
Abstract
Introduction
The terminology for female pelvic floor prolapse (POP) should be defined and organized in a clinically-based consensus Report.
Methods
This Report combines the input of members of two International Organizations, the International Urogynecological Association (IUGA) and the International Continence Society (ICS), assisted at intervals by external referees. Appropriate core clinical categories and a sub-classification were developed to give a coding to definitions. An extensive process of fourteen rounds of internal and external review was involved to exhaustively examine each definition, with decision-making by collective opinion (consensus).
Results
A Terminology Report for female POP, encompassing over 230 separate definitions, has been developed. It is clinically-based with the most common diagnoses defined. Clarity and user-friendliness have been key aims to make it interpretable by practitioners and trainees in all the different specialty groups involved in female pelvic floor dysfunction and POP. Female-specific imaging (ultrasound, radiology and MRI) and conservative and surgical managements are major additions and appropriate figures have been included to supplement and clarify the text. Emerging concepts and measurements, in use in the literature and offering further research potential, but requiring further validation, have been included as an appendix. Interval (5–10 year) review is anticipated to keep the document updated and as widely acceptable as possible.
Conclusion
A consensus-based Terminology Report for female POP has been produced to aid clinical practice and research.






































Similar content being viewed by others



Notes
In the era of advanced cellphone camera technology, a woman, at times, will bring photographic evidence of the prolapse at its worst. This can add to other clinical evidence, particularly if there is a discepancy between symptoms and signs.
The more formal classification of constipation is as follows:
Rome II diagnostic criteria for constipation:
• At least 12 weeks, which need not be consecutive, in the previous 12 months, of two or more of:
(i) Straining in > 1 in 4 defecations.
(ii) Lumpy or hard stools in > 1 in 4 defecations.
(iii) Sensation of incomplete evacuation in > 1 in 4 defecations.
(iv) Sensation of anorectal obstruction/ blockage in > 1 in 4 defecations.
(v) Manual manoeuvres to facilitate > 1 in 4 defecations (e.g.,: digital evacuation, support of the pelvic floor).
(vi) Less than 3 defecations per week.
• Loose stools are not present and there is insufficient evidence for IBS (irritable bowel syndrome)
A symptomatic-based subdivision of Stage II (see Appendix A) was overlooked at this time in favor of maintaining the current strictly anatomical definition of the “sign of POP”.
The axis of the retroverted uterus is parallel to that of the vaginal axis with less impediment to uterine (cervical) descent. In contrast, the anteverted uterus is perpendicular to the vaginal axis with impediment to descent by the posterior vaginal wall and behind that the rectum.
Detrusor underactivity: Detrusor contraction of reduced strength and/or duration, resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span.
Acontractile detrusor: The detrusor cannot be observed to contract during urodynamic studies resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span. The term “areflexia” has been used where there is a neurological cause but should be replaced by neurogenic acontractile detrusor.
Women with detrusor overactivity have a median UEBW of 48.0 g (95 % CI 46–51), with urodynamic stress incontinence a median UEBW of 30 g (95 % CI 29–31) and those who have associated detrusor overactivity and urodynamic stress incontinence have a median UEBW of 37.3 g (95 % CI 33–41) (p < 0.001) [37, 38]
Synthetic implant such as macroplastique, are hyperechogenic whereas collagen injections are hypoechoic and can be seen as spherical structures surrounding the bladder neck.
The importance of precise structural assessment of the urethral sphincter using multiple axial cross-sectional areas at set distances can assist the evaluation of women with stress urinary incontinence. It has been suggested that it may predict the severity of incontinence as well as the outcome of continence surgery since a weak sphincter will have a lower volume compared to a competent/continent urethral sphincter [39].
It is acknowledged this definition may not encompass cases of (i) symptoms of voiding dysfunction without abnormality of voiding parameters; (ii) abnormality of voiding parameters without symptoms of voiding dysfunction.
A more space occupying pessary.
A cuboid pessary does deliver ‘support’ by suction of the vaginal walls.
It was first described by Kelly in 1913 and involves dissection under the full thickness of the vaginal epithelium followed by central plication of the pubocervical fascia over the bulging bladder with excision of the ‘excess’ vaginal wall skin. The Kelly-Kennedy plication suture (Alt: bladder neck buttress) is an extrapolation of midline fascial plication involving placement of sutures under the proximal urethra and bladder neck to try and treat or prevent stress incontinence.
