
Abstract
Training volume in swimming is usually very high when compared to the relatively short competition time. High-intensity interval training (HIIT) has been demonstrated to improve performance in a relatively short training period. The main purpose of the present study was to examine the effects of a 5-week HIIT versus high-volume training (HVT) in 9–11-year-old swimmers on competition performance, 100 and 2,000 m time (T 100 m and T 2,000 m), VO2peak and rate of maximal lactate accumulation (Lacmax). In a 5-week crossover study, 26 competitive swimmers with a mean (SD) age of 11.5 ± 1.4 years performed a training period of HIIT and HVT. Competition (P < 0.01; effect size = 0.48) and T 2,000 m (P = 0.04; effect size = 0.21) performance increased following HIIT. No changes were found in T 100 m (P = 0.20). Lacmax increased following HIIT (P < 0.01; effect size = 0.43) and decreased after HVT (P < 0.01; effect size = 0.51). VO2peak increased following both interventions (P < 0.05; effect sizes = 0.46–0.57). The increases in competition performance, T 2,000 m, Lacmax and VO2peak following HIIT were achieved in significantly less training time (~2 h/week).
Similar content being viewed by others

Introduction
The racing distance in young swimmers aged 9–11 years usually ranges from 50 to 400 m, with an equivalent racing time of approximately 30 s to 7 min depending on the age and performance level. In contrast to this relatively short racing time, the training volume in this age group, inside and outside the pool, averages approximately 10–15 training hours per week depending on the individual performance level (Sharp 2000). Consequently, a great portion of the weekly training volume is usually performed at lower intensities with higher volumes (Maglischo 2003; Mujika 1998; Sharp 2000).
A recent study in post-pubescent swimmers at the age of 16.6 ± 1.4 years examined the effects of 4 weeks of high-intensity interval training (HIIT) versus high-volume endurance training (HVT) on 100 and 400 m times and demonstrated that, for a period of 4 weeks, high training volumes have no advantage compared to high-intensity training of lower volume (Faude et al. 2008). Costill et al. (1988) analyzed the effect of doubling the volume of training from 4,266 to 8,970 m per day with constant intensity for ten consecutive days in collegiate swimmers (19.1 ± 0.3 years). Maximum and sub-maximum blood lactate concentrations and heart rates decreased after the HVT period, whereas sprint performance did not change. Similar results were described in collegiate male swimmers (19.4 ± 0.4 years) when comparing two groups exercising with significantly different training volumes (5,000 vs. 9,300 m per day for 6 weeks), leading to the conclusion that a considerable increase in training amount does not lead to further performance enhancements, particularly over short distances (Costill et al. 1991). In children’s swimming (aged 9–11 years) little is known about the effects of HIIT on performance.
The preparation period in children’s swimming is often limited to school scheduling and other free-time activities, depending on the performance level. For this reason, effective time-saving training programs such as HIIT could improve endurance performance, resulting in enough time for the enhancement of other limiting skills such as stroke technique, starts and turns as well as sprinting and strength. So, in order to meet the energetic demands of children’s competitive swimming, particularly in 50–400 m events, as well as to develop performance-limiting skills, a lower overall training volume with an emphasis on high-intensity training (HIT) seems to be a rational consequence.
Therefore, the present study aimed at comparing a high-volume, low-intensity (HVT) to a low-volume, high-intensity interval training program (HIIT) with regards to physiological adaptations in competitive male and female youth swimmers. It was hypothesized that HIIT leads to significantly larger effects on physiological parameters and competition performance, whereas HVT does not.
Methods
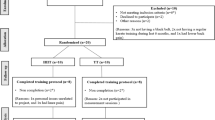
A crossover study design was administered, with each participant receiving a 2 × 5-week HIIT and a HVT intervention in randomly assigned order. Therefore, the participants were divided into group A (starting with HIIT) and group B (starting with HVT). An inactivity period was allocated before (2.5-week Easter break) and between (6 weeks summer break) the two training blocks (Fig. 1). Prior to both intervention periods, a 2-week pre-conditioning phase with equal amount of intensity and volume took place. Exercise testing of each athlete was performed at baseline in weeks 6, 14 and 20. The crossover design was chosen to allow a more precise comparison of treatments with a smaller number of subjects while maintaining appropriate statistical power.

