
Abstract
Aim
To assess anatomic changes on computed tomography (CT) after neoadjuvant FOLFIRINOX (5-fluorouracil/leucovorin/irinotecan/oxaliplatin) chemotherapy for secondary resected borderline resectable (BR) and locally advanced (LA) pancreatic adenocarcinoma and their accuracy to predict resectability and pathological response.
Methods
Thirty-six patients with secondary resected BR/LA pancreatic adenocarcinoma after neoadjuvant FOLFIRINOX chemotherapy (± chemoradiotherapy) were retrospectively included. Two radiologists reviewed baseline and pre-surgical CTs in consensus. NCCN (National Comprehensive Cancer Network) classification, largest axis, product of the three axes (P3A), and arterial/venous involvement were studied and compared to pathological response and resection status and to disease-free survival (DFS).
Results
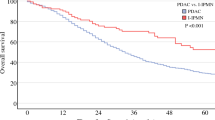
Thirty-one patients had R0 resection, including only six exhibiting a downstaging according to the NCCN classification. After treatment, the largest axis and P3A decreased (P < 0.0001). The pre-surgical largest axis and P3A were smaller in case of R0 resection (P = 0.019/P = 0.021). The largest axis/P3A variations were higher in case of complete pathological response (P = 0.011/P = 0.016). A decrease of the arterial/venous involvement was not able to predict R0 or ypT0N0 (P > 0.05). Progression of the vascular involvement was seen in two (5 %) patients and led to a shorter DFS.
Conclusion
In BR/LA pancreatic adenocarcinoma after the neoadjuvant FOLFIRINOX regimen (± chemoradiotherapy), significant tumour size decreases were observed on CT. However, CT staging was not predictive of resectability and pathological response.
Key Points
• Significant tumour size decreases were observed on CT after FOLFIRINOX (± chemoradiotherapy).
• CT is not able to predict R0 resection accurately after FOLFIRINOX (± chemoradiotherapy).
• CT is not able to predict complete response accurately after FOLFIRINOX (± chemoradiotherapy).
• Even with a stable NCCN classification, BR/LA pancreatic adenocarcinoma could have R0 resection.






