
Abstract
Objective
To study the acid–base effects of crystalloid strong ion difference (SID) during haemodilution.
Design
Prospective in vivo study.
Setting
University laboratory.
Subjects
Anaesthetised, mechanically ventilated Sprague-Dawley rats.
Interventions
Rats were studied in seven groups of three. Each group underwent normovolaemic haemodilution with one of seven crystalloids, with SID values from 0 to 40 mEq/l. Six exchanges of 9 ml crystalloid for 3 ml blood were performed.
Measurements and main results
[Hb] fell from 142±17 to 44±10 g/l (p<0.0001). Final plasma [lactate] was 1.1±0.6 mmol/l. Final standard base excess values ranged from −8 to +7 mmol/l, and were directly correlated with crystalloid SID (R2=0.91). By linear regression, the SID of a crystalloid balanced to maintain standard base excess=0 mmol/l was 23.7 mEq/l. Dilutions 2–5 produced similar results.
Conclusions
There is a linear relationship between crystalloid SID and post-dilutional metabolic acid–base status. The SID of a crystalloid balanced for normovolaemic haemodilution is 24 mEq/l. These principles are applicable in designing fluids for volume resuscitation, acute normovolaemic haemodilution and cardio-pulmonary bypass.
Similar content being viewed by others

Introduction
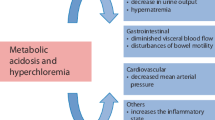
Large volumes of intravenous saline tend to cause a metabolic acidosis [1, 2, 3]. Although there is limited information on how much harm can result, the acidosis is regarded as an undesirable side effect [4]. Misinterpretation is an obvious concern. For example, a new or persistent metabolic acidosis during fluid resuscitation might be attributed to unresolved tissue hypoxia. Such an error could lead to excessive fluid loading, or even an unnecessary laparotomy [5].
More specific adverse effects have also been implicated. Human volunteers given 50 ml/kg normal saline over 1 h experienced mental changes, abdominal discomfort and relative oliguria, but not when the same volume of Hartmann’s solution was administered [6]. There is also a possible association with post-operative bleeding [7], and an increased gastric CO2 gap [8].In one animal model, hyperchloraemia reduced renal blood flow and glomerular filtration rate [9]; in another, acidosis due to HCl infusion caused NO production, hypotension and acute lung injury [10].
It may therefore be preferable to administer crystalloids balanced to avoid acid–base disturbances [11].The challenge has been to find a logical basis for their design. In our view, Stewart’s physical chemical analysis of acid–base provides such a framework [12, 13]. In the Stewart analysis, there are three independent variables determining acid–base balance—PCO2, ATOT and strong ion difference (SID). PCO2 in arterial blood is an equilibrium value set by alveolar ventilation and CO2 production. ATOT is the concentration of non-volatile weak acid. In plasma, ATOT largely derives from albumin and to a lesser extent inorganic phosphate [14]. Raising and lowering ATOT while holding SID constant cause a metabolic acidosis and alkalosis. respectively [12, 15].
Strong ions are chemical entities whose non-ionised concentrations are quantitatively unimportant under all biological acid–base conditions. Examples include Na+, K+, Cl− and lactate. In body fluids, total strong cation concentrations exceed strong anion concentrations. The surfeit is quantified by SID, which in normal plasma is approximately 42 mEq/l. Lowering and raising plasma SID while clamping ATOT cause a metabolic acidosis and alkalosis, respectively.
Fluids for intravenous administration can also be described in Stewart’s physical chemical terms, since they are administered into the same physiological milieu. No pure crystalloid contains ATOT, so that intravenous administration dilutes plasma ATOT. Saline has a zero SID, since Na+ and Cl− are present in equivalent concentrations. The SID of water, dextrose solutions and mannitol is also zero, since these fluids contain no strong ions. Infusion of large volumes of zero SID fluids will thus reduce plasma SID by admixture and equilibration, pushing acid–base balance towards metabolic acidosis [16, 17]. Importantly, although this type of acidosis is commonly hyperchloraemic, the acidosis can also occur with a reduction in plasma Cl-, depending on the fluid employed [18].