Study design: pre- and post-diagnostics with test procedures and the intervention phase of 2 × 5 weeks of high-intensity interval training (HIIT) and high-volume training (HVT). Group A started with HIIT and group B with HVT
Prior to the study, the participants were not aware of which intervention they would undergo. It was not possible to blind the primary investigator to the athlete. The children and or the parents were asked to immediately report any adverse physical or mental reactions to either training program to the coaches and/or the principal investigator. As an additional safety precaution, subjects were asked to complete a computer-based psychological questionnaire before each single intervention. This allowed the study investigators to identify and address any significant responses to either intervention as soon as possible. Protocol adherence was controlled via the coaches’ daily exercise log books.
Participants
A total of 26 (13 male/13 female) healthy competitive young swimmers took part in this study (mean ± SD: age, 10.5 ± 1.4 years; weight, 45.2 ± 9.7 kg; height, 156.5 ± 8.1 cm). All children were accustomed to a training workload of more than four training units per week and had been frequently involved in swimming competitions at distances between 50 and 100 m for at least 3 years. Five swimmers were members of a federal junior all star team. The others competed at West-German regional level. The group was initially divided into a training group that mainly performed high-intensity intervals and one training group with continuous loads of endurance training according to their personal 100 m freestyle best time. The participants, as well as their guardians, were informed about the design of the study, with special information about possible risks and benefits, and both subsequently signed an informed consent document prior to the start of the study. The study protocol was performed in accordance with the Declaration of Helsinki and the Ethical Committee of the German Sports University in Cologne, Germany.
Experimental procedures
Intervention
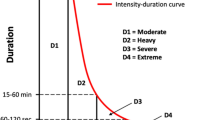
The training included 5 sessions per week in a 50 m outdoor pool. For both groups, 2 × 25 sessions were planned. One session was canceled because of poor weather conditions. Each training session had the same structure for both groups (Fig. 2).

a Example for the structure of one training session for both HIIT (high-intensity interval training) and HVT (high-volume training). b The total amount of intervals (50–800 m) for HIIT and HVT during one intervention phase
After a warm-up of approximately 400 m with varying medleys, a block with technical drills followed. In this, 10–15 × 20 m intervals were executed emphasizing different technical skills (stroke quality, start, turns, etc.). In the subsequent main part, the contents differed between the groups. The total length of this section was 30 min for HIIT versus 60 min for HVT. At the end of each session, a cool down followed.
During the main part of the training session, the intensity for each interval during HIIT was set at 92% of personal best time and for HVT it was 85% of personal best time of each distance. In each training session, all interval times for each child were taken manually and the rating of perceived exertion (Borg 1970) was recorded immediately after each interval during the main part of the training session. At the same time, blood samples for capillary lactate concentration were collected.
Diagnostics
Peak oxygen uptake (VO2peak) was assessed during a bicycle ramp protocol. For this purpose, a children’s bike (Pegasus-Arcona, ZEG eG, Köln, Germany) was installed in an ergometric appliance (Cyclus 2, RBM Elektronik-Automation GmbH, Leipzig, Germany). The initial workload was set at 25 W and increased every 3 min by 25 W. Oxygen uptake was measured with an open circuit breath-by-breath spirograph (nSpire, Zan 600 USB, Oberthulba, Germany) throughout the testing, using standard algorithms with dynamic account for the time delay between the gas consumption and volume signal. The spirograph was calibrated prior to each test, using calibration gas (15.8% O2, 5% O2 in N; Praxair, Düsseldorf, Germany) targeting the range of anticipated fractional gas concentration administered with a precision 1L syringe (nSpire, Oberthulba, Germany).
All respiratory data were averaged every 30 s. The highest values for oxygen uptake within the last 30 s of the test were used for statistical analysis. The criteria for VO2peak were (a) plateau in oxygen uptake, i.e. an increase less than 1.0 mL min−1 kg−1 despite an increase in power output, (b) respiratory exchange ratio greater than 1.10, (c) heart rate ± 5% of age predicted maximal heart rate, and (d) maximal capillary blood lactate after exercise greater than 6 mmol L−1. In all cases, at least three of the four criteria were met.
