
Abstract
Purpose
To characterize incidence of low, normal and “supranormal” central venous oxygen saturation (ScvO2) and the relation to markers of tissue hypoxia, course and outcome in cardiac surgery patients.
Methods
Prospective, observational study in a university multidisciplinary 50-bed intensive care unit including 205 consecutive patients undergoing elective cardiac surgery. Data were split into training and test data sets and subjected to 50 replications of fivefold cross-validation to estimate lower and upper bounds of ScvO2 indicative of impaired tissue oxygenation.
Results
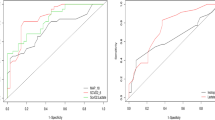
Both low (≤60.8%) and supranormal (≥77.4%) ScvO2 were associated with an unfavorable course, while the logistic EuroSCORE for risk adjustment was comparable between groups. Incidences of abnormal ScvO2 were 13.2% low and 30.7% supranormal. Patients with low ScvO2 and an uneventful course initially presented with normal lactate levels, whereas patients with supranormal ScvO2 displayed consistently higher serum lactate levels. High ScvO2 values were associated with the use of β-mimetics and signs of systemic inflammation. Mortality rates were comparable for patient populations presenting either low (14.8%) or supranormal ScvO2 (7.9%) and higher than normals (0%, p < 0.001). Lactate was comparably increased in patients that ultimately died, irrespective whether they had low or supranormal ScvO2 values. In contrast, neither low nor supranormal ScvO2 was associated with altered gastric pCO2.
Conclusions
High ScvO2 is an under-recognized warning sign for impaired tissue oxygenation in the peri-operative period. Including values ≥77.4% as ‘normal’ impaired performance of ScvO2 monitoring to predict a complicated perioperative course.




Similar content being viewed by others


Abbreviations
- aiDCO2 :
-
Arterio-intestinal pCO2-gradient
- AUC:
-
Area under the curve
- CABG:
-
Coronary artery bypass graft
- DO2 :
-
Oxygen delivery
- pCO2 :
-
Partial pressure of carbon dioxide
- SAPS II:
-
Simplified Acute Physiology Score II
- ScvO2 :
-
Central venous oxygen saturation
- SaO2 :
-
Arterial oxygen saturation
- SIRS:
-
Systemic inflammatory response syndrome
- SOFA:
-
Sepsis-related Organ Failure Assessment
- VO2 :
-
Oxygen uptake
References
Ander DS, Jaggi M, Rivers E, Rady My, Levine TB, Barry Levine AB, Masura J, Gryzbowski M (1998) Undetected cardiogenic shock in patients with congestive heart failure presenting to the emergency department. Am J Cardiol 82:888–891
Rady MY, Rivers EP, Nowak RM (1996) Resuscitation of the critically ill in the ED: responses of blood pressure, heart rate, shock index, central venous oxygen saturation, and lactate. Am J Emerg Med 14:218–225
Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M (2001) Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 345:1368–1377
Kortgen A, Niederprüm P, Bauer M (2006) Implementation of an evidence-based “standard operating procedure” and outcome in septic shock. Crit Care Med 34:943–949
Reinhart K, Rudolph T, Bredle DL, Hannemann L, Cain SM (1989) Comparison of central-venous to mixed-venous oxygen saturation during changes in oxygen supply/demand. Chest 95:1216–1221
Ladakis C, Myrianthefs P, Karabinis A, Karatzas G, Dosios D, Fildissis G, Gogas J, Baltopoulos G (2001) Central venous and mixed venous oxygen saturation in critically ill patients. Respiration 68:279–285
Chawla LS, Zia H, Gutierrez G, Katz NM, Seneff MG, Shah M (2004) Lack of equivalence between central and mixed venous oxygen saturation. Chest 126:1891–1896
Bellomo R, Reade MC, Warrillow SJ (2008) The pursuit of a high central venous oxygen saturation in sepsis: growing concerns. Crit Care 12:130
Bracht H, Hänggi M, Jeker B, Wegmüller N, Porta F, Tüller D, Takala J, Jakob SM (2007) Incidence of low central venous oxygen saturation during unplanned admission in a multidisciplinary intensive care unit: an observational study. Crit Care 11:R2
Hochman JS (2003) Cardiogenic shock complicating acute myocardial infarction. Expanding the paradigm. Circulation 107:2998–3002