Its essential feature is suturing the cut cardinal/uterosacral ligament complex in front of the stump of the cervix hence pulling the cervix upwards and backwards, maintaining anteversion and creating anterior vaginal wall length.: This procedure can be performed intra- or extra-peritoneally. Concurrent McCall culdoplasty or vaginal vault suspension techniques may be employed dependant on the extent of prolapse [48].
Variations in technique for all abdominal mesh/graft procedures: (i) Type of mesh or graft used; (ii) Shape of mesh /graft- single piece,‘DIY’ two piece ‘Y’ mesh, Y mesh kit product; (iii) Points and length of attachment to vagina. (iv) Suture material employed / Metal stapling devices; (v) Peritoneal closure over mesh/graft.
This is usually performed in a woman with a uterus who is no longer sexually active. It can be performed in the absence of a uterus in a woman with vaginal eversion instead of total colpectomy. The Le Fort’s procedure involves denuding the vagina of skin both anteriorly and posteriorly, typically in a rectangular shape, avoiding the bladder neck and cervix. The cut edges are sewn together to achieve vaginal closure whilst leaving a bilateral epithelium-lined tunnel behind. The Labhardt procedure involves the removal of a 1 cm horse shoe shape of vaginal epithelium is removed over the posterior fourchette up to just under the urethra. By closing the incision and building up the perineum, an extremely high posterior repair almost closing the vagina is created.
The vagina is totally denuded of skin, typically in sections, whilst avoiding the bladder neck region. The prolapse is then reduced by a series of successive purse-string sutures and the epithelium at the entrance closed.
Mean length of Level II in women at posterior colporrhaphy found to be 5.0 cm [52]
The outer edge of the vestibule is known as Hart’s line (see white line in Fig. 39 with blue line demarcating anterior and posterior vestibule).
Mean length in women at posterior colporrhaphy was found to be 1.8 cm [52].
References
Haylen BT, Freeman RM, de Ridder D et al (2010) An International Urogynecological Association (IUGA)—International Continence Society (ICS) Joint report into the terminology for female pelvic floor dysfunction. Neurourol Urodyn 29:4–20, International Urogynecology J 2010;21:5–26
Abrams P, Blaivas JG, Stanton SL et al (1988) The standardisation of terminology of lower urinary tract function. Scand J Urol Nephrol Suppl 114:5–19
Abrams P, Cardozo L, Fall M et al (2002) The standardisation of terminology of lower urinary tract function. Report from the standardisation subcommittee of the International Continence Society. Neurourol Urodyn 21:167–178
Bump RC, Mattiasson A, Bo K et al (1996) The standardization of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol 175:10–11
Haylen BT, Freeman RM, Swift SE et al (2011) An International Urogynecological Association (IUGA) / International Continence Society (ICS) Joint Terminology and Classification of complications related directly to the insertion of prostheses (meshes, implants, tapes) and grafts in female pelvic floor surgery. Int Urogynecol J 22:3–15, Neurourology and Urodynamics 30(1):2–12
Haylen BT, Freeman RM, Lee J, et al (2012) An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint terminology and classification of the complications related to native tissue female pelvic floor surgery. Int Urogynecol 23:515–26. Neurourol Urodyn 31:406–14
Toozs-Hobson P, Freeman R, Barber M, et al (2012) An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint report on the terminology for reporting outcomes of surgical procedures for pelvic organ prolapse. Int Urogynecol 23:527–35. Neurourol Urodyn 31:415–26
Sultan A, Monga A, Haylen BT, et al (2015) An International Urogynecological Association (IUGA) / International Continence Society (ICS) Joint Report on the Terminology for Anorectal Dysfunction in Women (In Committee Review)
Bo K, Frawley H, Haylen BT, et al (2015) An International Urogynecological Association (IUGA) / International Continence Society (ICS) Joint report on the terminology for the conservative management of pelvic floor dysfunction. (In Committee Review)
Rogers R, Thakar R, Petri E, et al (2015) An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint report on the terminology for the sexual health in women with pelvic floor dysfunction. (In Committee Review)
Riss P, Dwyer PL (2014) The POP-Q classification system: looking back and looking forward. Int Urogynecol J 25:439–440
Bump RC (2014) The POP-Q system: two decades of progress and debate. Int Urogynecol J 25:441–443
Toozs-Hobson P, Swift S (2014) POP-Q stage 1 prolapse: is it time to alter our terminology? Int Urogynecol J 25:445–446
Harmanli O (2014) POP-Q 2. 0: its time has come. Int Urogynecol J 2014;25:447–449
(1995) Concise Oxford English Dictionary. 9th Edition. Oxford: Clarendon Press. p1438.