The ventilatory threshold (V T) was automatically determined by the manufacturer’s software as an increase in the ventilatory equivalent for oxygen (V E/VO2) with no associated increase in the ventilatory equivalent for carbon dioxide (V E/VCO2) (Davis et al. 1979; Hoogeveen and Hoogsteen 1999). V T is expressed as percentage of VO2peak.
Two days after the ramp protocol a 2,000 m endurance test according to Maglischo (2003) took place. This was conducted to determine the swimmer’s time over 2,000 m (T 2,000 m). One day later, the maximum rate of lactate accumulation following a 100-m sprint was determined. For this, post-exercise capillary lactate concentrations were assessed in minutes 1, 3, 5, 7 and 10 after the 100-m sprint. This rate is assumed to be an indicator for anaerobic performance skills (Heck and Schulz 2002). Accordingly, the maximum rate of lactate accumulation (Lacmax) was calculated with the Eq. 1:
whereas Lacpeak = peak post-exercise lactate concentration, Lacpre = pre-start lactate concentration, T 100 = time for 100 m sprint and T alak = fictitious alactic time (2 s) at the beginning of the sprint (Heck and Schulz 2002).
Twenty microliters of blood samples were collected from the right earlobe in order to determine capillary lactate concentrations during intervention and diagnostics. All blood samples were analyzed amperometric-enzymatically for blood lactate concentration using Ebio Plus (Eppendorf, Germany). All blood samples were analyzed in duplicate and the mean of the two measures was used for statistical analysis.
Competition performance was assessed during the same swim events. For this, all children performed a 100-m freestyle and 50-m breast stroke competition at regional level before and after both intervention phases using the international LEN (“Ligue Européene de Natation”, the European Governing Body) pointing system to evaluate their performance. LEN is calculated with the Eq. 2:
whereas T WR = world records as of the last Olympic Games, T = time achieved by the athlete during competition.
During the intervention period, all swimmers were asked to verbally rate their perceived exertion based on a Borg’s 6–20 scale (Borg 1970) which was displayed on a waterproof sheet.
Tanner stages were used to assess sexual maturation (Tanner and Whitehouse 1976). The guardians were given line drawings and written explanations of each developmental stage, using pubic hair in boys and both pubic hair and breast development in girls. A researcher who was knowledgeable with the Tanner stage criteria was available to answer questions. Body weight and fat-free mass were obtained with a four electrode bioimpedance body scale (Tanita BC 418 MA, Tanita Corp., Tokyo, Japan).
Statistical analyses
All data were calculated with conventional procedures as mean values and standard deviation (SD). Pre to post differences were described as percentage differences and presented in Table 1. The effect size Cohen’s d (Cohen 1988) was calculated (Eq. 3) for all variables between pre- and post-testing.
whereas mean1 and SD1 represent the values for pre-testing and mean2 and SD2 for post testing. The thresholds for small, moderate, and large effects were 0.20, 0.50, and 0.80, respectively (Cohen 1988). All data were checked for normality, with no data needing further transformation. Repeated-measures ANOVA was used to compare responses in each variable across the four time points. When a global difference over time was determined, Bonferroni post hoc analysis was used to identify where changes occurred. An alpha of P < 0.05 was used for statistical significance and marked with an asterisk. All statistical tests were processed using the Statistica (version 7.1, StatSoft Inc., Tulsa, OK, USA) software package for Windows®.
Results
Training
The total training volume for HIIT averaged 5.5 km per week and 11.9 km for HVT. Within a 5-week period, 27.4 km were accomplished during HITT and 59.6 km during HVT. In both groups, 96% of all training sessions were completed. The ratings of perceived exertion on Borg’s scale were significantly higher during HIIT (18.5 ± 1.5) as compared to HVT (13.7 ± 2.4; P < 0.01). The average blood lactate concentration during HIIT (7.0 ± 1.5 mmol L−1) was ~3.5-fold higher compared to HVT (2.0 ± 0.8 mmol L−1; P < 0.01).