In the Stewart paradigm, crystalloid fluid loading brings about acid–base changes in two ways. ATOT is invariably lowered by dilution, which in isolation causes a metabolic alkalosis. Simultaneously plasma SID is altered towards that of the infused fluid [19]. Depending on the composition of the crystalloid, plasma SID can thus be raised (e.g. with sodium bicarbonate infusion), lowered or left unaltered. The end result represents the final plasma SID balanced against the metabolic alkalosis of ATOT dilution. It follows that saline preparations cause a metabolic acidosis only because SID reduction predominates. The SID of a properly balanced crystalloid must generate a fall in plasma SID which precisely counteracts the (ATOT) dilution alkalosis.
We have shown that crystalloids with SID <24 mEq/l cause a metabolic acidosis on in vitro haemodilution, whereas those with SID >24 mEq/l cause a metabolic alkalosis [20]. The SID of a crystalloid balanced for in vitro haemodilution is thus 24 mEq/l; however, additional investigation is required before in vivo extrapolation, since there are some important differences. In both situations, infused strong ions and water are distributed between plasma and erythrocytes, the final ionic concentrations satisfying Gibbs-Donnan equilibria and the laws of electroneutrality and of chemical equilibrium. In both scenarios plasma ATOT is reduced by dilution, but the in vivo spread of infused water and strong ions extends into the interstitial space, where ATOT is negligible [12]. Whether this influences the SID necessary for crystalloid balance is unclear.
We therefore developed an animal model of acute normovolaemic haemodilution to investigate the in vivo acid–base effects of crystalloids with a wide range of SID values.
Materials and methods
The protocol was approved by the Animal Experimentation Committee of the University of Queensland. The principles of laboratory animal care met the standards of the National Institutes of Health as well as those of the National Health and Medical Research Council of Australia.
Progressive normovolaemic haemodilution of mechanically ventilated rats was performed using seven crystalloid solutions with SID values ranging from 0 to 40 mEq/l (Table 1). Solutions were prepared fresh by admixture of 0.9% saline, 0.45% saline (Baxter Healthcare, Sydney, Australia) and 8.4% sodium bicarbonate (Astra Pharmaceuticals, Sydney, Australia) in proportions calculated to produce the electrolyte concentrations set out in Table 1.
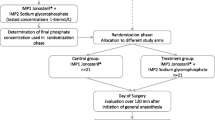
After a water-only overnight fast, male Sprague-Dawley rats (250–500 gm) from the Central Animal Breeding House of the University of Queensland were anaesthetised with sodium pentobarbitone 60 mg/kg IP and ventilated via a tracheostomy with air/oxygen and isoflurane using a Harvard Rodent Ventilator (Model 683, Southnatick, Mass). Heat loss was reduced by positioning the animals on a warming pad under reflecting metal foil. A 20-G cannula was placed in the common carotid artery for continuous monitoring of arterial blood pressure and for serial blood withdrawal and replacement.
Blood pressure was measured using a transducer (Model 43–212, Baxter Healthcare Corporation, Irvine, Calif.) zeroed to the mid-axillary line with output displayed on a portable monitor (Model 1275A, Hewlett Packard, Waltham, Mass.). The inspired isoflurane concentration was set to maintain a mean arterial pressure of approximately 100 mm Hg. Minute ventilation was adjusted until the arterial PCO2 was in the range 30–50 mm Hg, as determined by blood gas analysis (ABL 620, Radiometer, Copenhagen, Denmark).
Rats were divided into seven groups of three. Each group was allocated one of the seven prepared crystalloids. In each animal the allocated crystalloid was infused into the carotid artery at 3 ml/h throughout the experiment. After stability had been achieved, normovolaemic haemodilution was commenced. The technique consisted of withdrawing 3 ml of arterial blood over approximately 20 s, and replacing it with 9 ml crystalloid over the following 20 s. This process was repeated once every 10 min for a total of six exchanges. The first 0.5 ml of each withdrawal (after clearing the dead-space) was aspirated into a heparin-coated syringe, which was placed on ice. The remaining 2.5 ml of each aspirate was simply discarded. When the mean arterial pressure fell below 80 mm Hg between withdrawals, further crystalloid boluses of 0.5–1 ml were injected. Ten minutes following the sixth withdrawal, a final 0.5-ml specimen of arterial blood was collected.