(2006) Stedman’s medical dictionary. 28th Edition. Lippincott William and Wilkins, Baltimore. p 1884
Rogers GR, Villarreal A, Kammerer-Doak D et al (2001) Sexual function in women with/without urinary incontinence and or pelvic organ prolapse. Int Urogynecol J 12:361–365
Yang A, Mostwin J, Genadry R et al (1993) Patterns of prolapse demonstrated with dynamic fastscan MRI; reassessment of conventional concepts of pelvic floor weaknesses. Neurourol Urodyn 12:310–311
Swift SE, Woodman P, O’Boyle A et al (2005) Pelvic Organ Support Study (POSST): the distribution, clinical definition and epidemiology of pelvic organ support defects. Am J Obstet Gynecol 192:795–806
Swift SE, Tate SB, Nichols J (2003) Correlation of symptomatology with degree of pelvic organ support in a general population of women: what is pelvic organ prolapse? Am J Obstet Gynecol 189:372–379
Barber MD, Brubaker L, Nygaard I et al (2009) Pelvic floor disorders network. Obstet Gynecol 114:600–609
Dietz HP (2007) Quantification of major morphological abnormalities of the levator ani. Ultrasound Obstet Gynecol 29:329–334
Haylen BT (2006) The retroverted uterus: Ignored to date but core to prolapse. Int Urogynecol J 17:555–558
Symmonds RE (1982) Relaxation of pelvic supports. In: Benson RC (ed) Current obstetrics and gynaecological diagnosis and treatment. Lange Medical Publications, Los Altos, pp 285–291 (chap 12)
Swift S, Morris S, McKinnie V et al (2006) Validation of a simplified technique for using the POPQ pelvic organ classification system. Int Urogynecol J 17:615–620
Parekh M, Swift S, Lemos N et al (2011) Multicentre inter-examiner trial of the validation of simplified POPQ system. Int Urogynecol J 22:645–650
Haylen BT, Lee J, Logan V et al (2008) Immediate postvoid residuals in women with symptoms of pelvic floor dysfunction: prevalences and associations. Obstet Gynecol 111:1305–1312
Fantl JA, Smith PJ, Schneider V et al (1982) Fluid weight uroflowmetry in women. Am J Obstet Gynecol 145:1017–1024
Haylen BT, Ashby D, Sutherst JR et al (1989) Maximum and average urine flow rates in normal male and female populations - the Liverpool nomograms. Br J Urol 64:30–38
Haylen BT, Parys BT, Ashby D et al (1990) Urine flow rates in male and female urodynamic patients compared with the Liverpool nomograms. Br J Urol 65:483–488
Schafer W, Abrams P, Liao L et al (2002) Good urodynamic practices: uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol Urodyn 21:261–274
Groutz A, Blaivas JG, Chaikin DC (2000) Bladder outflow obstruction in women: definition and characteristics. Neurourol Urodyn 19:213–220
Poston GJ, Joseph AE, Riddle PR (1983) The accuracy of ultrasound in the measurement of changes in bladder volume. Br J Urol 55:361–363
Haylen BT, Frazer MI, Sutherst JR et al (1989) Transvaginal ultrasound in the assessment of bladder volumes in women. Br J Urol 63:152–154
Dietz HP, Velez D, Shek KL et al (2012) Determination of postvoid residuals by translabial ultrasound. Int Urogynecol J 23:1749–52
Pineda M, Shek K, Wong V et al (2013) Can hiatal ballooning be determined by two-dimensional translabial ultrasound? Aust N Z J Obstet Gynaecol 53:489–493. doi:10.1111/ajo.12111, Epub 2013 Aug 2
Bright E, Oelke M, Tubaro A et al (2010) Ultrasound estimated bladder weight and measurement of bladder wall thickness-useful noninvasive methods for assessing the lower urinary tract? J Urol 184:1847–1854. doi:10.1016/j.juro.2010.06.006
Panayi DC, Khullar V, Digesu GA et al (2009) Is ultrasound estimation of bladder weight a useful tool in the assessment of patients with lower urinary tract symptoms? Int Urogynecol J Pelvic Floor Dysfunct 12:1445–1449. doi:10.1007/s00192-009-0964-0
Digesu GA, Calandrini N, Derpapas A et al (2012) Intraobserver and interobserver reliability of the three-dimensional ultrasound imaging of female urethral sphincter using a translabial technique. Int Urogynecol J 8:1063–1068. doi:10.1007/s00192-012-1669-3, Epub 2012 Jan 21