Diagnostics
The mean pre and post changes and differences in percentage, as well as effect sizes for all variables following HIIT and HVT, and for groups A, B are presented in Table 1. Peak oxygen uptake increased after HIIT (+10.2%, effect size = 0.57) and HVT (8.5%, effect size = 0.46; P < 0.05) whereas V T remained unaltered (P = 0.31–0.41; effect size = 0.20–0.52) following HIIT and HVT. The rate of maximal lactate accumulation increased following HIIT (P < 0.01, effect size = 0.43) and decreased following HVT (P < 0.01; effect size = 0.51). According to the LEN-points, competition performance increased after HIIT by 14.8% (P < 0.01; effect size = 0.48) with no changes after HVT (5.8%, P = 0.28; effect size = 0.17). T 2,000 m decreased only after HIIT (P = 0.04; effect size = 0.21). T 100 m did not change after either intervention in both groups. Fat-free mass and body weight remained unaltered during the entire intervention (up to P = 0.11). Body stature increased in both groups (group A, 156.3 ± 7.4–158.3 ± 8.1 cm and group B, 156.3 ± 8.5–157.6 ± 9.0 cm; P < 0.01).
Discussion
The findings from this crossover intervention revealed a significant increase in competition and T 2,000 m performance following HIIT. Furthermore, Lacmax increased following HIIT and decreased after HVT. VO2peak increased following both interventions. These results were achieved in significantly less training time and volume in HIIT compared to HVT.
Training in young swimmers at the age of 9–11 is often limited by time factors, such as leisure time activities and school commitments. Coaches struggle with other training groups for water space for their athletes and time for the development of limiting factors. From this perspective, it seems logical that time-saving strategies for enhancing performance-limiting factors, such as efficient propulsion, endurance and strength performance are desirable. Furthermore, the athletes also want to achieve appropriate competition results for the time they invest in their training.
The authors of the present study are aware that assessing the young swimmers’ VO2peak and V T expressed as %VO2peak on a bicycle ergometer will not entirely reflect swim-specific aerobic capacity. A swim flume equipped with online VO2-measurement or portable breath-by-breath devices would potentially deliver closer swim-specific values. However, preliminary studies showed that the children of that age are not capable, or they feel uncomfortable, using a snorkel in the flume and the pool at high intensities. Nevertheless, oxygen uptake measurement on a bicycle ergometer may be a useful indictor for revealing changes in cardiovascular fitness. Several studies in different disciplines have shown that HIIT (4–6 sessions per week) executed for several weeks improves VO2max in moderately trained persons (Helgerud et al. 2001; Hickson et al. 1977; Laursen and Jenkins 2002; Tabata et al. 1996). Both training strategies in the present study showed increases in VO2peak (HIIT, +10.2% and HVT, +8.5%) with low to moderate effect sizes, indicating that both training approaches increased the swimmers’ aerobic capacities with a range of 0.4–0.5% per training session. This elevation in VO2peak with moderate to large effect size, by 8.5–10.2%, is comparable to improvements in VO2peak from other training studies that have compared HIIT and HVT (Baquet et al. 2002; Helgerud et al. 2001; McMillan et al. 2005).
During exercise testing at progressively increasing intensities, a work rate is reached where, relative to VO2, there is a disproportionate increase in CO2 output and ventilation; i.e., the ventilatory threshold (V T). In the present study no significant responses of V T expressed as %VO2peak were apparent for either training method. However, effect size calculation revealed moderate to high effects following HIIT and low to moderate effects following HVT. Changes in V T have been reported to be significantly correlated with the working muscles’ muscle oxidative capacity (Rusko et al. 1980). Thus, as swimmers predominantly perform upper body exercise, it may be possible that changes in V T will not be apparent when testing swimmers on a cycle ergometer. This would explain why no changes in V T were apparent, although we are unaware of data concerning the magnitude of changes in muscle oxidative capacity.