The animals were then killed by cardiotomy while still under anaesthesia.
Data collection
All arterial blood specimens were subjected to blood gas analysis at 37°C, and on the final specimen plasma [lactate] was also measured and recorded (ABL725, Radiometer, Copenhagen, Denmark).
Calculations
To quantify metabolic acid–base status in vivo we used the modification of base excess known as standard base excess (SBE), which reflects the acid–base status of the total extracellular space [21]. The SBE values were calculated by substituting plasma pH, blood PCO2 and a haemoglobin concentration of 50 g/l in the Van Slyke equation [22].
Data analysis
After each dilution, the relationship between crystalloid SID and SBE was determined by linear regression, whereupon crystalloid SID was solved for SBE=0 mmol/l.
The mean haemoglobin concentrations ([Hb]) for all 21 animals as one group were compared pre and post-dilution by paired Student’s t test, after confirmation of normal distribution. Significance for this test was accepted at p=0.05. Unless otherwise specified, data are presented as mean±SD.
Results
Mean SBE before haemodilution was –1.5±1.9 mmol/l. After the sixth and final dilution, [Hb] had fallen from 142±17 to 44±10 g/l (p<0.0001). Final arterial [lactate] was 1.1±0.6 mmol/l. From the second dilution on, crystalloid SID was directly correlated with SBE values (R2=0.53, 0.67, 0.82, 0.86 and 0.91 for dilutions 2–6, respectively; see Fig. 2). After dilution 6, final SBE values ranged from –8 to +7 mmol/l (Fig. 1). By linear regression it was determined that a crystalloid SID of 23.7 mEq/l maintains a post-dilutional SBE of 0 mmol/l (Fig. 1). The SBE=0 “balance points” were similar for dilutions 2–5 (Fig. 2).

Relationship between crystalloid strong ion difference (SID) and final standard base excess (SBE) after dilution 6. The regression line demonstrates the inverse correlation (R2=0.91). Note the “balance point” (SBE=0) of 23.7 mEq/l

Regression lines of SBE vs crystalloid SID for the second through sixth haemodilutions. R2=0.55, 0.68, 0.82, 0.86 and 0.91, respectively. The progressive increase in slopes represent escalating acid–base effects, but “balance points” (SBE=0) are consistently near 24 mEq/l. For clarity, individual data points are omitted
Discussion
The in vivo results reported here strongly support our previous in vitro findings [20]. Crystalloids balanced for acute haemodilution require a SID of 24 mEq/l. Crystalloids in which SID >24 mEq/l cause a metabolic alkalosis, and those with SID <24 mEq/l a metabolic acidosis. The acid–base characteristics of rat blood resemble human blood sufficiently to make an extrapolation to human subjects. Baseline plasma electrolytes (and thus SID), pH and PaCO2 are virtually the same [23, 24]. Rat whole blood [Hb] values are similar to human at around 156 g/l [25], and intravascular to interstitial volumetric relationships are also similar. This means that the human algorithm for standard base excess (based on a mean extracellular [Hb] of 50 g/l) should also quantify rat metabolic acid–base status.
One way to test these results is to consider the severest example of haemodilution possible, which is complete replacement of extracellular fluid with crystalloid. Plasma SID then becomes the SID of the diluting crystalloid. It is important to remember that SID defines an electrical space filled by weak ions to maintain electrical neutrality. In the SID space of normal plasma, the only quantitatively important weak ions are HCO3 − and A− (anions of the non-volatile weak acids HA, where ATOT=[A-]+[HA]). A− and HCO3 − are known collectively as the buffer base anions [14, 21]; thus, SID dictates the buffer base concentration ([A]+[HCO3 −]) by forming its boundaries.
