
Abstract
Purpose
Our purpose was to describe the clinical course, and individualized management approaches, of patients with migration of a dexamethasone implant into the anterior chamber.
Methods
This was a retrospective review of four patients with seven episodes of anterior chamber migration of a dexamethasone implant.
Results
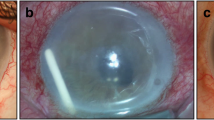
After 924 intravitreal dexamethasone injections, anterior migration of the implant occurred in four eyes of four patients (0.43%). All four eyes were pseudophakic: one eye had a posterior chamber intraocular lens in the capsular bag but in a post-laser posterior capsulotomy state, two eyes had a sulcus intraocular lens (IOL), and one eye had an iris-fixated retropupillary IOL. All eyes had a prior vitrectomy and no lens capsule. The time interval from injection to detection of the implant migration ranged from 2 to 6 weeks. Of the four eyes with corneal edema, only one eye required a corneal transplantation, although it was unclear whether the implant migration was the direct cause of the corneal decompensation because the patient had a history of bullous keratopathy resulting from an extended history of uveitis. All patients underwent surgical intervention: two patients with a repositioning procedure, and the other two patients with removal due to repeated episodes, although surgical removal was not always necessary to reverse the corneal complications.
Conclusions
In our study, not all patients required surgical removal of the implants. Repositioning the implant back into the vitreous cavity may be considered as an option in cases involving the first episode with no significant corneal endothelial decompensation. Considering potential anterior segment complications and the loss of drug effectiveness together, an individualized approach is recommended to obtain the best treatment outcomes and to minimize the risk of corneal complications.



Similar content being viewed by others


References
Lowder C, Belfort R Jr, Lightman S et al (2011) Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Arch Ophthalmol 129(5):545–553
Boyer DS, Yoon YH, Belfort R Jr et al (2014) Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology 121(10):1904–1914
Calvo P, Ferreras A, Al Adel F et al (2015) Dexamethasone intravitreal implant as adjunct therapy for patients with wet age-related macular degeneration with incomplete response to ranibizumab. Br J Ophthalmol 99(6):723–726
Vela JI, Crespi J, Andreu D (2012) Repositioning of dexamethasone intravitreal implant (Ozurdex) migrated into the anterior chamber. Int Ophthalmol 32(6):583–584
Kishore SA, Schaal S (2013) Management of anterior chamber dislocation of dexamethasone implant. Ocul Immunol Inflamm 21(1):90–91
Khurana RN, Appa SN, McCannel CA et al (2014) Dexamethasone implant anterior chamber migration: risk factors, complications, and management strategies. Ophthalmology 121(1):67–71
Bansal R, Bansal P, Kulkarni P et al (2012) Wandering Ozurdex® implant. J Ophthalmic Inflamm Infect 2(1):1–5
Pardo-Lopez D, Frances-Munoz E, Gallego-Pinazo R, Diaz-Llopis M (2012) Anterior chamber migration of dexametasone intravitreal implant (Ozurdex®). Graefes Arch Clin Exp Ophthalmol 250(11):1703–1704
Ruiz-Casas D, Gros-Otero J, Casado A (2016) Dexamethasone implant removal from anterior chamber: surgical technique. Retin Cases Brief Rep 10(4):313–315
Haller JA, Bandello F, Belfort R Jr et al (2010) Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology 117(6):1134–1146
Boyer DS, Faber D, Gupta S et al (2011) Dexamethasone intravitreal implant for treatment of diabetic macular edema in vitrectomized patients. Retina 31(5):915–923
Stepanov A, Codenotti M, Ramoni A et al (2016) Anterior chamber migration of dexamethasone intravitreal implant (Ozurdex®) through basal iridectomy (Ando) in a pseudophakic patient. Eur J Ophthalmol 26(3):e52–e54
Smith SG, Lindstrom RL (1985) Malpositioned posterior chamber lenses: etiology, prevention, and management. J Am Intraocul Implant Soc 11(6):584–591
Cronin KM, Govind K, Kurup SK (2012) Late migration of dexamethasone implant into anterior chamber. Arch Ophthalmol 130(6):711
Eadie JA, Lesser R, Capone A Jr (2012) Migration of ozurdex implant into the anterior chamber. Retin Cases Brief Rep 6(3):269–270
Voykov B, Bartz-Schmidt KU (2012) Dislocation of dexamethasone intravitreous implant. Arch Ophthalmol 130(6):706
Jonas JB, Schmidbauer M (2013) Steroid implant in anterior chamber of an aphakic vitrectomized eye. Graefes Arch Clin Exp Ophthalmol 251(1):385–386
Chan A, Leung LS, Blumenkranz MS (2011) Critical appraisal of the clinical utility of the dexamethasone intravitreal implant (Ozurdex) for the treatment of macular edema related to branch retinal vein occlusion or central retinal vein occlusion. Clin Ophthalmol 5:1043–1049
Rahimy E, Pitcher JD 3rd, Abbey AM et al (2015) No-touch removal of anterior segment-migrated dexamethasone implant. Retina 35(11):2414–2416
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations
with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
For this type of study, formal consent is not required
Informed consent
Informed consent was obtained from all individual participants included in the study.
Grant support
None
Funding
No funding was received for this research.
Rights and permissions
About this article

Cite this article
Kang, H., Lee, M.W., Byeon, S.H. et al. The clinical outcomes of surgical management of anterior chamber migration of a dexamethasone implant (Ozurdex®). Graefes Arch Clin Exp Ophthalmol 255, 1819–1825 (2017). https://doi.org/10.1007/s00417-017-3705-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-017-3705-y