Lacmax increased significantly after HIIT (+20.1%) and decreased after HVT (−30.1%). There are currently no simplified practical tests that allow an accurate determination of anaerobic capacity besides the mere measurement of sprint time. In different disciplines, the maximum rate of lactate accumulation is used to estimate anaerobic performance skills (Heck and Schulz 2002). Higher rates of blood lactate accumulation indicate increased anaerobic energy yielding. As Lacmax increases after HIIT, it may lead to a greater contribution of anaerobic pathways generating more energy in a short time. This also leads to greater power production while sprinting. Lacmax, on the other hand, decreased after HVT, which could explain the deteriorated competition performance after HVT, due to decreased anaerobic performance.
The data in this study demonstrate that competition performance (LEN-points) increased significantly, 8.1–12.5%, in both groups following HIIT. These achievements were accomplished in approximately 2 h/week less time and 50% less training volume compared to HVT. As the training periodization in young swimmers is more or less planned according to school breaks and does not focus on important swim events requiring special tapering, HIIT may be a useful tool for focusing valuable training time on aspects other than increasing cardio-respiratory fitness. A recent study showed that in post-pubertal swimmers, competitive 100 and 400 m performance times during a 3-month period were similarly enhanced after both HIIT and HVT training strategies (Faude et al. 2008). The doubling of training volume did not show any benefits on sprint performance, as described in adult swimmers (Costill et al. 1988, 1991). Additionally, Trinity et al. (2008) showed 8–14% higher maximal mechanical power values when compared to low-intensity tapering periods in competitive collegiate swimmers. Based on these data, an extraordinarily high aerobic capacity induced by high training volume does not seem to be a necessary precondition for competitions over 50–400 m in adults. However, a high aerobic capacity may allow the young swimmer to recover faster between maximal bouts. This may be important when training sessions contain physically demanding bouts or in a swimming competition when the swimmer has to participate in a number of events in a very short period of time, e.g., within 30–60 min.
Interestingly, in the present study the performance time in the swim-specific endurance test (T 2,000 m time) was enhanced after HIIT but not after HVT. In swimming, it was recently shown that increasing intensity not only increased physiological demands, but also compromised stroke length (Dekerle et al. 2002). Thus, intensities above the maximal lactate steady state represent a useful intensity at which to carry out technical work (Dekerle et al. 2002) and maintaining and/or developing aerobic and anaerobic capacity at the same time (Baron et al. 2003). This might explain why T 2,000 m increases following HIIT.
A sudden increase in volume and/or exercise intensity over a longer period, e.g., in intensity or volume blocks, comparable to the present intervention, could lead to “overreaching” or even overtraining symptoms (Baquet et al. 2002; Smith 2003). Such unwanted conditions may result in a reduced maximum physical capacity (Baquet et al. 2002) or “burnout” symptoms like a washed-out feeling, tiredness, lack of energy, chronic performance decrements, biomechanical changes, muscle and joint pain, as well as decreased immunity (Montpetit et al. 1987; Ryan et al. 1987). None of the swimmers or the parents reported any of these symptoms after both training periods. Longer training periods with chronic high intensities could possibly provoke these symptoms. Future studies with longer training periods will need to take this into account.
Conclusion
Five weeks of HIIT revealed a significant increase in competition and T 2,000 m performance. Furthermore, Lacmax increased following HIIT and decreased after HVT. VO2peak increased following both interventions. These short-term effects were achieved in 2 h per week less exercise time. From a coach’s perspective, exercise time, especially in children, is limited because of other factors such as school and recreational activities. Accordingly, time-saving strategies in swimming are necessary in order to enhance other relevant parameters, such as stroke technique. This data suggests that short-term high-intensity interval training, performed 4–5 times per week for 5 weeks, leads to an increase in peak oxygen uptake, 2,000 m time and competition performance. Secondly, the data show that high training volumes, usually performed in competitive swimmers, are not advantageous when compared to high-intensity training at lower volumes.