After complete replacement by crystalloid, the A− component of plasma buffer base disappears. HCO3 − now occupies the entire SID space; thus, crystalloid SID=plasma SID=plasma [HCO3 −]. Under these conditions there are no erythrocytes to initiate Cl− and HCO3 − exchange; thus, plasma [HCO3 −] is totally independent of PCO2. If normal metabolic acid–base status is to be achieved, this fixed value of plasma [HCO3 −] must generate a pH of 7.4 when PaCO2=40 mm Hg. Such criteria automatically define plasma [HCO3 −] as 24.4 mmol/l. Consequently, for the most extreme haemodilution possible, the SID of a balanced crystalloid must be 24.4 mEq/l. This value is in accordance with our experimental findings.
The more practical question is whether the same applies across a wide range of finite haemodilutions, where red cells are still present, where plasma differs from interstitial fluid and where plasma ATOT and thus [A-] remain quantitatively important. Our in vivo data provide strong confirmation, since from the second through final dilutional steps the “balance” points were consistently close to 24 mEq/l (Fig. 2); thus, the SID of a balanced crystalloid is 24 mEq/l, for all degrees of dilution ranging from mild to extreme. It is noteworthy that these findings apply only to crystalloids designed for haemodilution scenarios, e.g. cardiopulmonary bypass, acute normovolaemic haemodilution or correction of hypovolemia. They do not apply when designing fluids for renal replacement, where changes in ATOT are minimal.
To increase the SID of a fluid such as saline above zero, it is necessary to replace some Cl− ions with HCO3 −; however, HCO3 − in aqueous solution is in equilibrium with dissolved CO2, a highly diffusible gas. As a result, HCO3 − solutions are unstable if stored in permeable plastic, due to atmospheric CO2 loss. Such fluids must be stored in glass and infused promptly. This is why commercial balanced salt solutions contain organic anions such as lactate, acetate, gluconate and citrate as stable surrogates for HCO3 − (Table 2). Although these are actually strong ions with pKa values more than 2 units below physiological pH, they are metabolized following infusion. Provided their metabolic clearance is rapid, organic anions removed in this way can be regarded as weak ions.
The in vivo or “effective” SID of such fluids can be calculated from the component which is subject to metabolic “disappearance”. Taking Hartmann’s solution as an example, the total [lactate] is 29 mmol/l (Table 2). If the baseline plasma [lactate] remains at 2 mmol/l during infusion, the effective SID of Hartmann’s solution is 27 mEq/l. For years this crystalloid has contained only the L isomer (B. Houghton, pers. commun.), which can be metabolized at rates of 100 mmol/h or more by oxidation or gluconeogenesis [26, 27]; thus, only with rapid infusion coupled with marked impairment of lactate metabolism, e.g. in severe liver dysfunction, is the effective SID of Hartmann’s solution likely to be reduced.
Based on these calculations, a balanced SID of 24 mEq/l is slightly less than the effective SID of Hartmann’s solution. Dr. Hartmann himself considered his modification of Ringer’s injection “alkalinising” rather than neutral [28]. Judging by our findings, a mild alkalinizing effect does seem likely, although all that available evidence shows is that Hartmann’s solution reduces or eliminates infusion-related metabolic acidosis [2, 29]. It is noteworthy that in two experimental models of hemorrhagic shock, Ringer’s lactate outperformed saline in morbidity and survival [29, 30]. It remains to be established whether this translates into better outcomes in clinical practice.
The acid–base balance at the onset of resuscitation is relevant. If there is no metabolic acid–base disturbance prior to fluid loading (SBE close to zero), our findings indicate that fluids with a higher effective SID (e.g. Plasma-Lyte 148, effective SID=50 mEq/l; Table 2) are likely to cause a progressive metabolic alkalosis from the outset. Confirmatory published data are limited, but if Plasma-Lyte 148 is used to prime cardiopulmonary bypass circuits, arterial base excess increases by the end of bypass [31]. On the other hand, if there is a pre-existing metabolic acidosis, due to hypovolaemic shock, for example, higher SID crystalloids should correct the acidosis more rapidly, and counteract ongoing generation of acidosis more effectively. Even so, there is always the potential for over-correction and “break-through” metabolic alkalosis.