Tomic V, Russwurm S, Möller E, Claus RA, Blaess M, Brunkhorst F, Bruegel M, Bode K, Bloos F, Wippermann J, Wahlers T, Deigner HP, Thiery J, Reinhart K, Bauer M (2005) Transcriptomic and proteomic patterns of systemic inflammation in on-pump and off-pump coronary artery bypass grafting. Circulation 112:2912–2920
Steckel JH (1993) Cross validating regression models in marketing research. Mark Sci 12:412–427
Maillet JM, Le Besnerais P, Cantoni M, Nataf P, Ruffenach A, Lessana A, Brodaty D (2003) Frequency risk factors and outcome of hyperlactatatemia after cardiac surgery. Chest 123:1361–1366
Pölönen P, Ruokonen E, Hippeläinen M, Pöyhönen M, Takala J (2000) A prospective, randomized study of goal–oriented hemodynamic therapy in cardiac surgical patients. Anesth Analg 90:1052–1059
Smith I, Kumar P, Molloy S, Rhodes A, Newman PJ, Grounds RM, Bennet ED (2001) Base excess and lactate as a prognostic indicators for patients admitted to intensive care. Intensive Care Med 27:74–83
Kavarana MN, Frumento RJ, Hirsch AL, Oz MC, Lee DC, Bennet-Guerrero E (2003) Gastric hypercarbia and adverse outcome after cardiac surgery. Intensive Care Med 29:742–748
Bams JL, Mariani MA, Groeneveld AB (1999) Predicting outcome after cardiac surgery comparison of global hemodynamic and tonometric variables. Br J Anaesth 82:33–37
Lebuffe G, Decoene C, Pol A, Prat A, Vallet B (1999) Regional capnometry with air-automated tonometry detects circulatory failure earlier than conventional hemodynamics after cardiac surgery. Anesth Analg 89:1084–1090
Hameed SM, Cohn SM (2003) Gastric tonometry. The role of mucosal pH measurement in the management of trauma. Chest 123:475S–481S
Hamilton MA, Mythen MG (2001) Gastric tonometry: were do we stand? Curr Opin Crit Care 7:122–127
Bakker J (2001) Lactate: may I have your votes please. Intensive Care Med 27:6–11
Antonelli M, Levy M, Andrews PJD, Chastre J, Hudson LD, Manthous C, Meduri GU, Moreno RP, Putensen C, Stewart T, Torres A (2007) Hemodynamic monitoring in shock and implications for management. International consensus conference, Paris, France, 27–28. April 2006. Intensive Care Med 33:575–590
Pearse R, Dawson D, Fawcett J, Rhodes A, Grounds RM, Bennnet ED (2005) Changes in central venous saturation after major surgery, and association with outcome. Crit Care 9:694–699
Ince C, Sinaasappel M (1999) Microcirculatory oxygenation and shunting in sepsis and shock. Crit Care Med 27:1369–1377
Crouser ED (2004) Mitochondrial dysfunction in septic shock and multiple organ dysfunction syndrome. Mitochondrion 4:729–741
Burns AM, Keogan M, Donaldson M, Brown DL, Park GR (1997) Effects of inotropes on human leucocyte numbers, neutrophil function and lymphocyte subtypes. Br J Anaesth 78:530–535
Levy B (2006) Lactate and the shock state: the metabolic view. Curr Opin Crit Care 12:315–321
Hatherill M, Salie S, Waggie Z, Lawrenson J, Hewitson J, Reynolds L, Argent A (2007) The lactate: pyruvate ratio following open cardiac surgery in children. Intensive Care Med 33:822–829
Thackray S, Easthaugh J, Freemantle N, Cleland JG (2002) The effectiveness and relative effectiveness of intravenous inotropic drugs acting through the adrenergic pathway in patients with heart failure—a meta—regression analysis. Eur J Heart Fail 4:515–529
Follath F, Cleland JG, Just H, Papp JG, Scholz H, Peuhkurinen K, Harjola VP, Mitrovic V, Abdalla M, Sandell EP, Lehtonen L (2002) Efficacy and safety of intravenous levosimendan compared with dobutamine in severe low-output heart failure (the LIDO study): a randomised double-blind trial. Lancet 360:196–202
Fellahi JL, Parienti JJ, Hanouz JL, Plaud B, Riou B, Ouattara A (2008) Perioperative use of dobutamine in cardiac surgery and adverse cardiac outcome: propensity-adjusted analyses. Anesthesiology 108:979–987
Author information
Authors and Affiliations
Corresponding author
Additional information
The study was performed at the Department of Anesthesiology and Critical Care Therapy, Jena University Hospital, Jena, Germany.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Perz, S., Uhlig, T., Kohl, M. et al. Low and “supranormal” central venous oxygen saturation and markers of tissue hypoxia in cardiac surgery patients: a prospective observational study. Intensive Care Med 37, 52–59 (2011). https://doi.org/10.1007/s00134-010-1980-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-010-1980-8