References
Baquet G, Berthoin S, Dupont G, Blondel N, Fabre C, van Praagh E (2002) Effects of high intensity intermittent training on peak VO(2) in prepubertal children. Int J Sports Med 23:439–444
Baron B, Dekerle J, Robin S, Neviere R, Dupont L, Matran R, Vanvelcenaher J, Robin H, Pelayo P (2003) Maximal lactate steady state does not correspond to a complete physiological steady state. Int J Sports Med 24:582–587
Borg G (1970) Perceived exertion as an indicator of somatic stress. Scand J Rehabil Med 2:92–98
Cohen D (1988) Statistical power analysis for the behavioral sciences. Lawrence Erlbaum Associates, Hillsdale, NJ
Costill DL, Flynn MG, Kirwan JP, Houmard JA, Mitchell JB, Thomas R, Park SH (1988) Effects of repeated days of intensified training on muscle glycogen and swimming performance. Med Sci Sports Exerc 20:249–254
Costill DL, Thomas R, Robergs RA, Pascoe D, Lambert C, Barr S, Fink WJ (1991) Adaptations to swimming training: influence of training volume. Med Sci Sports Exerc 23:371–377
Davis JA, Frank MH, Whipp BJ, Wasserman K (1979) Anaerobic threshold alterations caused by endurance training in middle-aged men. J Appl Physiol 46:1039–1046
Dekerle J, Sidney M, Hespel JM, Pelayo P (2002) Validity and reliability of critical speed, critical stroke rate, and anaerobic capacity in relation to front crawl swimming performances. Int J Sports Med 23:93–98
Faude O, Meyer T, Scharhag J, Weins F, Urhausen A, Kindermann W (2008) Volume vs intensity in the training of competitive swimmers. Int J Sports Med 29:906–912
Heck H, Schulz H (2002) Diagnostics of anaerobic power and capacity. Dtsch Z Sportmed 53:202–212
Helgerud J, Engen LC, Wisloff U, Hoff J (2001) Aerobic endurance training improves soccer performance. Med Sci Sports Exerc 33:1925–1931
Hickson RC, Bomze HA, Holloszy JO (1977) Linear increase in aerobic power induced by a strenuous program of endurance exercise. J Appl Physiol 42:372–376
Hoogeveen AR, Hoogsteen GS (1999) The ventilatory threshold, heart rate, and endurance performance: relationships in elite cyclists. Int J Sports Med 20:114–117
Laursen PB, Jenkins DG (2002) The scientific basis for high-intensity interval training: optimising training programmes and maximising performance in highly trained endurance athletes. Sports Med 32:53–73
Maglischo EW (2003) Swimming fastest. Human Kinetics, Champaign, IL
McMillan K, Helgerud J, Macdonald R, Hoff J (2005) Physiological adaptations to soccer specific endurance training in professional youth soccer players. Br J Sports Med 39:273–277
Montpetit R, Duvallet A, Cazorla G, Smith H (1987) The relative stability of maximal aerobic power in elite swimmers and its relationship to training performance. J Swim Res 3:15–18
Mujika I (1998) The influence of training characteristics and tapering on the adaptation in highly trained individuals: a review. Int J Sports Med 19:439–446
Rusko H, Rahkila P, Karvinen E (1980) Anaerobic threshold, skeletal muscle enzymes and fiber composition in young female cross-country skiers. Acta Physiol Scand 108:263–268
Ryan R, Coyle E, Quick R (1987) Blood lactate profile throughout a training season in elite female swimmers. J Swim Res 6:5–10
Sharp R (2000) Physiology of swimming. In: Garret W, Kirkendall DT (eds) Exercise and sport science. Lippincott Williams and Wilkins, Philadelphia, pp 895–904
Smith DJ (2003) A framework for understanding the training process leading to elite performance. Sports Med 33:1103–1126
Tabata I, Nishimura K, Kouzaki M, Hirai Y, Ogita F, Miyachi M, Yamamoto K (1996) Effects of moderate-intensity endurance and high-intensity intermittent training on anaerobic capacity and VO2max. Med Sci Sports Exerc 28:1327–1330
Tanner JM, Whitehouse RH (1976) Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child 51:170–179
Trinity JD, Pahnke MD, Sterkel JA, Coyle EF (2008) Maximal power and performance during a swim taper. Int J Sports Med 29:500–506
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Susan Ward.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Sperlich, B., Zinner, C., Heilemann, I. et al. High-intensity interval training improves VO2peak, maximal lactate accumulation, time trial and competition performance in 9–11-year-old swimmers. Eur J Appl Physiol 110, 1029–1036 (2010). https://doi.org/10.1007/s00421-010-1586-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-010-1586-4