
Abstract
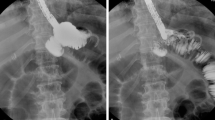
The esogastric anastomotic fistula,occurring after the replacement of esophagus by the stomach, is a post-operative complication always feared and awaited. Apart from other causes, there exist the anatomical dispositions notably the vascular and technical factors that stress this potential risk despite certain advantages of esophagogastroplasty. The goal of our study was to study the arterial distribution of the gastric transplants in order to identify the better modalities of their making. We used 39 stomachs taken from fresh cadavers of autochtone subjects. After a modeling treatment using three different techniques, they were subjected to a radiographic opacification of the right gastro-epiploic artery with sulphate of barium follow by an x-rays in incidence full-face (25 kv, 10 mAS). It was a matter of 15 entire stomachs (E.E.) with denudation of the small curvature, of 12 wide gastric tubes (W.T.) prepared according to the Akiyama technique modified and of 12 narrow tubes (N.T.) tubulized according to the Marmuse method. We studied the anastomotic type of the gastro-epiploic arterial circle according to the classification of Koskas, the collateral branches of the arterial circles of the gastric curvatures, the antral and corporeal anastomosis of these circles and the distribution anastomotic at the level of the summit of the anastomotic. Only 28 pieces (15 E.E., 8 W.T. and 5 N.T.) were able to be the object of a complete angiographic exploitation. The anastomosis of the arterial circle was type I in 64.1% of the cases, type II in 15.4% of the cases, type III in 15.4% of the cases and type IV in 5.1% of the cases. The average number of collateral branches originating from gastro-epiploic arterial circle was respectively 24, 17 and 22 for the E.E., the W.T. and the N.T. Only the two first ones presented collateral branches being borne of the small curvature circle. Fifty per cent of the N.T. did not possess any antral or corporeal anastomosis between the two arterial circles; some of them were even for a quarter of the W.T. In the case of gastric tubulization there existed an irrigation defect of the summit of the plasty for a third of the N.T. and a quarter of the W.T., despite a constant intramural bridge anastomosis between the two gastro-epiploic arteries. The usage of the entire stomach must be recommended for gastric oesophagoplasty; but when the operative indications require a resection of the small curvature it is preferable to use a wide gastric tube whose diameter respects the two left third of the initial width of the organ.









Similar content being viewed by others


References
Agossou-Voyémé AK, Hureau J, Germain MA (1990) Etude des problèmes vasculaires dans les o.p.g. après oesophagectomie ou pharyngo-laryngectomie circulaire. J Chir 127:141–149
Akiyama H, Miyazono H, Tsurumaru M, Hashimoto C, Kawamura T (1978) Use of the stomach as an esophageal substitute. Ann Surg 188:606–610
Collard JM, Otte JB, Kestens PJ (1990) Plastie oesophagienne utilisant l’estomac entier avec dénudation de la petite courbure. Lyon Chir 86:173–174
Collard JM, Tinton N, Malaise J, Romagnoli R, Otte JB, Kestens PJ (1995) Oesophageal replacement: gastric tube or whole stomach? Ann Thorac Surg 60:261–267
Cordier G, Debray C, Thomas J, Cabrol C (1955) Données récentes sur la vascularisation de la paroi gastrique. Conséquences pathologiques. Ann Chir 9:538–544
Dei Paoli M, Albertino B, Spalluto F, Andorno E, Bertero D, Gasparri G, Casalegno P, Ferrarotti G, Oliaro A (1990) Gastric angiography: data for oesophagogastroplasty. Panminerva Med 32:61–64
Diop M (1993) La vascularisation de l’estomac: données nouvelles sur la distribution des artères gastriques (à propos de 65 injection-corrosions) Thèse Médecine, Dakar, No. 3
El Eishi H, Ayoub JF, El Khalek M (1973) The arterial supply of the human stomach. Acta Anat 86:565–580
Hannoun L, Le Breton C, Bors V, Helenon C, Bigot JM, Parc R (1984) Radiological anatomy of the right gastroepiploic artery. Anat Clin 5:265–271
Khosrovani C, Le Neel JC, Kohen N, Guiberteau B, Vayre P (1994) Technique de gastroplastie oesophagienne isopéristaltique. Etude comparative de la vascularisation artérielle in vitro. J Chir 131:10–16
Khoury-Hélou A, Nonent M, Vandenbrouke F, Topart P, Lozac’h P (2001) Le déficit vasculaire est la cause majeure des fistules en chirurgie oesophagienne. Ann Chir 126:857–862
Koskas F, Gayet B (1985) Anatomical study of retrosternal gastric esophagoplasties. Anat Clin 7:237–256
Levasseur JC, Couinaud C (1968) Etude de la distribution des artères gastriques. J Chir 95:57–78
Liebermann-Meffert D, Meier R, Siewert J (1992) Vascular anatomy of the gastric tube use for esophageal reconstruction. Ann Thorac Surg 54:1110–1115
Marmuse JP (1988) Technique de l’oesophagectomie trans-hiatale. J Chir 125:585–592
Thomas D, Langford R, Russel R, Le Quesne L (1979) The anatomical basis for gastric mobilisation in total oesophagectomy. Br J Surg 66:230–233
Triboulet JP (1999) Intervention de Akiyama pour cancer de l’œsophage haut situé . J Chir 136:23–28
Vandamme JP, Bonte J (1986) Systématisation of the arteries in the splenic hilus. Acta Anat 125:217–224
Vandamme JP, Bonte J (1988) The blood supply of the stomach. Acta Anat 131:89–96
Yamato T, Hamonaka Y, Hirata S, Sakai K (1979) Esophagoplasty with an autogenous tubed gastric flap. Ann J Surg 137:197–202
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ndoye, JM., Dia, A., Ndiaye, A. et al. Arteriography of three models of gastric oesophagoplasty: the whole stomach, a wide gastric tube and a narrow gastric tube. Surg Radiol Anat 28, 429–437 (2006). https://doi.org/10.1007/s00276-006-0129-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-006-0129-5