Rodrigo N, Wong V, Shek KL et al (2014) The use of 3-dimensional ultrasound of the pelvic floor to predict recurrence risk after pelvic reconstructive surgery. Aust N Z J Obstet Gynaecol 3:206–211. doi:10.1111/ajo.12171, Epub 2014 Feb 18
Dietz HP, Shek C, De Leon J et al (2008) Ballooning of the levator hiatus. Ultrasound Obstet Gynecol 6:676–680. doi:10.1002/uog.5355
Colaiacomo MC et al (2009) Dynamic MR imaging of the pelvic floor: a pictorial review. Radiographics 29, e35
DeLancey JO, Morgan DM, Fenner DE et al (2007) Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol 109:295–302
Fielding JR (2002) Practical MRI, imaging of female pelvic floor weakness. RadioGraphics 22:295–304
Torricelli P, Pecchi A, Caruso-Lombardi A et al (2002) Magnetic resonance imaging in evaluating functional disorders of female pelvic floor. Radiol Med 103:488–500
Rizk DE, Czechowski J, Ekelund L (2004) Dynamic assessment of pelvic floor and bony pelvis morphologic condition with the use of magnetic resonance imaging in a multi- ethnic, nulliparous, and healthy female population. Am J Obstet Gynecol 191:83–89
Lamers BH, Broekman BM, Milani AL (2011) Pessary treatment for pelvic organ prolapse and health-related quality of life; a review. Int Urogynecol J 6:637–644
de Boer TA, Milani AL, Kluivers KB et al (2009) The effectiveness of surgical correction of uterine prolapse: cervical amputation with uterosacral ligament plication (modified Manchester) versus vaginal hysterectomy with high uterosacral ligament plication. Int Urogynecol J 20:1313–1315
DeLancey JO (1992) Anatomical aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol 166:117–124
Zemlyn S (1981) The length of the uterine cervix and its significance. J Clin Ultrasound 9:267–269
Vu D, Haylen BT, Tse K et al (2010) Surgical anatomy of the uterosacral ligament. Int Urogynecol J 21:1123–1128
Haylen BT, Kerr S, Naidoo S et al (2015) Posterior vaginal compartment repairs: where are the main anatomical defects? Neurourol Urodyn 34:S130–S131, Int Urogynecol J doi:10.1007/s00192-015-2874-7
Haylen BT, Avery D, Chiu T et al (2014) Posterior repair quantification (PR-Q) using key anatomical indicators (KAI). Int Urogynecol J 25(12):1665–1772, Neurourol Urodyn 2014;33:900–1
Haylen BT, Younis M, Naidoo S et al (2015) Perineorrhaphy quantitative assessment. Int Urogynecol J 26:539–544
Swenson CW, Simmen AM, Berger MB et al (2015) The long and short of it: anterior vaginal wall length before and after anterior repair. Int Urogynecol J 26:1035–1039
Acknowledgments
The assistance of Prof Steven Swift is gratefully acknowledged for the Simplified POP-Q section and other helpful input. Prof John DeLancey also contributed helpful input to “Prolapse quantification” and the Appendix. We thank our invited external reviewers Prof Steven Swift, Prof Mark Vierhout, Prof Michele Meschia, Prof Doug Tincello and Prof Don Wilson for their constructive contributions. We also thank those who submitted constructive comments following IUGA and ICS website presentation of Version 12: Dr Kiran Ashok, Prof Phil Toozs-Hobson, Dr Kamil Svabik. Further helpful comments were received at an open forum at ICS Montreal from Beth Shelly, Julia Herbert, Kari Bo and Joe Lee. The talents of medical illustrator, Levent Efe were crucial to the development of this document levent@leventefe.com.au.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
BT Haylen: No disclosures.
CF Maher: No disclosures.
MD Barber: No disclosures.
SFM Camargo: No disclosures.
V Dandolu: Research grant–Allegan, Consultant-Pfizer; A Digesu: Honorarium for lectures or sponsorship to cover travel expenses at Meetings from: Astellas, Pfizer, Allergan, AMS, Medtronic, Uroplasty.
HB Goldman: Consultant – Allergan, Medtronic, Uroplasty; Speaker – Astellas, Allergan, Medtronic, Uroplasty.
M Huser: No disclosures.
AL Milani: No disclosures.
PA Moran: Speaker & consultant: Astellas and Ethicon Women’s Health and Urology. Consultant: Boston Scientific.