Similarly, a crystalloid SID <24 mEq/l more rapidly corrects a pre-existing metabolic alkalosis, with the corresponding caveat of “break-through” metabolic acidosis. On first consideration this may seem relevant in critical illness, where ATOT tends to be decreased due to hypoalbuminaemia. Such a “primary hypoproteinaemic alkalosis” [32] is a potential argument for reducing the SID of resuscitation fluids below 24 mEq/l; however, the lower ATOT tends to be matched by a reduced SID due to increased plasma chloride [33], offsetting any metabolic alkalosis. A similar endogenous increase in plasma chloride has been noted in experimental resuscitated endotoxaemia [34]; hence, from an acid–base perspective, the argument for lower SID resuscitation fluids in critical illness and sepsis is not compelling.
We conclude that the previously demonstrated in vitro linear relationship between crystalloid SID and post-dilutional metabolic acid–base status also applies in vivo, the balanced crystalloid SID being 24 mEq/l. These principles are applicable in designing fluids for volume resuscitation, acute normovolaemic haemodilution and cardio-pulmonary bypass.
References
Scheingraber S, Rehm M, Sehmisch C, Finsterer U (1999) Rapid saline infusion produces hyperchloremic acidosis in patients undergoing gynecologic surgery. Anesthesiology 90:1265–1270
McFarlane C, Lee A (1994) A comparison of Plasmalyte 148 and 0.9% saline for intra-operative fluid replacement. Anaesthesia 49:779–781
Prough DS, Bidani A (1999) Hyperchloremic metabolic acidosis is a predictable consequence of intraoperative infusion of 0.9% saline. Anesthesiology 90:1247–1249
Mythen MG, Hamilton M, Grocott M (2002) Fluid management in gastrointestinal surgery. In: Gullo A (ed) APICE 16. Critical care medicine. Springer, Berlin Heidelberg New York, pp 655–670
Parekh N (2002) Hyperchloremic acidosis. Anesth Analg 95:1821–1822
Williams EL, Hildebrand KL, McCormick SA, Bedel MJ (1999) The effect of intravenous lactated Ringer’s solution versus 0.9% sodium chloride solution on serum osmolality in human volunteers. Anesth Analg 88:999–1003
Waters JH, Gottlieb A, Schoenwald P, Popovich MJ, Sprung J, Nelson DR (2001) Normal saline versus lactated Ringer’s solution for intraoperative fluid management in patients undergoing abdominal aortic aneurysm repair: an outcome study. Anesth Analg 93:817–822
Wilkes NJ, Woolf R, Mutch M, Mallet SV, Peachey T, Stephens R, Mythen MG (2001) The effects of balanced versus saline-based Hetastarch and crystalloid solutions on acid–base and electrolyte status and gastric mucosal perfusion in elderly surgical patients. Anesth Analg 93:811–816
Wilcox CS (1983) Regulation of renal blood flow by plasma chloride J Clin Invest 71:726–735
Pedoto A, Caruso JE, Nandi J, Oler A, Hoffman SP, Tassiopoulis AK, McGraw DJ, Camporesi EM, Hakim TS (1999) Acidosis stimulates nitric oxide production and lung damage in rats. Am J Respir Crit Care Med 159:397–402
Dorje P, Adhikary G, Tempe DK (2000) Avoiding iatrogenic hyperchloremic acidosis: call for a new crystalloid fluid. Anesthesiology 92:626
Stewart PA (1981) How to understand acid–base. In: Stewart PA (ed) A quantitative acid–base primer for biology and medicine. Elsevier, New York, pp 1–286
Stewart PA (1983) Modern quantitative acid–base chemistry. Can J Physiol Pharmacol 61:1444–1461
Schlichtig R, Grogono AW, Severinghaus JW (1998) Current status of acid–base quantitation in physiology and medicine. Anesthesiol Clin North Am 16:211–233
Rossing TH, Maffeo N, Fencl V (1986) Acid–base effects of altering plasma protein concentration in human blood in vitro. J Appl Physiol 61:2260–2265
