
Abstract
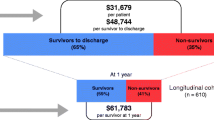
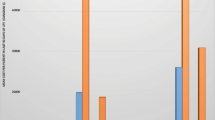
The purpose of this study was to compare the cost of a day spent in an intensive care unit and a day spent on a general nursing unit. A descriptive design was used, based on patient level data, to examine and compare unit costs per day for each of the ICU and non-ICU portions of a patient’s hospital stay. Records from 386 patients who were treated in a general medical/surgical ICU were analyzed. Records for patients who received both ICU and non-ICU care during their stay were retained. Patients were categorized according to whether they had received surgical care prior to admission to the ICU (surgical group) or had no surgical care (medical group). The groups were further divided, based on whether they were discharged from hospital (survivors), or died following transfers from the ICU (non-survivors). All four groups; surgical or medical, survivors and non-survivors, were analyzed separately. The ICU direct costs per day for survivors were between six and seven times those for non-ICU care. A one day substitution of general ward for ICU care would result in a cost reduction of $1,200 per patient for survivors. The results suggest that the savings achieved by moving a patient from ICU to non-ICU care are considerable, particularly for less severe surviving patients. In making such decisions, however, clinicians must examine prospective benefits as well as costs. If the health outcomes are not influenced, the savings from substitution are considerable, and there is a strong economic argument for substitution.
Résumé
Ce travail vise à comparer les coûts quotidiens de l’hospitalisation en unité de soins intensif (USI) à ceux de l’unité de soins réguliers. Un modèle basé sur l’observation des données spécifiques au patient est utilisé pour examiner et comparer les coûts quotidiens de chacune des périodes de séjour hospitalier dans l’USI et à l’extérieur de l’USI. Les dossiers de 386 patients traités dans une unité de soins intensifs médicochirurgicaux sont analysés. Seuls les dossiers de ceux qui ont reçu des soins à l’USI et hors de l’USI sont retenus. Deux catégories de patients sont établies; ceux qui ont reçu des soins chirurgicaux avant leur admission à l’USI (groupe chirurgical) et ceux qui n’ont pas reçu de soins chirurgicaux (groupe médical) avant leur admission à l’USI. Ces groupes ont été subdivisés: ceux qui ont reçu leur congé de l’hôpital (survivants) et ceux qui sont décédés après leur transfert de l’USI (décédés). Les quatre groupes: chirurgical, médical, survivant, décédé sont analysés indépendamment. Les coût directs par journée de séjour à l’USI par survivant se situent entre six et sept fois ceux du séjour hors USI. La substitution d’une journée d’USI pour une journée de séjour en unité régulière permet une économie de 1200 $ par survivant. Ces résultats permettent de croire que les économies réalisées en transférant un malade de l’USI vers une unité régulière sont importantes, particulièrement pour les survivants les moins malades. Cependant, en prenant de telles décisions, les cliniciens doivent tenir compte autant des bénéfices que des coûts. Si la substitution ne compromet pas le pronostic, les économies réalisées sont considérables et il devient impérieux d’adhérer à cette pratique.
Article PDF
Similar content being viewed by others

References
Russell LB. Technology in Hospitals: Medical Advances and Their Diffusion. Washington DC: The Brookings Institution, 1979.
Knaus WA, Thibault GE. Intensive care units today.In: McNeil BJ, Cravalho EG (Eds.). Critical Issues in Medical Technology. Boston: Auburn House Publishing Company 1982; 193–215.
Girolli MJ, Brown SJL. Reducing the costs of ICU admissions in Canada without diagnosis-related or case-mix groupings. Can Anaesth Soc J 1986; 33: 765–71.
Klem SA, Pollack MM, Getson PR. Cost, resource utilization, and severity of illness in intensive care. J Pediatr 1990; 116: 231–7.
Ridley S, Biggam M, Stone P. Cost of intensive therapy. A description of methodology and initial results. Anaesthesia 1991; 46: 523–30.
Slayter MA, James OF, Moore PG, Leeder SR. Costs, severity of illness and outcome in intensive care. Anaesth Intensive Care 1986; 14: 381–9.
Byrick RJ, Mindorff C, McKee L, Mudge B. Costeffectiveness of intensive care for respiratory failure patients. Crit Care Med 1980; 8: 332–7.
Civetta JM, Hudson-Civetta JA. Maintaining quality of care while reducing charges in the ICU. Ann Surg 1985; 202: 524–30.
Gilbertson AA, Smith JM, Mostafa SM. The cost of an intensive care unit: a prospective study. Intensive Care Med 1991; 17: 204–8.
Oye RK, Bellamy PE. Patterns of resource consumption in medical intensive care. Chest 1991; 99: 685–9.
Detsky AS, Stricker SC, Mulley AG, Thibault GE. Prognosis, survival, and the expenditure of hospital resources for patients in an intensive care unit. N Eng J Med 1981; 305: 667–72.
Lemeshow S, Teres D, Klar J, Avruni JS, Gehlbach SH, Rapoport J. Mortality probability models (MPM II) based on an international cohort of intensive care unit patients. JAMA 1993; 270: 2478–86.
Cullen DJ, Keene R, Waternaux C, Kunsman JM, Caldera DL, Peterson H. Results, charges, and benefits of intensive care for critically ill patients: update 1983. Crit Care Med 1984; 12: 102–6.
Wagner DP, Wineland TD, Knaus WA. The hidden costs of treating severely ill patients: charges and resource consumption in an intensive care unit. Health Care Financing Review 1983; 5: 81–6.
Nichols D. Developing actual costs of patient services: the University of Alberta Hospitals. Journal of Ambulatory Care Management 1993; 16: 61–8.
Norusis MJ. SPSS for Windows. Chicago, Illinois: SPSS Institute, 1993.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Norris, C., Jacobs, P., Rapoport, J. et al. ICU and non-ICU cost per day. Can J Anaesth 42, 192–196 (1995). https://doi.org/10.1007/BF03010674
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03010674