GN Schaer: Advisor (in Switzerland) for Astellas, Novartis, Pfizer.
MIJ Withagen: Research Grant 2010–Ethicon Women’s Health & Urology.
Additional information
International Urogynecology Journal, Vol. 27, No. 2, 2016. Copyright 2016. This material is reproduced with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc., and the International Urogynecological Association.
This document is being published simultaneously in Neurourology and Urodynamics (NAU) and the International Urogynecology Journal (IUJ), the respective journals of the sponsoring organizations, the International Continence Society (ICS) and the International Urogynecological Association (IUGA) in the February 2016 issue of each journal.
Standardization and Terminology Committees IUGA - Bernard T. Haylen, Christopher F. Maher, Paul A. Moran, Gabriel. N. Schaer
Joint IUGA / ICS Working Group on Female POP Terminology - Bernard T. Haylen, Christopher F. Maher, Matthew D. Barber, Sérgio Camargo, Vani Dandolu, Alex Digesu, Howard B. Goldman, Martin Huser, Alfredo L. Milani, Paul A. Moran, Gabriel. N. Schaer, Mariëlla I. J. Withagen.
Published online in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/nau.22922.
Appendix - Concepts and available measurements awaiting further validation
Appendix - Concepts and available measurements awaiting further validation
A: Subdivision of Stage II POP-Q:
An optional subdivision of Stage II into IIa (−1 to hymen) and IIb (hymen to +1) was considered at length. Stage IIA would then be defined as −1 to 0 (so the hymen, that is 0, is included in stage IIA) and stage IIB (>0 to +1), meaning the dependent part of prolapse beyond the hymen but no further than +1. It was felt that this might reflect a clinical difference between the two subdivisions in terms of symptoms. That change was not made at this time in part to maintain the current strictly anatomical definition of the “sign of POP”.
B: Vaginal Anatomical Levels and Lengths:
-
(i)
Level I: Uterine cervix (if present) and/or upper 2.5 cm of vagina. Footnote Footnote 18
-
(ii)
Level II: Mid-vagina from distal end of Level I to hymen. Footnote 19
-
(iii)
Level III – Vaginal vestibule: Vaginal entrance (Latin: “vestibulum” = “a space at the entrance of a canal”) from hymenal ring to just below the clitoris anteriorly (anterior vestibule), labia minora laterally and anterior perineum posteriorly (posterior margin of vestibule) (Fig. 39)Footnote 20
Fig. 39 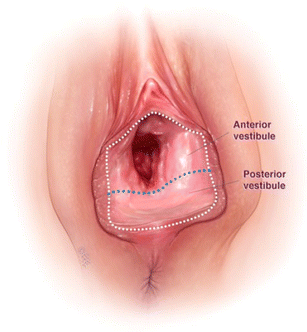
Anterior and posterior vestibule
-
(iv)
Posterior vestibule:Posterior hymenal ring to anterior perineum (posterior margin of vestibule) (Fig. 40)Footnote 21
-
(v)
Total vaginal length [4]: Posterior vaginal vault to hymen (cm), i.e., Levels I and II posteriorly.
-
(vi)
Total posterior vaginal length [52–54]: Posterior vaginal vault to posterior margin of vestibule (anterior perineum - cm), i.e., Levels I, II and III posteriorly.
-
(vii)
Anterior vaginal length: Anterior hymenal ring to the anterior vaginal vault (anterior cervicovaginal junction or anterior cuff post-hysterectomy) [55] (Fig. 41).


Posterior vestibule

Vaginal Levels (I to III) and Vaginal lengths (Anterior, Total, Total Posterior)
C: Additional available intraoperative measurements.
-
(i)
Perineal measurements:
-
(a,b)
Perineorrhaphy Width (PW) and Depth (PD) [54]: Width and depth of the excised perineum (Fig. 42)
Fig. 42 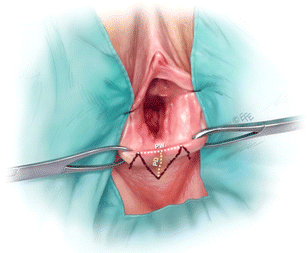
Perineorrhaphy width (PW) and perineorrhaphy depth (PD)
-
(c)
Perineal length (PL) [54]: Distance from posterior margin of vestibule to anterior anal verge (Fig. 43).
Fig. 43 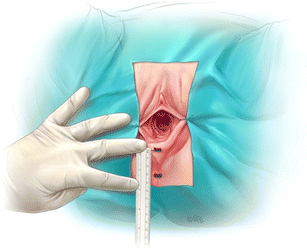
Perineal length
-
(d)
Mid-perineal thickness (MPT) [54]: Thickness (cm) of the mid-perineum in the midline (Fig. 44).