Miller LR, Waters JH (1997) Mechanism of hyperchloremic nonanion gap acidosis. Anesthesiology 87:1009–1010
Storey DA (1999) Intravenous fluid administration and controversies in acid–base. Crit Care Resusit 1:151–156
Makoff DL, Silva JA da, Rosenbaum BJ, Levy SE, Maxwell MH (1970) Hypertonic expansion: acid–base and electrolyte changes. Am J Physiol 218:1201–1207
LeBlanc M, Kellum J (1998) Biochemical and biophysical principles of hydrogen ion regulation. In: Ronco C, Bellomo R (eds) Critical care nephrology. Kluwer, Dordrecht, pp 261–277
Morgan TJ, Venkatesh B, Hall J (2002) Crystalloid strong ion difference determines metabolic acid–base change during in vitro haemodilution. Crit Care Med 30:157–160
Siggaard-Andersen O, Fogh-Andersen N (1995) Base excess or buffer base (strong ion difference) as measure of a non-respiratory acid–base disturbance. Acta Anesth Scand (Suppl 107):123–128
Siggaard-Andersen O (1977) The Van Slyke equation. Scand J Clin Lab Invest 37 (Suppl 146):15–20
Ringler DH, Dabich L (1979) Hematology and clinical biochemistry. In: Baker HJ, Lindsey JR, Weisbroth SH (ed) The laboratory rat, vol 1. Academic Press, Harcourt Brace Jovanovich, New York, pp105–121
Decaux G, Crenier L, Namias B, Gervy C, Soupart A (1994) Normal acid–base equilibrium in acute hyponatremia and mixed alkalosis in chronic hyponatremia induced by arginine vasopressin or 1-deamino-8-D-arginine vasopressin in rats. J Lab Clin Med 123:892–893
Baker HJ, Lindsey R, Weisbroth SH (1979) Selected normative data. In: Baker HJ, Lindsey JR, Weisbroth SH (ed) The laboratory rat, vol 1. Academic Press, Harcourt Brace Jovanovich, New York, pp 411–412
McLean AG, Davenport A, Cox D, Sweny P (2000) Effects of lactate-buffered and lactate-free dialysate in CAVHD patients with and without liver dysfunction. Kidney Int 58:1765–1772
Kierdorf HP, Leue C, Arns S (1999) Lactate- or bicarbonate-buffered solutions in continuous extracorporeal renal replacement therapies. Kidney Int 56 (Suppl 72):S32–S36
Hartmann AF, Senn MJ (1932) Studies in the metabolism of sodium r-lactate. 1. Response of normal human subjects to the intravenous injection of sodium r-lactate. J Clin Invest 11:337–344
Traverso LW, Lee WP, Langford MJ (1986) Fluid resuscitation after an otherwise fatal hemorrhage: 1. Crystalloids solutions J Trauma 26:168–175
Healey MA, Davis RE, Liu FC, Loomis WH, Hoyt DB (1998) Lactated Ringer’s is superior to normal saline in a model of massive hemorrhage and resuscitation. J Trauma 45:894–899
Liskaser FJ, Bellomo R, Hayhoe M, Story D, Poustie S, Smith B, Letis A, Bennett M (2000) Role of pump prime in the etiology and pathogenesis of cardiopulmonary bypass-associated acidosis. Anesthesiology 93:1170–1173
McAuliffe JJ, Lind LJ, Leith DE, Fencl V (1986) Hypoproteinemic alkalosis. Am J Med 52:1415–1420
Wilkes P (1998) Hypoproteinemia, strong-ion diference, and acid–base status in critically ill patients. J Appl Physiol 84:1740–1748
Kellum JA, Bellomo R, Kramer DJ, Pinsky MR (1998) Etiology of metabolic acidosis during saline resuscitation in endotoxemia. Shock 9:364–368
Acknowledgements
Financial support was provided by research grants from the Australian and New Zealand College of Anesthetists and the Royal Brisbane Hospital Research Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morgan, T.J., Venkatesh, B. & Hall, J. Crystalloid strong ion difference determines metabolic acid–base change during acute normovolaemic haemodilution. Intensive Care Med 30, 1432–1437 (2004). https://doi.org/10.1007/s00134-004-2176-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2176-x