinical, and manometric study. Gastroenterology 121: 5–14
Granderath FA, Kamolz T, Schweiger UM, Pasiut M, Haas CF, Wykypiel H, Pointner R (2002) Long-term results of laparoscopic antireflux surgery. Surg Endosc 16: 753–757
Horvath KD, Jobe BA, Herron DM, Swanstrom LL (1999) Laparoscopic Toupet fundoplication is an inadequate procedure for patients with severe reflux disease. J Gastrointest Surg 3: 583–591
Hunter JG, Trus TL, Branum GD, Waring JP, Wood WC (1996) A physiologic approach to laparoscopic fundoplication for gastroesophageal reflux disease. Ann Surg 223: 673–685; discussion 685–687
Jobe BA, Wallace J, Hansen PD, Swanstrom LL (1997) Evaluation of laparoscopic Toupet fundoplication as a primary repair for all patients with medically resistant gastroesophageal reflux. Surg Endosc 11: 1080–1083
Kahrilas PJ, Dodds WJ, Hogan WJ, Kern M, Arndorfer RC, Reece A (1986) Esophageal peristaltic dysfunction in peptic esophagitis. Gastroenterology 91: 897–904
Kamolz T, Granderath PA, Bammer T, Pasiut M, Wykypiel H Jr, Herrmann R, Pointner R (2002) Mid- and long-term quality of life assessments after laparoscopic fundoplication and refundoplication: a single unit review of more than 500 antireflux procedures. Dig Liver Dis 34: 470–476
Katz D, Rothstein R, Schned A, Dunn J, Seaver K, Antonioli D (1998) The development of dysplasia and adenocarcinoma during endoscopic surveillance of Barrett’s esophagus. Am J Gastroenterol 93: 536–541
Kauer WK, Peters JH, DeMeester TR, Heimbucher J, Ireland AP, Bremner CG (1995) A tailored approach to antireflux surgery. J Thorac Cardiovasc Surg 110: 141–146; discussion 146–147
Lafullarde T, Watson DI, Jamieson GG, Myers JC, Game PA, Devitt PG (2001) Laparoscopic Nissen fundoplication: five-year results and beyond. Arch Surg 136: 180–184
Liu JY, Woloshin S, Laycock WS, Schwartz LM (2002) Late outcomes after laparoscopic surgery for gastroesophageal reflux. Arch Surg 137: 397–401
Locke GR III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ III (1997) Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology 112: 1448–1456
Mahon D, Rhodes M, Decadt B, Hindmarsh A, Lowndes R, Beckingham I, Koo B, Newcombe RG (2005) Randomized clinical trial of laparoscopic Nissen fundoplication compared with proton pump inhibitors for treatment of chronic gastro-oesophageal reflux. Br J Surg 92: 695–699
Munitiz V, Ortiz A, Martinez de Haro LF, Molina J, Parrilla P (2004) Ineffective oesophageal motility does not affect the clinical outcome of open Nissen fundoplication. Br J Surg 91: 1010–1014
Novitsky YW, Kercher KW, Callery MP, Czerniach DR, Kelly JJ, Litwin DE (2002) Is the use of a bougie necessary for laparoscopic Nissen fundoplication? Arch Surg 137: 402–406
Oberg S, Wenner J, Johansson J, Walther B, Willen R (2005) Barrett esophagus: risk factors for progression to dysplasia and adenocarcinoma. Ann Surg 242: 49–54
Oelschlager BK, Barreca M, Chang L, Oleynikov D, Pellegrini CA (2003) Clinical and pathologic response of Barrett’s esophagus to laparoscopic antireflux surgery. Ann Surg 238: 458–464; discussion 464–466
Oleynikov D, Eubanks TR, Oelschlager BK, Pellegrini CA (2002) Total fundoplication is the operation of choice for patients with gastroesophageal reflux and defective peristalsis. Surg Endosc 16: 909–913
Patti MG, De Pinto M, de Bellis M, Arcerito M, Tong J, Wang A, Mulvihill SJ, Way LW (1997) Comparison of laparoscopic total and partial fundoplication for gastroesophageal reflux. J Gastrointest Surg 1: 309–315
Patti MG, Robinson T, Galvani C, Gorodner MV, Fisichella PM, Way LW (2004) Total fundoplication is superior to partial fundoplication even when esophageal peristalsis is weak. J Am Coll Surg 198: 863–869; discussion 869–870
Rattner DW (2000) Measuring improved quality of life after laparoscopic Nissen fundoplication. Surgery 127: 258–263
Ritter DW, Vanderpool D, Westmoreland M (1997) Laparoscopic Nissen fundoplication for gastroesophageal reflux disease. Am J Surg 174: 715–717; discussion 717–718
Shay S, Tutuian R, Sifrim D, Vela M, Wise J, Balaji N, Zhang X, Adhami T, Murray J, Peters J, Castell D (2004) Twenty-four hour ambulatory simultaneous impedance and pH monitoring: a multicenter report of normal values from 60 healthy volunteers. Am J Gastroenterol 99: 1037–1043
Stein HJ, Bremner RM, Jamieson J, DeMeester TR (1992) Effect of Nissen fundoplication on esophageal motor function. Arch Surg 127: 788–791
Terry M, Smith CD, Branum GD, Galloway K, Waring JP, Hunter JG (2001) Outcomes of laparoscopic fundoplication for gastroesophageal reflux disease and paraesophageal hernia. Surg Endosc 15: 691–699
Trus TL, Laycock WS, Waring JP, Branum GD, Hunter JG (1999) Improvement in quality-of-life measures after laparoscopic antireflux surgery. Ann Surg 229: 331–336
Tutuian R, Vela MF, Balaji NS, Wise JL, Murray JA, Peters JH, Shay SS, Castell DO (2003) Esophageal function testing with combined multichannel intraluminal impedance and manometry: multicenter study in healthy volunteers. Clin Gastroenterol Hepatol 1: 174–182
Tutuian R, Vela MF, Shay SS, Castell DO (2003) Multichannel intraluminal impedance in esophageal function testing and gastroesophageal reflux monitoring. J Clin Gastroenterol 37: 206–215
Valle C, Broglia F, Pistorio A, Tinelli C, Perego M (1999) Prevalence and impact of symptoms suggestive of gastroesophageal reflux disease. Dig Dis Sci 44: 1848–1852
Wetscher GJ, Glaser K, Wieschemeyer T, Gadenstaetter M, Prommegger R, Profanter C (1997) Tailored antireflux surgery for gastroesophageal reflux disease: effectiveness and risk of postoperative dysphagia. World J Surg 21: 605–610
Zornig C, Strate U, Fibbe C, Emmermann A, Layer P (2002) Nissen vs Toupet laparoscopic fundoplication. Surg Endosc 16: 758–766
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Novitsky, Y.W., Wong, J., Kercher, K.W. et al. Severely disordered esophageal peristalsis is not a contraindication to laparoscopic Nissen fundoplication. Surg Endosc 21, 950–954 (2007). https://doi.org/10.1007/s00464-006-9126-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-006-9126-3