Fig. 44 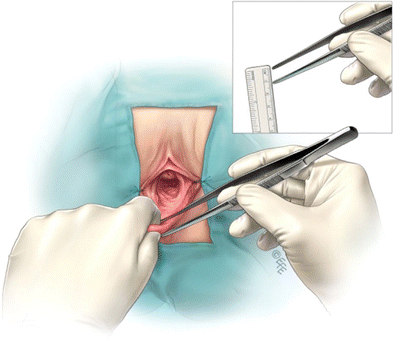
Mid-perineal thickness
-
(e)
Perineal Gap (PG) [52–54]: Thinned out medial area (cm) between Moynihan forceps placed bilaterally where the labia minora meet the perineum (Fig. 45).
Fig. 45 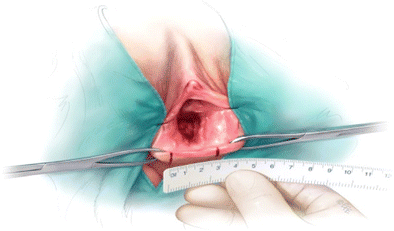
Perineal Gap
-
(f)
Perineorrhaphy Commencement Position (PCP): NEW Where in Level III, the perineorrhaphy is commenced, e.g., hymen, mid- vestibule, posterior margin of vestibule.
-
(a,b)
-
(ii)
Posterior vaginal measurements [53]:
-
(a)
Posterior Vaginal Vault Descent (PVVD [52, 53]: Descent of the posterior vaginal vault towards the perineal gap obtained by subtracting the inferiorly displaced vaginal vault and the anterior perineum (second figure) from the total posterior vaginal length (TPVL - first figure – posterior vaginal vault to anterior perineum). (Fig. 46 and Fig. 47)
-
(b)
Mid-Vaginal Laxity (MVL) (Undisplaced) [52, 53]: Laxity of the vaginal mucosa (anterior traction) midpoint in the vagina super- posteriorly and in the midline with the vaginal vault held in an undisplaced position (similar to that after vault fixation) (Fig. 48)
Fig. 46 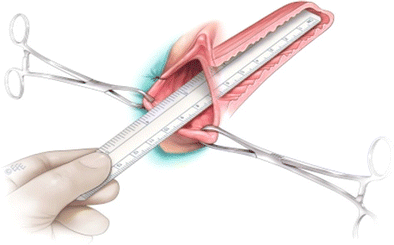
(left): Total posterior vaginal length (TPVL)
Fig. 47 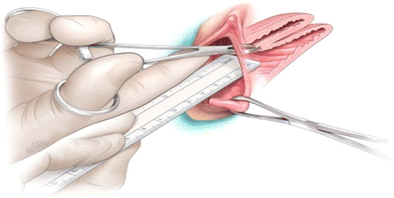
(right): Distance from vaginal vault (on traction) to anterior perineum. Posterior vaginal vault descent is the subtraction of this measurement from the TPVL
-
(c)
Recto-vaginal Fascial Laxity (RVFL) [52, 53]: Laxity of the rectovaginal fascia (anterior traction) midpoint in the vagina super- posteriorly (mucosa opened) and in the midline with the vaginal vault held in an undisplaced position (Figs. 49)
Fig. 48 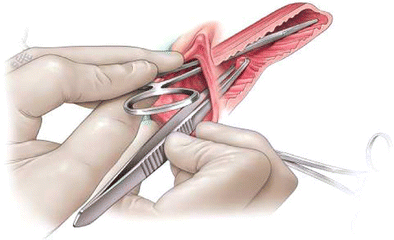
(left): Mid-vaginal laxity (vault undisplaced)
Fig. 49 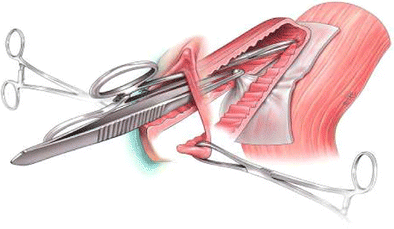
(right): Recto-vaginal fascial laxity
-
(a)








Rights and permissions
About this article

Cite this article
Haylen, B.T., Maher, C.F., Barber, M.D. et al. An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP). Int Urogynecol J 27, 165–194 (2016). https://doi.org/10.1007/s00192-015-2932-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-015-2932-1