Similar content being viewed by others

Abbreviations
- BR:
-
borderline resectable
- CA:
-
coeliac artery
- CT:
-
computed tomography
- HA:
-
hepatic artery
- LA:
-
locally advanced
- NCCN:
-
National Comprehensive Cancer Network
- P3A:
-
product of the three axes
- PD:
-
progressive disease
- PR:
-
partial response
- PV:
-
portal vein
- RECIST:
-
response evaluation criteria in solid tumours
- ROI:
-
region of interest
- SD:
-
stable disease
- SMA:
-
superior mesenteric artery
- SMV:
-
superior mesenteric vein
REFERENCES
Puleo F, Maréchal R, Demetter P et al (2015) New challenges in perioperative management of pancreatic cancer. World J Gastroenterol 21(8):2281–2293
Coleman MP, Gatta G, Verdecchia A et al (2003) EUROCARE-3 summary: cancer survival in Europe at the end of the 20th century. Ann Oncol 14(Suppl 5):v128–v149
Sa Cunha A, Rault A, Laurent C et al (2005) Surgical resection after radiochemotherapy in patients with unresectable adenocarcinoma of the pancreas. J Am Coll Surg 201(3):359–365
Burris HA, Moore MJ, Andersen J et al (1997) Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 15(6):2403–2413
Conroy T, Desseigne F, Ychou M et al (2011) FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 364(19):1817–1825
Von Hoff DD, Ervin T, Arena FP et al (2013) Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 369(18):1691–1703
Petrelli F, Coinu A, Borgonovo K et al (2015) FOLFIRINOX-based neoadjuvant therapy in borderline resectable or unresectable pancreatic cancer: a meta-analytical review of published studies. Pancreas 44(4):515–521
Ferrone CR, Marchegiani G, Hong TS et al (2015) Radiological and surgical implications of neoadjuvant treatment with FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer. Ann Surg 261(1):12–17
NCCN. National Comprehensive Cancer Network. NCCN practice guidelines for pancreatic cancer, version 2. Available at http://www.nccn.org/professionals/physician_glslrecently_updated.asp. 2014.
Cassinotto C, Cortade J, Belleannée G et al (2013) An evaluation of the accuracy of CT when determining resectability of pancreatic head adenocarcinoma after neoadjuvant treatment. Eur J Radiol 82(4):589–593
Morgan DE, Waggoner CN, Canon CL et al (2010) Resectability of pancreatic adenocarcinoma in patients with locally advanced disease downstaged by preoperative therapy: a challenge for MDCT. AJR Am J Roentgenol 194(3):615–622
Pietrasz D, Marthey L, Wagner M, et al (2015) Pathologic major response after FOLFIRINOX is prognostic for patients secondary resected for borderline or locally advanced pancreatic adenocarcinoma: an AGEO-FRENCH, prospective, multicentric cohort. Ann Surg Oncol 22 (Suppl 3):S1196–205
Cassinotto C, Mouries A, Lafourcade J-P et al (2014) Locally advanced pancreatic adenocarcinoma: reassessment of response with CT after neoadjuvant chemotherapy and radiation therapy. Radiology 273(1):108–116
Eisenhauer EA, Therasse P, Bogaerts J et al (2009) New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 45(2):228–247
Tempero MA, Malafa MP, Behrman SW et al (2014) Pancreatic adenocarcinoma, version 2.2014: featured updates to the NCCN guidelines. J Natl Compr Cancer Netw 12(8):1083–1093
Edge SB, Compton CC (2010) The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 17(6):1471–1474
Staley CA, Cleary KR, Abbruzzese JL et al (1996) The need for standardized pathologic staging of pancreaticoduodenectomy specimens. Pancreas 12(4):373–380
Katz MHG, Crane CH, Varadhachary G (2014) Management of borderline resectable pancreatic cancer. Semin Radiat Oncol 24(2):105–112
Tamm EP, Loyer EM, Faria S et al (2006) Staging of pancreatic cancer with multidetector CT in the setting of preoperative chemoradiation therapy. Abdominal Imaging 31(5):568–574
White RR, Paulson EK, Freed KS et al (2001) Staging of pancreatic cancer before and after neoadjuvant chemoradiation. J Gastrointest Surg 5(6):626–633
Balthazar EJ (2005) Pancreatitis associated with pancreatic carcinoma. Preoperative diagnosis: role of CT imaging in detection and evaluation. Pancreatology 5(4-5):330–344
Ishii H, Furuse J, Nakachi K, Suzuki E, Yoshino M (2005) Primary tumor of pancreatic cancer as a measurable target lesion in chemotherapy trials. Jpn J Clin Oncol 35(10):601–606
Acknowledgements
The scientific guarantor of this publication is Jean-Baptiste Bachet. The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. No complex statistical methods were necessary for this paper. Institutional Review Board approval was obtained. Written informed consent was waived by the Institutional Review Board.
All patients of the current study were included in a larger clinical study, which reports the postoperative and oncological outcomes of secondary pancreatic resection after neoadjuvant FOLFIRINOX in patients with initially BR or LA pancreatic adenocarcinoma (Pietrasz et al, Ann Surg Oncol 2015). This study focussed on the outcomes and did not overlap with the current study, as no imaging data were evaluated after the treatment in Pietrasz et al.
Ten patients of the current study were also included in a radiological study, assessing CT evaluation after neoadjuvant chemotherapy and chemoradiotherapy, whatever the chemotherapy regimen (Cassinotto et al, Radiology 2014). This study included only locally advanced pancreatic head adenocarcinoma, treated by neoadjuvant chemotherapy and chemoradiotherapy. Unlike in our study, the chemotherapy regimen was either GEMOX or FOLFORINOX. Even if there is an overlap between this study and the current study, the aim of the current study was to focus on the accuracy of CT to assess response after FOLFIRINOX and to predict complete resection after this specific chemotherapy regimen. Moreover, the scoring system used to assess the vascular involvement was different in the current study and we also assessed the downstaging according to the NCCN guidelines.
Methodology: retrospective, observational, multicentre study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Oliver Lucidarme and Jean-Baptiste Bachet contributed equally.
Rights and permissions
About this article

Cite this article
Wagner, M., Antunes, C., Pietrasz, D. et al. CT evaluation after neoadjuvant FOLFIRINOX chemotherapy for borderline and locally advanced pancreatic adenocarcinoma. Eur Radiol 27, 3104–3116 (2017). https://doi.org/10.1007/s00330-016-4632-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4632-8